
Abstract
Background:
The majority of small papillary thyroid cancers (sPTCs) are treated surgically, rather than by active surveillance. Patient and clinician preference for surgery may be partially driven by the use of cancer terminology. Some experts propose that changing terminology would better communicate the indolent nature of sPTCs and improve uptake of active surveillance. Others argue that terminology that includes “cancer” correctly reflects the biological nature of these tumors. The views of informed lay publics can provide value-based perspectives on complex issues and guide policy discussions.
Methods:
We recruited 40 people for three community juries, held in Sydney, Wodonga, and Cairns, Australia. Participants were of diverse backgrounds and ages, recruited through random digit dialing and a topic-blinded social media strategy. Juries were informed about thyroid cancer, overdiagnosis, and overtreatment, and heard arguments for and against terminology change before deliberation. The deliberative process in Jury 1 led to a refinement of jury charge, the updated version that was then used in Juries 2 and 3.
Results:
Jury 1 favored no terminology change, and Juries 2 and 3 were divided on the topic. Key reasons for opposing terminology change included a strong desire to retain terminology that aligns with the pathological definition of cancer, and to avoid even a minimal risk of harm that could arise if patients became complacent in follow-up. Key reasons to support terminology change included a desire to reduce psychological distress, stigma, and discrimination associated with a cancer diagnosis, and an argument that terminology change may be a more effective trigger for health system reform compared with other options. The juries unanimously recommended community education and health system reforms to reduce harms of overtreatment, and expressed an expectation that clinicians and researchers reach agreement on clinical guidelines to promote better uptake of active surveillance.
Conclusions:
The conceptual tension between a pathological and an outcome-based understanding of cancer was apparent in deliberation. This highlights an ongoing challenge for those advocating changing disease terminology. Regardless of action on terminology, jurors shared a strong expectation that practical changes would be made to respond to the harms of overtreatment.
Introduction
Low-risk small papillary thyroid cancers (sPTCs) have low risk of metastasis (1), yet are increasingly detected and brought to clinical attention (2,3). Most patients are treated surgically with thyroidectomy or lobectomy, the former potentially requiring long-term hormone treatments with quality-of-life impacting side effects (4). When a diagnosis is made as is considered correct in the relevant professional community, but is unlikely to cause harm to the patient, it is called overdiagnosis (5). When subsequent treatments do not lead to corresponding improvement in patient outcomes (2,3), or cause more harm than the disease itself, it is called overtreatment (5). Studies have demonstrated that active surveillance of low-risk sPTCs can be a management option (6,7), and guidelines now suggest considering this less invasive course of management (8). However, clinicians in Australia and the United States do not seem to be actively recommending or adequately explaining this option (9 –11), and most patients have a preference for surgical treatment, even if active surveillance is offered (11,12).
“Cancer” is an anxiety-provoking term leading to a preference for more invasive treatment options, including for papillary thyroid cancers (PTCs), compared with instances where another term is used (13 –16). To improve uptake of active surveillance, changing the terminology of sPTCs to align with clinical expectations of the condition has been proposed (17). This is known as nomenclature revision, and involves changing not only the condition name but also how it is classified. Nomenclature revision has occurred for a small proportion of PTCs, with noninvasive follicular thyroid neoplasm with papillary-like nuclear features (NIFTP) replacing many previous diagnoses of encapsulated follicular variant of PTC (18). However, nomenclature revision of intrathyroidal sPTCs is contentious, because although the risk of subsequent metastasis is low (1), its pathological features fit within the definition of a malignant tumor. According to a recent systematic review of patients with PTC undergoing active surveillance, the pooled proportion of growth among sPTCs <10 mm diameter without evidence of nodal metastasis at diagnosis was 5.3% at 5 years, and the pooled proportion growth of 5-year lymph node metastasis was 1.6% (1). So although the risk of metastases of sPTCs is extremely low and the condition shows good clinical prognosis, in contrast to NIFTP (18), a benign course cannot be guaranteed.
In consideration of the disagreement among experts about how to manage the risks of sPTC, the views of an informed lay public can usefully inform relevant health care research and policy making (19). Previous research (20) on public perspectives on low-risk PTC treatment indicates that while changing the terminology might reduce psychological impacts, people have concerns about the risk of disease progression and that a terminology change might confuse patients and create complacency. Building on this work, we conducted three community juries, using deliberative research methodology to allow an informed, extensive, two-way engagement between topic experts and community jury members (21). Each jury comprised citizens drawn from a cross section of the local community. We sought information on whether informed members of the public, from metropolitan, regional, and rural settings, consider terminology change to be an appropriate means of addressing overdiagnosis and overtreatment of sPTCs in the Australian community, and what other measures they thought should also be considered.
Methods
This study was approved by the University of Wollongong Human Research Ethics Committee (HREC 2019/362).
Study participants and jury procedure
Forty people were recruited from three community juries, held in Sydney, Wodonga, and Cairns (respectively, a metropolitan, rural, and regional site) aiming for geographic and socioeconomic diversity, sex parity, and representation across age groups (Table 1). The juries were held over 2 days on 3 weekends between December 2019 and March 2020. Each jury considered the “jury charge” (Box 1), the central question designed to prompt debate and elicit participant views on the topic. Four experts each provided a 20-minute prerecorded video presentation, offering different perspectives on disease definition, terminology, treatment decision-making, and the ethical implications of changing cancer terminology. Presenting experts participated in a live question and answer session, allowing jurors to clarify or seek new information. An expert in thyroid cancer terminology change attended each jury and answered questions raised during deliberations. There were two facilitated and one nonfacilitated deliberative session for jurors to reflect, debate, and consider the range of issues raised, before providing recommendations and reasons for their collective and individual views (the “verdict”) (see Fig. 1 for sequence of events). To explore changes in juror positions on the charge, a time point survey was taken four times (before expert presentations, after presentations, start of day 2, conclusion of day 2, see Fig. 1). Additional itemized information reporting the community jury procedures in accordance with the CJCheck checklist (22) is reported in Table 2.
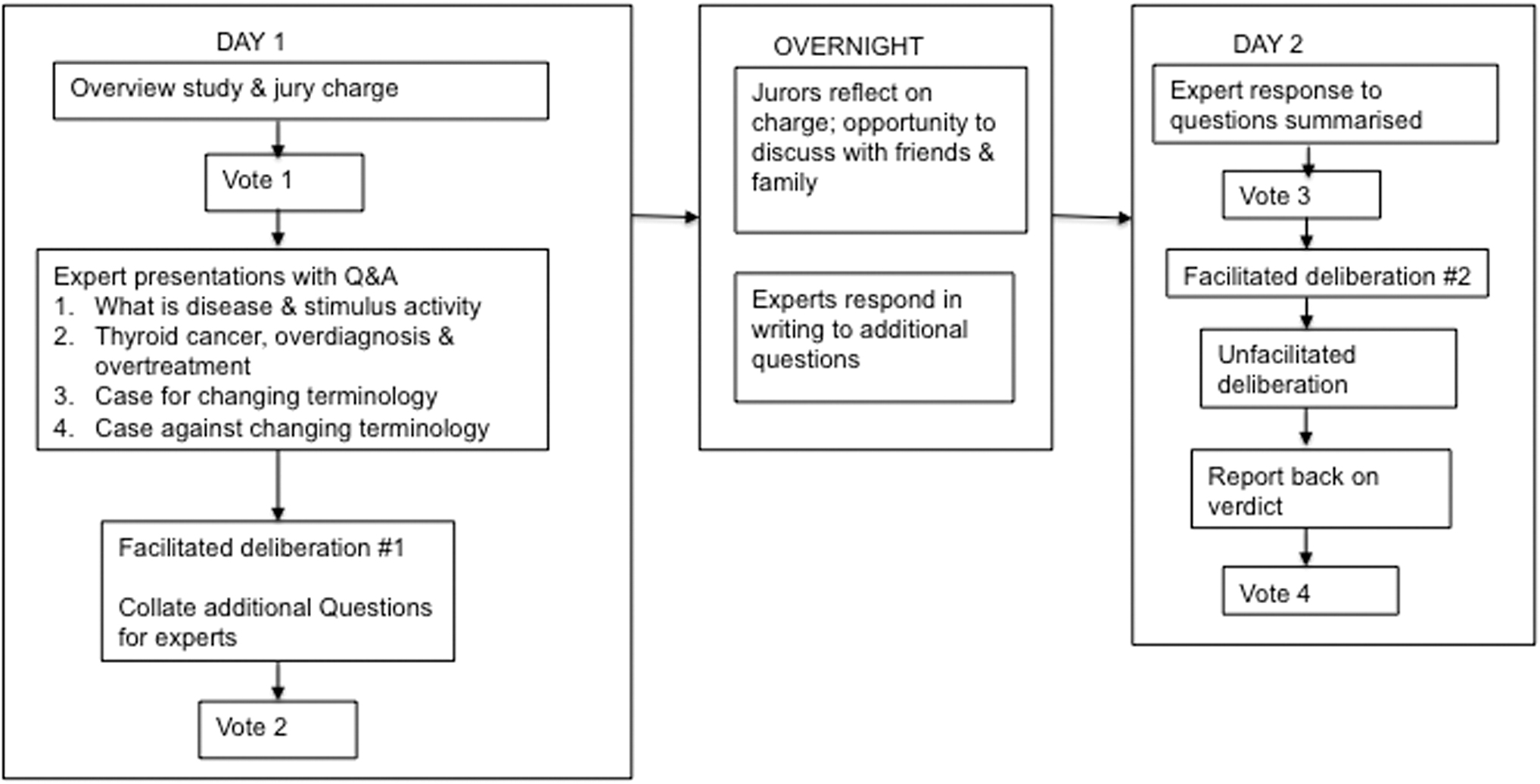
Community juries' procedure.
Jury Charge
Participant Characteristics
Based on socioeconomic index for area.
CJCheck Items Reported
Based on CJCheck items developed by Thomas et al. (22).
Clarification of jury charge after Jury 1
Although Jury 1 was intended to act as the first of three, some lack of clarity in the jury charge wording was identified. Participants questioned whether “relabeling” implied a superficial change in name but not a change in pathological classification. This was a potential source of misunderstanding and compromised the focus of the deliberations. The jury charge therefore was refined after Jury 1 to clearly state that the terminology change referred to the reclassification and renaming of the disease. The relevant expert presentations were also slightly revised to reiterate this point. The charge and expert presentations were consistent in Juries 2 and 3 (Box 1).
Results
Jury 1 voted 11-2 opposing changes to terminology. The key reason rested on the “truthful” representation of cancer via its terminology, and the preference for concentrating on preexisting health system resources in public education and patient support. Juries 2 and 3 were unable to reach a clear majority position (Fig. 2). The key divide was between the value placed on an objective pathological definition of the disease and reducing unwarranted psychological harm, and whether terminology change is an effective trigger for system change. The time point votes (Fig. 2) show that a significant number of jurors (8 in Juries 1 and 2; 6 in Jury 3) shifted their position (either supporting or opposing terminology change) during the deliberation process.
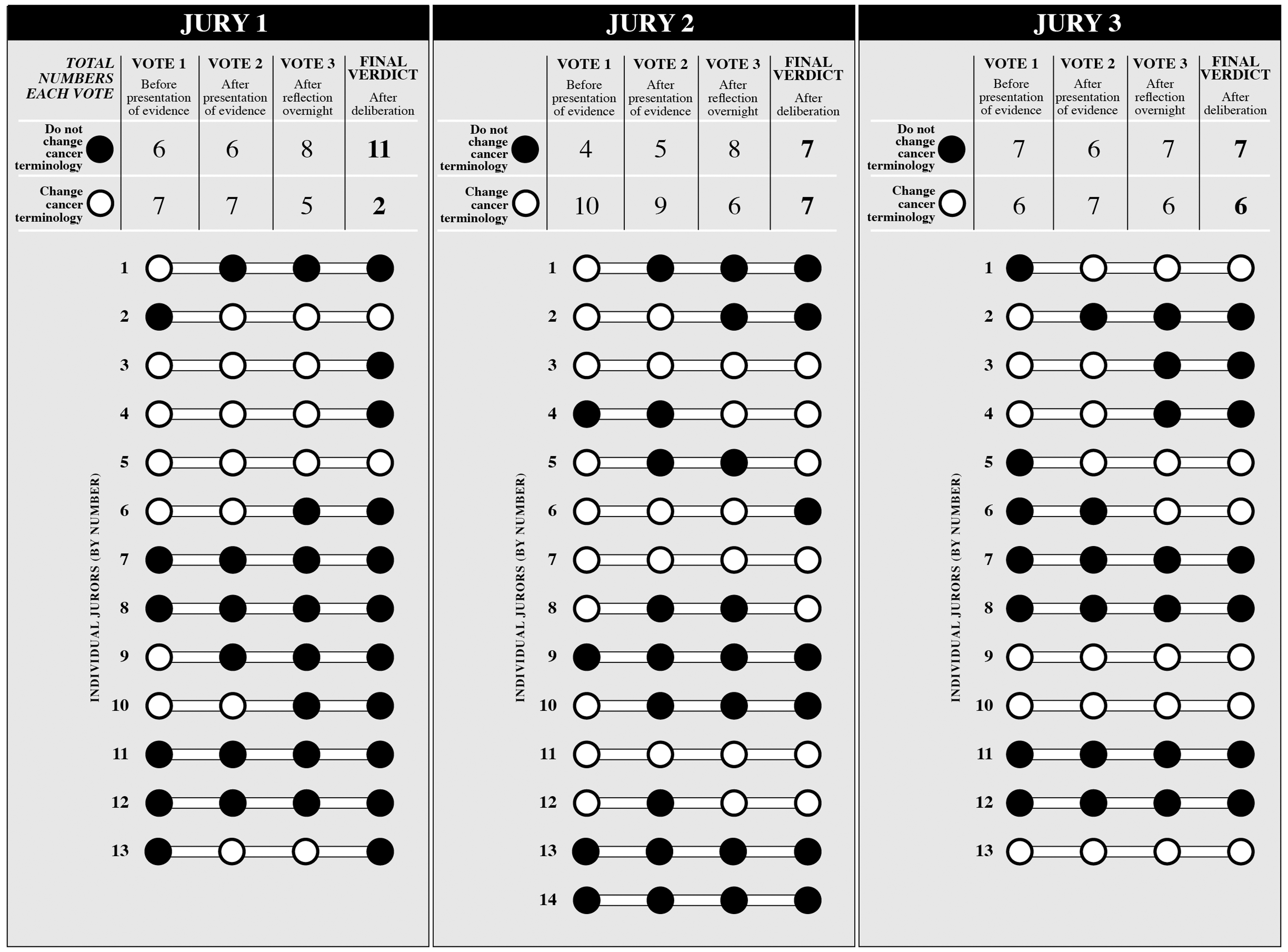
Summary of votes across juries and change in individual jurors' votes over time.
Key reasons highlighted for supporting or not supporting terminology change in each jury are described below, with further reasons outlined in Table 3.
Summary of Key Reasons for Jury Verdicts and Recommendations
sPTCs, small papillary thyroid cancers.
Reasons for not supporting terminology change
Current terminology reflects the malignant nature of sPTCs
Most jurors who voted against terminology change argued that sPTCs are, by definition, malignant and thus fall within the pathological classification of cancer. The view was expressed repeatedly during discussions, for example, “cancer is cancer” or “it is what it is,” and that not using the word “cancer” to label the condition may conceal the true nature of the disease. These jurors understood that the risk of metastasis occurred for a small minority of patients, but emphasized that pathological features of sPTCs include the potential to progress and metastasize. Jurors who took this position, particularly in Jury 3, reasoned it would be irresponsible to ignore even the lowest risk of harm by changing terminology because it could mislead patients to the extent that they expect no chance of disease progression, and/or result in complacency toward active surveillance. Members of Jury 1 also recognized the power of the term “cancer” in channeling research funding and public attention.
More evidence and research needed
Those unsupportive of terminology change also argued that current evidence was insufficient to support the proposed reforms. Jury 2 wanted more reassurance that any unintended consequences of reclassification can be mitigated. This position included openness to considering terminology change in the future should more evidence emerge to support it, such as new diagnostic technologies that allowed the differentiation of the type of sPTCs that would and would not progress and metastasize.
New terminology within the definition of cancer
Jury 3 suggested a conceptualization of cancer terminology beyond the wording provided in the jury charge. Some jurors proposed creating an additional category of classification within sPTCs that would retain reference to the potential for malignancy, but more strongly emphasize the low level of risk by nuancing terminology, primarily for the purpose of improving clinician/patient communication. They suggested a range of possible prefixes that denote lower risk (e.g., indolent, micro, or low risk). Although “microcarcinoma” (tumors ≤10 mm diameter) is a classification already available to pathologists, as presented in expert evidence, the jurors sought a label that would convey the risk and prognosis more clearly and consistently, particularly for lay audiences, and therefore be adequate, in practice, to encourage active-surveillance uptake and minimize psychological distress. In essence, these jurors did want to see a change to disease terminology in sPCTs in the interest of harm reduction, but also wished to maintain some recognition that these lesions are consistent with the pathological definition of cancer. All but one of the jurors who voted against terminology change in Jury 3 stated that this was their preferred scenario.
Reasons for supporting terminology change
Reduce psychological harm of a cancer diagnosis
In all juries, the primary reason for supporting terminology change was to reduce the harm caused by psychological distress and fear. Jurors argued that the term “cancer” (when applied to sPTCs) would trigger an unjustifiable and unwarranted degree of distress for patients, their families, and friends. This was because the majority of diagnosed cases of low-risk sPTCs would not progress or be life threatening, recognizing if people were not diagnosed, they would lead healthy lives. If sPTCs were reclassified to sit outside of “cancer,” disease terminology would be more aligned with its expected prognosis, therefore leading to less aggressive treatment recommendations. The two jurors supporting terminology change in Jury 1 also suggest there may be financial advantages for patients if they did not undergo unnecessary treatments.
Terminology change would trigger health system change
Some jurors reasoned that without a terminology change, the fundamental shifts in the health system required to reduce overtreatment (e.g., education programs, revising of clinical guidelines) would not occur. This was based on jurors' skepticism that community and clinician education alone would be sufficient to change clinical practice. Notably, eight jurors who opposed terminology change in their final verdict in Jury 1 agreed that if the health care system reforms they recommended did not objectively reduce harms caused by unnecessary treatment within a set time frame, then a terminology change would be a reasonable course of action.
Social and financial implications of changing terminology
Reducing wider social and financial harms or disadvantages associated with a cancer diagnosis was another reason for supporting terminology change. Jurors said a cancer diagnosis of any kind might preclude employment in some professions, and attract higher life and travel insurance premiums. Some jurors believed this was unjustifiable for people with such a low-risk form of cancer, especially for younger patients who would live longer with a diagnosis.
Recommendations and conditions
Each jury was also asked to outline any conditions under which they would either support or oppose terminology change. There was a clear agreement across the juries on two recommendations, irrespective of position on terminology change:
Education for patients and the public
All juries agreed that it was essential that community education be provided about overdiagnosis and overtreatment in low-risk sPTCs, and active surveillance be consistently offered as a disease management option. Jurors who voted against terminology change preferred education as the first course of action to respond to overdiagnosis. Jurors who voted for terminology change reasoned that community education should accompany the health system changes brought about by terminology change. There was a concern that terminology change may only be a “quick fix” if education is not available. Education was proposed to focus on changing public attitudes surrounding cancer treatment and stigma, and to promote an understanding of the diversity in risk levels and outcomes for different types of cancers; outline the range of treatment options; provide psychological support; and recognize that people with sPTCs can survive and “live normally.”
Clinical responsibility and health system change
All juries emphasized that, as health care professionals were custodians of and authorities on sPTC-related knowledge and medical practice, they should carry most of the responsibility for reducing the harms of overtreatment. Accordingly, health systems should initiate processes and infrastructure to improve the offering and uptake of active surveillance. Jury 2 suggested setting up a national register providing regular reminders for follow-up for diagnosed patients, which may also act as a resource for building an epidemiological database to better understand disease progression, and thus better evidence and research for sPTCs.
Support for rural and regional patients
Both Juries 2 and 3 were conducted outside of major metropolitan areas. Participants in these groups drew on their experiences of having limited access to good-quality specialist health services in these regions, suggesting that patients with cancer are more likely to opt for more aggressive treatments due to the cost and inconvenience of travel for monitoring. They recommended that any change in thyroid cancer treatment practices should ensure affordability, accessibility, and coverage for regional and rural Australians.
Discussion
The community jury deliberations highlighted the conflict between two key concerns when considering terminology change: ensuring that terminology reflects the pathological features of the disease and minimizing the psychological and treatment harms caused by a diagnosis of a low-risk cancer.
The pathological definition of cancer offers clinicians and patients a sense of objectivity, which hinges on a clear link to the risk of potential metastasis, however minimal. The reluctance to remove the connotations of seriousness and severity that come with the label “cancer” is a practical concern about ensuring adherence to disease monitoring, and reflects the cultural fear of cancer and the value placed on avoiding its potential harms. This is consistent with previous studies on thyroid cancer terminology change, which show the same reservations among clinicians, patients, and members of the public (9,12,20).
However, when given balanced evidence and opportunity for discussion, almost half of the participants in the latter two juries were prepared to support a definition of disease that explicitly reflected the low-risk outcomes for the majority of patients with sPTCs. This also demonstrates a high cultural value placed on reducing psychological harm and overtreatment caused by a distressing disease label. That jurors often changed their minds between the time point votes indicates the complexity of the topic, and that many felt there were important and convincing reasons for both supporting and opposing terminology change in sPTCs. To our knowledge, the current study is the first to show some support among members of the public for this way of thinking about changing disease terminology.
The proposal by Jury 3 for the nuancing of terminology within sPTCs to de-escalate expectations and actions of the disease suggested a middle-ground to bridge changing pathological definitions on one hand and communication practices on the other. While more work would elucidate this issue further, it highlights the limitation of current terms such as “microcarcinoma,” which may convey prognosis to those with specialist expertise about the disease, such as pathologists and clinicians, but potentially not to patients insofar as it enables them to be more open to consider active surveillance.
Overall, there was strong support for improving the uptake of active surveillance as the best and most immediate way to reduce the high level of unnecessary surgery, irrespective of the position on terminology change. Recent studies conducted at Kuma Hospital in Japan among patients with sPTCs and in Canada with older patients with slower progressing low-risk PTC have found high uptake of active surveillance (23,24). This suggests patients are accepting of active surveillance when given informed and balanced options for treatment, particularly when clinicians promote this option (23,24).
Without evidence of outcomes from active surveillance such as that provided by Kuma Hospital, the uptake of this treatment option in other populations may be lower. In Australia and the United States, studies with clinicians and patients indicated that clinicians were not yet comfortable in recommending active surveillance, and patients had strong preferences for the reassurance afforded by surgical treatment (9,11,12). A more recent study in the United States suggested that patients' knowledge about thyroid cancer was low, and there were assumptions that a cancer diagnosis would lead automatically to surgery; therefore, education about the range of possible treatments would be important (10). Clinician recommendations and the treatment decisions of patients are influenced by the context of their health care system, and therefore, system reform is a logical approach to encouraging change. This is clearly reflected in the recommendation by all three juries, including the strengthening and standardizing of current clinical guidelines in response to the overdiagnosis and overtreatment of sPTCs.
Similarly, the scaling up of community education was another favored response to overdiagnosis and overtreatment by jurors in our study, a strategy widely recommended to initiate a cultural change around the social understanding of cancer and attitudes toward the expected clinical practice (17,25,26). However, as a number of jurors recognized, there are limits to community education and a slow pace of change in clinical practice, prompting the view that terminology change was a necessary “trigger” for more prompt and widespread change.
While our community juries aimed to recruit diverse members of the public from different geographic areas, the results are not intended to assert a generalizable representation of public opinion, nor reflect cultural contexts or health systems outside of Australia. Individual opinions can be influenced by contextual aspects such as the differences in personalities, focus of issues, and direction of questions and answers. The specific design and makeup of presentations by experts, and the issues and arguments they focus on may also shape the outcome. The wording modification, although minor after Jury 1, may have influenced the different outcomes of Juries 2 and 3, but it is not possible to determine if this was the key driver of such a result.
The key contribution of this study is its strength in bringing public views on cancer terminology change into dialogue with expert perspectives, to facilitate a fuller understanding of cancer diagnosis and its long-term consequences for patients and the wider community. The breadth of perspectives elicited in community juries signifies the importance of engaging the public in developing potential solutions for challenging health care issues.
Footnotes
Acknowledgments
We thank Marijka Batterham and James de Vries for supporting data visualization, and Kathleen Prokopovich for assisting with the initial literature searches.
Authors' Contributions
P.S., B.N., S.M.C., C.D., R.T., and K.M. planned and designed the study. J.P.B. and D.S.A.M. contributed to refining the study design and took part in data collection. All authors contributed to the analysis of the study results and approved the submitted article.
Author Disclosure Statement
There are no conflicts of interests to declare.
Funding Information
This project is funded by a National Health and Medical Research Council Centre for Research Excellence Grant (No. 1104136). RT is supported by a National Health and Medical Research Council Program grant (No. 1106452).
Supplementary Material
Supplementary Appendix SA1