
Abstract
Background:
Subclinical and overt thyroid dysfunction is easily detectable, often modifiable, and, in younger age groups, has been associated with clinically relevant outcomes. Robust associations in very old persons, however, are currently lacking. This study aimed to investigate the associations between (sub-)clinical thyroid dysfunction and disability in daily living, cognitive function, depressive symptoms, physical function, and mortality in people aged 80 years and older.
Methods:
Four prospective cohorts participating in the Towards Understanding Longitudinal International older People Studies (TULIPS) consortium were included. We performed a two-step individual participant data meta-analysis on source data from community-dwelling participants aged 80 years and older from the Netherlands, New Zealand, United Kingdom, and Japan. Outcome measures included disability in daily living (disability in activities of daily living [ADL] questionnaires), cognitive function (Mini-Mental State Examination [MMSE]), depressive symptoms (Geriatric Depression Scale [GDS]), physical function (grip strength) at baseline and after 5 years of follow-up, and all-cause five-year mortality.
Results:
Of the total 2116 participants at baseline (mean age 87 years, range 80–109 years), 105 participants (5.0%) were overtly hypothyroid, 136 (6.4%) subclinically hypothyroid, 1811 (85.6%) euthyroid, 60 (2.8%) subclinically hyperthyroid, and 4 (0.2%) overtly hyperthyroid. Participants with thyroid dysfunction at baseline had nonsignificantly different ADL scores compared with euthyroid participants at baseline and had similar MMSE scores, GDS scores, and grip strength. There was no difference in the change of any of these functional measures in participants with thyroid dysfunction during five years of follow-up. Compared with the euthyroid participants, no 5-year survival differences were identified in participants with overt hypothyroidism (hazard ratio [HR] 1.0, 95% confidence interval [CI 0.6–1.6]), subclinical hypothyroidism (HR 0.9 [CI 0.7–1.2]), subclinical hyperthyroidism (HR 1.1 [CI 0.8–1.7]), and overt hyperthyroidism (HR 1.5 [CI 0.4–5.9]). Results did not differ after excluding participants using thyroid-influencing medication.
Conclusions:
In community-dwelling people aged 80 years and older, (sub-)clinical thyroid dysfunction was not associated with functional outcomes or mortality and may therefore be of limited clinical significance.
Introduction
Circulating levels of thyroid hormones influence cell metabolism of nearly all types of tissues in the human body (1). Consequently, in young and middle-aged individuals, both hypo- and hyperthyroidism have been associated with several adverse clinical outcomes (2 –5).
However, evidence is starting to accumulate that adverse health associations of thyroid dysfunction, found in younger age groups, cannot be extrapolated to persons aged 80 years and older (6), possibly due to changes in thyroid metabolism associated with aging. For example, in a recent meta-analysis of 13 studies investigating the association between subclinical hypothyroidism and cognitive decline or the risk of dementia, a significant risk was identified in participants younger than 75 years but not in participants older than 75 years (7). In addition, clinical outcomes such as cardiovascular risk (8 –10) and activities of daily living (ADL) (11), associated with thyroid dysfunction in younger age groups, have not been replicated in older adults (12).
Researchers are currently unable to reach robust conclusions for the people aged 80 years and older due to methodological or logistic difficulties, such as low numbers of older participants included.
In this study, we combine the individual participant data (IPD) from four large, international prospective cohorts of community-dwelling very old persons to investigate associations between (sub-)clinical thyroid dysfunction and disabilities in ADL, functioning (including cognitive function, depressive symptoms, and physical function), and mortality in people aged 80 years and older.
Materials and Methods
Study population
Ethical approval was obtained before initiating recruitment and before subsequent waves of data collection from the following institutional review bodies: Medical Ethical Committee of the Leiden University Medical Center (the Leiden 85-plus study), the Northern X Regional Ethics Committee of New Zealand (LiLACS NZ study), the Newcastle and North Tyneside 1 research ethics committee (Newcastle 85+ study) and the ethics committee of Keio University School of Medicine (Tokyo Centenarian Study).
The Towards Understanding Longitudinal International older People Studies (TULIPS) Consortium was established in 2014 and set out to investigate determinants of successful aging and health outcomes in older persons using the data from large-scale, prospective, population-based cohort studies. The data for the analyses in this article were provided by four international cohort studies: The Leiden 85-plus study, The Life and Living in Advanced Age: a cohort study in New Zealand (LiLACS NZ) study, Newcastle 85+ study, and Tokyo Centenarian study (TCS).
The Leiden 85-plus study
All inhabitants of Leiden, The Netherlands, reaching the age of 85 years between September 1997 and September 1999 (n = 705) were eligible for participation, of which 599 participated (13). During a 5-year follow-up, participants were visited for interviews, performing of functional tests, and the collection of venous blood samples. Thyrotropin (TSH) and free thyroxine (fT4) at baseline were available for 553 participants.
LiLACS NZ study
The LiLACS NZ study consists of two cohorts running in parallel, one with exclusively Māori (the indigenous people of New Zealand) and one with non-Māori participants (14). All potential participants living in the Lakes or Bay of Plenty District Health Board areas in 2010 (aged 85 years in 2010 for non-Māori or aged 80–90 years in 2010 for Māori) were eligible (n = 1636), of which 937 were enrolled (15). Participants were visited annually for a structured questionnaire, a physical health assessment, and collection of venous blood samples. TSH and fT4 at baseline were available for 195 participants in the Māori cohort and for 352 participants in the non-Māori cohort.
Newcastle 85+ study
All citizens born in 1921 registered with a participating general practitioner in Newcastle upon Tyne or North Tyneside primary care trusts, the United Kingdom, were approached in 2006 for participation (n = 1470), of which 851 were enrolled with complete health assessment and record review (16). Participants received visits at baseline and at 18, 36, and 60 months of follow-up for the questionnaire collection, measurements and function tests, and blood tests (17). TSH and fT4 at baseline were available for 763 participants.
Tokyo Centenarian study
Of an estimated 1735 centenarians living in Tokyo, Japan, 1194 centenarians (68.8%) were randomly selected and approached with a survey between 2000 and 2002, of which 304 agreed to participate (18). All participants were visited for blood sample collection, cognitive, mental, and physical functioning assessments. TSH and fT4 at baseline were available for 251 participants.
Data collected
For all cohorts, baseline data per participant on sociodemographic characteristics (age, sex, race/ethnicity, current tobacco and alcohol use, and education level) were collected. Follow-up data for thyroid-influencing medication use (levothyroxine, antithyroid medication, amiodarone, lithium, glucocorticosteroids, or interferon-α) and the outcome variables described below were collected at every visit.
Thyroid status
In the Leiden 85-plus study, nonfasting blood samples were drawn between 8 and 11 a.m., and plasma TSH and fT4 levels were analyzed using a Elecsys 2010 automated system (Hitachi, Tokyo, Japan) (19). For the LiLACS NZ cohort, fasting blood samples were either drawn at time of interview or in a local public laboratory. Thyroid assays were analyzed using a Cobas immunoassay system (Roche, Switzerland). In the Newcastle 85+ study, blood was drawn after an overnight fast before 10.30 a.m. and analyzed using a Centaur chemiluminescent immunoassay system (Siemens, United Kingdom) (20). In the TCS, nonfasting blood samples were obtained at time of interview and were stored at −80°C until the subsequent assay was performed. Serum TSH and fT4 concentrations were measured using a chemiluminescent enzyme immunoassay with a Lumipulse Forte fully automated system (Fuji Rebio, Tokyo, Japan).
For all studies, the reference ranges were defined as 0.3–4.8 mIU/L for serum TSH and as 13–23 pmol/L (1.01–1.79 ng/dL) for fT4. Five clinical strata of thyroid function at baseline were used to classify participants: overt hypothyroidism (TSH >4.8 and fT4 < 13), subclinical hypothyroidism (TSH >4.8 and fT4 within reference range), euthyroidism (0.3 ≤ TSH ≤4.8), subclinical hyperthyroidism (TSH <0.3 and fT4 within reference range), and overt hyperthyroidism (TSH <0.3 and fT4 > 23).
Outcome measures
Disability in ADL
Disability in ADL was measured in the Leiden 85-plus study using the Groningen Activity Restriction Scale [GARS (21), range 18–72, higher summed scores more disability] consisting of 18 items of daily function and independent living. In the Newcastle 85+ study, a summed disability score derived from 17 ADL was used (range 0–17, higher summed scores more disability) (20). For the LiLACS NZ study, the Nottingham Extended Activities of Daily Living (NEADL) Index (range 0–15, higher summed scores less disability) (22) was used. For the TCS, ADL was assessed at baseline using the Barthel Index (BI, range 0–100, higher summed index scores less disability) (23).
All disability in ADL questionnaires used have been shown to be valid and reliable indicators of physical disability in older persons (24 –27).
Cognitive function
In all studies, cognitive function was assessed with the Mini-Mental State Examination (MMSE) questionnaire at every visit (maximum score of 30). The MMSE questionnaire has previously been validated in this age group (28). Higher scores indicate better cognitive functioning. MMSE scores in TCS were available at baseline.
Depressive symptoms
The Geriatric Depression Scale (GDS-15) was used to evaluate the presence of depressive symptoms in the Leiden 85-plus, LiLACS NZ, and Newcastle 85+ cohorts (29). This questionnaire contains 15 items adding up to maximum summed score of 15, with higher scores indicating more depressive symptoms. The GDS-15 questionnaire has previously been validated in this age group (29). In the Leiden 85-plus and Newcastle 85+ cohorts, the GDS was not undertaken in individuals with established cognitive impairment. Depressive symptoms were not assessed in TCS.
Physical function
Hand grip strength measurements in kilograms were used as a proxy for overall muscle strength (30), and handheld dynamometry has been validated in this age group for measuring muscle strength (31). A Jamar hand dynamometer (Sammons Preston, Inc., IL) was used in the Leiden 85-plus study. A Takei hand dynamometer Grip-D (Takei Scientific Instruments Co., Niigata-City, Japan) was used in the LiLACS-NZ and Newcastle 85+ cohorts. Grip strength was not assessed in TCS.
Mortality
Date of death was collected from the records of Statistics Netherlands (Centraal Bureau voor de Statistiek, The Hague, The Netherland) for the Leiden 85-plus study. General practitioner records and mortality administrative data (held by the Ministry of Health) were consulted for the LiLACS NZ study. Information on mortality for the Newcastle 85+ study was provided by NHS Digital (United Kingdom). For TCS, all-cause mortality was ascertained by telephone contact or mail survey conducted every 12 months (32). Survival time was calculated as the time between the baseline visit and date of death or censored at 5 years if death had not yet occurred.
Statistical analyses
All measurements are analyzed at yearly intervals from baseline (i.e., after 1, 2, 3, 4, and 5 years). Measurements for Phase 2 of the Newcastle 85+ study, however, were taken 18 months after baseline and, to allow linear mixed model analyses, were assumed constant at the 2-year analysis.
Results were reported separately for the Māori and non-Māori cohorts to do justice to potential differences in Māori and non-Māori preferences and practices in research (33).
A two-stage IPD meta-analysis approach was employed for all analyses (34,35). All variables for the analyses were coded similarly for each study, analyzed on a study level using the same syntax, and finally pooled for meta-analysis.
Study-level analyses
Continuous variables are presented as mean with standard deviation or as median with interquartile range (IQR), where appropriate, and categorical variables are presented as frequency with percentage of the total.
Five-year survival analysis was carried out using Cox proportional hazards regression models, corrected for age and sex, and presented as a hazard ratio (HR) with 95% confidence intervals [CIs]. The proportionality of hazards assumption was checked.
Repeated-measurements linear mixed-effect models using restricted maximum likelihood estimation and an unstructured covariance matrix, corrected for age and sex, were used to assess the associations between thyroid function and MMSE, GDS, grip strength, and disability in ADL.
Disability in ADL scores were inverted for TCS (BI), and for the LiLACS-NZ study, the mean was subtracted from the scores (NEADL) to standardize the direction of the scales, a prerequisite for pooling (36). Considering that for disability in daily living the same outcome was measured using different scales in the cohorts, standardized mean differences (SMDs) were calculated for each study using independent-groups pretest–post-test calculations (37). By dividing the mean outcome difference between a thyroid dysfunction group and the euthyroid group with the standard deviation among the participants, the size of the between-group effect in each study is normalized relative to the variability observed in the study (see Supplementary Data S1).
All analyses used the euthyroid participants as the reference group or used TSH levels as a continuous independent variable.
Pooled analyses
All cohort effect estimates were subsequently pooled using random-effects models with inverse-variance weighting and summarized in forest plots. Inconsistency between cohorts due to heterogeneity was quantified using the I 2-statistic and found not to be important for all summarized values (I 2 < 40%).
Sensitivity analysis
All participants (n = 236, 11%) using any form or combination of thyroid-influencing medication (levothyroxine, antithyroid medication, amiodarone, lithium, glucocorticosteroids, or interferon-α) were excluded for additional sensitivity analyses.
The study-level analyses were performed using IBM SPSS Statistics version 22.0 (IBM, Armond, NY). All pooled analyses were performed using Review Manager 5.3 (The Cochrane Collaboration, Copenhagen, Denmark) (38).
Results
Table 1 displays the baseline characteristics of the combined study population and for the cohorts separately. The combined cohort consisted of 2116 participants. The mean participant age was 87 (range 79–109) years and 1311 (62%) were female. The median follow-up time over all cohorts was 5.3 (IQR 2.6–6.9) years.
Baseline Characteristics of Study Participants
IQR, interquartile range; GARS, Groningen Activity Restriction Scale; NEADL, Nottingham Extended Activities of Daily Living; ADL, activities of daily living; BI, Barthel Index; TSH, thyrotropin; fT4, free thyroxine; LiLACS NZ, Life and Living in Advanced Age: a cohort study in New Zealand.
The median serum TSH level in the combined cohort was 2.1 (IQR 1.3–3.2) mIU/L, and the median serum fT4 was 14.9 (IQR 13.2–16.5) pmol/L, both within the normal reference ranges. One thousand eight hundred eleven (85.6%) participants were euthyroid. Thyroid dysfunction was found in 305 (14.4%) participants: 136 (6.4%) participants with subclinical hypothyroidism, 105 (5.0%) with overt hypothyroidism, 60 (2.8%) with subclinical hyperthyroidism, and 4 (0.2%) with overt hyperthyroidism. In the hypothyroidism categories, 18 (17.1%) participants with overt hypothyroidism and 41 (30.1%) participants with subclinical hypothyroidism used a preparation of thyroid hormone at any point during the follow-up.
The median MMSE score was 27 points (IQR 23–29), and the median GDS score was 1 point (IQR 1–2). The median disability in ADL scores were 28 (IQR 22–40) on the GARS questionnaire (Leiden 85-plus study); 19 (IQR 16–20) for the Māori subgroup and 19 (IQR 17–20) for the non-Māori subgroup on the NEADL questionnaire (LiLACS NZ); 3.0 (IQR 1–7) on the ADL sum scores (Newcastle 85+ study); and 45 (IQR 15–80) on the BI questionnaire (TCS).
Figure 1 shows ADL scores according to clinical thyroid state at baseline and after 5 years of follow-up. At baseline, no significant SMDs in ADL scores were identified in the clinical strata with thyroid dysfunction compared with the euthyroid participants; the mean difference was 0.01 [CI −0.19 to 0.21] points for overt hypothyroidism, −0.00 [CI −0.18 to 0.17] points for subclinical hypothyroidism, 0.00 [CI −0.25 to 0.26] points for subclinical hyperthyroidism, and 0.01 [CI −0.97 to 1.00] points for overt hypothyroidism. Although all groups showed decline in ADL, over time there were no significant SMDs of decline in ADL scores (SMD between −0.01 and 0.00, IQR between −0.99 and 0.97) between euthyroid participants and participants with thyroid dysfunction. In this study population, a calculated SMD of −0.01 corresponds with a 3.5-point decrease on the GARS scale.

Activities of daily living per clinical thyroid stratum at baseline and after five years of follow-up. Standardized mean differences calculated per clinical thyroid stratum and per cohort using independent-groups pretest–post-test calculations compared with the euthyroid participants. Higher scores represent worse outcomes. IQR, interquartile range; GARS, Groningen Activity Restriction Scale; NEADL, Nottingham Extended Activities of Daily Living; BI, Barthel Index.
At baseline, estimated marginal means of MMSE scores did not differ significantly between participants with thyroid dysfunction (means between 23.6 points [CI 18.2–29.0] and 26.3 points [CI 25.5–27.4]) and participants with euthyroidism (mean 23.7 points [CI 21.0–26.5]). Similarly, no differences were found for depressive symptom scores (means between 1.9 points [CI 1.5–2.3] and 5.1 points [CI 2.7–7.5] for participants with thyroid dysfunction, and 2.1 points [CI 1.4–2.7] for euthyroid participants) and grip strength (means between 18.1 kg [CI 9.8–26.4] and 26.0 kg [CI 22.6–29.5] for participants with thyroid dysfunction, and 24.1 kg [CI 23.1–25.1] for euthyroid participants) (Table 2).
Functional Parameters Per Clinical Thyroid Stratum at Baseline
Euthyroidism is the reference group.
Estimated marginal means [95% confidence intervals] estimated using linear mixed models per cohort, adjusted for baseline age and sex, and pooled using random-effects models with inverse-variance weighting.
Beta [95% confidence intervals] estimated using repeated-measures linear mixed models per cohort, adjusting for baseline age and sex, and pooled using random-effects models with inverse-variance weighting, representing change in outcome measure over five years of follow-up.
MMSE, Mini-Mental State Examination; GDS, Geriatric Depression Scale.
Over time, no differences were identified in decline in MMSE scores for participants with thyroid dysfunction (means between −0.4 points less decline [CI −1.4 to 0.5] and 0.4 points more decline [CI −0.9 to 2.1]) compared with euthyroid patients. Nor were differences identified for depressive symptoms scores (means between −0.1 points less decline [CI −0.6 to 0.3] and 1.7 points more decline [CI −0.2 to 3.5] for participants with thyroid dysfunction compared with euthyroid participants) and grip strength (means between −3.3 [CI −10.0 to 11.3] and 1.7 [CI −1.9 to 5.2] for participants with thyroid dysfunction compared with euthyroid participants) (Table 2). Forest plots for all thyroid categories stratified per cohort are presented in the Supplementary Data.
Pooled HRs were calculated to estimate five-year mortality (Fig. 2). No difference in survival risks was found for overt hypothyroidism (HR 0.98 [CI 0.63–1.51]), subclinical hypothyroidism (HR 0.89 [CI 0.67–1.17]), subclinical hyperthyroidism (HR 1.11 [CI 0.75–1.65]), or overt hypothyroidism (HR 1.46 [CI 0.36–5.88]). Similarly, in a cox-regression survival analysis across the clinical thyroid strata, TSH as a continuous variable did not predict 5-year mortality (HR 0.99 [CI 0.96–1.02]).
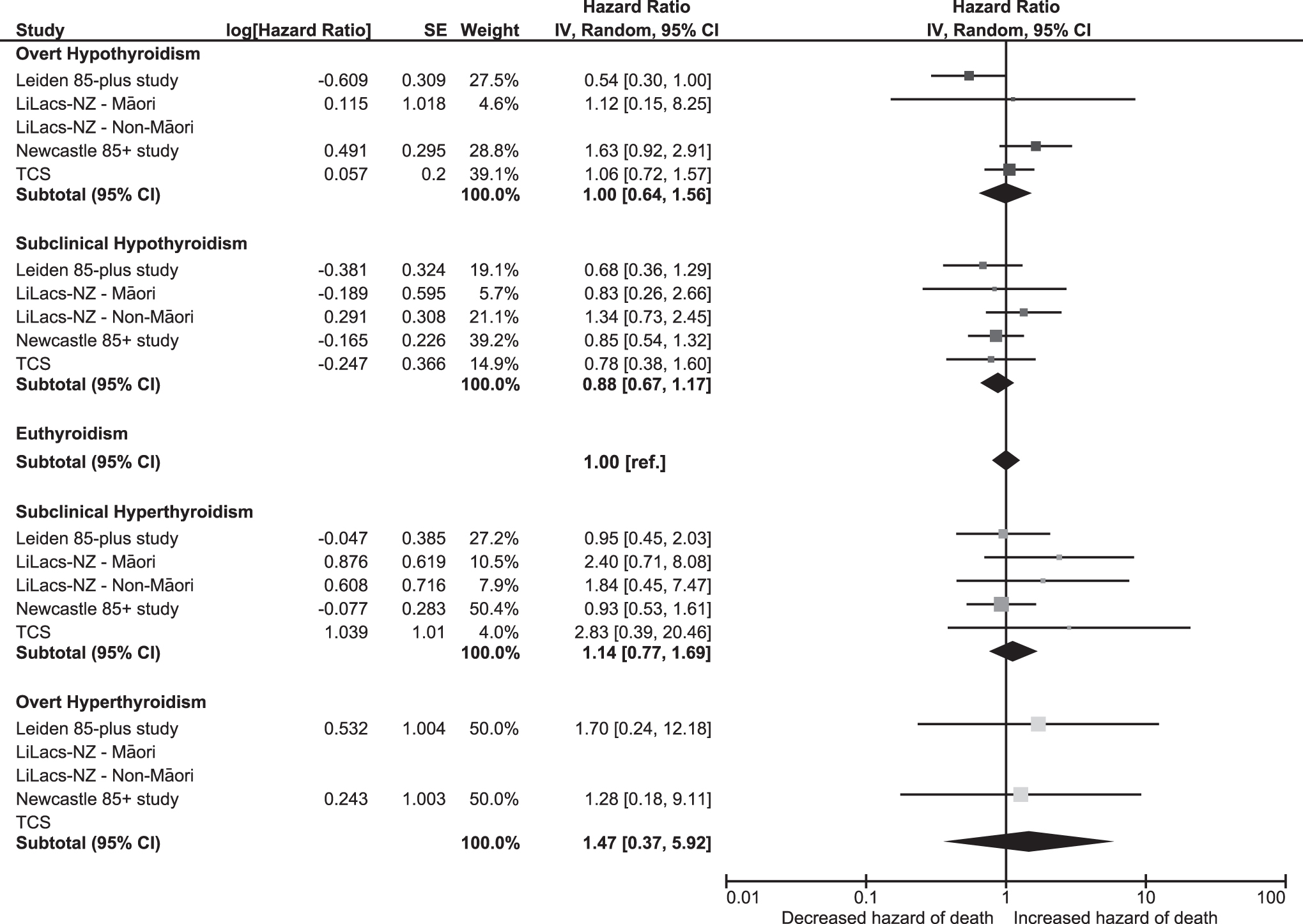
All-cause five-year mortality per clinical thyroid stratum at baseline. Pooled hazard ratios [95% CI] per clinical thyroid stratum estimated using Cox proportional hazards regression models adjusting for sex and age at baseline compared with participants with euthyroidism. When mortality rates were too, low hazard ratios could not be estimated. CI, confidence interval.
In sensitivity analyses, excluding all participants (n = 236, 11%) using any or a combination of thyroid-influencing medications at any point during follow-up did not alter the association estimates substantially in either direction of effect or significance (data not shown).
Discussion
The findings of this large IPD meta-analysis of four prospective observational cohorts among community-dwelling participants aged 80 years and older are twofold. First, there was no association of thyroid dysfunction with disability in ADL nor with cognition, physical function, or depressive symptoms at baseline or during the follow-up. Second, thyroid dysfunction was not associated with increased mortality during an average 5 years of follow-up.
Earlier research investigating the outcomes of thyroid dysfunction in old age yielded greatly conflicting data. For example, some studies demonstrated decreased cognitive function (39 –41), increased depressive symptoms (42,43), decreased physical function (44), and increased cardiovascular or all-cause mortality (45 –47) in participants with subclinical or overt thyroid dysfunction. Others, however, were unable to replicate these findings (10,48 –58).
Due to differences in, for example, the thyroid reference and age ranges used, follow-up time chosen, the participants selected, study design employed, and outcome measures used, the aforementioned studies could not be pooled without suffering from significant methodological heterogeneity. This study was optimized to address these specific limitations by pooling the results of four of the most comparable cohort studies of community-dwelling oldest old.
Our findings are in line with most previous publications from the individual data sets used in this study, such as an absence of association between thyroid function and disabilities in daily living, cognitive function, and depressive symptoms (19). Additionally, no association was found between fT4 or TSH and all-cause mortality in earlier studies (20,59). However, some nonunanimous results have been described using these data sets as well. For instance, in the Leiden 85-plus study, increasing levels of TSH were associated with lower mortality rates (19). It should be noted that the aggregate negative findings in our pooled analyses do not invalidate any earlier identified associations in any of the individual cohorts or other publications, as these may be a representation of associations in that specific population being sampled, at that time, using those specific methods, study designs, and analyses.
Nevertheless, the findings from this IPD meta-analysis do more accurately reflect an estimation of effects for a more universal population of older people, with uniform definitions and follow-up times, by pooling the results and allowing statistically for sampling error and biases. These findings suggest that the influence of thyroid dysfunction on disabilities in daily living, cognitive function, depressive symptoms, physical function, and mortality in persons aged 80 years and older is limited, particularly in the subclinical thyroid disease subgroups.
For older age groups with subclinical thyroid dysfunction, evidence supporting beneficial effects from treatment has generally been of lower grade and contradictory, as acknowledged in international guidelines. Currently, these recommend routine or trial treatment in patients older than 65 years with subclinical thyroid dysfunction, although individualized, gradual and closely monitored (60,61). However, they simultaneously acknowledge the lack of evidence in the scientific literature and call for large prospective studies with a long-term follow-up in older persons. Recently, two international multicenter trials demonstrated no beneficial effects of levothyroxine treatment for subclinical hypothyroidism in persons aged 65 years and older, and in persons aged 80 years and older (62,63).
The lack of associations between (mild) thyroid dysfunction and relevant outcomes described in this article, and the absence of beneficial effects of levothyroxine treatment for subclinical hypothyroidism in older persons, reinforces the notion that for older persons with subclinical hypothyroidism, routine treatment does not seem indicated and that the thresholds for treatment initiation (i.e., currently the normal reference ranges) ought to be redefined. This is not necessarily the same as the definition of the reference ranges. Whether all thyroid reference ranges in aging need to be reevaluated to distinguish physiological states from pathophysiological ones is still a much-debated issue and will require further evaluation. Future research, focusing on how thyroid-related (patho-)physiological processes change with aging and how these affect outcomes, are needed, including the influence of other established thyroid markers and treatment modalities.
This study used data from some of the largest, unselected, population-based observational cohorts of community-dwelling persons aged 80 years and older to date, with considerable follow-up time and a substantial international representation of countries, cultures, and persons. The IPD meta-analysis design allowed for harmonization of thyroid function categories, standardization of definitions and variables, and consistency in analyses. The two-step design allowed the presentation of overall results on an aggregate level, while maintaining maximum transparency on any potential intercohort variation, for example, between Māori and non-Māori populations.
Some limitations do need to be acknowledged. First, TSH and fT4 were only available for the baseline measurements, and it could be possible that thyroid function changed during the observational periods. However, a recent study in almost 3000 community-dwelling older persons has demonstrated high stability of thyroid function over five years of follow-up, and therefore, we estimate the odds of erroneous misclassification as small (64). Second, the ADL questionnaires were too heterogeneous in scale and structure to pool in any traditional way. Standardization with the SMD method allowed for methodologically sound pooling but may have introduced additional uncertainty to the analyses leading to underestimation of true associations.
In participants aged 80 years and older, (sub-)clinical thyroid dysfunction is not associated with functional outcomes or mortality and may therefore be of limited clinical significance.
Footnotes
Authors' Contributions
Dr. R.S.D.P. had full access to the study data and article and takes responsibility for the integrity of the work as a whole. The corresponding author attests that all listed authors meet authorship criteria according to the ICMJE Recommendations and that no others meeting the criteria have been omitted. Study concept and design: R.S.D.P., R.K.E.P., W.P.J.d.E., N.K., C.J., Y.A., and J.G. Acquisition, analysis, or interpretation of data: R.S.D.P., R.K.E.P., N.K., C.J., Y.A., N.H., and J.G. Drafting of the article: R.S.D.P., R.K.E.P., and J.G. Critical revision of the article for important intellectual content: R.S.D.P., R.K.E.P., S.P.M., W.P.J.d.E., N.K., R.T., C.J., S.H.S.P., Y.A., N.H., and J.G. Statistical analysis: R.S.D.P. Obtained funding: N.K. Administrative, technical, or material support: R.S.D.P., R.K.E.P., N.K., C.J., S.H.S.P., Y.A., and J.G. Supervision: N.K., C.J., Y.A., and J.G.
Explanation of the Role of Funder/Sponsor
The sponsors had no role in the design and conduct of the study, in the collection, analysis, and interpretation of the data, nor in the preparation, review, or approval of the article.
Access to Data Statement
Request for access to the TULIPS consortium data is to be addressed to the corresponding author.
Acknowledgments
The Newcastle 85+ study is grateful to Mr. Steve Turner of the Royal Victoria Infirmary Biochemistry laboratories for invaluable assistance with thyroid hormone assays. The LiLACS NZ study wishes to acknowledge the study participants, their families, and whanau for supporting the study. We are extremely grateful Te RōpuKaitiaki o ngā tikanga Māori for their guidance, and we acknowledge the community partners (Western Bay of Plenty Primary Health Organisation, Ngā Matāpuna Oranga Kaupapa Māori Primary Health Organisation, Te Korowai Aroha Trust, Te Rūnanga o Ngati Pikiao, Rotorua Area Primary Health Services, Ngati Awa Research and Archives Trust, Te Rūnanga o Ngati Irapuaia, and Te Whanau a Apanui Community Health Centre).
Author Disclosure Statement
No competing financial interests exist.
Funding Information
The Leiden 85-plus study was partly funded by an unrestricted grant from the Dutch Ministry of Health, Welfare and Sports (1997–2001). The Life and Living in Advanced Age: a cohort study in New Zealand, Te Puāwaitanga o Nga Tapuwae Kia Ora Tonu, was funded by the Health Research Council of New Zealand program grant (HRC 09/068B), Ministry of Health New Zealand (MOH ref: 345426/00), and Ngā Pae o te Māramatanga (the New Zealand National Centre for Research Excellence for Māori; funded Māori engagement and project management) project grant, National Heart Foundation project grant for investigating cardiac markers and Oakley Mental Health Foundation project grant for investigating dementia. The Tokyo Centenarian study was supported in part by a grant from the Japanese Ministry of Health and Welfare for the Scientific Research Project on Longevity (N.H.) and by the Program for Initiative Research Projects from Keio University and Keio University Global Research Institute (Y.A.). The Newcastle 85+ study was funded by the Medical Research Council (grant no. G0500997), the Biotechnology and Biological Sciences Research Council, the Dunhill Medical Trust, the National Institute for Health Research Biomedical Research Centre at Newcastle upon Tyne Hospitals National Health Service Foundation Trust, and Newcastle Hospitals Healthcare Charity.
Supplementary Material
Supplementary Data