
Abstract
Background:
Differentiated thyroid cancer (DTC) is the only cancer entity for which the UICC/AJCC (Union for International Cancer Control and American Joint Committee on Cancer) TNM (tumor–node–metastasis) staging system involves an age cutoff as a prognostic criterion. However, the optimal age cutoff has not yet been determined in detail. The aim of our study was therefore to investigate the optimal age cutoff for the TNM staging system to predict disease-specific survival (DSS) with a focus on differences between patients with papillary thyroid cancer (PTC) and follicular thyroid cancer (FTC).
Methods:
We retrospectively studied two large well-described cohorts of adult DTC patients from a Dutch and a German university hospital. DSS was analyzed for DTC overall, and for PTC and FTC separately, using several age cutoffs (per 5-year increment between 20 and 85 years and subsequently 1-year increments between 35 and 55 years), employing the histopathological criteria from the TNM staging system, eighth edition.
Results:
We included 3074 DTC patients (77% PTC and 23% FTC; mean age at diagnosis was 49 years). Median follow-up was seven years. For DTC and for PTC and FTC separately, the majority of the age cutoffs had a better statistical model performance than a model with no age cutoff. For DTC overall and for PTC, an age cutoff of 50 years had the best statistical model performance, while it was 40 years for FTC.
Conclusions:
In this large European population of DTC patients, when employing the histopathological criteria of the TNM system (eighth edition), the optimal age cutoff to predict DSS is 50 years rather than the 55 years currently in use. With the optimal age cutoff being 50 years for PTC and 40 years for FTC, there was a substantial difference in age cutoff for the respective histological entities. Therefore, implementation of different age cutoffs for PTC and FTC could improve the predictive value of the TNM staging system.
Introduction
The joint Union for International Cancer Control and American Joint Committee on Cancer (UICC/AJCC) tumor–node–metastasis (TNM) staging system in its various iterations is consistently among the best systems used to predict disease-specific survival (DSS) in differentiated thyroid cancer (DTC) (1,2). For DTC, a unique feature of the TNM staging system is the fact that age plays a major role in the classification of patients into different prognostic groups, which is in contrast to other malignancies (1). In January 2018, the eighth edition of the UICC/AJCC TNM staging system for DTC was introduced in clinical practice (3). Besides a changed definition of T3 tumors and a downstaging of N1 disease, a raised age cutoff from 45 to 55 years was a major difference compared with the seventh edition (1). Several studies compared the performance of the eighth with the seventh edition in patients with DTC (4 –18), and the majority of these studies showed a slight superiority of the eighth edition.
An issue in DTC staging concerns clinical differences between its histological subtypes. It is well established that follicular thyroid cancer (FTC) has a different clinical manifestation than papillary thyroid cancer (PTC) as lymph node metastasis is uncommon and patients are, in general, older and more often have distant metastasis at initial presentation (19). Two studies showed superiority of the eighth edition compared with the seventh edition of the TNM system in patients with FTC (9,11), while another study showed no differences (13). To the best of our knowledge, however, it has not yet been firmly established whether the age cutoffs for FTC and PTC are, in fact, similar.
The raised age cutoff for the eighth edition of the TNM system was based on three earlier studies showing that an age cutoff of 55 years led to better prediction of DSS in patients with DTC (20 –22). However, these studies were performed using the histopathological criteria of the seventh edition of the TNM staging system; an extrapolation of these results to the different histopathological staging criteria of the eighth edition may therefore not necessarily be correct. Consequently, the aim of the present study was to investigate the optimal age cutoff for the TNM system to predict DSS, employing the histopathological criteria of the current eighth edition. The secondary aim of our study was to examine whether differences with regard to age cutoff exist between patients with PTC and FTC.
Materials and Methods
Study population
For the current study, we combined two established well-described databases from The Netherlands and Germany (9,10,23 –27). These databases were earlier used to investigate, among others, the predictive value of the eighth edition of the TNM system in patients with DTC (9,10).
From the Erasmus Medical Center (Erasmus MC), Rotterdam, The Netherlands, we retrospectively obtained data from patients, aged 18 years or above, who were diagnosed and/or treated for either PTC or FTC (including Hürthle cell carcinoma) between January 2002 and December 2016. All patients underwent thyroid surgery and were treated according to the previous and current Dutch guidelines (28). Demographic, disease, treatment, and mortality characteristics were obtained from patient records. Cause of death was obtained from hospital or general practitioner records. Survival was defined as the time from the date of initial diagnosis to the date of the last known follow-up, death, or end of study (December 2017), whichever occurred first. The study protocol was approved by the Institutional Review Board of the Erasmus MC.
From the University of Würzburg thyroid cancer database, we retrospectively obtained data on patients, aged 18 years or above, who were treated for either PTC or FTC between January 1980 and December 2015. All patients underwent thyroid surgery and were treated further in accordance with the standards of the respective time period, as described previously (25,26). Demographic, disease, treatment, and mortality data were immediately recorded in the database at each patient visit. Cause of death was obtained from hospital or general practitioner records or public registration offices. Survival was defined as the time from the initial diagnosis to last date of follow-up, death, or end of study data collection (December 2016), whichever occurred first. The Würzburg Thyroid Cancer Database was maintained with approval of and continuous monitoring by the local medical ethics committee.
Patients from both cohorts were reclassified using the histopathological criteria from the eighth edition of the TNM system, but applying different age cutoffs. For this purpose, we investigated age cutoffs at 5-year increments from 20 up to and including 85 years. Additionally, we also investigated 1-year increments between 35 and 55 for sensitivity analysis. These analyses were performed separately for both PTC and FTC, as well as combined for the overall DTC patient population.
Statistical analyses
For DTC, using the previously described age cutoffs for the TNM staging system, DSS was analyzed using the Kaplan–Meier method and compared across stages using the log-rank test. To assess the statistical model performance of the TNM staging system with different age cutoffs, we used the concordance index (Harrell's C-index) (29,30), Akaike information criterion (AIC) (31), and Bayesian information criterion (BIC) (32). The C-index measures the discriminative power of a model and is a measure of goodness of fit. It ranges from 0.5 to 1.0, with 0.5 meaning the model is no better than random chance and 1.0 being the perfect prediction model. Furthermore, the AIC and BIC measure the relative quality of a statistical model and they provide the relative information lost when a statistical model is used to represent the true model. The model with the highest C-index and lowest AIC and BIC values is considered to be the best model for predicting outcomes. Therefore, using these three criteria, we aimed to find the age cutoff that optimizes statistical performance. The same analyses as for DTC were performed for both PTC and FTC separately. Thereafter, a Cox proportional hazards model was created to estimate and compare the effects of both disease types on DSS. These analyses were performed, unadjusted and adjusted for age, sex, and cohort.
p-Values below 0.05 were considered significant. All analyses were performed using either SPSS Statistics for Windows (version 25.0) or the open-source statistical software R (version 3.4.1) with the survC1 package for estimating the C-index (33).
Results
Population characteristics
A total of 3074 patients fulfilled the inclusion criteria and had sufficient information to adequately determine their TNM stage. Table 1 lists the characteristics of the study population. PTC was present in 2355 patients (77%), whereas the remaining 719 patients (23%) had FTC. The median available follow-up time was 84 months. Of the 3074 patients, the majority (2254; 73%) were included from the University of Würzburg. These characteristics can be found in Supplementary Table S1.
Characteristics of the Study Population
Values are means ± standard deviations, medians (25–75 interquartile range), or numbers of patients (percentage of the respective population).
p-Value comparing PTC and FTC.
DSS, disease-specific survival; DTC, differentiated thyroid cancer; FTC, follicular thyroid cancer; HCC, Hürthle cell carcinoma; OS, overall survival; PTC, papillary thyroid cancer
TNM stage
Using the eighth edition's original age cutoff, 2430 patients (79%) were classified as stage I, 384 (13%) as stage II, 88 (3%) as stage III, and 172 (6%) as stage IV. Lowering the age cutoff resulted in a lower number of patients in stage I; these patients were redistributed over the other three stages. Increasing the age cutoff resulted in a higher number of patients being classified as stage I and fewer patients as having higher stage disease (Table 2). This same pattern was also seen for PTC and FTC separately.
Distribution of Patients Across Stages, Employing Different Age Cutoffs in Addition to the Established Histopathological Staging Criteria of the Eighth Edition of the Tumor–Node–Metastasis System
Values are n (%).
Survival prediction
The 10-year DSS was significantly higher for PTC than FTC (p < 0.001). After adjusting for age, sex, and cohort, the difference between PTC and FTC remained significant (p < 0.001; Table 3). The 10-year DSS data per stage for DTC overall, and for PTC and FTC separately, are shown in Table 4.
Effect of the Differentiated Thyroid Cancer Histological Subtype on Survival
p-Value comparing FTC with PTC (PTC as the reference group).
Model I; unadjusted.
Model II; adjusted for age and sex.
Model III; adjusted for age, sex, and cohort.
CI, confidence interval; HR, hazard ratio.
Ten-Year Disease-Specific Survival for Differentiated Thyroid Cancer, Papillary Thyroid Cancer, and Follicular Thyroid Cancer, Employing Different Age Cutoffs in Addition to the Established Histopathological Staging Criteria of the Eighth Edition of the Tumor–Node–Metastasis System
For DTC, and PTC and FTC separately, the majority of the age cutoffs had a better statistical model performance than the model without any age cutoff (Fig. 1). Furthermore, using 5-year increments for age cutoffs, the highest C-index and lowest AIC and BIC values were identified for an age cutoff of 50 years for DTC overall as well as for PTC separately, while it was 40 years for FTC (Fig. 2). From the original age cutoff toward the best identified cutoffs, 3.7% (DTC), 3.4% (PTC), and 11.7% (FTC) of patients migrated to a higher stage (Fig. 3). Using 1-year increments, for DTC overall, the highest C-index was established with an age cutoff of 50 years (lowest AIC and BIC values at 46 years). For PTC, the highest C-index was identified at 48 years (lowest AIC and BIC values at 50 years), while for FTC, the highest C-index and lowest AIC and BIC values were all identified at 41 years (Supplementary Fig. S1). C-index and AIC and BIC values for patients from the University of Würzburg and the Erasmus MC separately are shown in Supplementary Figures S2, S3, and S4.
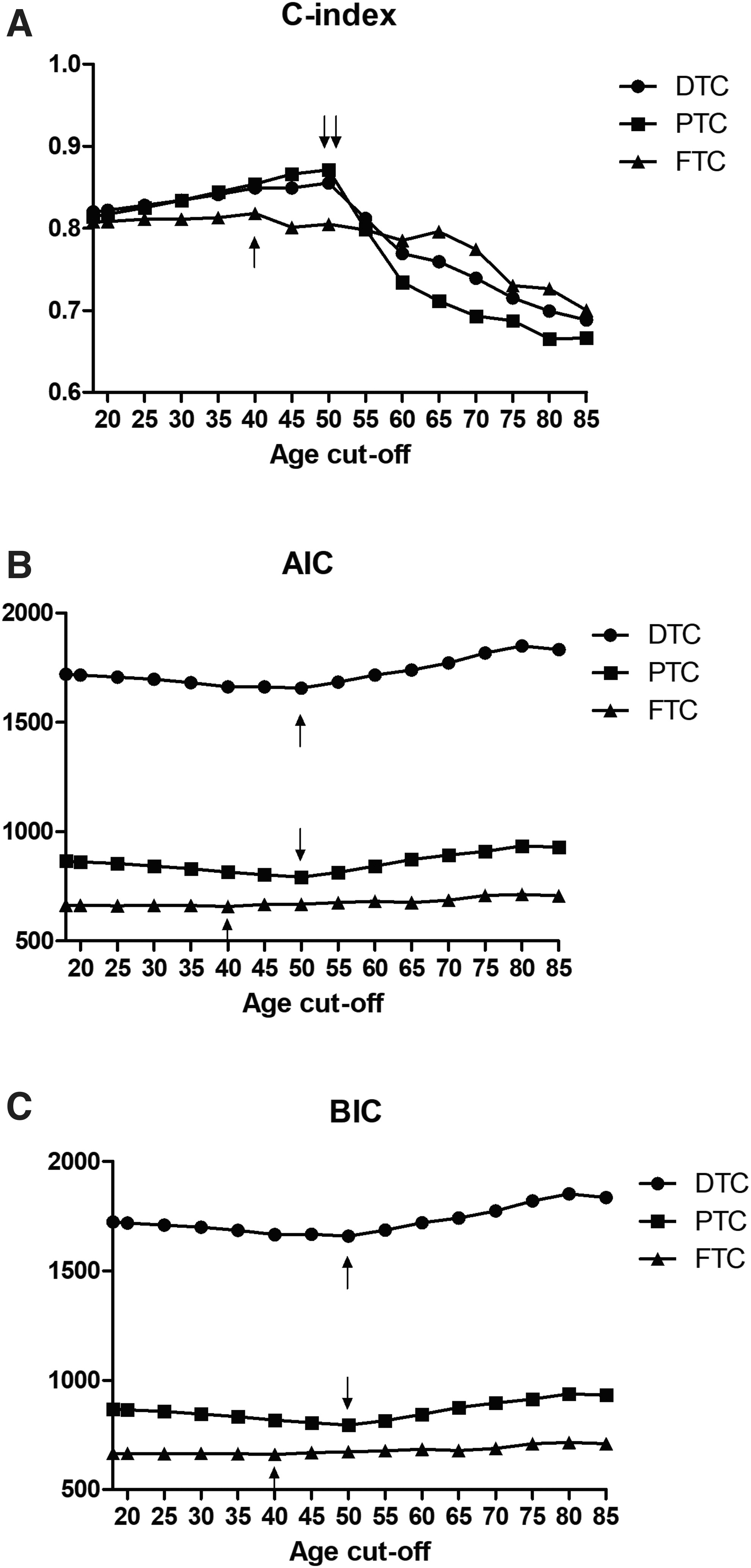
Statistical model performance for (
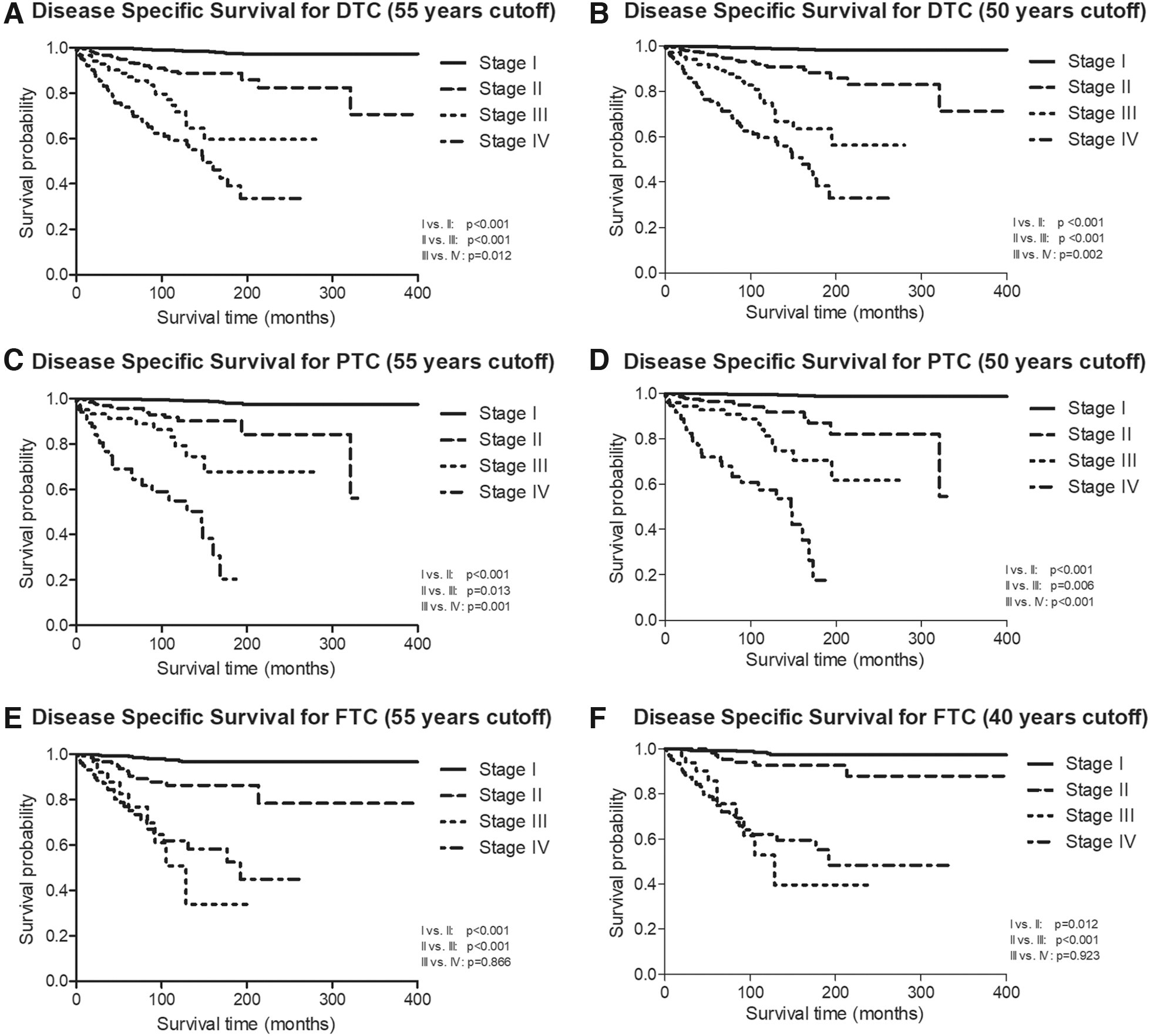
Kaplan–Meier curves for DSS in (
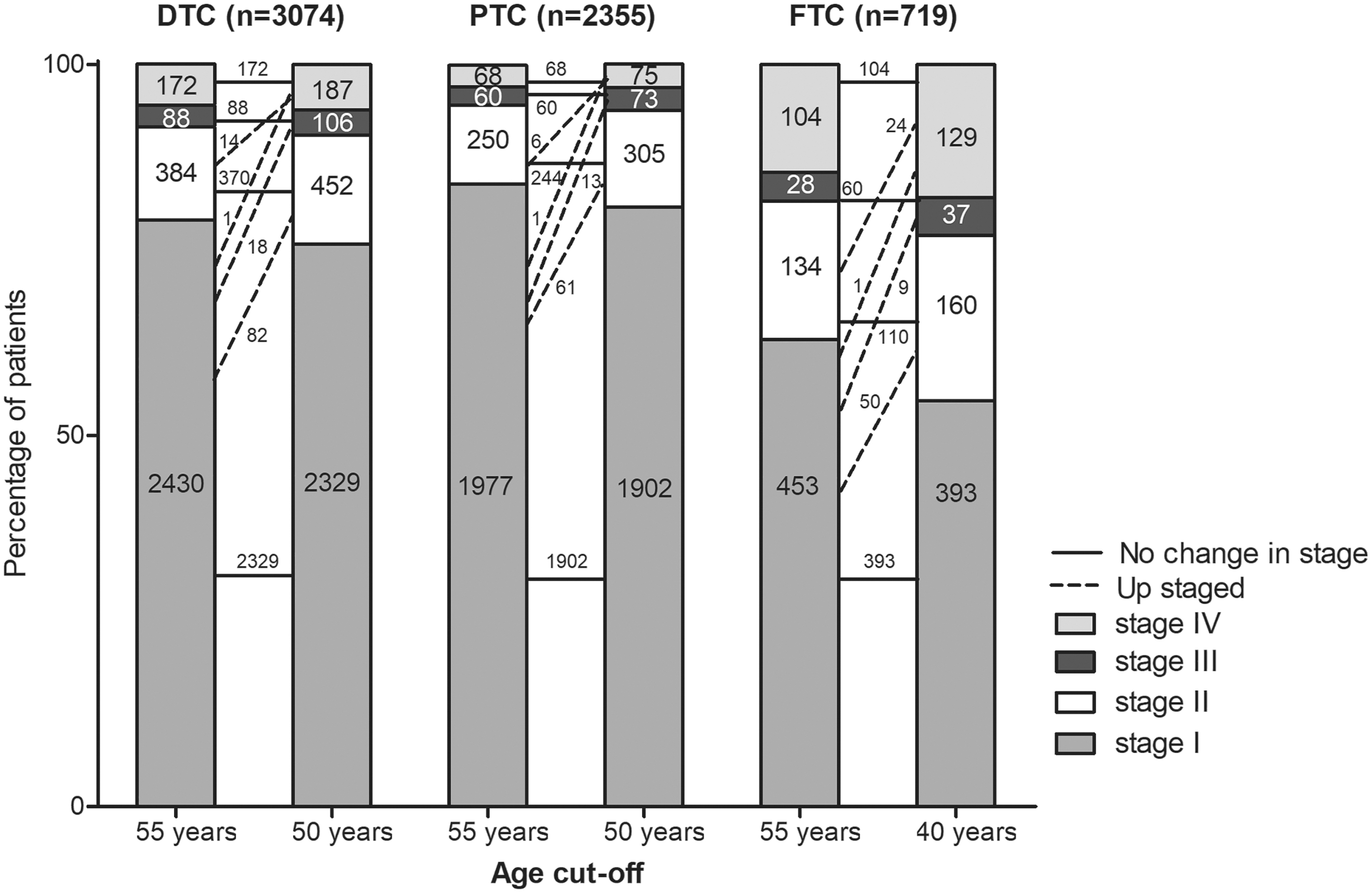
Distribution of patients per disease type and stage according to the original 55-year age cutoff and best identified age cutoffs for the TNM staging system. TNM, tumor–node–metastasis.
Using Cox proportional hazards models, unadjusted significant differences between PTC and FTC were seen for all age cutoffs, except for 65 and 70 years. Adjusting for age, sex, and cohort, there were significant differences between PTC and FTC for age cutoffs of 45, 50, 75, and 85 years (Supplementary Table S2).
Discussion
In the present study, combining two, large, well-described DTC patient cohorts from two different European countries, we showed that when employing the histopathological staging criteria from the eighth edition of the TNM system, the optimal age cutoff for classification of disease stage with respect to DSS is 50 years rather than the 55 years currently being used in the staging system. In addition, there was a 10-year difference in age cutoff for patients with PTC versus FTC.
Nixon et al. showed that when employing the histopathological criteria of the seventh edition of the TNM system in DTC patients from the United States, an age cutoff of 55 years outperformed the standard cutoff of 45 years (20). Later on, they confirmed this result in DTC patients from centers across the world, although no groups from Europe or Asia were included (21). Kim et al. also confirmed this result in DTC patients from Asia as the receiver operating characteristic analysis revealed an optimal cutoff of 55.4 years by employing the histopathological criteria of the seventh edition of the TNM system (22). Ito et al. compared the original seventh edition of the TNM system with a slightly different version in Japanese PTC patients. The different version also included a changed age cutoff of 55 years (34). They showed that their altered system performed better than the original seventh edition. Unfortunately, they did not investigate different age cutoffs. Except for the study by Kim et al., no other age cutoffs than 45 and 55 years were reported and therefore it is unknown if in these three studies, another age cutoff would have given an optimized result. Besides, these four studies employed the histopathological staging criteria of the seventh instead of the eighth TNM edition used in the current study.
There have been several studies that investigated the influence of age on prognosis without consideration of staging factors (35 –37). Based on these results, it was argued that an age cutoff does not do justice to the continuous effect age likely has on prognosis and that it should therefore be considered to remove a dichotomizing age criterion from the TNM staging system (38). In the present study, it was clearly shown that addition of an age-based cutoff increases the prognostic power of the TNM system as the majority of the age cutoffs significantly outperform a model based on histopathological criteria alone. However, this still does not necessarily imply that using a dichotomized age classification is optimal. Therefore, further research is needed to investigate whether there is a better method to incorporate age into the TNM staging system, for example, adjusting for relative survival rates (25,39), combining histopathological staging criteria with age (continuously or, e.g., per decade) in a risk calculator, or considering employing multiple age cutoffs. It is also important to focus not only on statistical performance but also on the feasibility of using this information in clinical practice.
Our results showed that for FTC, the optimal age cutoff was 41 years (40 years for 5-year increments). For PTC, the C-index showed 48 years (50 years for 5-year increments), while 50 years also was the optimal cutoff using the AIC or BIC. For DTC overall, the C-index showed 50 years, which is in agreement with the 5-year increment analysis, while 46 years was the optimal cutoff using the AIC or BIC—which is remarkably close to the cutoff of 45 years employed in previous iterations of the TNM system up to and including the seventh edition. Overall, as there were only minor differences between the one- and five-year increment analyses, it is more convenient to use a multiple of five in prognostic systems aimed for use in clinical practice. We feel that the results of the five-year increment analysis represent a good clinically (easily) usable compromise between minor differences of various statistical analyses.
To the best of our knowledge, the present study is the first one to investigate the optimal age cutoff specifically for patients with FTC. Compared with PTC, patients with FTC in our population were older and had more advanced disease in terms of both local disease and distant metastases, which is in accordance with literature (19). The DSS for stage III FTC patients is relatively low and its Kaplan–Meier curve overlaps the curve of stage IV patients (p = 0.923). This might be caused by older patients with T4 tumors with poor prognosis in this study. This phenomenon was also seen in our earlier study (9). Therefore, one might consider combining stage III and IV disease in patients with FTC into a single staging category, resulting in three instead of four stages for FTC. However, further research on this topic is needed.
Two earlier studies, in partially overlapping populations, compared PTC and FTC using either the seventh or eighth edition of the TNM system regarding prognosis and found no significant differences between the two histological subtypes (9,40). In the present study, these earlier results from both our centers cannot be confirmed in their entirety. When combining the two populations into a single large cohort, the optimal overall DTC cutoff of 50 years results in a survival difference between PTC and FTC in stage I. This is likely explained by the difference in optimal age cutoff observed between these two distinct histological entities in the present study, with a misclassification of a number of patients over 40 years with higher risk FTC erroneously classified as having stage I disease. Consequently, this results in an optimal age cutoff of 40 years for FTC, which is markedly different from the optimal age cutoff for PTC. As stated earlier, it is well established that FTC and PTC have different clinical manifestations (19), and our study further emphasizes this. Hence, the present study implies that PTC and FTC should be staged as separate entities.
In the present study, we included patients from two large university medical centers from Europe. With respect to the statistical model performance for FTC, both populations showed an optimal age cutoff of 40 years. For PTC, there was a minor discrepancy as for the Erasmus MC, the optimal age cutoff was 45 years, while it was 50 years for the University of Würzburg. However, when using the 1-year increment analysis, the difference between both populations was minor (only 3 years), that is, 47 years for the Erasmus MC and 50 years for the University of Würzburg. These differences might, in part, be attributable to differences in baseline characteristics at diagnosis as patients from the Erasmus MC more often had local and/or distant metastases and higher DTC-related mortality, which is possibly due to the fact that the Erasmus MC is a reference center for thyroid cancer in The Netherlands and therefore has a comparatively high proportion of patients with advanced disease. Combining populations with minor differences, but treating both in high-quality health care systems, may increase the robustness of results, resulting in a more generalizable conclusion. Additionally, because differences between the optimal age cutoffs were small, we consider our findings to be valid. Nonetheless, further research in populations from around the globe is needed to further confirm and/or refine our results.
The strengths of our study include the substantial proportion of patients with advanced disease stages compared with other studies as 9% of our patients had distant metastasis at presentation. Furthermore, the relatively high proportion (23%) of FTC patients enabled us to be, to our knowledge, the first to investigate the optimal age cutoff in patients with FTC and, additionally, compare PTC with FTC patients. A limitation of our study is the fact that it is retrospective and therefore patients were reclassified using the histopathological criteria from the eighth edition of the TNM system; it might be that in some cases, the reclassification differs from direct classification by a pathologist using the eighth edition's criteria. Additionally, it is possible that an unknown proportion of DTC patients would, in the current day, be classified otherwise. Unfortunately, the retrospective nature of our study leaves no way of ascertaining this. Therefore, longitudinal studies are needed to confirm our results. We used three statistical measures (C-index, AIC, and BIC) to be able to define the age cutoff that optimizes statistical performance. These three measures in the various analyses occasionally showed only minor discrepancies, allowing us to weigh the purely statistical analyses with pragmatic clinical considerations to balance various results.
In summary, the present study shows that in a large European population of patients with DTC harboring a large subset of FTC patients, the overall optimal age cutoff, employing the histopathological staging criteria of the eighth edition of the TNM system to predict DSS, is 50 years for patients with PTC, but not for patients with FTC where 40 years was the optimal cutoff. Therefore, our study implies that for an optimal estimate of prognosis, PTC and FTC should be staged as separate entities.
Footnotes
Author Contributions
E.V.V., F.A.V., and R.P.P. designed the current study. E.V.V., W.E.V., M.T.S., R.P.P., U.M., C.R., and F.A.V. created the original databases to collect clinical data. E.V.V. and M.T.S. conducted the statistical analyses and E.V.V. wrote the manuscript. All authors reviewed and revised the manuscript to improve its intellectual and technical content.
Author Disclosure Statement
F.A.V. has received consultancy fees from Sanofi, EISAI, and Jubilant DraxImage, as well as speaker honoraria from Sanofi and research support from EISAI. R.P.P. received teaching fees from Sanofi and Bayer. E.V.V., W.E.V., M.T.S., U.M., C.R., F.J.K., and T.V.G. declare no conflicts of interest, and no competing financial interests exist.
Funding Information
No funding was received for this article.
Supplementary Material
Supplementary Table S1
Supplementary Table S2
Supplementary Figure S1
Supplementary Figure S2
Supplementary Figure S3
Supplementary Figure S4