
Abstract
Background:
While numerous factors determine prognosis in papillary thyroid carcinoma (PTC), distant metastasis (M1) represents one of the most dire. Escalating nodal burden and aggressive histology may contribute to higher metastatic risk, but this relationship is poorly defined and challenging to anticipate. We evaluate the predictive impact of these histological features on predicting distant metastases at initial presentation.
Methods:
Univariate and multivariable logistic regression models of conventional and aggressive thyroid cancer variants (well-differentiated papillary thyroid carcinoma [WDPTC], diffuse sclerosing variant [DSV], tall cell variant [TCV], poorly differentiated thyroid cancer [PDTC], and anaplastic thyroid carcinoma [ATC]) identified via U.S. cancer registry data were constructed to determine associations between M1 status and quantitative nodal burden. Associations between metastatic lymph node (LN) number and M1 disease were modeled using univariate and multivariable logistic regression with interaction terms, as well as a linear continuous probability model.
Results:
Overall, M1 prevalence at disease presentation was 3.6% (n = 1717). When stratified by subtype, M1 prevalence varied significantly by histology (WDPTC [1.0%], DSV [2.3%], TCV [4.1%], PDTC [17.4%], ATC [38.4%] [p < 0.001]). For WDPTC, M1 prevalence escalated with metastatic LN number (0 LN+ [0.5%], 1–5 LN+ [2.0%], 6–10 LN+ [3.4%], >10 LN+ [5.5%] [p < 0.001]) and LN ratio (p < 0.001). A statistically significant interaction was observed between histology and increasing nodal burden for M1 risk. On multivariable analysis, each successive metastatic LN conferred increased M1 risk for WDPTC (odds ratio [OR] 1.06 [1.05–1.08], p < 0.001) and TCVs (OR 1.04 [1.02–1.07], p < 0.001). In contrast, other aggressive variants had a higher baseline M1 risk, but this did not vary based on the number of positive LN (DSV, OR 1.02 [0.95–1.10], p = 0.52; PDTC, OR 1.00 [0.98–1.02], p = 0.66; ATC, 1.00 [0.98–1.02], p = 0.97).
Conclusions:
Progressive nodal burden independently escalates the risk of distant metastasis in WDPTC and TCVs of PTC. Conversely, aggressive variants such as PDTC and ATC have substantial M1 risk at baseline and appear to be minimally affected by metastatic nodal burden. Consideration of these factors after surgery may help tailor clinical decision-making for treatment and surveillance. Further studies are warranted to calibrate the ideal management approach for these higher risk patient groups.
Introduction
The incidence of papillary thyroid carcinoma (PTC) has continued to outpace that of other malignancies worldwide (1 –3), yet it is widely acknowledged that mortality risk remains low (4). Such high cure rates have led to treatment deintensification across all arms of treatment (5). Nonetheless, a considerable percentage of PTC (10–15%) is deemed high risk (6,7): recognition of these aggressive subtypes may profoundly affect management.
Risk factors that influence prognosis include advanced age, low radioactive iodine (RAI) avidity, and large tumor size (5). Yet distant metastasis appears to be the main driver affecting cancer-specific survival. Prior reports have estimated 5-year overall survival in patients with M1 disease to be less than 50% (8 –11). Anticipating distant metastasis at presentation is thus a key challenge for clinicians, who must parse high-risk variants from an otherwise low-risk population.
Regional lymph node (LN) burden in PTC, often identified by radiological or pathological means, may be an intuitive surrogate or marker for distant metastasis (12,13). Although increasing metastatic LN number itself has a mixed role in staging and prognosis, it may signal distant spread as a natural gateway to other sites. Similarly, aggressive PTC histologies may also predict for M1 disease: their less differentiated biology corresponds to aberrant signaling pathways that resist RAI and enhance potential for metastasis (14 –16). Both factors remain understudied as proxies for metastatic risk, yet are ideal for large-scale analysis given that they are known after initial management with surgery. We investigate the independent significance of LN burden and histological subtype on distant metastasis prevalence.
Methods
Selection criteria
Data were extracted from the National Cancer Database (NCDB) (Version 2017 Participant User File), a hospital-based registry that captures 70% of all cancers in the United States. This study was deemed exempt from the Cedars-Sinai Institutional Review Board review.
Patients with well-differentiated papillary thyroid carcinoma (WDPTC) (topographic identifier C73) were selected with the following codes: papillary carcinoma NOS (8050), papillary carcinoma of thyroid (8260), follicular variant of PTC (8340), papillary microcarcinoma (8341), encapsulated papillary carcinoma (8343) (Supplementary Fig. S1). Morphological subtypes recognized by the World Health Organization and selected for analysis included diffuse sclerosing variant (DSV) (8350), tall cell variant (TCV) (8344), and poorly differentiated thyroid cancer (PDTC) (8020). Insular variant (8337) was included as a subtype of PDTC. For comparison, anaplastic thyroid carcinoma (ATC) (8021) cases were included. WDPTC cases with grade of “poorly differentiated” or “undifferentiated/anaplastic” were redesignated as PDTC and ATC, respectively.
Patients were excluded if missing the following data elements: unknown diagnostic confirmation, missing tumor size, unknown regional LN data, unknown T-stage, unknown N-stage, unknown follow-up, or unknown vital status. Cases were also omitted if missing Charlson–Deyo comorbidity score, great circle distance, academic facility, or income data. NCDB has documented M0 versus M1 status since inception of the database. All years (2004–2016) were included to broadly capture overall M1 prevalence. For metastatic site (e.g., lung, liver, bone), the NCDB used the Collaborative Stage (CS) Data Collection System between the years 2010–2015. Other years were not consistently captured, and as such the specific sites in these cases are listed as unknown.
Lymph node ratio (LNR) was calculated for comparison to metastatic LN number. To minimize ratio distortion and filter out excisional node biopsies, a minimum threshold of 5 LN examined was used, based on prior American Thyroid Association (ATA) Surgical Affairs Committee findings of recurrence risk (17), and the 2015 ATA Guidelines distinction of what constitutes low risk compared with intermediate risk (5).
Statistical methods
Baseline patient demographics were stratified by PTC histology and compared using the one-way analysis of variance, Kruskal–Wallis test, and the Pearson's chi-square test for continuous and categorical variables as appropriate. Univariate and multivariable logistic regression was used to assess the association of increasing LN burden on distant metastasis across PTC histology. To determine if the effect of increasing LN burden differed across PTC histologies, the multivariable model included an LN burden × histology interaction term while adjusting for all patient and clinical characteristics as presented in Table 1. The multivariable model was then used to visualize the probability of distant metastasis with increasing LN burden by PTC histology based on a reference population (most common) selected from our cohort: academic institution, east region, age 56 years, white race, private insurance, income $38,000−$63,000, medium educational attainment (7 − 20.9%), great circle distance <10 miles, Charlson–Deyo score 0, tumor size 0–1 cm, surgery total thyroidectomy, no extrathyroidal extension, no RAI or radiation therapy, and no chemotherapy (18).
Univariate and Multivariable Analyses of Distant Metastasis in Papillary Thyroid Cancer Variants and Anaplastic Thyroid Carcinoma
Included as interaction term.
ATC, anaplastic thyroid carcinoma; CI, confidence interval; DSV, diffuse sclerosing variant; EBRT, external beam radiation therapy; ETE, extrathyroidal extension; LN, lymph node; OR, odds ratio; PDTC, poorly differentiated thyroid cancer; RAI, radioactive iodine; TCV, tall cell variant; WDPTC, well-differentiated papillary thyroid carcinoma.
All statistical analyses were performed using R software package version 4.0.3. A two-sided test and a p-value <0.05 were considered significant.
Results
Altogether, 47,844 cases were evaluated, including WDPTC (n = 39,307), DSV (n = 463), TCV (n = 3752), PDTC (n = 1915), and ATC (2407) (Supplementary Fig. S1). Across these subgroups, 57.5% were T1, while 74.6% were N0 (Supplementary Table S1). The mean number of LN examined was 5.0 (standard deviation [SD] 11.2), while the mean number of metastatic LN was 2.0 (SD 4.6). The prevalence of distant metastasis (M1) at disease presentation was 3.8% (n = 1717).
When stratified by subtype, M1 prevalence varied significantly (WDPTC [1.0%], DSV [2.3%], TCV [4.1%], PDTC [17.4%], ATC [38.4%] [p < 0.001]) (Supplementary Table S1) (Fig. 1). When examining only N0 patients, M1 prevalence exhibited a similarly wide spectrum (WDPTC [0.5%], DSV [0.7%], TCV [1.8%], PDTC [11.0%], ATC [27.4%]) (p < 0.001). For Nx patients, M1 distribution was also similar (WDPTC [1.8%], DSV [11.1%], TCV [11.5%], PDTC [42.1%], and ATC [58.7%]). Specifically for WDPTC, site distribution of M1 disease was predominantly lung (35.2% of M1 cases, or 62.9% of known M1 sites) followed by bone (18.1% of M1 cases, or 32.4% of known M1 sites). Multisite disease was relatively uncommon (4.1% of M1 cases, or 7.6% of known M1 sites). Baseline characteristics of M1 patients who did not undergo surgery are listed in Supplementary Table S2.

Prevalence of distant metastasis, stratified across papillary thyroid cancer subtypes. Site percentages include both single and multifocal metastatic cases, and as such each subtype does not add up to 100%. Other/unknown sites are documented M1 disease without specified location. DSV, diffuse sclerosing variant; PDTC, poorly differentiated thyroid cancer; WDPTC, well-differentiated papillary thyroid carcinoma. Color images are available online.
On multivariable analysis, aggressive histology was a strong predictor for M1 risk. However, a statistically significant interaction was observed between the associations of histology and increasing nodal burden with M1 risk (Table 1). Specifically, pairwise tests of interaction for WDPTC versus other histologies showed no significant difference for DSV (p = 0.30) or TCVs (p = 0.16) in terms of the relationship between nodal burden and M1 risk, but significant differences for WDPTC versus PDTC (p < 0.001) and ATC (p < 0.001).
On multivariable analysis, each successive metastatic LN conferred increased M1 risk (odds ratio [OR] per LN 1.06 [1.05–1.08], p < 0.001) for WDPTC. Using LN ratio, each 0.1 unit increase for WDPTC showed similar escalation (OR per 0.1 LNR increase 1.11 [1.05–1.17], p < 0.001). Increasing M1 risk with increasing nodal burden was also observed for TCV (OR per LN 1.04 [1.02–1.07], p < 0.001). In contrast, there was no increase in M1 risk with increasing nodal burden for other aggressive histologies (DSV, OR per LN 1.02 [0.95–1.10], p = 0.52; PDTC, OR per LN 1.00 [0.98–1.02], p = 0.66; ATC, OR per LN 1.00 [0.98–1.02], p = 0.97) (Fig. 2).
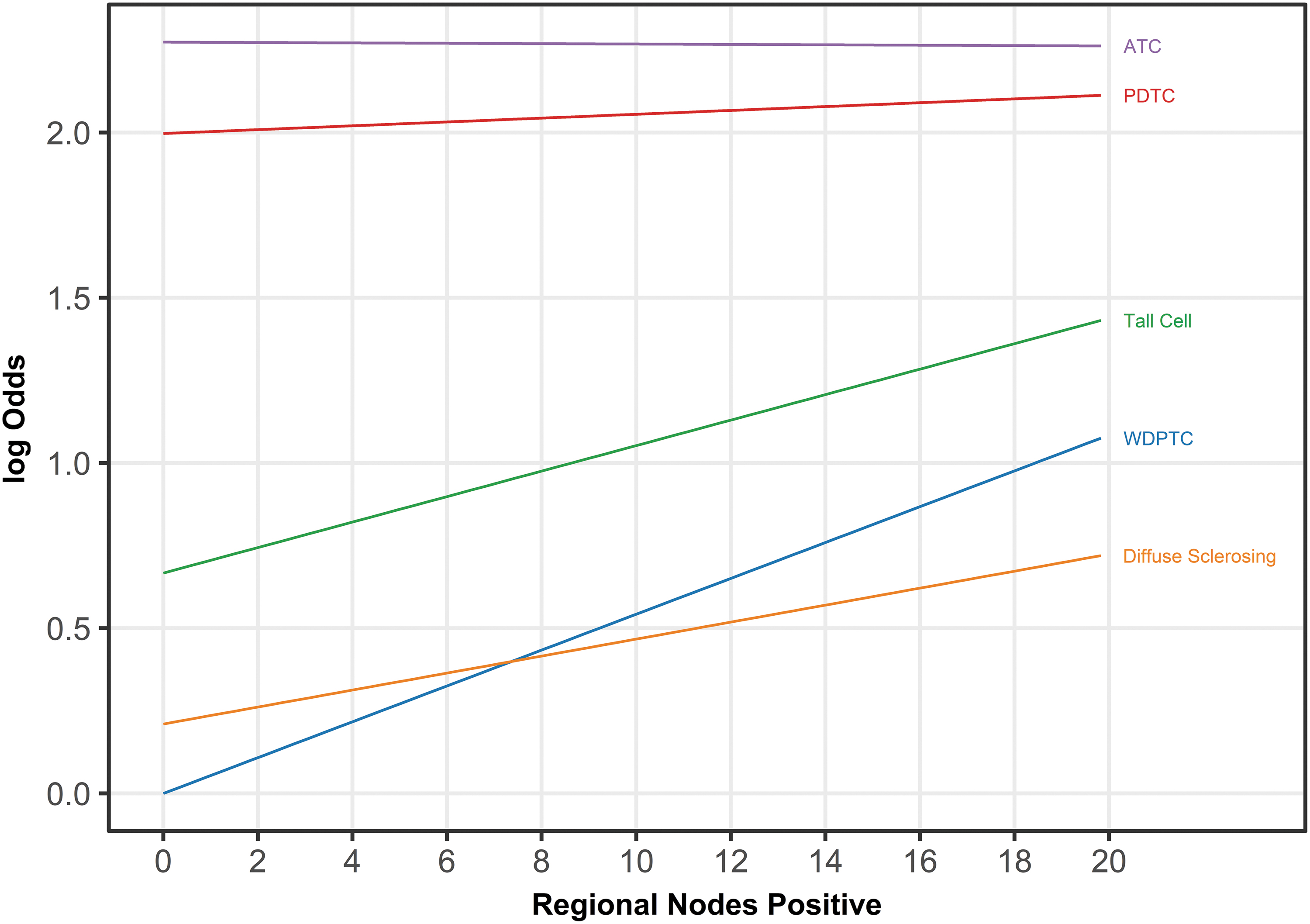
Log odds change for distant metastatic risk for every 1 unit increase in metastatic LNs, stratified by thyroid cancer histology and based on the multivariable model and fitting an interaction between number of metastatic LNs with histology. ATC, anaplastic thyroid carcinoma; LN, lymph node. Color images are available online.
Specifically for WDPTC, M1 risk showed significant escalation with increasing nodal burden when stratified by metastatic LN groups (0 LN+ [0.5%], 1–5 LN+ [2.0%], 6–10 LN+ [3.4%], >10 LN+ [5.5%] [p < 0.001]) (Fig. 3). Applying 10 LN+ as a threshold, the M1 prevalence was 1.1% (0–10 LN+) compared with 5.5% (>10 LN+) (p < 0.001). Using a reference WDPTC population, the probability of M1 was found to have a hyperbolic relationship with escalating metastatic LN number and for LN ratio (Fig. 4).
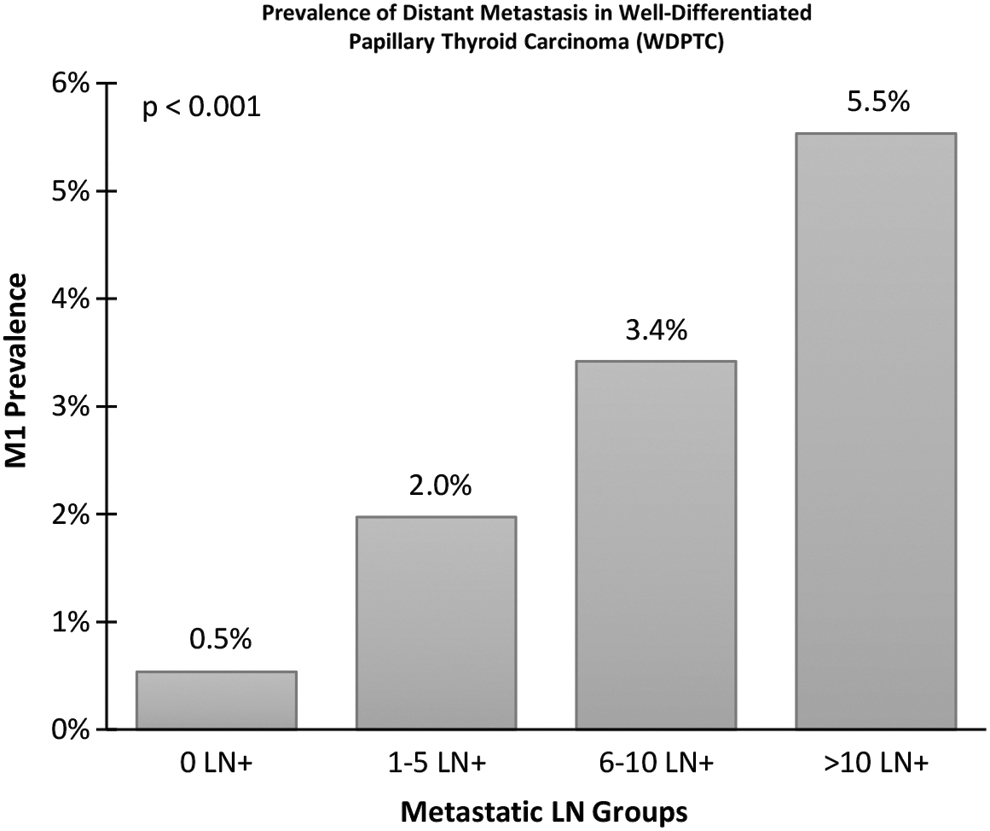
Prevalence of distant metastases in WDPTC, stratified by metastatic LN tranches.
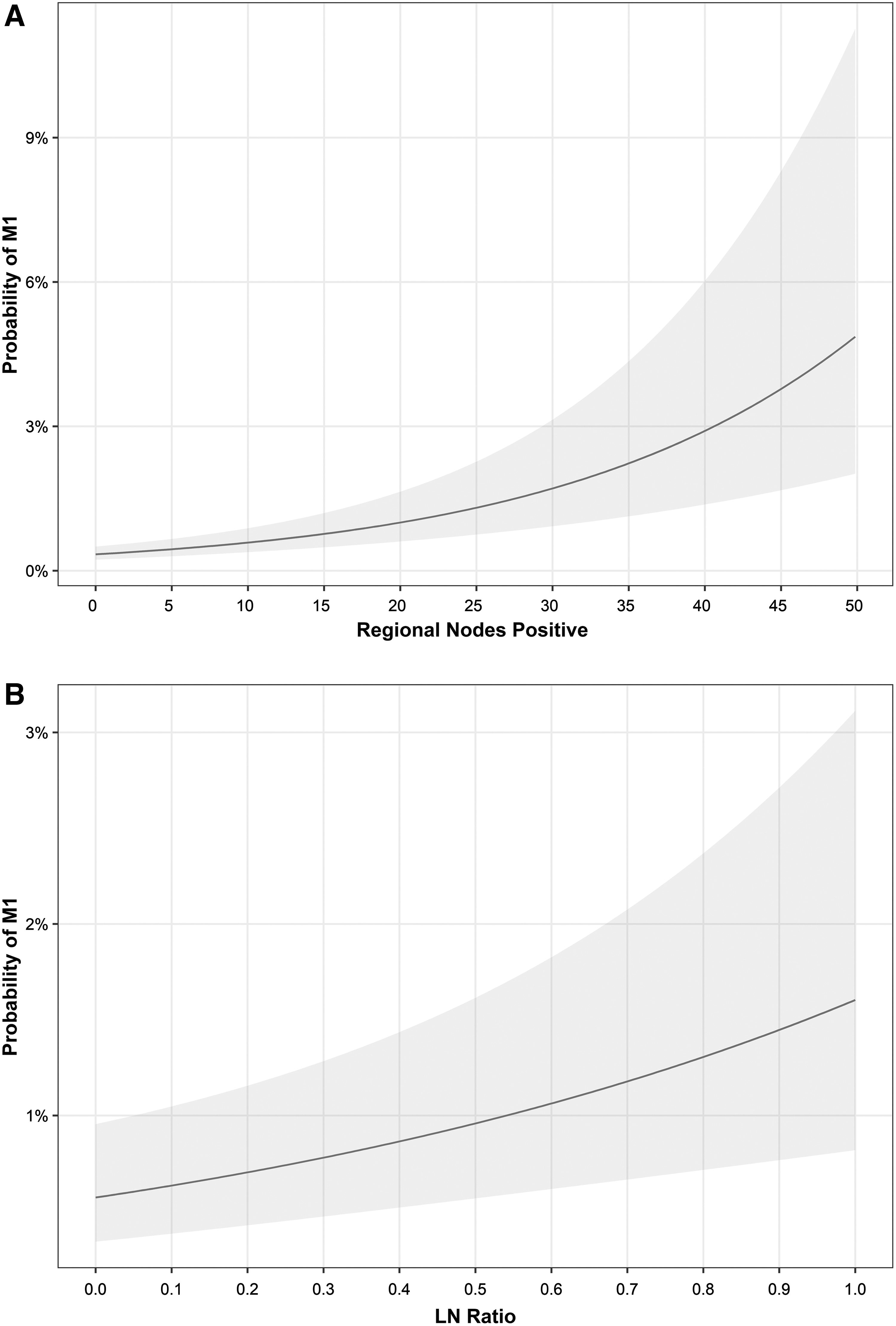
Estimated probability of M1 for WDPTC with increasing (
Discussion
In this study, we observed how escalating metastatic LN number conferred divergent effects as predictors of thyroid cancer distant metastasis, depending on histology. By employing a continuous multivariable regression model, we quantified the degree that successive positive LN increased the odds of M1 disease at presentation. For variants such as well-differentiated and tall cell PTC, substantial M1 risk emerges with increasingly heavy LN burden; conversely, histologies such as poorly differentiated and ATC have considerable M1 risk at baseline and are minimally affected, if at all, by increasing regional nodal spread.
Our findings build upon prior work evaluating the association of positive LN number with distant metastasis (10,19). Our analysis incorporated a number of key differences, including a more expansive multivariable adjustment for potential confounders, as well utilizing the largest metastatic PTC cohort reported to date. Stratification by PTC subtypes furthermore led to discrete risk profiles across variants that might otherwise be consolidated.
Consideration of LN burden when accounting for prognosis has remained controversial in thyroid cancer (5,20,21). Unlike other malignancies, it is unclear, for example, whether a thyroid cancer patient with a single metastatic LN will fare better than a similar patient with a dozen positive LNs, in terms of overall survival. Remarkably, both patients might be staged the same; for younger ages, both patients would in fact be classified as Stage I. Similar ambiguity exists for the value of central neck dissection, and the numerical metastatic node cutoff at which RAI would be recommended (17,22).
In contrast, the presence of distant metastasis constitutes a poor prognosis, with 5-year overall survival dropping from near 99% to below 50% (4,8 –11). Moreover, the cause of death in thyroid cancer patients is often due to M1 disease rather than locoregional recurrence (23). Agents including tyrosine kinase inhibitors and mitogen-actived protein kinase kinase inhibitors continue to broaden therapeutic approaches to achieve durable control of disease, if implemented in timely manner (24). As such, identification of distant spread is all the more crucial to discern early, so as to not miss the window of opportunity to treat. Identification of M1 risk profiles based on metastatic LN burden, either in groups (Fig. 3) or continuous probability (Fig. 4), offers a richer, more granular approach for valuing nodal disease. In comparison, the current American Joint Committee on Cancer Eighth Edition (AJCC 8E) staging stratifies nodal disease based only on central (N1a) versus lateral (N1b) location. Incorporating readily available factors such as quantitative nodal burden into staging may broaden prognostic insights on M1 hazard, the main driver underlying cancer-specific death.
We furthermore confirmed our findings when examining LNR (Fig. 4B), which has been found to confer improved prognostic ability when compared with the AJCC TNM staging system (25 –28). The advantages of LNR include its ability to account for extent of nodal dissection as well as the extent of nodal disease. However, it may also be prone to distortion: LNR is affected by the comprehensiveness of the surgeon and pathologist in procuring and counting total LN number, respectively. In general, a high LNR confers a worse prognosis, but it can be difficult to interpret at the extremes. For example, an excisional LN biopsy with 1 metastatic LN and only 1 LN removed would have a misleading LNR of 1.0; the same case would have a very different LNR of 0.1 if 10 LN had been harvested. A minimum number of LN harvested (LN yield) would need to be defined, which is a further area of controversy. For this study, 5 LN examined was selected as a minimum based on ATA risk stratification (5,17,29). Metastatic LN number, although also imperfect, may be more parsimonious. Altogether, both escalating metastatic LN number and LN ratio appear to correspond with increased risk for distant metastasis.
Thyroglobulin levels and whole-body scans currently remain foundational pillars of detection beyond what ultrasound monitoring can achieve. Their roles remain important for modern surveillance for distant metastasis. Nonetheless, thyroid cancer exists along a spectrum of differentiation, with aggressive variants losing the mechanistic ability to produce thyroglobulin and concentrate RAI. Indeed, perhaps 10% of classic PTC may lose these attributes (30 –32). Consideration of regional metastatic LN number as a tool to gauge risk would rationally add value to such complex decision-making: this might include modalities such as chest computed tomography (CT) or positron emission tomography/CT for greater nodal burden cases with a high index of suspicion, or a greater willingness to treat empirically with higher RAI dosages. These strategies might be especially rational for aggressive histologies that harbor outsized M1 risk at baseline.
Of interest, diffuse sclerosing PTC variant did not mirror WDPTCs nodal relationship with M1 disease, despite a similar M1 prevalence. Although various groups have contested whether it truly behaves as an aggressive subtype (33,34), its more favorable prognosis far exceeds that of PDTC or ATC. Notably, many DSV analyses have identified it to harbor a comparatively high degree of nodal metastasis (35 –38): this high N1 prevalence at baseline may account for its poor M1 correlation, in contrast to the high M1 baseline prevalence seen with PDTC or ATC.
Although NCDB does not distinguish central (N1a) versus lateral (N1b) site, it is notable that AJCC 8E also does not differentiate site in overall staging: patients younger than 55 years remain Stage I, and patients older than 55 years are upstaged to Stage II for any N1 status (39). Similarly, patients change from ATA low risk to ATA intermediate risk when >5 metastatic LN are found, independent of central or lateral location (5). Anatomically, metastatic central neck lymphatic drainage patterns may not need to traverse the lateral neck to travel distantly and may just as easily spread to the lungs directly from the central neck. This may further mitigate the difference between N1a and N1b when considering distant metastasis.
A number of caveats may limit the generalization of our findings. These include its retrospective nature, incomplete data, and the prospect of coding errors inherent to a national cohort study. Not all thyroid cancer patients undergo neck dissection, thereby increasing the potential for misconstruing true nodal burden. Moreover, not all M1 patients undergo surgery and therefore would have been excluded from our study: U.S. and international thyroid cancer guidelines nonetheless recommend locoregional surgery in such M1 cases to facilitate RAI (5,40,41). While we characterized the sites of M1 disease, a percentage of our cases did not have these data captured (Fig. 1). Details underlying M1 disease burden were also not available, such as volume of disease and multifocality. While multivariable analysis corrected for confounders, our study cannot account for thyroid-specific factors such as RAI avidity and mutational status, although these would not affect M1 status. The NCDB also does not record metastatic LN size or extranodal extension for thyroid cancer, which may influence distant spread (17,42). Some neck dissections are furthermore limited in scope, underestimating the true regional extent of disease. Finally, it is important to remember that the NCDB measures only disease at the time of initial presentation and initial treatment: we cannot account for cases of delayed metastatic spread.
In summary, we find that escalating nodal burden independently intensifies the risk of distant spread in WDPTC. This influence diverges when stratified by aggressive PTC variants: TCV follows a similar WDPTC pattern, while PDTC and ATC likely pose an already high baseline risk of M1 spread that is minimally affected by LN burden. Our findings altogether expand beyond the impact of current N-stage classification: deciphering such risk factors underlying distant metastasis is imperative given its outsized impact on cancer-related mortality. Deeper consideration of LN burden may augment the dynamic risk stratification principles adopted in modern treatment guidelines.
Footnotes
Authors' Contributions
Conception and design (Z.S.Z., G.D.B., W.L.S., and A.S.H.); acquisition and analysis of data (N.A., C.P., C.F.F., I.S., M.L., Z.S.Z., J.M.-S.C., Y.C., M.J., M.M.C., D.-C.L., H.B., and A.S.H.); drafting/revision (N.A., C.P., C.F.F., M.L., Z.S.Z., Y.C., M.J., M.M.C., J.M.-S.C., D.-C.L., H.B., G.D.B., W.L.S., and A.S.H.). All authors gave final approval to the submission.
Author Disclosure Statement
Z.S.Z. was on the external advisory board for the Scripps Proton Therapy Center and was a paid consultant for EMD Serono. The remaining authors have no conflicts to disclose.
Funding Information
No funding was received for this article.
Supplementary Material
Supplementary Figure S1
Supplementary Table S1
Supplementary Table S2