
Abstract
Background:
The use of prescribed medications during pregnancy is a challenge and an underestimated source of treatment burden. Levothyroxine (LT4) for the treatment of overt and subclinical hypothyroidism is extensively prescribed during pregnancy. To this end, we aimed to explore the patients' perceived benefits and risks, knowledge, beliefs, attitudes, and related burden of LT4 therapy during pregnancy.
Methods:
In this cross-sectional study, we surveyed pregnant women who were treated with LT4 during pregnancy from January 1, 2019, to December 31, 2019, in a tertiary academic medical center of the United States. The anonymous online survey included questions to gather demographic data and multiple-choice questions regarding the benefits and risks, knowledge, beliefs, attitudes, and burden related to LT4 use during pregnancy.
Results:
Sixty-four pregnant women (mean age 31.5 years) completed the study survey (response rate: 96%): 62% were diagnosed with hypothyroidism more than 12 months before pregnancy, 16% less than or about 12 months before pregnancy, and 22% during pregnancy. We found that one-third of pregnant women using LT4 had a feeling of uneasiness/anxiety due to their hypothyroidism diagnosis. About half of the respondents (45%) reported that they did not receive an explanation by their clinician regarding the maternal/fetal risks of uncontrolled hypothyroidism or the benefits of adequate control. Finally, two in three patients expressed various concerns of LT4-related treatment burden.
Conclusions:
Our findings support the need for increased effective communication and tailored counseling to address fears, anxiety, and uncertainties about the benefits and risks of LT4 use in pregnancy. For patients with clear benefits from LT4 treatment in pregnancy, it could help to overcome their concerns, promote adherence, and decrease adverse maternal/fetal outcomes. For patients with no clear benefits established, clinicians need to be aware of LT4-related treatment burden in pregnancy and implement patient-centered approaches in their clinical practices.
Introduction
Prescribing medications during pregnancy is a challenge due to possible alterations in their metabolism and the potential of causing harm to the fetus and the mother (1 –4). Therefore, adequate counseling and consideration of the indication, benefits, and risks of any medication for pregnant women are highly important.
Accordingly, there is general hesitation toward medication use during pregnancy among women. Furthermore, the beliefs about prescription medications result in decreased treatment adherence, and potentially, worse treatment outcomes (5 –7). According to the Beliefs about Medicines Questionnaire (BMQ), users of prescription medications with high adherence have shown more positive and less negative beliefs about medicines than nonadherent users (6). Indeed, patients who reported more negative beliefs about medications had 2.1 times greater odds (95% confidence interval [CI 1.3–3.7]) of low medication adherence compared with patients with less negative beliefs (5).
Levothyroxine (LT4) is the recommended prescription medication for hypothyroidism during pregnancy (8). Hypothyroidism is a relatively common disorder during pregnancy; overt hypothyroidism (OH) is present in 0.2–0.5% of pregnant women (9), while subclinical hypothyroidism (SCH) prevalence ranges from 1.5% to 42.9% depending on the thyrotropin (TSH) cutoff level used for diagnosis, geographic region, and ethnicity (10). OH during pregnancy is a well-known risk factor for several maternal/fetal complications and offspring detriments; thus, treatment with LT4 is strongly recommended (9,11 –14). Multiple studies have also reported an association of SCH during pregnancy with an increased risk for adverse pregnancy and neonatal outcomes (15 –18). Although two large clinical trials did not show a benefit of LT4 therapy in cognitive function of children of pregnant women with SCH (19,20), other studies have found that it can decrease the risk for miscarriage (21) and preterm delivery (22,23). Current clinical practice guidelines (19,20) place a high value on accruing any potential benefit of LT4 therapy, while its use is seen as low risk of treatment burden. However, although rare, adverse effects related to thyroid hormone replacement could themselves negatively impact the health of the pregnant woman and her offspring (24).
Despite the extensive use of LT4 during pregnancy, the knowledge, attitudes, and health beliefs of pregnant women about hypothyroidism and its treatment burden have not been investigated. To this end, we aimed to explore the perceived benefits and risks, knowledge, beliefs, attitudes, and the related burden of the LT4 therapy during pregnancy.
Materials and Methods
Setting and participants
In this cross-sectional study, we surveyed pregnant women recruited from two Obstetrics clinics (one mainly serving the Medicaid population and the other mostly serving the privately insured sector) and the Endocrinology clinic (9% of study sample, serving a mixed Medicare, Medicaid, and privately insured population) of the University of Arkansas for Medical Sciences. These clinics were selected due to the highest average number of LT4-treated pregnant women visits within three months before study initiation (five visits/week). We consecutively included adult pregnant women who were treated with LT4 for hypothyroidism during pregnancy from January 1, 2019, to December 31, 2019. Women unable to read/understand English written material were excluded. Potential participants were found either through schedule screening or clinic referrals. This study was approved by the local Institutional Review Board.
Study survey
Two authors (S.M. and F.J.K.T.) prepared an initial draft of the survey according to the study objectives and adaptations of previously standardized survey tools to assess the thyroid-related quality of life (Thyroid-specific Patient-Reported Outcome short-form; ThyPRO 39) and beliefs about medicines (BMQ-specific) (25,26). Subsequent survey drafts were distributed among the coauthors, and after an iterative process of feedback and discussion, a final version was prepared (Supplementary Data S1). The survey consisted of 24 questions, including demographic data and multiple-choice questions regarding the knowledge, attitudes, beliefs, current feelings regarding having hypothyroidism, and treatment burden related to LT4 use during pregnancy. Supplementary Table S1 summarizes the survey questions used to assess the study outcomes. We adopted the definition of treatment burden described by Boyd et al.: “the patient's perception of the aggregate weight of the actions and resources they devote to their healthcare, including difficulty, time, and out-of-pocket costs dedicated to the healthcare tasks such as adhering to medications, dietary recommendations, and self-monitoring” (27). We used the Brief Screening Questions for Health Literacy, a validated tool, to assess the health literacy among survey respondents (28,29). This tool contains three questions and the responses are expressed on a five-point Likert scale (1—Never, 2—Occasionally, 3—Sometimes, 4—Often, and 5—Always). Any response that is ≥3 on any question indicates inadequate health literacy. We limited questions to achieve a survey response time of <10 minutes. Survey responses were anonymously collected and stored electronically (Google forms, Mountain View, CA), and data were password-protected. No personally identifiable information was collected.
Study procedures and data collection
A study team member approached potential participants to explain the study. After patient agreement to participate in the study, verbal informed consent was obtained. After the first three participants completed the survey, we followed cognitive debriefing procedures (30). As per participants' suggestion, we started providing educational materials related to hypothyroidism in pregnancy after survey completion.
Statistical analysis
Summary statistics are presented as frequencies (percentages) for the categorical variables and as mean and standard deviation (SD) for continuous variables. Differences in categorical variables were analyzed with chi-square or Fisher's exact test and for continuous variables with the independent t-test or Mann–Whitney test, as appropriate. Two multivariable logistic regression models were performed. Model 1 assessed the possible drivers for the feeling of current anxiety due to hypothyroidism after adjusting for age, educational level, marital status, self-reported lack of previous explanation of the hypothyroidism diagnosis by a clinician, and being in the first pregnancy. Model 2 assessed the possible drivers for the perceived hardness to take LT4 during pregnancy after adjusting for age, race, educational level, being in the first pregnancy, and marital status. All analyses were two-tailed with alpha set at 0.05 and conducted using IBM SPSS Statistics version 25.
Results
Demographics of responders
Seventy-two patients were eligible for the study. Five were excluded due to the inability to read/understand English written material. Of the 67 pregnant women invited to participate in the study, 64 completed the survey (96% response rate) and 3 declined participation. The demographic characteristics of the responders are summarized in Table 1. Responders' average age was 31.5 (SD 6.2) years and one-fourth were in their first pregnancy. The majority of women were white (56%). Participants had a wide range of educational levels. The majority of women indicated that they never need any help reading materials from their doctor's office or hospital (66%), 55% were very/fairly confident filling out medical forms by themselves correctly, and 46% never had issues learning about their health problems because it was hard to understand written information. Participants showed fair health literacy, with 39% describing any degree of inadequate health literacy.
Demographic Characteristics of Survey Respondents
GED, General Educational Development.
History of thyroid disease and current status
Among the respondents, 62% were diagnosed with hypothyroidism (OH or SCH) >12 months before pregnancy, 16% ≤ 12 months before pregnancy, and 22% during current pregnancy. Regarding thyroid function tests (TFTs) and current health status, women reported the following: 66% TFTs were controlled and were feeling well; 6% TFTs were under control, but they were not feeling well; 6% TFTs were uncontrolled, but they were feeling well; 2% TFTs were uncontrolled and they were not feeling well; and 20% did not know the current TFT status. The majority of women (97%) reported excellent treatment adherence taking LT4 daily.
Having hypothyroidism caused women to feel uneasy or anxious (34%), sad (11%), afraid (8%), and angry (2%) (Fig. 1). Women with a diagnosis during current pregnancy were more likely to feel anxious (57%) due to their hypothyroidism compared with those with a diagnosis before pregnancy (28%) (p = 0.04). In a multivariable analysis adjusting for age, educational level, and marital status, the feeling of anxiety was significantly predicted by the self-reported lack of previous explanation of the hypothyroidism diagnosis by a clinician (odds ratio [OR] = 1.32, [CI 1.05–1.87]) and being in the first pregnancy (OR = 1.36, [CI 1.02–2.11]).
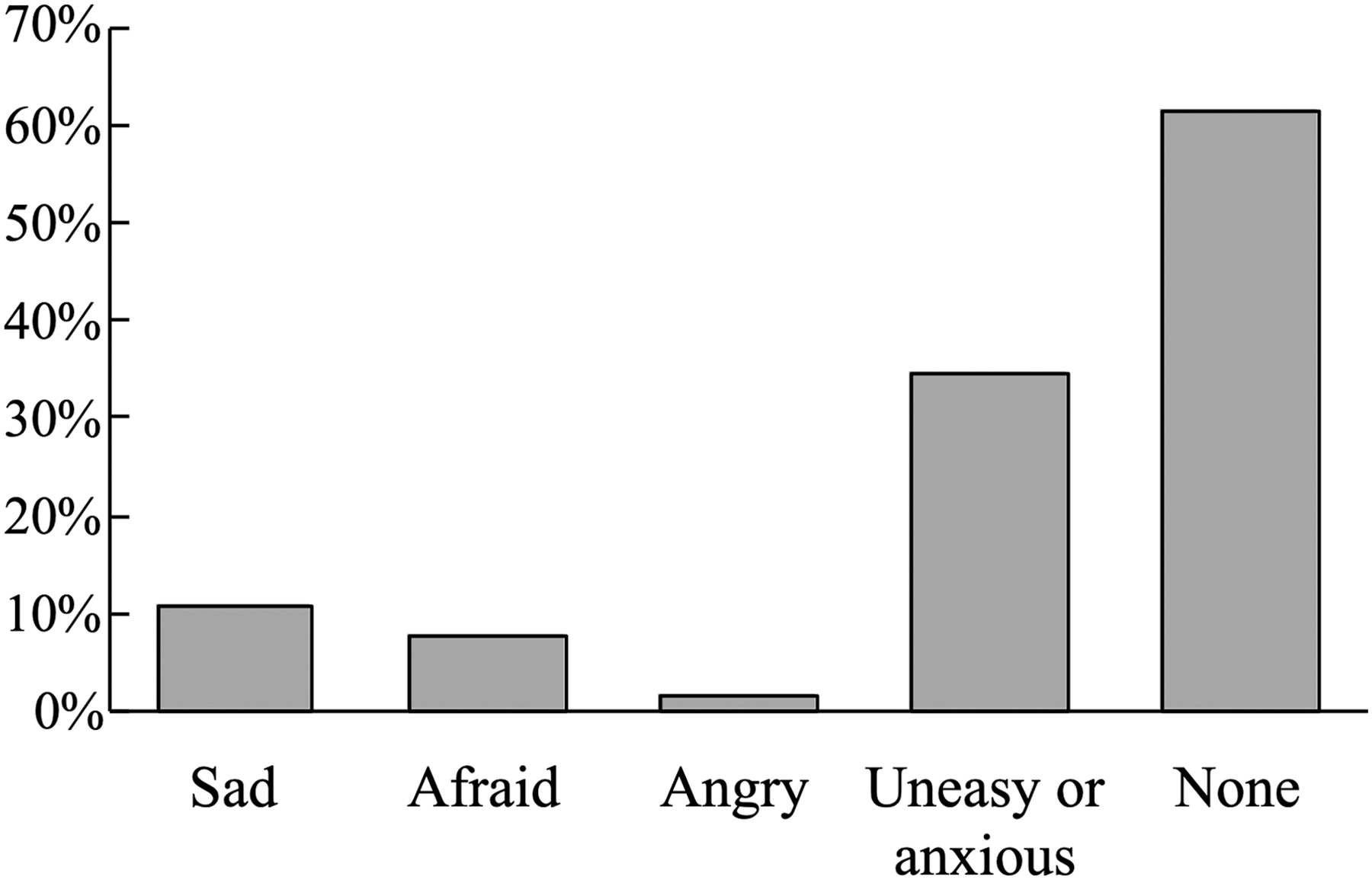
Reported current feelings regarding having a thyroid disorder during pregnancy.
Knowledge and perceptions—hypothyroidism during pregnancy
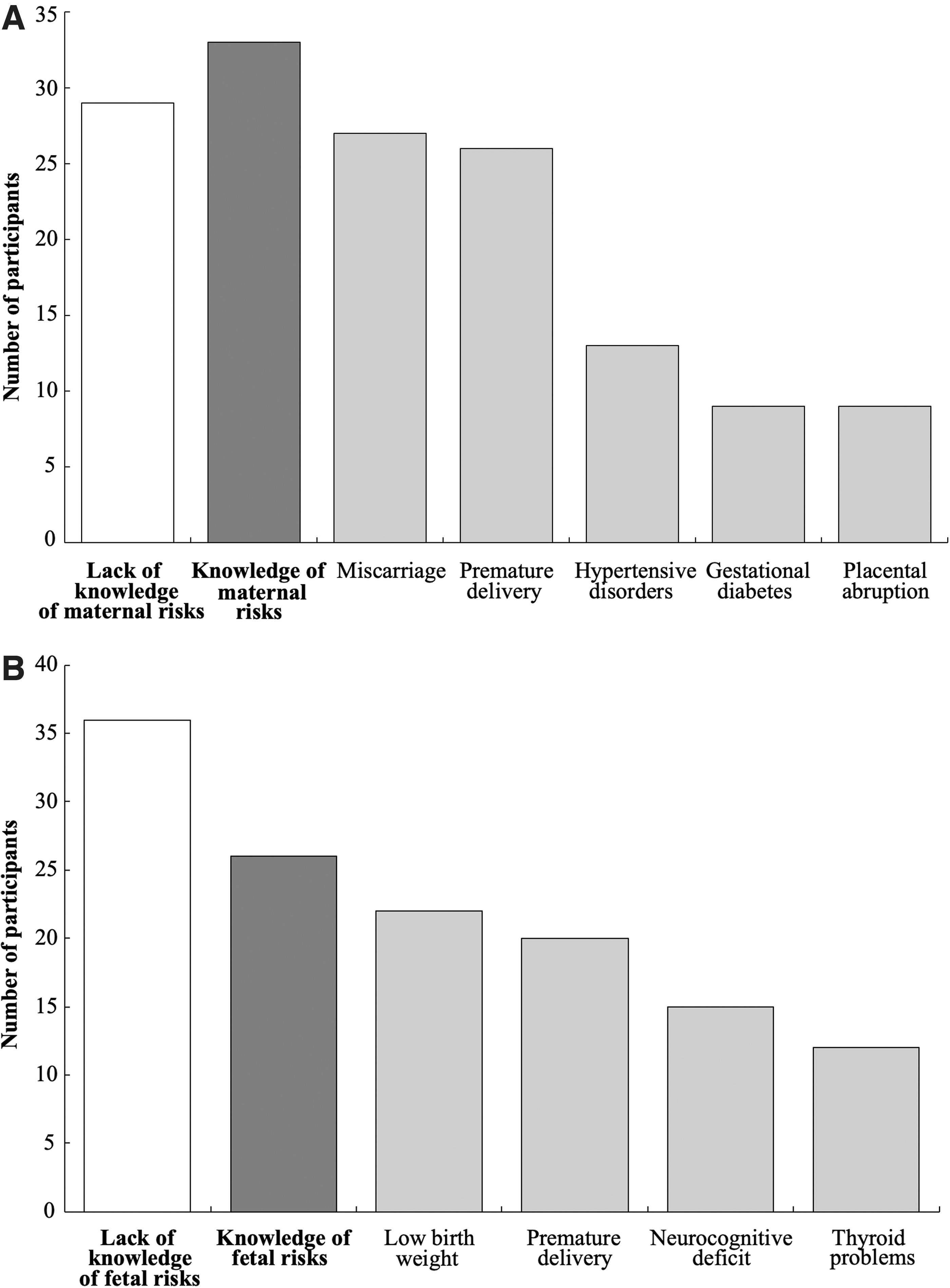
The majority of women reported receiving an explanation of the general meaning of having hypothyroidism (86%). Women with a diagnosis during current pregnancy (22%) were less likely to report receiving such an explanation compared with those with a diagnosis before pregnancy (78%) (p = 0.002). In addition, 45% of the participants did not recall having received an explanation by their clinician regarding the maternal/fetal risks of uncontrolled hypothyroidism during pregnancy or the benefits of adequate control. Roughly half of the responders (53%) described knowing the maternal risks associated with uncontrolled hypothyroidism during pregnancy. The most cited risks were as follows: miscarriage (82%), premature delivery (79%), hypertensive disorders (39%), gestational diabetes (27%), and placental abruption (27%) (Fig. 2A). Only 42% of the participants reported knowing any neonatal or offspring risks due to uncontrolled hypothyroidism during pregnancy. The most cited risks were low birth weight (85%), premature delivery (77%), neurocognitive deficit (58%), and thyroid problems (46%) (Fig. 2B).
Patients with inadequate health literacy were more likely not to know the risk of maternal/fetal (63%, p = 0.049) or offspring (75%, p = 0.032) complications due to uncontrolled hypothyroidism during pregnancy compared with those with adequate health literacy (37% and 47%, respectively). Pregnant women with a diagnosis of hypothyroidism during current pregnancy were more likely not to know the risk of offspring (85%, p = 0.017) complications due to uncontrolled hypothyroidism during pregnancy compared with those diagnosed before pregnancy (50%).
Knowledge and perceptions—LT4 use
LT4 use during pregnancy was described as completely safe (54%) or mostly safe (32%), and only 14% of women did not know the safety of LT4 use during pregnancy. Two-thirds of the participants (67%) considered that taking LT4 during pregnancy is more important than before pregnancy, and 33% considered that it is as important as before. The main perceived benefits of taking LT4 during pregnancy included decreased offspring risks (95%), decreased maternal risks (80%), improved symptoms (67%), and controlled TFTs (47%) (Fig. 3A).
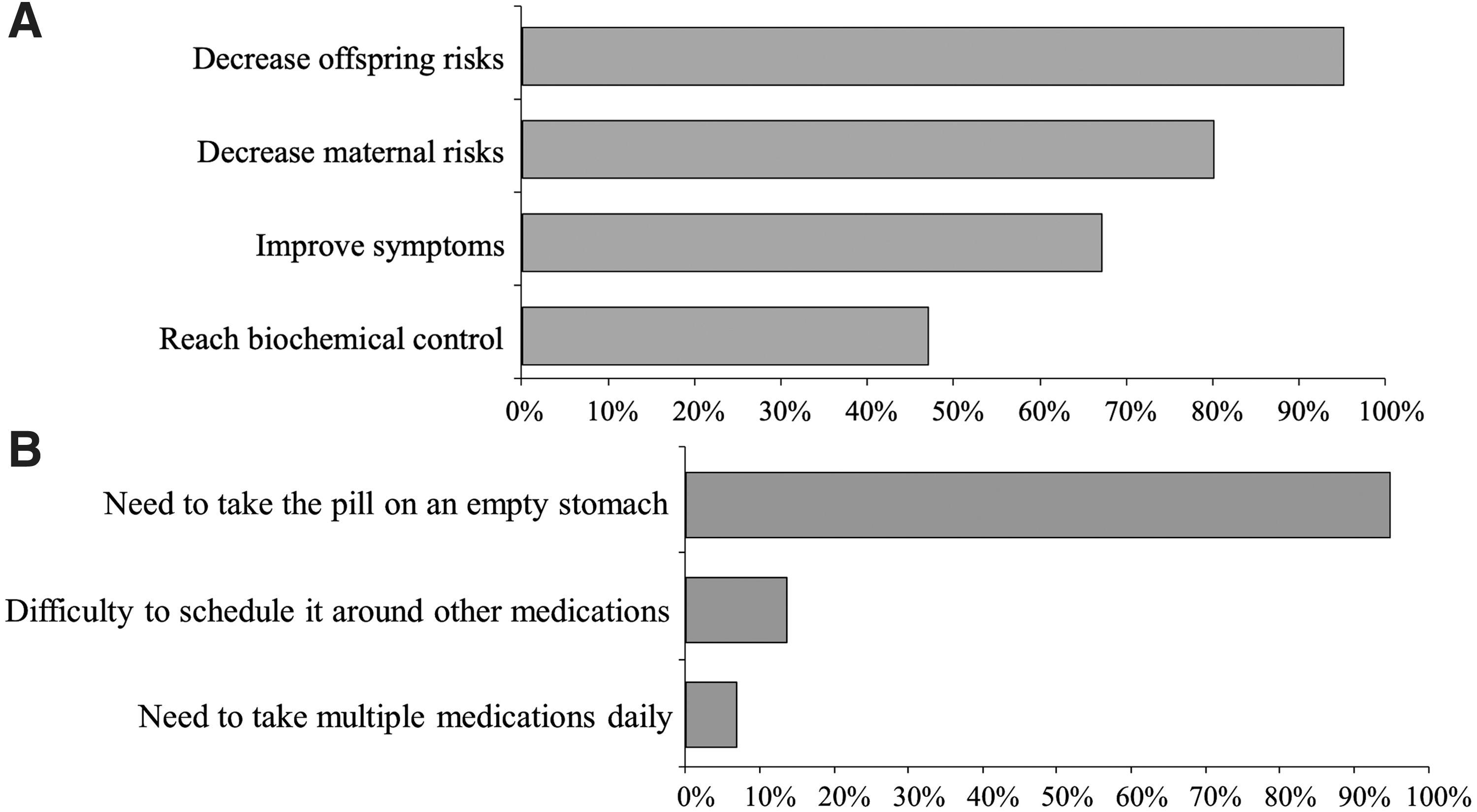
Treatment burden—LT4 use
Approximately one in four pregnant women considered that taking LT4 during pregnancy is hard. The main reasons of reporting treatment burden were as follows: need to take LT4 on an empty stomach (93%), difficulty to schedule it around other medications (13%), and need to take multiple medications daily (7%) (Fig. 3B). Among participants, 52% strongly agreed or agreed that they sometimes worry about the long-term effects of using LT4, 27% agreed that taking LT4 worries them, 25% agreed that taking LT4 makes their life harder, and 22% agreed that they sometimes worry about the financial problems caused by hypothyroidism and its treatment (Fig. 4). Among participants, 67% expressed at least one concern related to treatment burden due to LT4 use during pregnancy: hardness or worry of taking LT4, concern of its long-terms side effects, and associated financial problems.
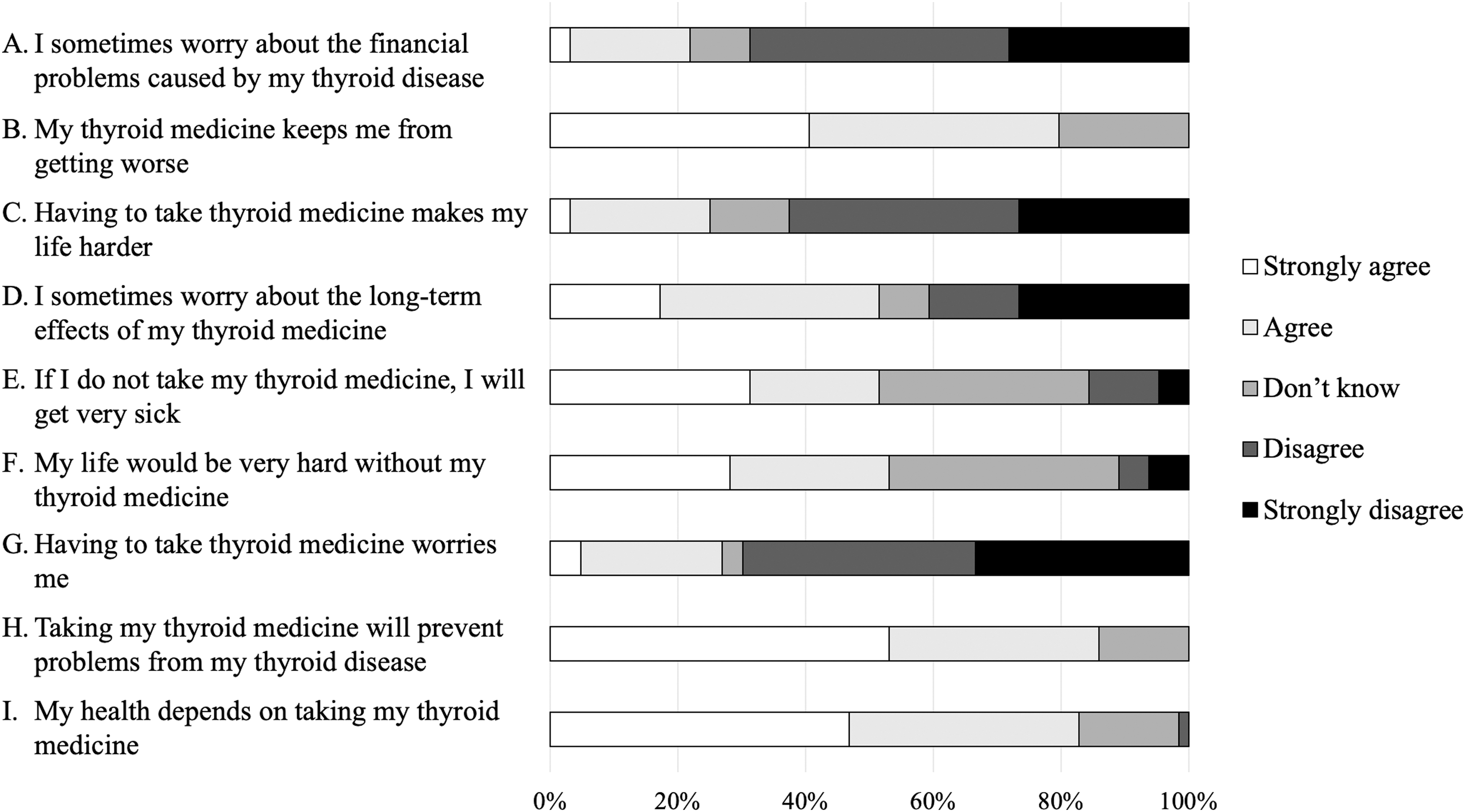
Participants' agreement level with statements related to the treatment burden of using LT4 during pregnancy.
In a multivariable analysis, age was the only significant predictor of the perceived hardness of taking LT4 during pregnancy (OR = 1.31, [CI 1.05–1.65]) after adjusting for race, educational level, being in the first pregnancy, and marital status.
Beliefs and attitudes related to LT4 use during pregnancy
The majority of women strongly agreed or agreed that their health depends on taking LT4 (82%), taking LT4 will prevent future hypothyroidism-related problems (86%), and LT4 use keeps them from getting worse (80%). Roughly half of the responders agreed that their life would be very hard without LT4 (53%) and that they will get sick without taking LT4 (52%). Figure 4 shows a summary of the participants' agreement levels with these statements.
Discussion
We found that one-third of pregnant women using LT4 had a feeling of uneasiness/anxiety due to their hypothyroidism diagnosis. This feeling was more frequent in women during first pregnancy, and it was predicted by the self-reported lack of a previous explanation of the hypothyroidism diagnosis and its implications by a clinician. Our results show some degree of ineffective clinician–patient communication, as roughly half of the responders did not recall receiving an explanation regarding the maternal/fetal risks of uncontrolled hypothyroidism during pregnancy or the benefits of adequate control. In addition, we found significant LT4-related treatment burden, since two in three patients expressed various concerns of treatment burden during pregnancy.
LT4 treatment of OH is strongly recommended due to its undoubted benefits in maternal/fetal and offspring outcomes (8,31 –33). Similarly, due to multiple studies showing LT4 benefit for pregnant women with SCH (21 –23,34,35), guidelines (8,31) advocate for obtaining any potential benefit of LT4 therapy in women with SCH, while considering low the risk for treatment burden, anxiety, or any possible adverse effects of thyroid hormone replacement. In fact, we recently showed that only 19% of clinicians consider therapy adverse effects when they prescribe LT4 for SCH in pregnancy, while only half take patient preferences into account when determining therapy (36). However, we found that LT4-related treatment burden and anxiety are frequent issues among pregnant women and should not be disregarded during the decision-making for LT4 use, particularly in pregnant women for whom there is no clear treatment benefit established, such as pregnant women with TSH level between 2.5 mIU/L and upper limit of normal (21) or euthyroid women with thyroid autoimmunity (37).
Pregnancy is a significant source of anxiety among women and their partners, which may increase considerably with the occurrence of maternal/fetal complications and prescription of new medications. Kannenberg et al. found that concerns for offspring's disease constituted the greatest source of anxiety for pregnant women (38). Similarly, Nyholm et al. (39) found that pregnant women perceived the use of medicines as less trustworthy in pregnancy. The majority of these women worried about taking medicines during pregnancy due to unknown long-term adverse effents on offspring (39). Accordingly, having hypothyroidism during pregnancy was an important source of anxiety among our participants, probably due to the reported uncertainty regarding the maternal/fetal risks and potential adverse effects of LT4 use during pregnancy. Therefore, ensuring adequate patient education and excellent clinician–patient communication could mitigate the anxiety of hypothyroid pregnant women on LT4 therapy.
Effective clinician–patient communication has been cited as a decisive factor for decreasing medication-related anxiety, alleviating unclear perceptions of maternal/fetal risks among pregnant women, and improving treatment adherence during pregnancy (39 –42). Nyholm et al.'s study also reported that when concerns/anxiety about medicines arose during pregnancy, pregnant women appreciated being able to gather information from their clinician; even a brief conversation made some participants feel more relaxed, especially during the first trimester (39). Adherence to prescribed medications during pregnancy is affected by the state of disease, type of therapy, expected side effects, uncertainty of benefit, and perceived risk of adverse outcomes in the offspring (41,43 –45). Therefore, how clinicians communicate the need for one medication influences the attitudes toward medication adherence in pregnant women (44). Shanmugalingam et al. performed a mixed-methods study to understand the factors, from the women's perspective, that influenced adherence with prophylactic aspirin during pregnancy (42). They reported that consistently adequate communication and good relationship between pregnant women and their clinicians positively impacted the uptake of aspirin, and repeated re-enforcement on adherence with aspirin by clinicians emphasized its importance. Our results add to the evidence regarding the potential inadequate clinician–patient communication during pregnancy and shed light on the existence of this issue in the specific context of hypothyroidism.
Although several studies describe that overall pregnant women perceive as beneficial the use of prescribed medicines during pregnancy, they often cite concerns about the potential side effects of using these medications long term (7,46 –48). However, there is a lack of studies directly assessing the treatment burden of LT4, or other prescribed medications, during pregnancy. Shanmugalingam et al. found that pregnant women were on 3.5 (range 2–6) medications at any point in pregnancy, and of the women with <90% treatment adherence, 74% reported pill burden as an issue (42). In addition, restrictions around administration (e.g., take on empty stomach) are commonly cited contributing factors of treatment burden and low adherence (42,49). In line with this evidence, we found that many women described that taking LT4 during pregnancy is hard or cited various concerns of LT4-related burden. Further research is needed to examine if effective patient education and patient–clinician communication could potentially attenuate the LT4-treatment burden in pregnant women with hypothyroidism.
To our knowledge, this is the first study analyzing the perceived benefits and risks, knowledge, beliefs, attitudes, and the LT4-related burden during pregnancy. Moreover, the high response rate and the recruitment of a diverse sample of the population (variation in education and socioeconomic background) provide important insights into our study's aims. However, a few study limitations should be considered. This is a single-center, cross-sectional study conducted in a relatively small population of pregnant women, and due to the nature of its design, it is not possible to establish causal conclusions. In addition, the lack of data regarding the type of hypothyroidism diagnosis (OH vs. SCH) limits our ability to perform comparative analysis between these subgroups. As the current hypothyroidism status was self-reported, the reporting of some results depended on the women's awareness of their medical condition. Furthermore, although our survey questions stem from validated tools to assess thyroid-related quality of life and beliefs about medicines, this survey has not been validated. Moreover, the use of electronic surveys carries a risk of recall bias and selection bias toward a population with higher literacy, and patients' responses may have been subject to reporting bias. Finally, the generalizability of our findings may need to be established among pregnant women in other parts of the world.
In summary, we described the authentic account of a subgroup of pregnant women reporting LT4-related treatment burden during pregnancy. In addition, our findings indicate the need for increased communication and tailored counseling to address fears, anxiety, and uncertainties about the benefits and risks of LT4 use in pregnancy. For patients with clear benefit from LT4 treatment in pregnancy, it could help to overcome these concerns, promote adherence, and decrease adverse maternal/fetal outcomes. For patients with unclear benefits established from LT4 treatment, our findings highlight the need for clinicians to be aware of LT4-related treatment burden in pregnancy and to implement patient-centered approaches in their clinical practices.
Footnotes
Acknowledgments
Data necessary for the conception of this study were provided by the Arkansas Clinical Data Repository (AR-CDR) and maintained by the Department of Biomedical Informatics in the College of Medicine at the University of Arkansas for Medical Sciences. This material is the result of work supported with resources and the use of facilities at the Central Arkansas Veterans Healthcare System, Little Rock, AR. The contents do not represent the views of the U.S. Department of Veterans Affairs or the U.S. Government.
Authors' Contributions
S.M. and F.J.K.T. conceived and designed the study with input from all the coauthors. F.J.K.T., S.E.T., S.N., B.K., S.M.J., E.A., and N.K.D. helped recruit participants. F.J.K.T. carried out data collection and statistical analysis with input from S.M. All coauthors contributed to the critical appraisal and review of the survey questionnaire and the article. All authors reviewed and agreed on the final version of the article.
Disclaimer
The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
Dr. S.M. receives support from the Arkansas Biosciences Institute, the major research component of the Arkansas Tobacco Settlement Proceeds Act of 2000. Dr. N.M.S.O. was supported by the National Cancer Institute of the National Institutes of Health under Award Number K08CA248972.
Supplementary Material
Supplementary Data S1
Supplementary Table S1