
Abstract
Background:
The management of patients with locally advanced or metastatic differentiated thyroid cancer (DTC) that is refractory to radioiodine (RAI) remains a therapeutic challenge. The multi-tyrosine kinase inhibitors (TKIs) sorafenib and lenvatinib have been approved based on phase 3 clinical trials.
Patients and Methods:
We aimed at describing the efficacy and safety of TKI treatment of RAI-refractory DTC in a real-world setting at six German referral centers. One hundred and one patients with locally advanced or metastatic RAI-refractory DTC treated with sorafenib, lenvatinib, and/or pazopanib were included. Progression-free survival (PFS) and overall survival (OS) probabilities were estimated by using the Kaplan-Meier method.
Results:
Ninety-seven of 101 patients had progressive disease before TKI initiation. The median PFS for first-line treatment with sorafenib (n = 33), lenvatinib (n = 53), and pazopanib (n = 15) was 9 (95% confidence interval 5.2–12.8), 12 (4.4–19.6), and 12 months (4.4–19.6), respectively. The median OS for first-line treatment was 37 (10–64) for sorafenib, 47 (15.5–78.5) for lenvatinib, and 34 months (20.2–47.8) for pazopanib. Serious complications (e.g., hemorrhage, acute coronary syndrome, and thrombosis/venous thromboembolism) occurred in 16 out of 75 (21%) patients taking lenvatinib, in 3 out of 42 (7%) patients taking sorafenib, and in 3 out of 24 (13%) patients taking pazopanib.
Conclusions:
Sorafenib, lenvatinib, and pazopanib are effective treatment options in the majority of patients with RAI-refractory DTC. The PFS and six-month survival rate in patients treated with lenvatinib und pazopanib appear to compare favorably with sorafenib in the first-line treatment setting. However, a more advanced disease stage at treatment initiation in sorafenib- and pazopanib-treated patients in the era before TKI-approval and the retrospective nature of this study precludes a direct comparison of TKIs.
Introduction
Multimodal treatment for differentiated thyroid cancer (DTC) includes surgery, radioiodine (RAI) therapy, and thyrotropin suppression with levothyroxine. Patients with evidence of advanced, progressive DTC that is refractory to RAI may require systemic treatment when other palliative local therapeutic strategies are not an option and continuation of active surveillance is no longer justified due to the extent of tumor burden and/or significant disease progression. The multi-tyrosine kinase inhibitors (TKIs) sorafenib and lenvatinib have been approved for patients with advanced and progressive RAI-refractory DTC in 2014 and 2015, respectively, based on two randomized placebo controlled phase 3 clinical trials: A significantly longer median progression-free survival (PFS) of 10.8 months was observed on sorafenib (n = 207) compared with 5.8 months on placebo in the DECISION trial (n = 210; hazard ratio [HR] 0.59; p < 0.0001) (1), and objective response was more frequent on sorafenib (12.2%) compared with placebo (0.5%; p < 0.0001) (1). In the SELECT study (2), median PFS was 18.3 months in the lenvatinib treatment arm versus 3.6 months in the placebo group (HR 0.21, p < 0.001) with a remarkable objective response rate (ORR) of 64.8%, including four complete responses (CR) in the lenvatinib group (p < 0.001) (2). Subgroup analysis demonstrated improved overall survival (OS) with lenvatinib treatment versus placebo in older patients (>65 years), despite higher toxicity (3). Beyond the currently approved TKIs, cabozantinib, pazopanib, sunitinib, and axitinib have been studied in phase 2 clinical trials (4 –8).
In this retrospective study, we aimed at analyzing patient characteristics, parameters reflecting TKI treatment practice and efficacy, as well as TKI treatment of emergent adverse events (TEAEs) in patients with RAI-refractory DTC receiving sorafenib, lenvatinib, and/or pazopanib at six German tertiary care centers.
Patients and Methods
Setting
This registry study was conducted as part of the German Study Group for rare malignant tumors of the thyroid and parathyroid glands. Prospectively and retrospectively collected data were obtained from records of patients diagnosed with RAI-refractory DTC between 1981 and 2019 in six German tertiary care centers and retrieved by trained personnel. All patients provided written informed consent, and the study was approved by the ethics committee of the University of Würzburg (96/13) and subsequently by the ethics committees of all participating centers.
Data acquisition
Eligible patients were adults with histopathological evidence of DTC with RAI-refractory disease who underwent TKI treatment with sorafenib, lenvatinib, and/or pazopanib outside of a clinical trial. Treatment and follow-up was done according to local clinical practice of participating centers. Response was assessed locally by positron emission tomography/computed tomography (PET/CT), CT, magnetic resonance imaging of the liver and bone scintigraphy in analogy to RECIST 1.0 or 1.1 criteria, and with serum thyroglobulin (Tg) testing every three to six months. Bone metastases were not considered as target lesions, except for the new occurrence of bone metastases on treatment. Patients still alive at the last follow-up were censored.
Statistical analyses
The PFS and OS probabilities were estimated by using the Kaplan-Meier method. Potential prognostic factors were evaluated by log-rank tests and performed with stepwise forward selection Cox regression analysis with an inclusion and exclusion threshold of 0.05 for the Wald statistics. For comparison of non-normally distributed data, we used the Mann-Whitney U test. p-Values <0.05 were considered statistically significant. Statistical analyses were performed with SPSS Version 25 (IBM, Chicago, IL).
Results
Clinical characteristics
One hundred and one patients (48 male, 53 female) were included. Baseline clinical characteristics are shown in Table 1. The median follow-up from initial DTC diagnosis was 7.6 years (range 0.4–35), and the median follow-up from the start of TKI treatment was 22 months (range 1–109). In addition to data shown in Table 1, at the time of diagnosis of RAI-refractory disease, 36 patients had local regional lymph node metastases, and 85 patients had distant metastases (brain 2 [n = 56 with cerebral imaging, 4%], mediastinal lymph nodes 33 [39%], lung 78 [92%], liver 10 [12%], pleura 5 [6%], and bone 29 [34%]).
Clinical Characteristics of the Study Cohort
DTC, differentiated thyroid cancer; FTC, follicular thyroid cancer; PDTC, poorly differentiated thyroid cancer; PTC, papillary thyroid cancer; TKI, multi-tyrosine kinase inhibitor; TSH, thyrotropin.
Tumor-specific therapy
Two patients underwent hemithyroidectomy and 99 underwent total thyroidectomy as initial therapy. Before TKI treatment, all patients had undergone RAI therapy. The median time between primary surgery and first RAI therapy was 31 days. The median RAI activity was 17.5 GBq (range 0.6–91.2). Two patients received redifferentiation therapy by using dabrafenib and 16 with retinoic acid or rosiglitazone. The treatment for local recurrence before TKI treatment was surgery in 36 patients, and external beam radiation to the neck in 19 patients. The treatment of distant metastases included surgery in 35, external beam radiation in 37, and cytotoxic chemotherapy in 10 patients (pemetrexed/paclitaxel, carboplatin/paclitaxel, and docetaxel/cisplatin).
Treatment characteristics with TKI in first-line treatment are summarized in Table 2. In total, 75 patients received lenvatinib, 46 sorafenib, and 24 pazopanib regardless of the treatment line (patients who received several TKIs were considered multiple times). Sixty-two patients received one TKI, 28 received two TKIs, 9 received three TKIs, 1 received four TKIs, and 1 received 5 TKIs consecutively. The reasons for not giving a second-line treatment were: persistent partial remission (PR) or stable disease (SD) on first-line treatment in 31 patients (50%), death in 23 patients (37%), patient refusal of recommended second-line treatment in 2 patients (3%), a switch to palliative care in 2 patients (3%), lost to follow-up in 2 patients (3%), and advanced patient age in 1 patient (2%).
Therapeutic Characteristics of First-Line Treatment
EMA, European Medicines Agency.
The median age at TKI initiation was 63 years and the median time between initial diagnosis and TKI initiation was 53 months (range 1–405) or, in patients with distant metastases at initial diagnosis, 50 months (range 1–405). Indications for TKI treatment were progressive disease (PD) in 97 patients. In one patient, treatment was started with the aim of inducing shrinkage of metastatic lesions to enable resection. The reason for initiating TKI treatment was unavailable in three patients. At the data cutoff, 34 (34%) patients were still receiving TKI treatment, 7 (7%) patients were undergoing active surveillance, 44 (44%) patients had died, and 16 (16%) patients were lost to follow-up.
Sorafenib as first-line treatment
The characteristics and efficacy data of first-line treatment with sorafenib are described in Table 3.
Treatment Characteristics and Response Rates of First-Line Treatment
Patients who received more TKIs were considered multiple times.
CI, 95% confidence interval; CR, complete response; NR, not reached; OS, overall survival; PFS, progression-free survival; PR, partial remission; SD, stable disease.
At the time of sorafenib initiation, 18 (55%) patients had locoregional lymph node metastases, and 32 (97%) patients had distant metastases (brain 4 [n = 23 with cerebral imaging, 17%], mediastinal lymph nodes 18 [55%], lung 32 [97%] [100%], liver 4 [12%], bone 14 [42%]). The median time between the primary diagnosis of DTC and sorafenib initiation was 53 months (range 2–405). Thirty-three patients (32%) received sorafenib as first-line treatment. The median PFS from sorafenib initiation was 9 (95% confidence interval [CI] 5.2–12.8; Fig. 1A
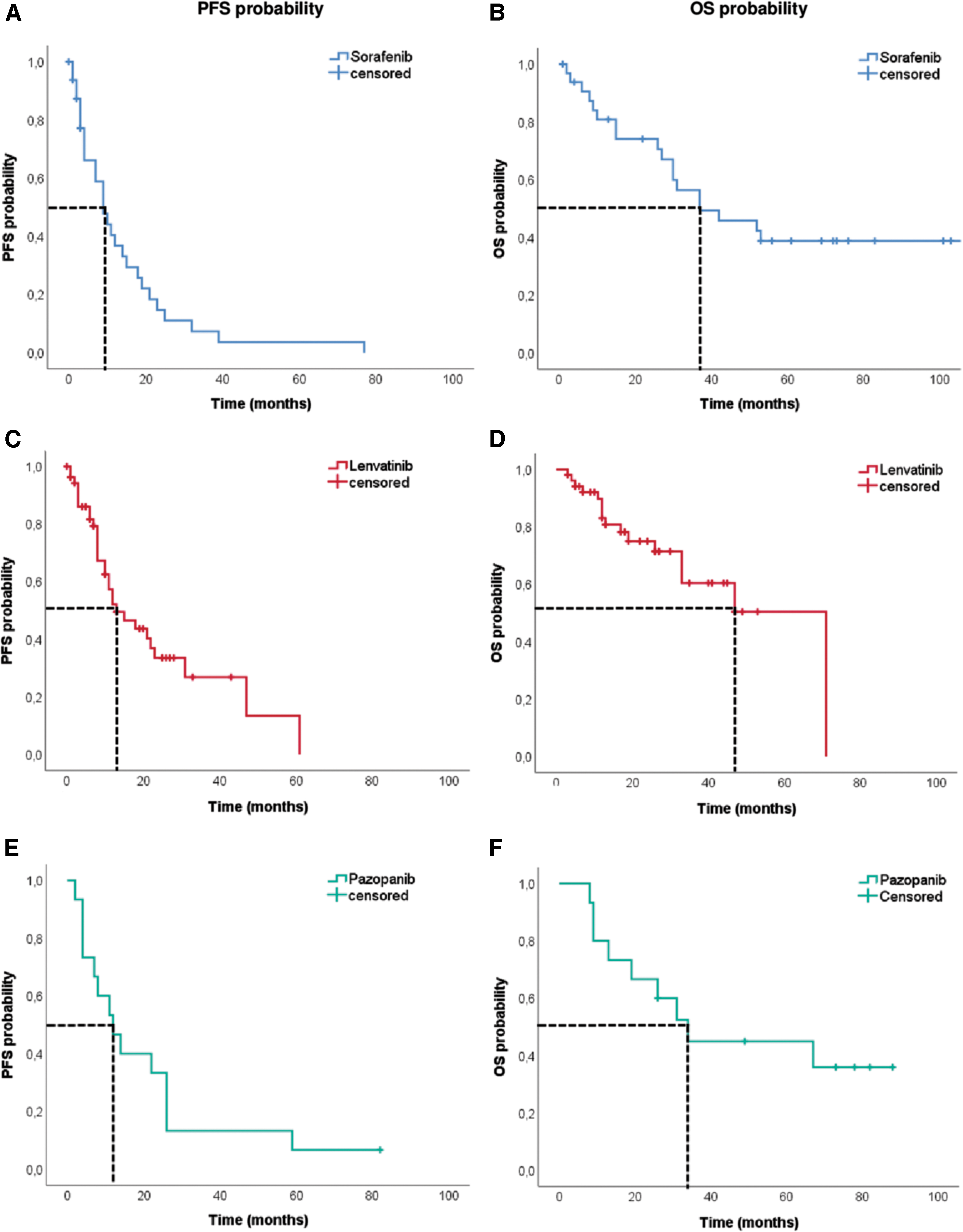
PFS and OS (in months) in patients taking sorafenib (n = 33), lenvatinib (n = 53), and pazopanib (n = 15) as first-line treatment. (
Lenvatinib as first-line treatment
At the time of lenvatinib treatment initiation, 28 (53%) patients had locoregional lymph node metastases, and 50 (94%) had distant metastases (brain 3 [n = 43 with cerebral imaging, 7%], mediastinal lymph nodes 26 [49%], lung 47 [89%], liver 10 [19%], bone 25 [47%]). The median time between primary diagnosis of DTC and lenvatinib initiation was 37 months (range 1–402). Fifty-three patients (52% of the whole patient cohort; 98% of the patients who were started on TKI after European Medicines Agency [EMA] approval of lenvatinib) received lenvatinib as first-line treatment. The median PFS on lenvatinib was 12 (CI 4.4–19.6; Fig. 1C) and OS was 47 months (CI 15.5–78.5; Fig. 1D). Fourteen (26%) patients received lenvatinib for ≥24 months.
Pazopanib as first-line treatment
At the time of pazopanib treatment initiation, 6 (40%) patients had locoregional lymph node metastases, and 15 (100%) distant metastases (brain 1 [n = 12 with cerebral imaging, 8%], mediastinal lymph nodes 9 [60%], lung 15 [100%], liver 4 [27%], bone 3 [20%]). The median time between primary diagnosis of DTC and pazopanib initiation was 58 months (range 20–209). Fifteen (15%) patients received pazopanib as first-line treatment: 14 out of 15 patients before EMA approval of sorafenib and 15 out of 15 patients before EMA approval of lenvatinib in June 2015, and 1 patient after EMA approval of sorafenib. PFS was 12 (CI 4.4–19.6; Fig. 1E), and OS was 34 months (CI 20.2–47.8; Fig. 1F). Six (40%) patients received pazopanib for ≥24 months, and 10 (67%) discontinued treatment due to PD.
Biochemical response of first-line treatment
Serum Tg levels showed a significant reduction in patients treated with sorafenib, lenvatinib, and pazopanib (p = 0.002, p < 0.001, p = 0.035). Eight (24%) patients treated with sorafenib, 37 (70%) treated with lenvatinib, and 8 (53%) treated with pazopanib showed a reduction in serum Tg levels ≥60%.
Efficacy of second-line treatment
Efficacy data of second-line treatment are summarized in Supplementary Table S1. For second-line treatment, median PFS was 4 (CI 2.5–5.5), 15 (CI 9.4–20.6), and 40 months (CI 0–89.4) for sorafenib, lenvatinib, and pazopanib, respectively (Fig. 2A, C, E) and median OS was 32 (CI 27.2–36.8), and 30 (CI, not reached [NR]) months for sorafenib and lenvatinib, respectively. The median OS was NR for pazopanib-treated patients (Fig. 2B, D, F).

PFS and OS (in months) in patients taking sorafenib (n = 11), lenvatinib (n = 20), and pazopanib (n = 5) as second-line treatment. (
Factors associated with PFS and OS end points
The association of prognostic features with PFS and OS is summarized in Tables 4 and 5. The PFS in sorafenib-treated patients was significantly negatively associated with the presence of distant metastases at the time of diagnosis of RAI-refractory DTC and the presence of bone metastases at the time of TKI initiation, which were confirmed in multiple step-wise Cox regression analysis.
Association of Different Baseline Features with Progression-Free Survival and Overall Survival by Log-Rank Test
Bold values are statistically significant.
In multiple Cox regression with stepwise forward selection of the potential prognostic factors such as age (≤/> 60 years), sex, tumor entity (PTC, FTC, PDTC), distant metastases (absent, present), lung metastases (absent, present), liver metastases (absent, present), and bone metastases (absent, present) as potential prognostic factors, variables that were relevant in univariate analyses were confirmed as single independent prognostic variables for PFS with sorafenib, and for PFS and OS with lenvatinib.
RAI, radioiodine; Tg, serum thyroglobulin.
Association of Different Treatment Features with Progression-Free Survival and Overall Survival by Log-Rank Test
Bold values are statistically significant.
In multiple Cox regression with stepwise forward selection of the potential prognostic factors such as age (≤/> 60 years), sex, tumor entity (PTC, FTC, PDTC), distant metastases (absent, present), lung metastases (absent, present), liver metastases (absent, present), and bone metastases (absent, present) as potential prognostic factors, variables that were relevant in univariate analyses were confirmed as single independent prognostic variables for PFS with sorafenib, for PFS and OS with lenvatinib, and for PFS with pazopanib.
In lenvatinib-treated patients, a significantly longer PFS was observed for papillary thyroid cancer compared with follicular thyroid cancer and poorly DTC. Baseline Tg levels below the median of 971.5 ng/mL and absence of liver metastases at TKI initiation showed a significantly longer PFS. The OS was significantly positively associated with the presence of lung metastases at the time of TKI initiation. Tumor histology and liver metastases at TKI initiation were confirmed as independent prognostic variables adversely affecting PFS, and lung metastases were confirmed as a positive prognostic variable for OS after multivariable adjustment.
Pazopanib-treated patients who had baseline Tg levels below the median of 130 ng/mL had a significantly longer OS, which was, however, not significant after multivariable adjustment.
Safety and tolerability
Fourteen (30%) patients receiving sorafenib, 23 (31%) receiving lenvatinib, and 4 (17%) receiving pazopanib discontinued treatment due to TEAEs.
In sorafenib-treated patients, the most frequently reported drug-related TEAEs were loss of appetite/weight (46%), diarrhea (43%), and hand–foot syndrome (37%). In lenvatinib-treated patients, the most frequently reported drug-related TEAEs were loss of appetite/weight (49%), hypertension (45%), fatigue (44%), and diarrhea (44%). In pazopanib-treated patients, the most frequently reported drug-related TEAEs were diarrhea (42%), fatigue (29%), and loss of appetite/weight (25%).
Serious complications, including hemorrhage, acute coronary syndrome, and thrombosis/venous thromboembolism, occurred in 16 out of 75 (21%) lenvatinib-treated patients, in 3 out of 42 (7%) sorafenib-treated patients, and in 3 out of 24 (13%) pazopanib-treated patients. Aerodigestive fistula formation did not occur in our cohort.
One (1%) lenvatinib-treated patient developed posterior reversible encephalopathy syndrome. Sixteen (21%) patients taking lenvatinib were hospitalized due to TEAEs, and 2 (3%) patients taking lenvatinib had TEAEs resulting in death. Death-related adverse events included acute respiratory failure induced by sepsis and acute coronary syndrome. The hospitalization rate was 4% for patients receiving sorafenib and pazopanib, respectively. None of the patients treated with sorafenib and pazopanib died because of a TEAE.
Discussion
Here, we studied real-world clinical data from patients with metastatic or locally advanced RAI-refractory DTC who received treatment with sorafenib, lenvatinib, and/or pazopanib outside the framework of a clinical trial. The results confirm that TKIs are effective treatment options in the majority of patients with RAI-refractory DTC, and we found response rates and PFS to be comparable with published data sets with some remarkable differences.
Our study cohort is one of the largest of TKI treatment in RAI-refractory DTC, but it is limited by its retrospective nature, small patient numbers in the different subgroups, lack of systematic follow-up, heterogeneity of patient management, and the evaluation of imaging findings by different radiologists and/or nuclear medicine specialists.
The efficacy of sorafenib in our retrospective analysis is in accordance with previously reported results; the median PFS was 9 versus 10.8 months in the phase 3 trial (DECISION trial) and 9.7 months in real-world data from Korea (1,9). A higher proportion of papillary thyroid cancer in the series by Cheng et al. and Oh et al. (more than 70% and 68%, respectively vs. 31% in our cohort) and a longer median duration between initial DTC diagnosis and sorafenib treatment initiation (6.5 and 9 vs. 4.4 years in our cohort) suggest the presence of patients with a more aggressive clinical course in our cohort (10,11). Longer median OS of 37 months in comparison to 28.9 months in the Chinese real-world data may be related to a higher fraction of patients with lung and bone metastases (88.9% and 31.9%).
In comparison to the DECISION study, we observed a higher ORR (1), which might be caused by a lack of central review, while safety and tolerability are consistent with prior studies (1,9,10). The rate of treatment discontinuation due to TEAEs (30%) in our analysis was higher than in the phase 3 study (18.8%) and the published real-world data (1,9 –11).
The PFS of 12 months in lenvatinib-treated patients is comparable to some studies (12 –14) but shorter than in the SELECT trial and studies from Asia (2,15,16). One case with CR and 36 with PR were observed. The seemingly more favorable outcome of lenvatinib-treated patients in comparison with the sorafenib-treated patients may be explained by the lack of systemic treatment approaches before the approval of sorafenib and therefore a rather late start of sorafenib treatment, which is confirmed by the longer time period between initial diagnosis and TKI treatment in sorafenib-treated patients (4.4 years) compared with lenvatinib-treated patients (3.1 years). On the other hand, the shorter median time between the diagnosis and start of lenvatinib could also be due to a more aggressive course of disease in lenvatinib-treated patients.
The TEAE profile in lenvatinib-treated patients is consistent with the SELECT study findings. It must be noted that an increased risk for thrombotic events is a major concern of antiangiogenic therapies (17). Accordingly, our data showed chest pain/myocardial infarction and thrombosis/venous thromboembolism in 13% of patients taking lenvatinib and in 4% of sorafenib- and pazopanib-treated patients, respectively.
Fifteen patients received first-line treatment with pazopanib, and we found a comparable response as in previous phase 2 clinical trials (5,18): We found CR in 7%, PR in 53%, and SD for ≥24 weeks in 13% of patients, which translated into a PFS of 12 months. While the retrospective study design precludes a formal comparison of efficacy data, the high ORR of 60% appears to compare favorably with sorafenib (18%) and is similar to that in lenvatinib-treated patients (70%), although the small number of patients is a limitation.
Further, in comparison to sorafenib and lenvatinib, pazopanib-treated patients showed a median duration of treatment of 19 versus 8 months for sorafenib and versus 12 months for lenvatinib. The proportion of patients with dose reduction was 40% for pazopanib versus 48% for sorafenib and 58% for lenvatinib. The proportion of discontinuation due to TEAEs was 17% for pazopanib versus 30% for sorafenib and 31% for lenvatinib.
Comparing sorafenib, lenvatinib, and pazopanib, our efficacy data seem to favor first-line treatment with lenvatinib and pazopanib. However, it has to be considered that patient populations and time of treatment initiation differed, as outlined earlier. Collectively, our data underscore the potential value of pazopanib in patients with advanced RAI-refractory DTC.
In second-line treatment, we did not find any objective response in sorafenib-treated patients while pazopanib resulted in PR in 60% and lenvatinib in 30% of patients, consistent with results by Oh et al., who found PR rate in 20% of lenvatinib-treated patients (11). In this context, it should be noted that cabozantinib, which has been already approved for the treatment of advanced medullary thyroid cancer, has demonstrated significant improvement in PFS in patients with RAI-refractory DTC (11 months for cabozantinib vs 1.9 months for placcebo) who have progressed after up to two prior vascular endothelial growth factor receptor-targeted therapies versus placebo, meeting the primary endpoint of the COSMIC-311 clinical trial (19).
Interestingly, we found significantly shorter PFS in patients with bone metastases treated with sorafenib but not lenvatinib and pazopanib. This is not consistent with the subgroup analyses in the DECISION trial and data from Korea, showing no difference in the therapeutic efficacy of sorafenib (1,11). Further, in lenvatinib-treated patients, PFS was significantly associated with the presence of liver metastases at TKI initiation with a shorter PFS in patients with versus those without liver metastases. Based on data from Gianoukakis et al. (20) and in line with findings by Brient et al. (21), which showed a shorter median duration of response in lenvatinib-treated patients with liver metastases, the 2019 European Thyroid Association Guidelines for the treatment and follow-up of advanced RAI-refractory thyroid cancer stated that liver metastases might be less responsive than other metastatic sites (20,22). At variance, an association between location of metastases and efficacy of TKIs had not been identified in the DECISION and SELECT trials (1,2,22).
It is noteworthy that papillary thyroid cancer was associated with a significantly more favorable PFS compared with follicular thyroid cancer or poorly DTC in patients treated with lenvatinib. Since there is only one study with a similar result (23), our finding requires confirmation by other studies, in particular given the lack of data on driver mutations in the study cohort. Further, PFS in lenvatinib-treated and OS in pazopanib-treated patients were significantly influenced by baseline serum Tg levels, showing baseline serum Tg levels < median to be associated with a favorable outcome compared with patients with a baseline serum Tg level ≥ median. While this may suggest a higher therapeutic efficacy when treatment is started at earlier tumor stages, Song et al. did not find any association between PFS and median baseline Tg or a reduction in Tg levels ≥60% with treatment response to lenvatinib (16). Although the clinical value of Tg is well accepted in the management of patients with DTC (24), changes in Tg during treatment with sorafenib, lenvatinib, and pazopanib did not show association with response to treatment in our cohort. Werner et al. found serum Tg fluctuations to be a frequent phenomenon in patients with RAI-refractory DTC undergoing TKI treatment with lenvatinib, which does not necessarily reflect structural change in tumor size or volume (25). Nevertheless, a continuous rise in Tg should raise suspicion: Patients with true PD demonstrate a continuous rise in Tg, whereas patients with truly controlled disease present with oscillating tumor markers after an initial nadir without PD (25).
In summary, we demonstrate that sorafenib, lenvatinib, and pazopanib are effective drugs in patients with DTC with progressive RAI-refractory disease in the real-world setting, with lenvatinib and pazopanib potentially having superior efficacy. It must be noted, though, that patients with sorafenib and pazopanib were treated at a later stage of disease due to limited therapy options before TKI approval. However, the higher rate of hospitalization and deaths due to TEAEs in lenvatinib-treated patients need to be considered when comparing efficacy data. In case of PD, second-line treatment with either lenvatinib or pazopanib resulted in a considerable PR rate in contrast to sorafenib. Collectively, our data suggest considering pazopanib as a treatment alternative in later lines of treatment in compassionate use given its relatively favorable toxicity profile and substantial ORR. Nevertheless, our study design precludes a definitive efficacy and safety comparison between the different TKIs.
Footnotes
Author Contribution Statement
V.F.K.: data acquisition, analysis, and interpretation; drafted the article; and designed the tables/figures. E.B., P.A., G.-L.W., A.P., J.M.K., B.S., C.T.F., and S.A.: data acquisition, critical revision, and final approval of the article. M.L., C.L., N.R., M.C.K., M.S., and A.T.: supervising physician, critical revision, and final approval of the article. E.H.: methodological and statistical advice, critical revision, and final approval of the article. M.F.: critical revision and final approval of the article. M.K. and C.S: supervising physician, involved in planning, and supervised the work, critical revision, and final approval of the article.
All authors discussed the results and commented on the article.
Author Disclosure Statement
V.F.K. has received honoraria for lectures and travel expenses from Novartis and Sanofi. M.C.K. has received honoraria from Eisai, Novartis, Ipsen, Bayer Health, Pharmtrace, Liam GmBH, Lilly, Exelixis, Onkowissen.de, and Sanofi Genzyme; for Consulting or Advisory (Board) role from Eisai, Ipsen, Bayer, and Lilly; for research funding from GE Healthcare, Sanofi, Exelixis, and Lilly; and for travel, accommodation, and expenses from Sanofi Genzyme, Eisai, Ipsen, Bayer, Novartis, and Pharmtrace. S.A. has received honoraria for lectures and travel expenses from Sanofi. M.S. has received honoraria for advisory boards and lectures from Sanofi, Eisai, and Ipsen. M.K. has received institutional research support from Ipsen, Loxo Oncology, and Lilly; travel support from Eisai, Ipsen, HRA Pharma, MCI Germany, and Lilly, Ipsen; honoraria for lectures from Eisei, Lilly, and MSD; and consultancy honoraria from Lilly and Bayer. C.S. has received honoraria for advisory boards and lectures from Ipsen, Lilly, Bayer, Eisai, and Genzyme. E.B., P.A., G.-L.W., A.P., M.L., J.M.K., C.L., B.S., N.R., C.T.F., E.H., A.T., and M.F. have no competing financial interests.
Funding Information
This work was supported by the Deutsche Forschungsgemeinschaft, Priority Programme SPP1629 (SP 581/6-2) and Collaborative Research Center SFB 824 (project C8), and by the “Förderprogramm Forschung und Lehre (FöFoLe), Reg.-Nr. 1031” of the medical faculty of the LMU Munich.
The German Study Group for Rare Malignant Tumors of the Thyroid and Parathyroid Glands received unrestricted grant support from Bayer and Eisai.
Supplementary Material
Supplementary Table S1