
Abstract
Background:
The American Thyroid Association (ATA) published the 2015 Management Guidelines for patients with thyroid nodules and differentiated thyroid cancer, recommending a shift to less aggressive diagnostic, surgical, and postoperative treatment strategies. At the same time and perhaps related to the new guidelines, there has been a shift to outpatient thyroid surgery. The aim of the current study was to assess physician adherence to these recommendations by identifying and quantifying temporal trends in the rates and indications for thyroid procedures in the inpatient and outpatient settings.
Methods:
Using the IBM® MarketScan® Commercial database, we identified employer-insured patients in the United States who underwent outpatient and inpatient thyroid surgery from 2007 to 2018. Thyroid surgery was classified as total thyroidectomy (TT), thyroid lobectomy (TL), or a completion thyroidectomy. The surgical indication diagnosis was also determined and classified as either benign or malignant thyroid disease. We compared outpatient and inpatient trends in surgery between benign and malignant thyroid disease both before and after the release of the 2015 ATA guidelines.
Results:
A total of 220,088 patients who underwent thyroid surgery were included in the analysis. Approximately 80% of TLs were performed in the outpatient setting versus 70% of TTs. Longitudinal analysis showed a statistically significant changepoint for TT proportion occurring in November 2015. The proportion of TT as compared with TL decreased from 80% in September 2015 to 39% by December 2018. For thyroid cancer, there is an increasing trend in performing TL over TT, increasing from 17% in 2015 to 28% by the end of 2018.
Conclusions:
There was a significant changepoint occurring in November 2015 in the operative and management trends for benign and malignant thyroid disease.
Introduction
The incidence of thyroid cancer (TC) has increased >300% over the past four decades, and U.S. prevalence exceeds 700,000 patients (1). This rising incidence is concomitant with an increased identification of small, indolent, low-risk papillary thyroid carcinomas that are not associated with significant effects on patient survival (2,3). In the United States, the majority of patients with low-risk, differentiated thyroid cancer (DTC) are treated operatively. Most studies have shown that treating low-risk DTCs with total thyroidectomy (TT) does not result in improved outcomes compared with thyroid lobectomy (TL) (4,5). Moreover, risks of surgical complications and the need for thyroid hormone are less for patients undergoing TL (6).
The American Thyroid Association (ATA) released guidelines in October 2015, supporting the use of less aggressive patient management strategies for adult patients with thyroid nodules and DTC (7). Based on the similar outcomes for patients with follicular-cell derived TC between 1.0 and 4.0 cm who are treated by TL or TT, the 2015 ATA guidelines recommended TL as a reasonable option for these patients. In addition, the 2015 ATA guidelines included recommendations that performing thyroid surgery in the outpatient setting was an option based on increasing evidence that outpatient thyroid surgery is safe (8,9).
Nonadherence to guidelines is associated with worse survival (10). Although patient clinical and pathological factors have been cited, racial disparities, physician experience, and quality of data may be associated with nonadherence to guideline-concordant care (10,11). Prior studies using clinical databases focus on the cancer population or inpatient cohorts alone (4,12,13). Research also shows that thyroid procedures are increasingly being performed in the outpatient setting (14,15), for safety and cost reasons (16,17).
Our aim was to assess physician adherence to the 2015 ATA guidelines by using a nationwide and employment-based medical claims dataset that captures insurance claims from both the inpatient and outpatient settings. We used this fully adjudicated database to examine trends in thyroid surgery, explore the characteristics of patients undergoing surgery from 2007 to 2018, and assess the adherence to the 2015 ATA guidelines on surgical management of thyroid disease.
Materials and Methods
Data source
The IBM® MarketScan® Commercial Database (MarketScan) is a nationwide and employment-based convenience sample of medical claims data from more than 350 payers. The database contains more than 20 billion insurance claims from large employers, health plans, and government and public organizations. These service records capture person-specific clinical utilization, expenditures, and enrollment across inpatient, outpatient, prescription drug, and carve-out services. MarketScan data links paid claims and encounter data to detailed patient information longitudinally and across sites and types of providers from both the inpatient and outpatient settings. It contains data from active employees, early retirees, individuals with continuation of health coverage from Consolidated Omnibus Budget Reconciliation Act (COBRA), and dependents insured by employer-sponsored plans.
Study population
From MarketScan we obtained medical claims data from 2007 to 2018 for active employees and dependents, early (non-Medicare) retirees, and COBRA continuees younger than 65 years old with a diagnosis of a goiter or thyroid nodule and without a previous diagnosis of thyroid malignancy or thyroid procedure.
Current procedural terminology (CPT) and International Classification of Disease (ICD-9 and ICD-10) codes for initial diagnosis leading to workup and potential surgery were used as follows: thyroid nodule, goiter (simple), goiter (unspecified), nontoxic uninodular goiter, nontoxic multinodular goiter, and unspecified/other nontoxic nodular goiter (Supplementary Table S1). TT, TL, and completion thyroidectomy trends were obtained by using CPT and ICD procedural codes (Supplementary Table S2). Subtotal thyroidectomies were classified as TLs. Patients with two or more claims for thyroid surgery within 6 months were classified as having a lobectomy and a subsequent completion thyroidectomy. The frequency of procedures by operative diagnosis was determined by using CPT and ICD codes (Supplementary Table S3). Only the primary diagnosis code listed on the surgery claim was used. If the patient did not have an operative diagnosis classified as “malignant,” “hyperthyroidism,” or “uncertain,” at the time of surgery, they were assumed to have a “benign” operative diagnosis. Given the longitudinal nature of our data query, all rates from 2007 to 2018 are expressed as a proportion of the total sample for that year or month to control for the decreasing total annual number of patients undergoing thyroid surgery.
Covariables
Patient-level characteristics at the time of surgery were collected, including demographics, comorbidities, insurance plan type, and geographical region of residence as delineated by MarketScan. Comorbidities were defined by using the Agency for Healthcare Research and Quality (AHRQ) formulation for the weighted Elixhauser Index (18). The explanatory variables for the inpatient and outpatient models were: age, sex (female, male), indication diagnosis (“benign,” “hyperthyroidism,” “uncertain,” “malignant”), Elixhauser index (0, 1–4, 5 or greater), and insurance type, which include Health Maintenance Organization (HMO), Preferred Provider Organization (PPO), Point-of-Service (POS), Exclusive Provider Organization, and Comprehensive plans.
Statistical analysis
Descriptive statistics were generated as median and interquartile range for continuous variables, and frequency and proportion for categorical variables. To account for the skewed distributions of the explanatory variables, a generalized linear regression model approach was used to determine the significant predictors of receiving a TL versus TT. Models were created for each setting, inpatient and outpatient, by using the candidate explanatory variables that were selected based on a priori statistical significance (p < 0.001) from the univariate model. A stay was considered an inpatient stay if it followed certain criteria defined by MarketScan. MarketScan differentiates an inpatient stay from an outpatient stay by whether a room and board charge was incurred. If the 23-hour admission claim did not include fees for room and board, it would be classified as an outpatient stay.
Pettitt's test, a non-parametric method for single changepoint analysis in continuous time-series data, was performed to detect whether there was a statistically significant changepoint in the thyroid surgical management trends from January 2007 to December 2018 (19). A two-tailed Pettitt's test was used to evaluate the null hypothesis of no changepoint in thyroid surgery trend with the alternative hypothesis that there exists a certain date at which a changepoint can be detected.
All statistical analyses were performed by using R versions 3.6.3 and 4.0.0 (R-Core Team, 2020). All R packages used are listed in Supplementary Table S4. This study was deemed exempt from review by the Institutional Review Board due to the use of nationally available, de-identified data.
Results
The overall population undergoing thyroid procedures had a median age of 48 years and was predominantly female (74%). The majority of patients undergoing thyroid surgery had a score of 0 comorbidities (67%), as defined by the AHRQ-weighted Elixhauser index. Most patients were on a PPO plan (61%) at the time of surgery and were the primary beneficiary of the plan (62%) (Table 1).
Baseline Characteristics of Patients with Thyroid Surgery Claims in the 2007–2018 MarketScan Commercial Claims and Encounters Database
Note: All percentages were rounded to the nearest integer. A thyroidectomy procedure was considered a completion if the operation occurred within 6 months of the index operation. Indication diagnoses are based on the classification described by Supplementary Table 3. The Elixhauser Index was calculated according to the weighted AHRQ Elixhauser Comorbidity Index. Insurance types included under “Other” are: Basic/major medical, EPO, CDHP and HDHP plans.
AHRQ, Agency for Healthcare Research and Quality; CDHP, Consumer-Driven Health Plan; EPO, Exclusive Provider Organization; HDHP, High Deductible Health Plan; HMO, Health Maintenance Organization; IQR, interquartile range; POS, Point-of-Service Organization; PPO, Preferred Provider Organization; TL, thyroid lobectomy; TT, total thyroidectomy.
Of the 220,088 thyroid procedures, ∼23% (49,788/220,088) were performed in the inpatient setting versus 77% (170,300/220,088) in the outpatient setting. Table 2 shows the detailed longitudinal data.
Yearly Counts of Thyroid Procedures by Clinical Setting
From 2007 to 2018, the proportion of thyroid procedures performed in the inpatient setting decreased every year. The proportions of TT relative to TL and completion thyroidectomies rose from 2007 to 2015 and started to decrease thereafter (Fig. 1).
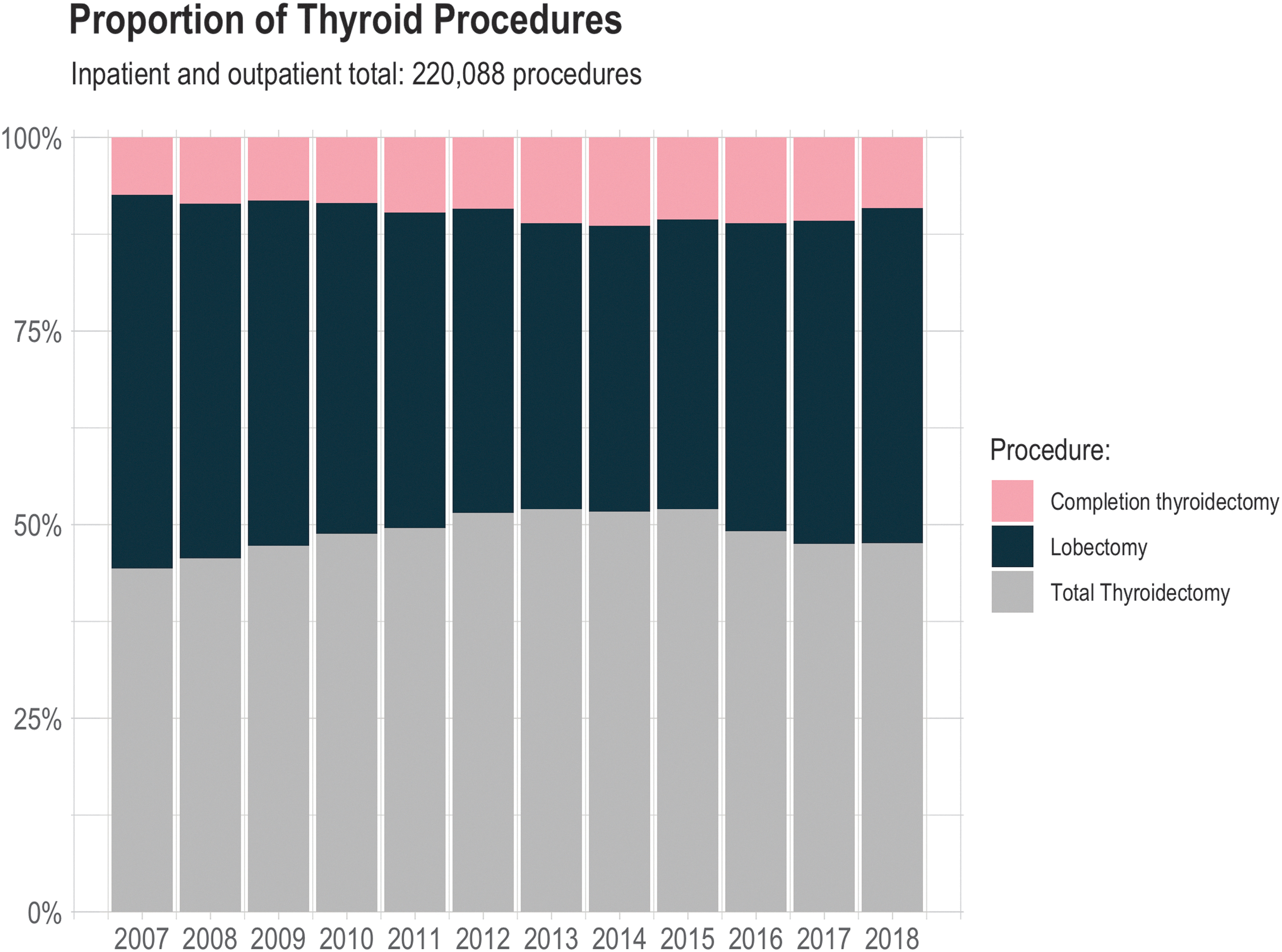
Proportion of thyroid procedures. Inpatient and outpatient total: 220,088 procedures. Color images are available online.
The majority of thyroid surgeries were performed on patients whose surgical diagnosis was classified as benign thyroid disease (Table 1). Approximately 26% (55,202/220,088) of patients undergoing thyroid surgery were suspected to have malignant disease, based on their indication diagnosis. In 2015, TL accounted for 51% (3794/7448) of the procedures performed for benign disease and 17% (550/3192) for malignant disease. By the end of 2018, TL accounted for 56% (3227/5719) of the procedures performed for benign disease and 28% (793/2859) for malignant disease. The increasing trend in performing TL for benign and malignant disease was found in both the inpatient (Fig. 2A) and outpatient (Fig. 2B) settings.

Surgical indication diagnosis by setting and procedure type: (
From 2007 to 2018, the proportion of surgeries performed in the outpatient setting for both benign and malignant thyroid disease increased (Fig. 3). For benign disease, 67% (6698/9976) of the procedures were performed in the outpatient setting in 2007; 95% (5432/5719) were outpatient by the end of 2018. For malignant disease, 51% (1447/2867) of the surgeries were performed in the outpatient setting in 2007; this rose to more than 89% (2552/2859) by the end of 2018.
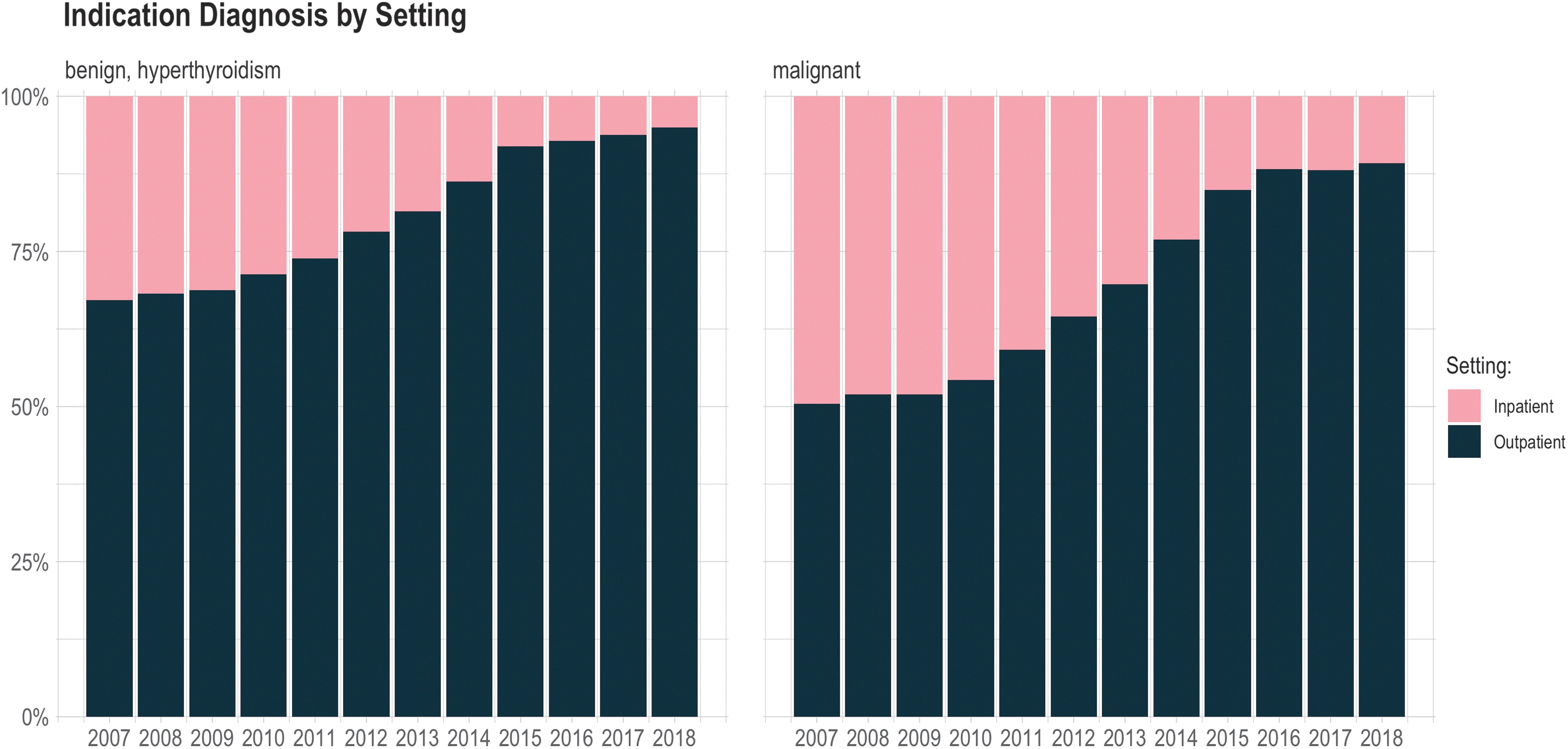
Indication diagnosis by setting. Color images are available online.
The baseline factors predictive of TT versus TL were age, female sex, a surgical indication diagnosis of “hyperthyroidism” or “malignant,” Elixhauser index, South region of the United States, having a comprehensive medical plan, a POS or capitated POS plan, or an HMO plan (p < 0.001) (Table 3). Patients with a thyroid malignancy (odds ratio (OR) = 5.36 [confidence interval {CI} 5.22–5.50]) or hyperthyroidism diagnosis (OR = 6.48 [CI 6.15–6.84]) at the time of surgery had the highest odds of undergoing a TT. Patients had higher odds of undergoing a TL if they had a surgical indication diagnosis of “uncertain” (OR = 0.68 [CI 0.65–0.71]). Female patients were ∼25% more likely (OR = 1.25 [CI 1.22–1.28]) to have a TT than male patients. Increasing Elixhauser index was associated with a higher likelihood of TT versus TL (OR = 1.05 [CI 1.05–1.05]). The HMO (OR = 1.10 [CI 1.06–1.24]), POS (OR = 1.18 [CI 1.14–1.23]), and Comprehensive (OR = 1.14 [CI 1.06–1.22]) insurance plans were associated with a higher likelihood of TT. Patients receiving surgery in the South region of the United States were more likely to have a TT (OR = 1.24 [CI 1.21–1.28]).
Univariate Analysis for Factors Associated with Inpatient or Outpatient Total Thyroidectomy
In the inpatient setting, the baseline factors significantly associated with undergoing a TT versus a TL were age, female sex, Elixhauser index, and a thyroid malignancy and hyperthyroidism diagnosis at the time of surgery (p < 0.001). Patients with a thyroid malignancy (OR = 3.44 [CI 3.24–3.66]) or hyperthyroidism diagnosis (OR = 4.02 [CI 3.67–4.41]) at the time of surgery had the highest odds of having an inpatient TT. Patients had a higher likelihood of a TL if they had a surgical indication diagnosis of “uncertain” (OR = 0.67 [CI 0.55–0.82]). Female patients were ∼25% more likely (OR = 1.24 [CI 1.18–1.31]) of having an inpatient TT than male patients. Increasing Elixhauser index was associated with a higher likelihood of TT versus TL (OR = 1.04 [CI 1.03–1.04]). Patients receiving surgery in the North central region of the United States were less likely to have a TT (OR = 0.86 [CI 0.80–0.91]).
In the outpatient setting, the factors associated with having a TT were age, female sex, Elixhauser index, North Central and South regions of the United States, a thyroid malignancy or hyperthyroidism diagnosis, having an HMO, POS, or comprehensive insurance plan (p < 0.001). Patients with a thyroid malignancy (OR = 6.24 [CI 6.05–6.43]) and hyperthyroidism (OR = 7.68 [CI 7.19–8.21]) at the time of surgery had the highest likelihood of receiving an outpatient TT compared with all other baseline patient covariables. Patients had higher odds of having an outpatient TL if they had an “uncertain” diagnosis at the time of surgery (OR = 0.73 [CI 0.70–0.77]). Other factors that increased the odds of having an outpatient TT were female sex (OR = 1.25 [CI 1.22–1.29]), having a POS plan (OR = 1.23 [CI 1.17–1.29]), an HMO plan (OR = 1.12 [CI 1.07–1.17]), or a Comprehensive plan (OR = 1.16 [CI 1.07–1.26]). Increasing Elixhauser index (OR = 1.12 [CI 1.11–1.14]) and having surgery in the North central (OR = 1.09 [CI 1.05–1.13]) or in the South (OR = 1.39 [CI 1.34–1.43]) regions of the United States were also associated with a higher likelihood of a TT.
Using Pettitt's test, we detected a statistically significant changepoint in the monthly proportion of TT (p < 0.001). The changepoint was November 2015, corresponding to the month following the online ATA guideline release in October 2015. The mean proportion of TT (vs. TL) was 80% the month preceding the ATA guideline release (September 2015) and it gradually declined to 39% by December 2018 (Fig. 4).
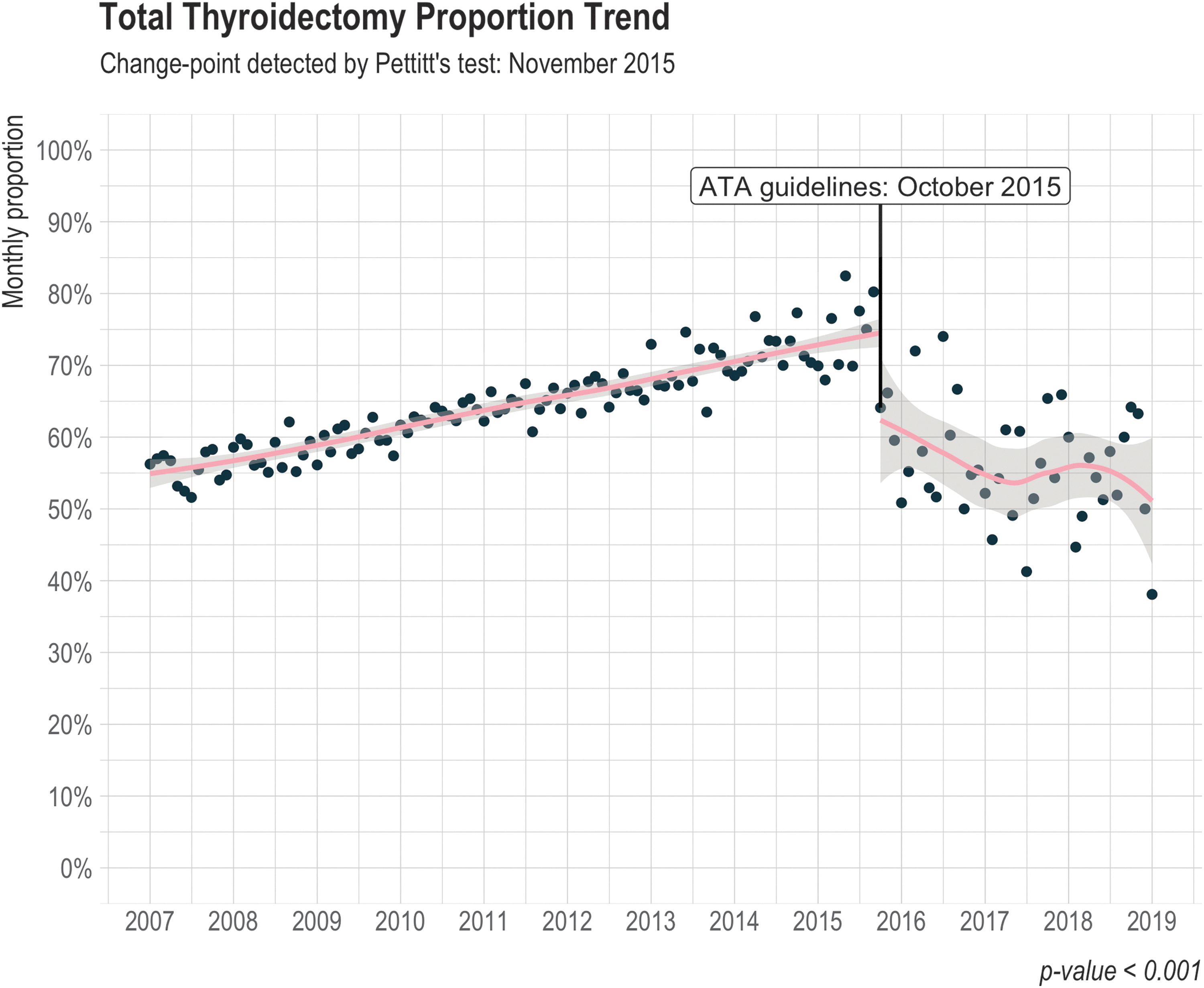
Total thyroidectomy proportion trend. The statistically significant changepoint detected by Pettitt's test was November 2015 (p < 0.001). A line of best fit using linear smoothing was plotted on the time-series data both before and after the online release of ATA guidelines in October 2015. ATA, American Thyroid Association. Color images are available online.
Discussion
In this study, we queried the nationwide MarketScan database from 2007 to 2018 to examine trends in thyroid surgery. To examine the effect of the 2015 ATA guidelines on surgical thyroid nodule management, longitudinal analysis was employed. A changepoint in the monthly trend of TT was identified in November 2015, just 1 month after the online release of the ATA guidelines in October 2015. This analysis supports the claim that nationwide practices were influenced by the release of the ATA guidelines and fewer TT were performed in favor of TL for both benign and malignant thyroid disease.
Other analyses have reported a relative decrease in TT following the release of the 2015 ATA guidelines in the inpatient setting for the TC population (13,20). Hirshoren et al. (20) showed an increase in TL compared with TT for well-DTC at their tertiary medical center in Israel. Ullmann et al. (13) also found that, among 35,291 inpatient and outpatient cancer patients, the rate of TL in the United States increased ten-fold from 2009 to after the release of the 2015 ATA guidelines. Of note, Ullmann et al. (13) used the National Surgery Quality Improvement Program (NSQIP) database to assess surgical trends. The NSQIP is a large and nationally validated database; however, it only contains data from participating institutions engaged in quality improvement initiatives. Our study also shows a decrease of about 25% in the proportion of TT following the release of the ATA guidelines (Fig. 4). The trend toward less extensive surgery was observed in both benign and malignant thyroid disease after the 2015 guideline release. We hypothesize that the stronger response to the 2015 ATA guidelines compared with earlier releases (such as the 2009 ATA guidelines) could be due to the increasing and recent body of high-quality evidence informing those guidelines and the knowledge that adherence to guidelines is correlated with level of evidence. The 2009 ATA recommendations with regards to performing TT versus TL for high-risk patients (21) were largely based on studies conducted in the 1980s and 1990s (22 –24), with just one study conducted in 2007 for low-risk TC (25).
There may be several factors behind the relative increase in TT from 2007 to 2015 followed by an increase in TL from 2015 to 2018. The steady increase in the proportion of TT from 2007 to 2015 could be attributed to research showing similar recurrence and survival in patients who had TT versus TL, which motivated recommendations 25 and 26 of the 2009 ATA guidelines (21). This increasing trend of TT is consistent with the findings of Mitchell et al. (26) and Sosa et al. (27), both of which showed a relative increase in TT in the timespans of 1978–2004 and 2006–2011, respectively. There may be several explanations for the significant relative increase of TL versus TT for benign thyroid disease from 2015 to 2018. Since 2012, molecular testing has been used to rule out malignant disease and therefore avoid the need for TT or surgery altogether (2,28). It is plausible that molecular testing has contributed to less aggressive surgical management of indeterminate or benign nodules and thus contributed to the increased relative rate of TL for benign thyroid disease. Unfortunately, non-invasive follicular thyroid neoplasm with papillary-like nuclear features (NIFT-P) is not an ICD diagnosis so the impact of the NIFT-P designation cannot be studied by using MarketScan; however, it is also possible that TL rates have increased due to the diagnostic TL performed for NIFT-P (7). Perhaps the focus on avoiding thyroid hormone replacement due to detrimental effects on quality of life has also driven the shift toward more TL (29). Moreover, a hypothesis proposed by Mitchell et al. (26) suggests that women (particularly young women) could be seeking health care services at higher rates than men. This could lead to increased detection of thyroid incidentalomas and thus TC, and it could explain why there is a higher likelihood of receiving a TT among female patients (OR = 1.25 [CI 1.22–1.28]) (26).
Nonadherence to 2009 ATA and 2010–2011 National Comprehensive Cancer Network guidelines was associated with worse survival for TC (10). Factors associated with nonadherence included discordance between the two guidelines, Black race/ethnicity, and treatment at a nonacademic center. Adam et al. (10) showed that on multivariable analysis, TT and TL had an equivocal impact on survival. The impact on survival was not studied for this article. There may also be external factors motivating this rise in TT, such as financial incentives and socioeconomic differences. In this study, the likelihood of receiving a TT versus TL was associated with insurance plan type. It appears that patients having insurance plans with less generous cost-sharing (e.g., HMO and POS) are at a lower likelihood of receiving TT (p < 0.001). This may be due to the willingness of patients to potentially receive 2–3 separate procedures (such as two-stage diagnostic TL followed by a completion thyroidectomy, or a TL followed by a completion thyroidectomy) instead of TT, a one-time procedure. This willingness to receive multiple treatments is particularly relevant in light of the Affordable Care Act's essential health benefits that do not currently apply to thyroid surgery. The association between insurance status and extent of TT may also be driven by differences in referral networks. It is well established that physicians practicing in lower socioeconomic settings that are likely associated with underinsured patients have smaller networks (30) and may be less guideline-concordant. Spatial variations, along with other socioeconomic factors, will be addressed in our next investigation.
There are limitations to this study. Medical claims data can suffer from missing data and have the potential for procedure and diagnosis coding errors. In addition, CPT and ICD diagnosis and procedural codes are not sufficiently granular to capture all oncologic data. Of note, the diagnosis code listed at the time of surgery is not informed by the final histopathologic diagnosis. This study also used first-position only procedural and diagnosis codes in determining the thyroid procedure and indication diagnosis, respectively. We followed this conservative approach, because first-position codes are considered to be the main procedure and diagnosis in the patient's stay (i.e., the procedure and diagnosis that incurred the majority of the costs associated with the episode of care). Another limitation of this study is the longitudinal nature of our data query to MarketScan. Our inclusion criteria for every year were a diagnosis of a goiter or thyroid nodule. Given the time difference between a goiter/thyroid nodule diagnosis and surgery, there is a decrease of yearly total procedures in the most recent years of our study period (Table 2). Although MarketScan data comes from more than 350 payers, weights need to be applied to transform it into a nationally representative sample of the U.S. employer-insured population, which represents about half of the U.S. population. Future research will include standardizing utilization trends and other estimates to the U.S. employer-insured population. Further economic analysis to assess the impact of the shift to mostly outpatient surgery and less aggressive surgery will help elucidate the impact of these trends on long-term clinical and economic outcomes. Future work will assess demographic, spatial, and socioeconomic characteristics that may influence practice variation. In this study, we focused on the relative trends of TT versus TL, because the 2015 ATA guidelines do not provide well-defined recommendations on completion thyroidectomies. Future work will also explore completion thyroidectomy trends and outcomes. Finally, future work will also assess whether the shift to less aggressive management will mitigate over-diagnosis and over-treatment in this population and to identify improved risk-stratified approaches.
Our study provides a comprehensive examination of nationwide surgical trends in a fully adjudicated database containing more than 200,000 thyroid surgical insurance claims in the timespan of 12 years. We show that the release of the 2015 ATA guidelines was associated with a significant changepoint in the decrease of thyroidectomies and increase in lobectomies nationwide in both the inpatient and outpatient settings. Our study supports the effect of the 2015 ATA guidelines in influencing the surgical management of thyroid nodules in the United States.
Footnotes
Authors' Contributions
Concept and design: A.T., C.C.L.; acquisition of data: A.T.; analysis and interpretations of data: A.T., C.C.L., C.D., V.V., M.S.J., J.C., G.S.G., and R.R.K.; drafting of the article: A.T., C.C.L.; critical revision of the article for important intellectual content: A.T., C.C.L., C.D., V.V., M.S.J., J.C., G.S.G., and R.R.K.; supervision: C.C.L.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This work was supported by NIH/NCI R37 CA231957 (C.C.L.). The funder had no role in the design and conduct of the study; collection, management, analysis, and interpretation of the data; preparation, review, or approval of the article; and decision to submit the article for publication.
Supplementary Material
Supplementary Table S1
Supplementary Table S2
Supplementary Table S3
Supplementary Table S4