
Abstract
Background:
We report the therapeutic use of K1-70™, a thyrotropin receptor (TSHR) antagonist monoclonal antibody, in a patient with follicular thyroid cancer (FTC), Graves' disease (GD), and Graves' ophthalmopathy (GO).
Methods:
A 51-year-old female patient, who smoked, presented in October 2014 with FTC complicated by GD, high levels of TSHR autoantibodies with high thyroid stimulating antibody (TSAb) activity, and severe GO. K1-70 was administered at 3 weekly intervals with the dose adjusted to block TSAb activity. Her cancer was managed with lenvatinib and radioiodine therapy.
Results:
Following initiation of K1-70 therapy, TSAb activity measured in serum decreased and GO (proptosis and inflammation) improved. On K1-70 monotherapy during the pause in lenvatinib, several metastatic lesions stabilized while others showed progression attenuation compared with that before lenvatinib therapy.
Conclusions:
These observations suggest that blocking TSHR stimulation with K1-70 can be an effective treatment for GO and may also benefit select patients with FTC and GD.
Introduction
The human monoclonal autoantibody K1-70™ is a specific thyrotropin receptor (TSHR) antagonist with therapeutic potential in patients who would benefit from blocking the actions of thyroid stimulators on the TSHR (1 –4). We now describe the effects of K1-70 in a patient with advanced follicular thyroid cancer (FTC), Graves' disease (GD), and severe Graves' ophthalmopathy (GO).
Materials and Methods
Study patient
A 51-year-old female presented at the Mayo Clinic in October 2014 with progressive weight loss, fatigue, weakness, and a large left thyroid mass with associated left neck adenopathy. She smoked and had GO, significant thyrotoxicosis, and high levels of autoantibodies to the TSHR with high thyroid stimulating antibody (TSAb) activity. Imaging demonstrated a large suspicious 8 cm left thyroid lobe mass with left lateral neck adenopathy (about 3 cm). Following near-total thyroidectomy, pathology confirmed an 8.7 cm widely invasive FTC with soft tissue extension and associated multiple metastatic cervical lymph nodes. A thyrogen-stimulated 123I whole-body scan demonstrated iodine avid metastatic foci within the neck, mediastinum, chest, and skeletal system. She received 250 mCi 131I therapy followed by thyrotropin (TSH) suppression with thyroxine (T4). The patient remained on T4 throughout the course of her disease with suppressed TSH levels and stable T4 and triiodothyronine (T3) levels. There were no significant elevations in T4 and T3 levels throughout the observation period. As T4 was not withdrawn, endogenous T4 and T3 levels could not be assessed. Tumor progression necessitated two further neck operations, debulking thoracotomies for mediastinal disease and a second dose of 131I. Her GO, in the context of ongoing smoking, high TSAb activity, selenium therapy, and multiple doses of 131I, remained active and progressive, with a clinical activity score (CAS) of 6/7 and diplopia, the latter precluding her ability to drive.
The patient's GO and rapidly progressive FTC with local recurrences were postulated to be influenced, at least in part, by her high TSAb activity. Attempts at mitigating the effects of TSAb on her disease with intravenous-immunoglobulin (IV-IG) were unsuccessful. Following IV–IG therapy in December 2016, the CAS was 6/7 with proptosis 21/21 compared with CAS 2/7 and proptosis 20/23 in October 2016. Furthermore, high-dose steroids administered in May 2018 at the time of further 131I therapy showed no clear effects. Genomic evaluations of her nodal disease identified NRAS (Q61R), RBM10 (E770fs*17), and TERT promoter (−124C>T) alterations, which, together with high TSAb activity, were likely associated causally with her advanced disease. Lenvatinib antiangiogenic therapy was initiated in January 2017, ∼2 years after her initial FTC diagnosis, with a partial tumor response, but she had dose-limiting toxicities (fatigue, chest pain, and decreased appetite). A multispecialty Tumor Board review recommended targeting the TSHR with the novel human monoclonal antibody, K1-70, a recombinant immunoglobulin G that is a specific and powerful TSHR antagonist designated for intramuscular (i.m.) or intravenous (i.v.) administration (3,4). A single patient expanded access application was granted by the U.S. Food and Drug Administration for this patient for therapy with K1-70, in combination with systemic antineoplastic therapies. The expanded access use was approved by the local Institutional Review Board.
K1-70 administration
In April 2017, the patient received her first dose of K1-70 (17.6 mg i.m.; Table 1). K1-70 was then administered at 3 weekly intervals with the dose increased to 40 mg i.m. and then to 120 mg i.m. and this blocked her high TSAb activity (Table 1; Fig. 1). Thereafter, doses of K1-70 were adjusted according to measurements of serum TSAb activity with the dose reduced to 60 mg i.m. when serum TSAb became undetectable, and increased to 120 mg i.m. when TSAb activity started to increase (Table 1).
Administration of K1-70 in the Patient with Metastatic Thyroid Follicular Cancer, Graves' Disease, and Graves' Ophthalmopathy
Reproduced with permission of the copyright holder, AV7 Ltd.
Concentration of K1-70 was measured using a PK K1-70 enzyme-linked immunosorbent assay from RSR Ltd. The validated measuring range of the assay was from 10 to 140 ng/mL.
TSI (reference range is ≤1.3) was measured using the Thyretain™ TSI Reporter BioAssay (Quidel).
TSAb activity was measured in a bioassay using Chinese hamster ovary cells stably expressing human TSHR (5). Stimulation >180% relative to the response obtained with a healthy blood donor serum pool was considered positive.
Reported improvement in eye disease.
Eye surgery.
Pause for 123I scan and 131I therapy (300 mCi)
Eye examinations:
Prior K1-70 therapy, December 2016: CAS 6/7, exophthalmometry 21 mm bilaterally.
August 2017: CAS 0-1/7, exophthalmometry 19 mm bilaterally.
October 2018: CAS 0/7, exophthalmometry 18 mm bilaterally.
i.m., intramuscular; i.v., intravenous; NA, result not available; TSAb, thyroid stimulating antibody; TSHR, thyrotropin receptor; TSI, thyroid stimulating immunoglobulin.
Laboratory measurements
Serum TSAb levels were measured at the Mayo Clinic using the Thyretain™ thyroid stimulating immunoglobulin (TSI) Reporter BioAssay (Quidel, San Diego, CA). In addition, a bioassay based on stimulation of cyclic adenosine monophosphate production in TSHR expressing Chinese hamster ovary cells was used at FIRS to measure serum TSAb activity and serum thyroid stimulating blocking activity (RSR™ TSAb and RSR™ TSBAb, respectively) (5).
Serum K1-70 concentrations were measured by enzyme-linked immunosorbent assay from RSR Ltd. Anti K1-70 antibody (ADA) levels were assessed using a Meso Scale Discovery platform. Thyroglobulin (TG) concentrations in serum were measured at the Mayo Clinic using a Beckman Access Thyroglobulin assay run on a UniCel DxI 800.
Results
GO course
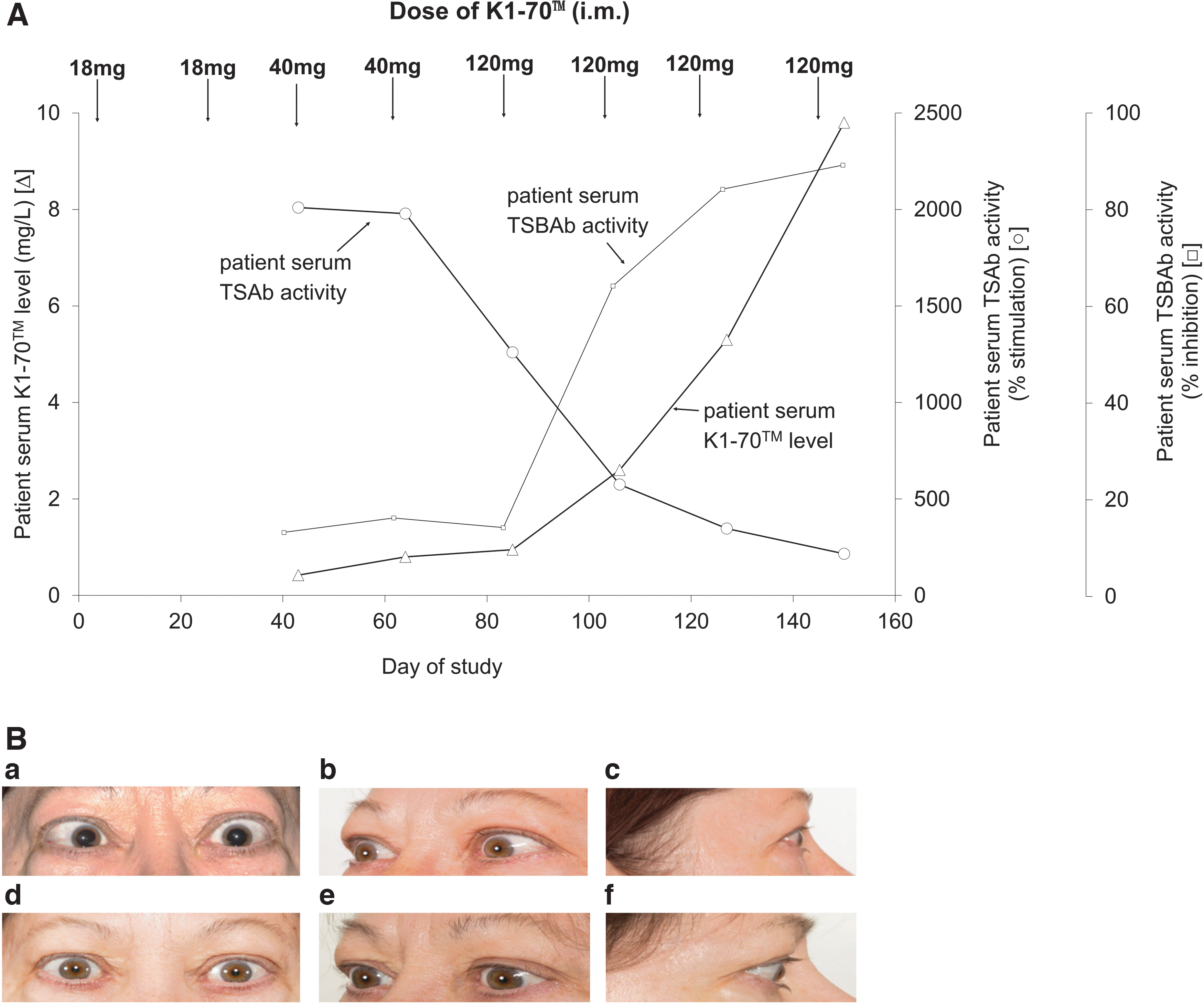
Soon after (within 22 days) the first dose of K1-70, the patient reported improvement in her eye symptoms. She was reassessed by a GO expert in August 2017 (after 4 months K1-70; Table 1), at which time her CAS decreased to 0–1/7 and exophthalmometry reduced from 21 to 19 mm bilaterally despite ongoing smoking. These improvements enabled eye surgery to correct her diplopia and restored her driving ability for the first time in several years (Fig. 1B). GO symptoms remained under control while on K1-70 therapy alone or in combination with lenvatinib. Her GO was stable, while lenvatinib was held for 4 months (July–October 2017; Table 1) due to intolerance, and continued to be stable when lenvatinib was restarted.
In April 2018, after 16 doses of K1-70 every 3 weeks, K1-70 was held before a whole-body 123I scan and thyrogen-stimulated 131I therapy. During the break in K1-70 and before this third dose of 131I, her TSAb activity increased (Table 1) and the patient reported worsening eye symptoms, which required prednisone treatment (20 mg per day orally, decreasing to 5 mg/d). Three weeks after 131I, K1-70 treatment was resumed (June 2018) at 120 mg i.m., her GO improved rapidly and prednisone was discontinued. However, at this stage, serum concentrations of K1-70 were much lower compared with those seen with 120 mg i.m. dosing in the first few months of treatment. Consequently, in August 2018, the injection route was changed to i.v. (Table 1). The reasons why serum concentrations of K1-70 were not reaching the levels observed initially are not clear. Data from stability and compatibility studies available from the drug supplier did not indicate that K1-70 breakdown or adsorption to the drug delivery equipment could be responsible. There was no detectable serum ADA response after multiple (n = 14) K1-70 administrations. However, impaired absorption from the injection site could have been related to lenvatinib therapy. K1-70 serum concentrations were high and the corresponding TSAb activity lowest when the patient was receiving i.m. K1-70 while lenvatinib was on hold (July 2017–October 2017; Table 1).
When assessed by an ophthalmologist in October 2018, her eyes were white and quiet with CAS 0/7, exophthalmometry of 18mm bilaterally with no evidence of any clinical activity (Table 1). GO was stable, despite persistent smoking until January 2019 and thereafter until the patient's death in July 2019 due to acute cardiopulmonary collapse deemed unrelated to K1-70 therapy. In total, the patient received 2755 mg of K1-70 (1675 mg i.m. and 1080 mg i.v.) in 33 three weekly doses (19 i.m and 14 i.v.; Table 1). K1-70 was well-tolerated except for discomfort associated with i.m. injections. There were no adverse effects such as nausea, vomiting, headache, or allergic reactions following either i.m. or i.v. K1-70.
Serum K1-70 and TSAb
As doses of K1-70 increased, concentrations of serum K1-70 increased with the corresponding blocking of endogenous TSAb activity (from 2010% to 216% 150 days after starting the therapy; Fig. 1A). Also, serum thyroid stimulating blocking activity (TSBAb) activity increased accordingly (Fig. 1A). The decrease of TSI index and TSAb activity observed with increasing doses of K1-70 reflected net serum activities of the mixture of endogenous TSAb and administered K1-70. The excess of K1-70 in serum effectively blocked binding of the endogenous TSAb to the TSHR in the bioassays (1 –4,6).
FTC course
Despite multiple neck operations, thoracotomies, and high-dose 131I therapies for iodine-avid FTC (cumulative dose 500 mCi), her disease progressed rapidly. At the time of initiating K1-70 therapy, serum TG levels were 190 ng/mL on 20 mg per day of lenvatinib (Table 1). After 3 months on K1-70 (in July 2017), she reported feeling “very well” and requested a break in treatment with lenvatinib due to intolerance. Lenvatinib was held for 4 months while she continued on K1-70 therapy. Compared with prelenvatinib therapy, attenuation of tumor progression was observed on K1-70 alone and the Mayo Clinic quality-of-life score of 6/10 recorded on lenvatinib alone improved to 9/10. However, during this time, her tumors showed a mixed response. Some tumors were stable or showed slight or mild progression, while some were stable or showed slight regression on K1-70 alone. As some tumor foci showed progression and TG increased on K1-70 alone, lenvatinib was restarted in October 2017 although at reduced doses (10–14 mg/d) in combination with K1-70. Subsequently, the dose of lenvatinib was titrated up to a maximum of 24 mg per day in November 2018.
Her TG level of 800 ng/mL in December 2016, despite 250 mCi radioiodine 3 months prior, fell to 190 ng/mL in April 2017 (Table 1) after initiation of lenvatinib 20 mg daily. Following dose increments of K1-70 from April to September 2017, TG levels remained at about 200 ng/mL (Table 1) despite holding lenvatinib for 3 months due to toxicities, suggesting at least a transient effect of K1-70 itself on the FTC. This corresponded to observed stabilization of foci of disease on imaging described above (data not shown).
Due to the poor tolerability of lenvatinib and disease progression, salvage therapy with 300 mCi 131I was given as per Tumor Board discussion for persistent iodine-avid metastatic foci in May 2018. Unfortunately, although not unexpectedly, there was no evidence of tumor response. In November 2018, on lenvatinib 24 mg daily, 80 mg doses of K1-70 i.v., and detectable TSAb, her TG nadir was 1153 ng/mL (Table 1), suggesting combination therapy synergy on tumor control. Intolerance to lenvatinib continued with fatigue, nausea, vomiting, and loose stools. Due to dose-limiting toxicities leading to therapy interruptions and overall disease progression, treatment was switched in January 2019 to pazopanib, also dose adjusted for toxicities (600 mg/d). Her serum TG levels dropped to 694 ng/mL in June 2019 (Table 1) with stable structural disease. However, the patient developed pulmonary and respiratory symptoms, which responded initially to antibiotics but progressed to lung abscess/cavities leading to an acute cardiopulmonary collapse and death in July 2019.
Discussion
In this single-case report of a patient with advanced FTC and GO in the setting of smoking and high-dose 131I therapies, K1-70 appears to have attenuated, at least in part, the eye disease and maybe the FTC.
This was consistent with our initial hypothesis that blocking the TSHR with K1-70 in combination with established antineoplastic therapies may be helpful in the difficult challenge of controlling disease such as hers (7 –10).
Therapy with K1-70 appeared to attenuate at least some foci of FTC growth. This effect is somewhat analogous to the use of thyroid hormone treatment to reduce TSH levels and attenuate tumor growth in differentiated thyroid cancers (10 –18). However, oncogenic events, in particular RAS and TERT, are dominant drivers of thyroid cancer progression and targeting the TSHR alone is unlikely to have durable control (15,16).
The impact of K1-70 treatment on our patient's eye disease was rapid and persistent. Furthermore, when K1-70 was withdrawn before 131I therapy, her eye disease deteriorated and then resolved quickly after prednisone support and resumption of K1-70.
The observed effect of K1-70 on the patient's GO was most likely due to K1-70 preventing TSAb from stimulating retro-orbital tissue TSHR (17
–19). K1-70 provides an opportunity to directly target the TSHR, which has a key role in the pathogenic pathway in GO (18). The potent TSHR blocking activity of K1-70 suggests that relatively low doses of the drug should be needed to counteract the effects of endogenous TSAb in patients' sera (1,3,4). Results from preclinical studies (3,4) and from a UK phase 1 trial (
Footnotes
Acknowledgments
M. Regina Castro of Division of Endocrinology, Mayo Clinic, Rochester, Minnesota, provided endocrine care. Katarzyna Kabelis of AV7 Limited, Cardiff, United Kingdom, carried out testing and analysis of the samples for TSAb assays. Jane Wilmot of AV7 Limited, Cardiff, United Kingdom, carried out testing and analysis of the samples for K1-70 PK assays. Yang Li of AV7 Limited, Cardiff, United Kingdom, helped with analysis of the results, record keeping, and regulatory aspects. The authors thank Carol James for her excellent assistance in article preparation.
Authors' Contributions
M.R. made substantial contributions to the design of the study, carried out the study, enrolled the patient to the study, assessed and interpreted the results and adjusted the treatment as required, oversaw the regulatory aspects of expanded access use, was the principal investigator on the study, and wrote and critically revised the article for important intellectual content. M.W. made substantial contributions to the design of the study, oversaw the regulatory aspects of expanded access use, and critically revised the article for important intellectual content. A.A.-S. made substantial contributions to data acquisition and analysis, provided and interpreted laboratory results on TSH receptor antibody (TRAb), TSI, and TG, and critically revised the article for important intellectual content. J.C.M. made substantial contributions to the design of the study, the assessment of the effects of treatment, and critically revised the article for important intellectual content. J.G. made substantial contributions to data acquisition and analysis, provided clinical ophthalmology care, and critically revised the article for important intellectual content.
J.S. made substantial contributions to the design of the study, advised on treatment adjustment as required, carried out analysis and interpretation of the samples for TRAb, TSAb, and K1-70 PK assays, and wrote and critically revised the article. S.Y. made substantial contributions to the analysis of patient's samples, carried out testing and interpretation of the results for TRAb and TSAb, and critically revised the article for important intellectual content. *P.S. made substantial contributions to the analysis of patient's samples, carried out testing and interpretation of the results for K1-70 PK assays, and critically revised the article for important intellectual content. J.F. made substantial contributions to the design of the study and data analysis, advised on treatment adjustment as required, and wrote and critically revised the article for important intellectual content.
B.R.S. made substantial contributions to the design of the study and data analysis, advised on treatment adjustment as required, and wrote and critically revised the article for important intellectual content. All authors reviewed and approved the final version to be published and agreed to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Author Disclosure Statement
AV7 Limited provided the K1-70 free of charge for the expanded access use therapy. M.R., M.W., A.A.-S., J.C.M., J.G., and P.S. have no conflict of interest to declare. J.F., J.S., and B.R.S. are Directors of AV7 Limited.
Funding Information
There is no funding information to declare.