
Abstract
Background:
The recurrent laryngeal nerve (RLN) can be injured during thyroid surgery, which can negatively affect a patient's quality of life. The impact of intraoperative anatomic variations of the RLN on nerve injury remains unclear. Objectives of this study were to (1) better understand the detailed surgical anatomic variability of the RLN with a worldwide perspective; (2) establish potential correlates between intraoperative RLN anatomy and electrophysiologic responses; and (3) use the information to minimize complications and assure accurate and safe intraoperative neuromonitoring (IONM).
Methods:
A large international registry database study with prospectively collected data was conducted through the International Neural Monitoring Study Group (INMSG) evaluating 1000 RLNs at risk during thyroid surgery using a specially designed online data repository. Monitored thyroid surgeries following standardized IONM guidelines were included. Cases with bulky lymphadenopathy, IONM failure, and failed RLN visualization were excluded. Systematic evaluation of the surgical anatomy of the RLN was performed using the International RLN Anatomic Classification System. In cases of loss of signal (LOS), the mechanism of neural injury was identified, and functional evaluation of the vocal cord was performed.
Results:
A total of 1000 nerves at risk (NARs) were evaluated from 574 patients undergoing thyroid surgery at 17 centers from 12 countries and 5 continents. A higher than expected percentage of nerves followed an abnormal intraoperative trajectory (23%). LOS was identified in 3.5% of NARs, with 34% of LOS nerves following an abnormal intraoperative trajectory. LOS was more likely in cases of abnormal nerve trajectory, fixed splayed or entrapped nerves (including at the ligament of Berry), extensive neural dissection, cases of cancer invasion, or when lateral lymph node dissection was needed. Traction injury was found to be the most common form of RLN injury and to be less recoverable than previous reports.
Conclusions:
Multicenter international studies enrolling diverse patient populations can help reshape our understanding of surgical anatomy during thyroid surgery. There can be significant variability in the anatomic and intraoperative characteristics of the RLN, which can impact the risk of neural injury.
Introduction
The recurrent laryngeal nerve (RLN) has long been recognized as a critical anatomical structure to preserve during thyroid surgery to prevent significant postoperative morbidity (1). Injury to the RLN and resultant vocal cord paresis or paralysis (VCP) can have a major impact on patient's quality of life and is a leading cause of medico-legal litigation after thyroidectomy (2,3). Lahey (Boston) and Riddell (London) (1,2) are credited with improving rates of nerve preservation through the gold standard technique of routine RLN identification during thyroid and parathyroid surgery. While the incidence of RLN injury is portrayed as low in the literature, the true injury rate is widely believed to be underreported (4 –6).
Numerous studies have investigated the anatomical variation of the RLN and its relationship with various landmarks, including the tracheoesophageal groove, inferior thyroid artery (ITA), and ligament of Berry (LOB) (4). Intraoperative neuromonitoring (IONM) of the RLN is used as an adjunct to direct visualization to better understand detailed surgical anatomic variation and electrophysiologic function. IONM facilitates neural mapping of the RLN before visual identification and can assist in the recognition of anatomical variants and branching patterns of the RLN that have a higher risk of injury (7).
The International RLN Anatomic Classification System was created in 2015 (published in 2016) to allow surgeons to simply classify RLN anatomic variations. The intraoperative trajectory of the RLN is categorized as normal/typical, acquired abnormal (either ventrally or medially/laterally displaced by thyroid disease), or embryologic abnormal (nonrecurrent) (Fig. 1; Table 1) (5,8). The classification system also includes potential clinically important neural anatomic features, such as extralaryngeal branching, neural entrapment or invasion, or thin caliber of the nerve. Estimated prevalence data for RLN trajectories and anatomic features are reported based on review of the world's literature and expert opinion by the International Neural Monitoring Study Group (INMSG) board. Dynamic elements of surgery, encompassing neural electrophysiologic loss of signal (LOS) and extensive neural dissection, were also included given their potential impact on postoperative glottic function (5).

The international RLN anatomic classification system (5). RLN, recurrent laryngeal nerve; SLN, superior laryngeal nerve. Color images are available online.
The Estimated International Recurrent Laryngeal Nerve Anatomic Classification System Versus Observed SAR Study Data
Adapted with permission from Randolph et al. (5). SAR study prevalence values in bold differ from the estimated prevalence.
EMG, electromyography; L/R, left/right; LOB, ligament of Berry; LOS, loss of signal; NAR, nerves at risk; RLN, recurrent laryngeal nerve; SAR, surgical anatomy of the recurrent laryngeal nerve.
The primary purpose of this international multicenter registry database study is to better understand the variability of the surgical anatomy of the RLN with the use of the International RLN Anatomic Classification System as a means for standardized reporting of surgical anatomic detail and comparison with previously estimated prevalence data. In addition, with the use of IONM, potential correlates between RLN intraoperative anatomy, and electrophysiologic responses can be evaluated. Nerve injuries can be assessed based on intraoperative anatomical and electrophysiologic details as well as functional outcomes.
Methods
Study design
This is a large international registry database study with prospectively collected data conducted by the INMSG across 17 centers. Institutional Review Board approval was obtained at all participating institutions. The study protocol was sent to all participating centers with request for consecutive cases to be submitted, with specific inclusion and exclusion criteria provided. Patients undergoing thyroid surgery with IONM according to the standards set forth in the INMSG guidelines were included (7). Thyroidectomies performed in isolation or with concurrent central or lateral neck dissections were included. Surgeries were performed between March 2015 and November 2017. Cases with bulky lymph node metastases of the central or lateral neck were excluded given the potential independent impact on RLN trajectories. Cases with technical IONM failures were also excluded. All patients underwent preoperative laryngoscopy as well as postoperative laryngoscopy within 2 months of surgery. Patients with postoperative VCP were followed with laryngoscopy to evaluate for recovery of vocal fold mobility within the first 12 months after surgery.
Data collection
Data were collected prospectively via electronic submission for each patient to an online data repository developed and managed by Dr. Jennifer Shin, MD (Brigham and Women's Hospital, Boston, MA). Each submitting center was requested to include consecutive cases meeting patient inclusion and exclusion criteria. Each submission included prospectively collected and recorded data. The first 1000 nerves at risk (NARs) submitted were included in this study.
For each submission, patient demographic data were included, along with dominant nodule size and lobar dimensions based on preoperative imaging, type and extent of surgery, postoperative diagnosis, postoperative complications, and extent of RLN dissection (Table 2). Recovery of VCP was defined as return of normal vocal cord mobility by 12 months. Intraoperative anatomic data collected for the RLN were recorded according to the International RLN Anatomic Classification (Fig. 1; Table 1) (5). Length of dissection or exposure of the RLN was defined as limited (<2 cm), partial (2–5 cm), or complete (>5 cm). Thin nerves were defined as thickness <1 mm. Electrophysiologic data included mode of IONM used as well as intraoperative predissection vagal (V1), postdissection vagal (V2), predissection RLN (R1), and postdissection RLN (R2) amplitudes and latencies as specified by the INMSG guidelines (Table 3) (7).
Patient Demographics
Performed in conjunction with central neck surgery.
Hypocalcemia.
BMI, body mass index; SD, standard deviation.
Electrophysiologic Data
R1, predissection RLN response; R2, postdissection RLN response; V1, predissection vagal response; V2, postdissection vagal response.
For cases of LOS of the RLN, the type of lesion and the mechanism of injury were also documented (Tables 1 and 4). LOS was defined as loss of a normal, biphasic RLN waveform at supramaximal stimulation with an amplitude <100 μV when the initial amplitude was at least 500 μV. In accordance with INMSG guideline definitions, Type 1 LOS was defined as a focal neural injury where signal is maintained distal to the point of injury, whereas Type 2 LOS was defined as a global injury with lack of signal from the vagus nerve and all along the RLN up to the laryngeal nerve entry point (9). All LOS nerves were managed following the troubleshooting algorithm described in the INMSG guidelines (7).
Mechanisms of Recurrent Laryngeal Nerve Injury
Adapted with permission from Randolph et al. (5), Snyder et al. (23), Casella et al. (33), and Dionigi et al. (35).
A total of 35 LOS nerves were reported, with mechanisms of injury reported for 24 nerves. Three injured nerves had more than one mechanism reported, for a total of 28 mechanisms of injury reported. For mechanisms B1 through E, all injuries were Type 1 LOS focal injuries.
EBD, energy-based devices; VCP, vocal cord paresis or paralysis.
Statistical analysis
Continuous data were reported using the mean ± standard deviation and range. One-way analysis of variance test, Pearson's chi-square test, and logistic regression analysis were used to evaluate for differences in study populations using STATA version 16.0. Fisher's exact test was used to compare the rates of Type 1 and Type 2 LOS in nerves with abnormal anatomic trajectories. Odds ratios (ORs) were reported with 95% confidence intervals (CIs) and p-values. A p-value of <0.05 was determined statistically significant.
Results
Demographics
A total of 1000 RLNs at risk (NARs) were evaluated from 574 patients from 17 centers in 12 countries from 7 geographic regions and 5 continents (Table 2). Additional patient characteristics are described in Table 2. Postoperative complications were rare. Of the patients with postoperative VCP, 10 (38%) were noted to be symptomatic, and 14 (54%) showed recovery by 12 months.
Anatomical data
Neural trajectory and anatomical data for 499 right NARs and 501 left NARs were included in the study (Table 1). Limited exposure of the nerve (<2 cm) was performed for 62 (6%) NARs. Partial exposure (2–5 cm) was performed for 554 (55%) NARs, and complete exposure (>5 cm) was performed for 381 (38%) NARs. With regard to the circumferential degree of dissection, 58 (6%) NARs were extensively dissected and 185 (19%) nerves were completely dissected 360 degrees.
Of note, only 769 (77%) nerves showed a normal trajectory (Fig. 1; Table 1). Three hundred one (30%) NARs were fixed, splayed, or entrapped at the level of the capsule of the thyroid, with this percentage rising to 50% in cases of substernal goiter. Entrapment at the LOB and its associated vessels was observed in 411 (41%) nerves, and thin nerves (<1 mm) were observed in 156 (16%) cases. Extralaryngeal branching was demonstrated in 277 (28%) NARs, with mean distance from the laryngeal entry point similar for left and right RLNs at 1.8 ± 1.4 cm (range 0.5–7.2 cm) and 1.8 ± 1.5 cm (range 0.5–7.5 cm), respectively. Less than 3% of nerves were invaded by cancer.
Electrophysiologic data
Intermittent IONM was used for 714 NARs (71.4%), whereas continuous + intermittent IONM was used for 286 NARs (28.6%). The mean intraoperative recorded pre- and postdissection amplitudes and latencies for the right and left vagus and RLN are presented in Table 3.
Loss of signal
Of the 1000 NARs, 35 nerves (3.5%) had LOS, including 22 (4.4%) right RLNs and 13 (2.6%) left RLNs (Table 1). Although 63% of LOS nerves were right RLNs (nearly double that of left RLNs), this did not reach statistical significance (p = 0.12). Intermittent IONM was performed in 25 cases of LOS, while continuous + intermittent IONM was performed in the remaining 10 cases of LOS. Twenty-six (74%) RLN injuries were Type 1 focal segmental injuries and 9 (26%) RLN injuries were Type 2 global injuries without identifiable focal injury (Table 1). Nine Type 1 injuries and one Type 2 injury were observed in cases utilizing continuous IONM + intermittent IONM.
Trajectory and anatomical data for LOS nerves are reported in Table 1. Of note, only 22 (63%) LOS nerves showed a normal anatomic trajectory, with the remaining LOS nerves showing an abnormal acquired trajectory. Twenty (57%) LOS nerves were fixed, splayed, or entrapped at the capsule of the thyroid. Twenty (57%) LOS nerves were found to be entrapped at the LOB and its associated vessels. Using IONM LOS as a test of postoperative VCP, the sensitivity was 92.8%; the specificity was 98.9%; the positive predictive value was 74.3%; and the negative predictive value was 99.8%. See Figure 2 for further details regarding cases of neural injury and resultant VCP.
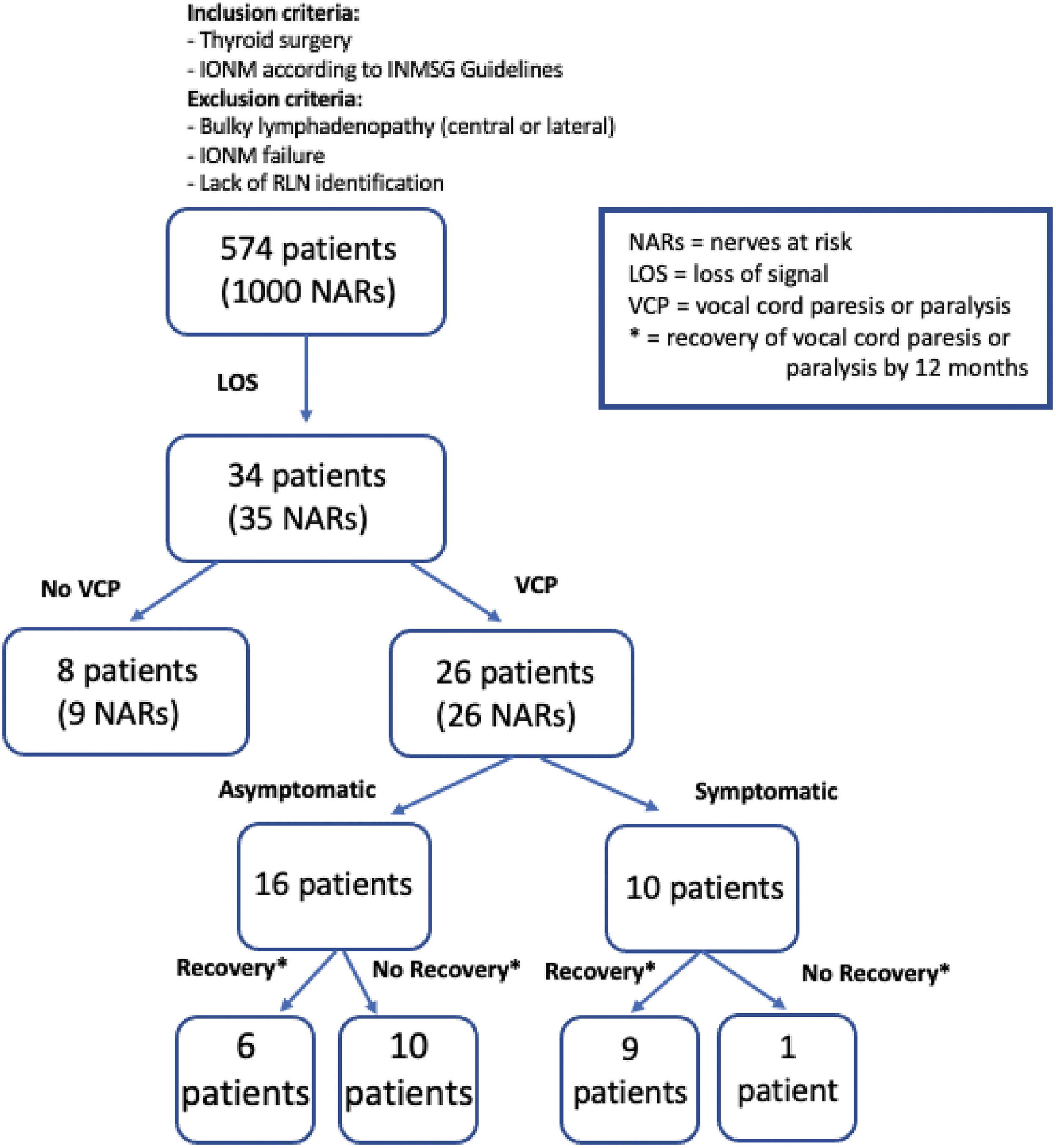
Patient flowchart for neural injury. Color images are available online.
Multivariate analysis
Comparison between NARs without LOS and with LOS using the Pearson's chi-square test and logistic regression analysis showed a higher rate of lateral lymph node dissection for right LOS nerves (OR = 4.43 [CI 1.21–16.27], p = 0.03), and a higher body mass index (BMI) for patients with left LOS (OR = 1.01 [CI 1.001–1.03], p = 0.032). There was a higher likelihood of extensive neural dissection in the LOS group for both right- and left-sided nerves (OR = 11.56 [CI 3.52–38.02), p < 0.0001 and OR = 6.42 [CI 1.61–25.63], p = 0.008). Right LOS nerves were less likely to follow a normal intraoperative trajectory (OR = 0.19 [CI 0.05–0.75], p = 0.02). LOS nerves with an abnormal trajectory were not more likely to have a Type 1 LOS injury versus Type 2 LOS injury (Fisher's exact test, p = 0.4496).
Right LOS nerves were more likely to be entrapped at the LOB (OR = 3.25 [CI 1.38–7.66], p = 0.01), and both right and left LOS nerves were more likely to be fixed to the thyroid capsule (OR = 16.63 [CI 6.53–42.26], p < 0.0001 and OR = 3.45 [CI 1.03–11.53], p = 0.044, respectively). There was a nonsignificant trend toward a higher likelihood to be thin for right LOS nerves (OR = 2.54 [CI 0.96–6.71], p = 0.06). Right and left LOS nerves were more likely to be invaded by cancer, with OR = 18.3 [CI 2.89–115.69], p = 0.002, and OR = 15.5 [CI 1.5–159.99], p = 0.021, respectively, and postoperative VCP was more likely with neural invasion by cancer (p < 0.001). RLN fixation to the thyroid capsule and increased length of RLN exposure (>2 cm) were also risk factors for postoperative VCP, although only significant for right-sided nerves (p = 0.006) (Table 5).
Anatomic Risk Factors for Recurrent Laryngeal Nerve Injury
Bold values are statistically significant.
CI, confidence interval; L2, postoperative vocal cord mobility; OR, odds ratio.
Mechanism of nerve injury
Of the 35 LOS nerves, 28 mechanisms of injury were reported for 24 nerves (Table 4). Three injured nerves had >1 mechanism of injury reported. Twenty-two (63%) injuries were traction injuries (A1 or A2 injuries), with either Type 1 or Type 2 LOS. All mechanical and thermal injuries were Type 1 LOS injuries. There was no constriction or accidental transection injuries. Eighteen (82%) traction injuries (A1 or A2) resulted in postoperative VCP, with 8 (44%) symptomatic cases and 11 (61%) recovering by 12 months. Thirteen (76%) traction injuries with Type 1 LOS resulted in VCP, with 7 (54%) symptomatic and 8 (62%) recovering by 12 months. All five traction injuries with Type 2 LOS showed VCP postoperatively, with one (20%) symptomatic and three (60%) recovering by 12 months. Three (60%) cases of mechanical trauma resulted in VCP postoperatively, and all six nerves with mechanical or thermal injuries recovered by 12 months (Table 4).
Discussion
To our knowledge, this is the first large international multicenter registry database study with prospectively collected data of surgical RLN anatomy categorized by an international classification system and incorporating intraoperative electrophysiologic intraoperative data and postoperative outcome measures. Multivariate analysis revealed that abnormal trajectories of the RLN, including those associated with thyroid disease-related acquired nerve displacements, were associated with an increased risk for intraoperative LOS, meeting statistical significance for right RLNs. Based on the anatomic classification system used in this study, only 77% of RLNs followed a normal expected course. Thus, nearly a quarter of RLNs in this study followed abnormal pathways, which when present could be associated with a poorer outcome, suggested previously in the literature (5,10). This is a finding of great clinical significance.
Rates of postoperative complications after thyroid surgery were low and similar to previous reports in the literature (11 –14). The rate of VCP of 2.6% of NARs was low and consistent with rates seen from high-volume centers, although a wide range of rates are reported in the literature (15). Patients with VCP were symptomatic only 38% of the time, emphasizing the need for a laryngeal examination for accurate postoperative complication assessment.
A summary of risk factors for RLN LOS and VCP in this study is shown in Table 5. BMI was higher in patients with left LOS but with an OR of only 1.01, and no difference was noted for right-sided LOS patients, which is in alignment with the literature (16,17). Patients with right-sided LOS had a higher likelihood of lateral neck dissection compared with patients without LOS, consistent with a higher risk of nerve injury with more extensive surgery and possibly greater severity of disease (2,5). Extensive neural dissection was a significant risk factor for LOS. Right and left RLNs with LOS showed a higher risk of invasion by cancer, which was also associated with a higher risk of postoperative VCP. Comparison of patients with and without LOS showed no difference in age, gender, race, geographic region, the extent of thyroidectomy, or lobar or nodule size.
Mean predissection V1 vagal amplitudes in this study were consistent with normative values and >500 μV as recommended by the INMSG for reliable IONM (7,18). Mean reported RLN and vagal latencies were also consistent with the literature (18,19). Of the 1000 NARs, 3.5% of nerves had LOS. This was nearly twice as high (4.4%) for right RLNs than for left RLNs (2.6%) although not statistically significant (p = 0.12). There is some suggestion in the literature of higher injury rates for right RLNs in thyroid surgery (20 –22), perhaps because of the more oblique course of the nerve (21).
Higher than expected rates of thyroid capsular fixation of NARs were observed, with up to 50% in cases of substernal goiter, and this was even higher in the LOS group (OR = 16.63 for the right and 3.45 for the left) (Table 1). Higher overall rates of neural entrapment at the LOB, known to be the most likely location for RLN injury during thyroid surgery, were reported, with right LOS nerves showing the highest rates (5,23). The most common location for traction injury, which is recognized as the most common cause of RLN injury in thyroid surgery, is at the LOB region (5,23 –25). In fact, a study of 115 nerves with LOS showed that traction injuries made up 83% of RLN injuries, and 60% of these injuries occurred at or near the LOB (26).
Extralaryngeal branching of the RLN was observed in 28% of NARs, within the range reported in the literature of 24–75% (5,27 –31). Branching is most often cited to occur within 2 cm of the laryngeal entry point of the nerve (27,32), consistent with 1.84 cm observed in this study. Nearly 45% of extralaryngeal branching was observed proximal to the RLN-ITA crossing point, higher than previous reports (5). Extralaryngeal branching as a risk factor for RLN injury has been described in the literature (5,10,33,34) but was not observed in this study. Thin nerves have been suggested to have a higher likelihood of nerve injury by some authors (5), although only a nonsignificant trend toward a higher risk of LOS for thin right RLNs was observed in this study.
The risk of postoperative VCP was associated with a greater length of exposure of the RLN (>2 cm) for right nerves (Table 5). RLNs with LOS were more likely to be extensively dissected compared with NARs without LOS (Table 1). Extensive neural dissection, especially the 360-degree dissection, is a potential risk factor for RLN injury via traction injury when lifted off the neural bed (5).
Most cases of LOS were Type 1 focal segmental injuries (74%) versus Type 2 diffuse or global injuries (26%). The majority of LOS occurred via traction at the LOB (Table 4) and were Type 1 injuries, presumably from direct focal traction at the LOB, despite discussion in the literature that traction injuries are most often Type 2 injuries without an identifiable focal lesion. All reported Type 2 injuries were, however, traction injuries and in alignment with the assumption that Type 2 injuries may reflect more indirect mechanisms of injury (6).
Postoperative VCP was observed in 82% of traction injuries, with only 62% recovering at 12 months. This low recovery rate may be due to a lower number of Type 2 global injuries in this group, which are thought to have a better clinical outcome in the literature (5,6,35). Interestingly, all other mechanisms of injury (i.e., mechanical and thermal injuries) were Type 1 LOS injuries, with all VCP cases recovering by 12 months. The lower than expected recovery rate for Type 2 LOS traction injuries should be interpreted with caution, given the very limited number of cases (26).
There are several limitations to this study. While the protocol for patient submission specified prospective collection of data from consecutive cases meeting the inclusion and exclusion criteria, this could not be confirmed by the authors in this large database study, which raises the risk of selection bias. Furthermore, because database submissions were counted chronologically (up to 1000 NARs for this first study), 6 centers with later submissions had only 1 or 2 patients included, accounting for 10 NARs and 2 cases of LOS, further impacting the possibility of selection bias. Future studies with a larger number of NARs will serve to address this potential bias.
While the online data repository was created as an efficient easy way for study site submission, some clinical judgment was required in data reporting. Specifically, terms including “hypocalcemia” and “symptomatic” for VCP were not defined a priori for data collection and were left up to the judgment of the submitting surgeon, which could lead to some heterogeneity in reporting these outcomes. Initial postoperative evaluation of vocal cord mobility was allowed up to 2 months after surgery, causing a potential for missed cases of recovered temporary paresis or paralysis. For the 35 LOS nerves, only 24 nerves had mechanisms of injury reported, 3 of which had more than one mechanism accounting for the LOS, limiting interpretation of the data. Cases of VCP were also small in number, limiting our analysis, with further studies planned to address this with a larger number of NARs.
Conclusion
The International RLN Anatomic Classification System has been previously proposed as a standardized method for capturing detailed surgical anatomic variability of the RLN, which can be correlated to electrophysiologic responses of the nerve, including LOS (Table 5). Of particular note, nearly a quarter of RLNs in this study followed abnormal pathways and a higher than expected percentage of RLNs were fixed, splayed, or entrapped on the surface of the thyroid, both of which were associated with poorer outcomes, a finding of great clinical significance.
The need for routine postoperative laryngeal examination to accurately predict neural outcomes is further suggested by the low rate of symptomatic VCP in this study (38%). Neural monitoring in these 1000 monitored nerves was shown to be a powerful and accurate surgical tool with a positive predictive value of 75% and an negative predictive value of 99.8%. Our inability to preoperatively predict abnormal RLN courses would add support to the consideration of routine IONM in thyroid surgery. In alignment with the goals of this study, future studies with a larger number of RLNs at risk are being conducted by the INMSG.
Footnotes
Acknowledgments
G.W.R. acknowledges the ongoing support of John and Claire Bertucci and Mike and Eliz Ruane for his research efforts.
Authors' Contributions
W.L. contributed to the design of the work, analysis and interpretation of data, and drafting of the work. J.J.S., C.-W.W., and G.D. contributed to the design of the work, acquisition of data, and critical revision of the work. G.D., Y.G.S., A.I., C.C., N.A., M.U., K.B., B.C., F.T., M.B., H.Y.K., E.F., N.I., K.V., J.S., A.F.R., and A.H.A.A. contributed to the acquisition of data and critical revision of the work. B.W. and A.C. contributed to the analysis of data and critical revision of the work. F.-Y.C. and R.S. contributed to the design of the work and critical revision of the work. H.T. and Y.S. contributed to the critical revision of the work. O.O. contributed to the acquisition of data, analysis and interpretation of data, and drafting of the work. D.K. contributed to the acquisition of data, analysis of data, and critical revision of the work. H.D. contributed to the design of the work, interpretation of data, and critical revision of the work. G.W.R. contributed to the design of the work, acquisition of data, analysis and interpretation of data, and critical revision of the work.
Author Disclosure Statement
G.D. reports financial contracts for lectures and training courses from Medtronic Int., Olympus Italy, and Inomed (Germany), and remuneration for the development of new technology from Medtronic Int. and AFS Medical (Vienna, Austria). J.J.S. receives textbook royalties from Evidence-Based Otolaryngology, Shin JJ, Randolph GW, editors; New York: Springer, 2008, and from Otolaryngology Prep and Practice, Shin JJ, Cunningham MJ, editors; Plural Publishing, 2013. J.J.S. is a recipient of the American Academy of the Otolaryngology-Head and Neck Surgery Foundation Maureen Hannley grant, the Brigham Care Redesign Program and DOS Outstanding Citizenship Awards, and the Schlager Family Innovations Fund Award. The remaining authors have nothing to disclose.
Funding Information
The authors received no financial support for the research, authorship, and/or publication of this article.