
Abstract
Background:
A thyroid incidentaloma (TI) is an unexpected, asymptomatic thyroid lesion discovered during the investigation of an unrelated condition. The aim of the present study is to examine the incidence of 18Fluorodeoxyglucose (FDG)-positron emission tomography (PET) TI, the associated management strategies and the outcomes in a tertiary cancer referral center.
Methods:
This study involves a retrospective cohort study of 1003 patients with TI found on 18FDG-PET/CT scans performed between January 2010 and January 2020 for a nonthyroidal malignancy. The Kaplan–Meier method was used for survival analyses in patients concerning an underlying malignancy, with a prevalence of 5% or higher in this cohort. Logistic- and cox regression analyses were performed to analyze predictors of thyroid malignancy and mortality. A propensity score weighted method was used to control for baseline differences between the intervention (additional TI diagnostics) and control (no TI diagnostics) group.
Results:
FDG-positive TI occurred in 1.9% (1003/52,693) of the oncologic 18FDG-PET/CT scans performed in our center. Thyroid surgery was performed in 47 patients (6%) and a thyroid malignancy was detected in 31 of them, which is 66% of those who had an operation and 4% of all patients. During the follow-up (median 6 years), 334 deaths (42%) related to different types of cancer (38%) or other causes (4%) were observed. One patient died from medullary thyroid cancer. In multivariate analysis adjusted for age, gender and the type- and stage of nonthyroidal malignancy, were independent predictors of survival (P < .05).
Conclusions:
The incidence of TI in this tertiary cancer referral center was comparable to current literature. Further thyroid workup was performed in less than half of the patients, and only a minority of patients underwent thyroid surgery. Since only one patient died from thyroid cancer, the strategy to withhold from thyroid diagnostics and treatment seems valid for most TI. Active thyroid treatment might benefit a subgroup of patients in whom the primary nonthyroidal malignancy is successfully treated or presumably stable. A wait-and-see policy with ultrasound follow-up could be an alternative strategy. These considerations should be part of the shared decision making in cancer patients with a TI.
Introduction
18F
There is yet much to learn about the clinical relevance of TI in patients with underlying malignancies. The 2015 American Thyroid Association (ATA) guideline recommends ultrasound investigation of thyroid nodules 1 cm or larger with or without fine-needle aspiration cytology (FNAC) in patients without relevant comorbidities (11,12). The predominant indication for an 18FDG-PET/CT scan in cancer patients is staging of the primary malignancy. Therefore, this specific population has relevant comorbidities influencing prognosis. The strategy to actively pursue all TI of 1 cm and larger in this population may lead to overtreatment of thyroid nodules that might never become clinically relevant. Moreover, DTC is associated with an estimated survival of 95–98% (13). The clinical impact of an asymptomatic thyroid malignancy in the context of an active nonthyroidal malignancy is unknown, and there is a need for guidelines in the management of TI in cancer patients.
The aim of the present study was to examine the incidence of 18FDG-PET TI in a tertiary cancer referral center over a 10-year period of time. We also describe the different treatment strategies and the results of these different approaches in 18FDG-PET TIs patients with a nonthyroid primary cancer. This study also aimed at identifying predictors of thyroid malignancy and at analyzing survival for cancer patients with an 18FDG-PET TI.
Methods
This study was approved by the Institutional Review Board (IRB) from the Antoni van Leeuwenhoek Hospital (AvL), a tertiary oncological referral hospital in Amsterdam, The Netherlands (IRBd19178). It involves a retrospective cohort study of 18FDG-PET/CT scans that were performed in this cancer center between January 2010 and January 2020. The 18FDG-PET/CT scans were performed in the AvL Hospital for diagnosis, staging, or treatment response measurement for a known or suspected (nonthyroidal) malignancy and reviewed by two specialized radiologists according to the European Association of Nuclear Medicine (EANM)-guidelines for 18FDG-PET/CT scans (14). The decision to perform ultrasound and FNAC was dependent on the physician's preference and the patient's risk factors for thyroid cancer, anxiety, comorbidities, life expectancy, and other relevant considerations. The ATA guidelines to refrain from FNAC in thyroid nodules <1 cm unless there was cervical lymphadenopathy or another finding associated with a higher cancer risk were used and since 2017 The Thyroid Imaging Reporting and Data System (TIRADS) was used (11,15). The TI sizes in the ultrasound examination reports were re-evaluated by a specialized radiologist (C. Lange).
The FNAC results were analyzed by dedicated pathologists based on the Bethesda System for Thyroid Cytopathology (16). Clinical and pathological staging was reported according to the TNM classification criteria by the American Joint Committee on Cancer (AJCC). The reports from the Department of Nuclear Medicine were selected anonymously and retrospectively by screening for the word “thyroid.” The reports were than manually screened by the author M.W.P. to verify the presence of FDG uptake in the thyroid gland. Patients with known thyroid cancer or thyroid disease and non-avid thyroid nodules were excluded. All patients with focal- or diffuse FDG uptake in the thyroid gland primarily depicted by 18FDG-PET/CT scans were included in this study. We retrospectively reviewed medical records of the included patients and collected the primary malignancy type and stage, FDG avidity, extent of thyroid investigation, treatment, and follow-up.
Statistical analyses
Baseline values of continuous variables are reported as mean ± standard deviation or median with interquartile range (25th–75th percentile), and baseline categorical variables were presented as frequencies and percentages. Differences between the two groups were tested with the Pearson's chi-square test. All statistical tests were two-tailed, and a value of p ≤ 0.05 was considered statistically significant.
In univariate analysis, individual variables and their association with TI final pathology results were analyzed by using adjusted odds ratios. Multivariate Cox regression models for patient survival were created based on the variables assessed in the univariate analysis, with stepwise removal of factors with a p-value of <0.1. A p-value of 0.05 was taken to indicate statistical significance.
The Kaplan–Meier method was used to estimate overall survival (OS). The OS was measured from the date of the 18FDG-avid TI to the date of death from any cause, censoring patients who were still alive at the date of last contact. The main diagnoses that occurred ≥5% in this cohort (breast cancer, lung cancer, melanoma, colon cancer, head and neck cancer, and urothelial cancer) were included in the analysis to increase the strength of the association. The OS was compared across the aforementioned groups by using the log-rank test.
Propensity score weighting (PSW) was used to control for the baseline differences between the treatment groups to compare cancer-related mortality. This analysis was performed post hoc. Two groups were created: patients who underwent additional diagnostic tests for TI (intervention) versus patients who had no TI diagnostic tests (control). Additional diagnostics consisted of an ultrasound and FNAC. The included patients had focal FDG uptake on 18FDG-PET/CT. The propensity score was calculated by using logistic regression. Baseline covariates that differed between the intervention and control group were included in the analysis: age, the stage and type of primary nonthyroidal malignancy that occurred ≥5% in this cohort of patients. The occurrence of a local, regional, or distant recurrence or a second primary tumor during follow-up were also included in the analysis because this affected the performance of TI diagnostic tests. Patients with missing data were excluded from this analysis. Propensity weights were then calculated by using the propensity scores. To allow weighted estimates, each intervention patient received a weight of
Results
Patient selection
Between 2010 and 2020, a total of 52,693 18FDG-PET/CT scans were performed in this center, of which 3928 (7.5%) nuclear medicine scan reports included the word “thyroid.” After the exclusion of duplicates and triplicates, 1424 patients (2.7%) with an increased uptake of 18F-FDG in the thyroid gland were found. Based on the exclusion criteria for this report, we excluded 421 patients and included 1003 (1.9%) patients in this study, that is, FDG-positive TI occurred in 1.9% (1003/52,693) of oncologic 18FDG-PET/CT scans that were performed in this cancer center. The process for patient selection is presented in Figure 1.
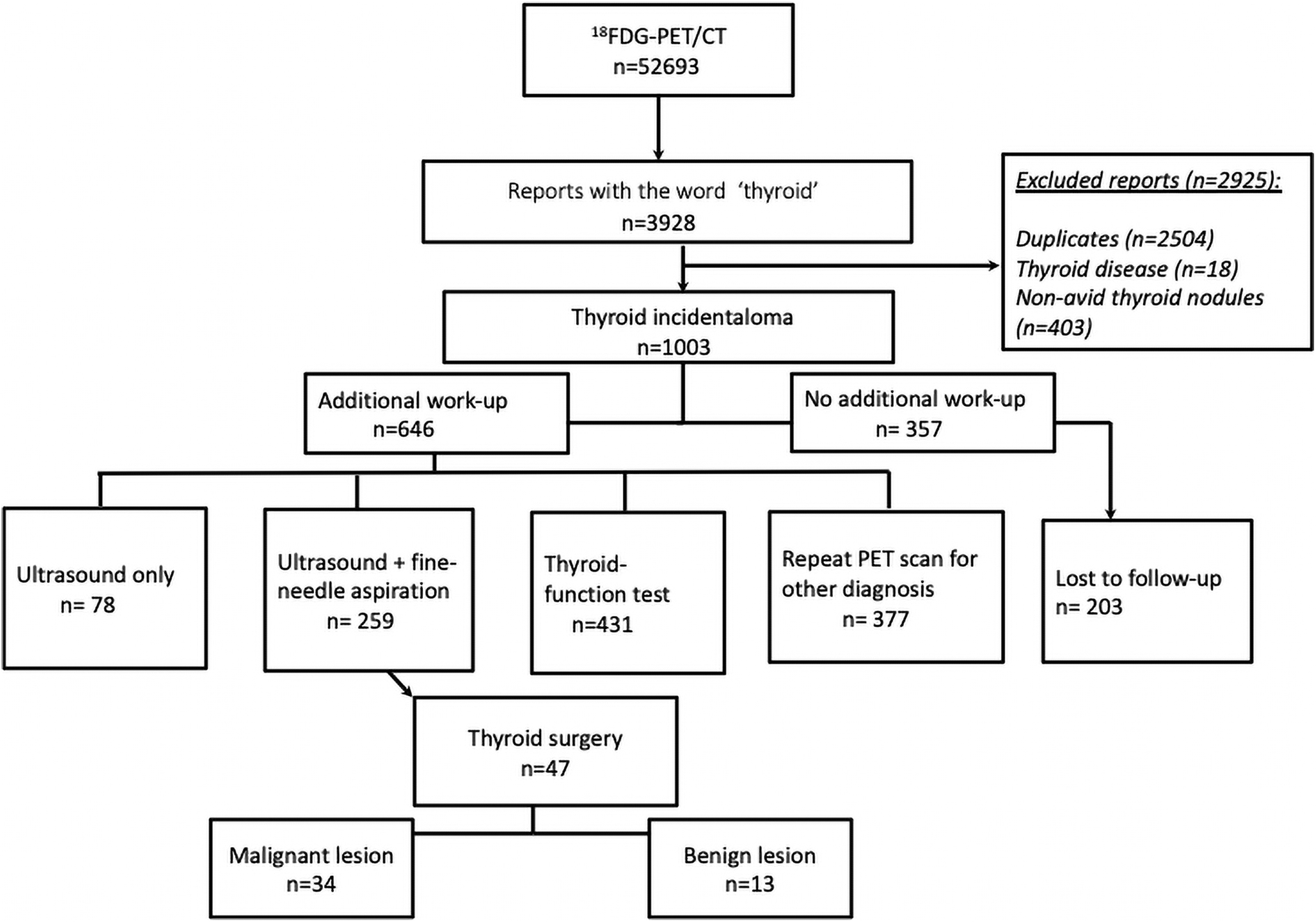
Flowchart of patient selection.
18FDG-PET/CT TI investigation and treatment
Two hundred and three patients (20%) were referred to our center for PET imaging only and were subsequently treated in a different hospital. We included these patients in the initial work-up concerning PET/CT and laboratory data (N = 1003) but excluded them from the TI treatment analysis (N = 800). Baseline characteristics are described in Table 1.
Clinical Characteristics of Study Cohort and 18Fluorodeoxyglucose-Positron Emission Tomography/Computed Tomography Data
FDG-PET, 18Fluorodeoxyglucose-positron emission tomography; IQR, interquartile range; NET, neuroendocrine tumor; SD, standard deviation; SUVmax, standardized uptake value.
Of the 800 patients who were treated in our center, subsequent evaluation by ultrasound was performed in 337 (42%) patients (Table 2). FNAC was done in 259 (77%) of the 337 patients who underwent ultrasound. In this study population, 47 patients (6%) had surgery, most frequently (75%) a hemithyroidectomy. The median age of the patients who had an operation was 65.6 (55.8–73.8) years, and the median tumor dimension of the TI was 1.25 (0.8–2.3) cm. The final pathology report showed a thyroid malignancy in 31 patients, which is 67% of those who had an operation and 4% of all patients who were treated for a nonthyroid primary cancer in our hospital. In Figure 2, the final pathology results are shown by Bethesda classification.
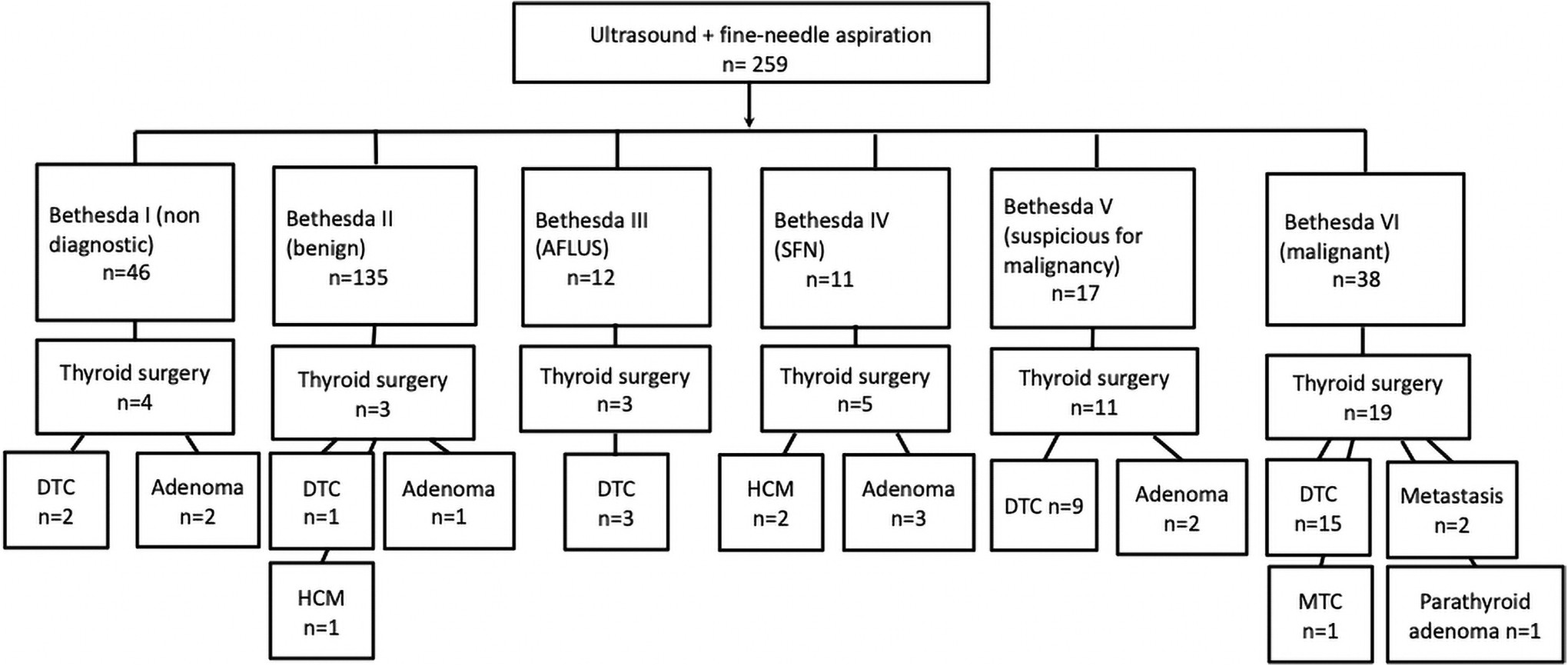
Flowchart of pathology results after thyroid surgery stratified by Bethesda classification. AFLUS, atypical follicular lesion of undetermined significance; DTC, differentiated thyroid carcinoma; HCM, hürtle cell metaplasia; MTC, medullary thyroid carcinoma; SFN, suspicious for follicular neoplasm.
Thyroid Incidentalomas Investigation and Treatment
Percentage of patients who underwent US.
Percentage of patients who underwent FNAC.
Percentage of patients who underwent thyroid surgery.
Percentage of patients who underwent a neck dissection.
FNAC, fine-needle aspiration cytology; PA, pathology; US, ultrasound.
The predictive factors analyzed for the final pathology results are shown in Table 3 (N = 47 patients). Univariable analysis showed that none of these independent covariates were statistically significant predictors of TI being malignant on pathology.
Results of Univariable Logistic Regression Model to Predict Thyroid Malignancy (n = 47)
AOR, adjusted odds ratio; TI, thyroid incidentalom.
Follow-up and survival
The median follow-up was 6 years (range 4–8 years). During follow-up, 21% of patients received treatment for recurrent disease of their primary cancer diagnosis, 13% of patients for a secondary nonthyroid type of cancer, and 24% of the study patients had no cancer-related event after the TI finding. After the total follow-up period, 334 patients (42%) had died. In 300 patients (38%), the cause of death was related to their primary cancer and in 33 patients (4%) to a noncancer related event. One patient, who had the PET scan to identify a neuroendocrine tumor, had a medullary thyroid carcinoma and died of this 21 months after diagnosis.
Kaplan–Meier analyses showed significant differences in OS between different subgroups categorized by the nonthyroid primary cancer (log-rank p < 0.0005) (Fig. 3). Patients with lung cancer and urothelial cancer had the lowest OS (median survival time: 35 months) followed by patients with colon cancer (median survival time: 42 months). Five-year survival rates in these groups (lung, urothelial, and colon cancer) were 31.1%, 33.2%, and 36.6%, respectively. Patients with breast cancer had the most favorable prognosis, with a 5-year survival rate of 72.3%.
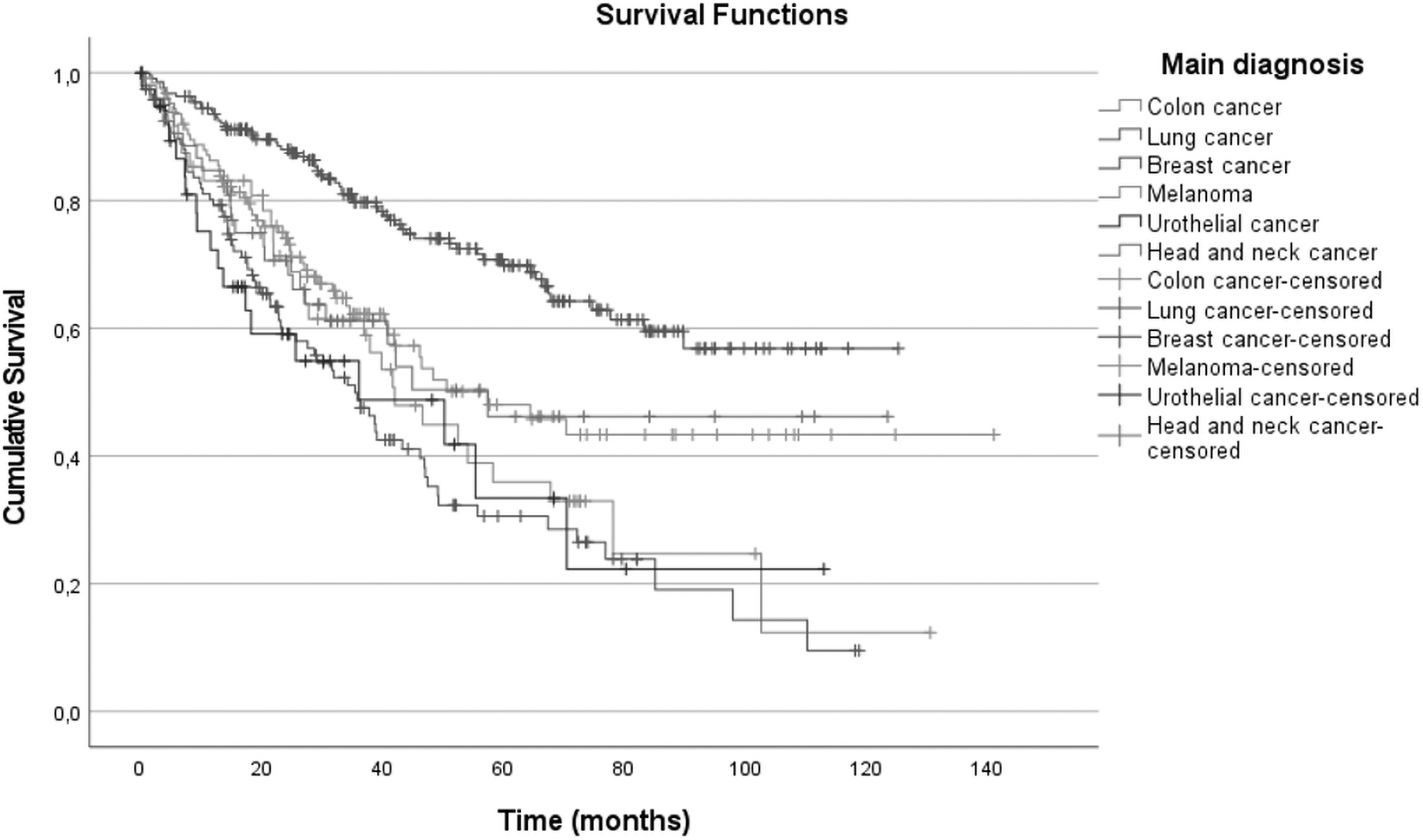
Kaplan–Meier analysis of OS comparing different subgroups based on the main cancer diagnosis with a study prevalence of ≥5% of the patient cohort (n = 606). Patients were censored due to loss to follow-up. OS, overall survival.
Univariate and multivariate Cox regression analyses were used to examine the relationship between patient survival and multiple prognostic variables. TI characteristics (Bethesda classification, tumor dimension, and final pathology results) were not predictive for patient survival in univariate analysis. The following predictive factors for patient survival were included in a multivariate analysis (Table 4): age, male sex, the AJCC stage and the type of nonthyroidal primary malignancy (≥5% of the patient cohort), distant metastasis of the primary tumor, and a second primary nonthyroidal tumor during follow-up. In multivariate analysis, these factors remained important determinants of survival.
Results of Multivariable Cox Regression Model to Predict Mortality (n = 800)
Recurrence of the primary nonthyroidal malignancy.
AJCC, American Joint Committee on Cancer; CI, confidence interval; HR, hazard ratio.
Comparison of TI treatment strategy groups
In the studied patient cohort, there appear to be substantial differences in the patients who underwent subsequent ultrasound imaging and FNAC of the 18FDG-PET TI (intervention group) compared with those who did not (control group). Therefore, a propensity score analysis was performed to balance prognostic variables and compare patient survival between the these two groups. A total of 539 patients were included in the propensity score analysis, and 464 patients were excluded due to missing data in any of the covariates. The baseline characteristics of the propensity-weighted population in the intervention and control group are displayed in Table 5. It shows significant differences in the distributions of age, main diagnosis, and AJCC stage (p ≤ 0.05). The nonthyroidal primary malignancies with a worse prognosis (Fig. 3) were predominant in the control group.
Patient Characteristics of Propensity-Weighted Population (N = 539)
AJCC stage of the nonthyroidal primary malignancy.
Before the propensity score weighting, there was a significant patient survival advantage in the TI intervention group compared with the control group (unadjusted hazard ratio [HR] 0.57; confidence interval [CI 0.42–0.78], p < 0.001). When comparisons of the patient survival among the intervention and control group were made with the PSW adjustment, there was no significant difference between the two groups (adjusted HR, 0.77 [CI 0.56–1.07], p = 0.13).
Discussion
This study shows that TIs were found in 1.9% of the 18FDG-PET/CT scans that were performed in our tertiary cancer referral center from 2010 to 2020. In total, 42% of the patients with known follow-up data (n = 800) underwent additional ultrasound and 32% of the patients also underwent FNAC. In 47 patients (6%), thyroid surgery was performed. The majority of the patients (66%) who had an operation had a histologically proven thyroid cancer. Our study population showed no significant predictors for TI malignant pathology results. In 38% of the analyzed patients, the cause of death was related to their nonthyroid primary cancer, in 4% to a noncancer related event, and one patient (0.1%) died from medullary thyroid cancer. The primary nonthyroidal malignancies were predictive for patient survival and differed between the TI treatment groups. These factors were corrected for by the propensity-weighted analysis, which resulted in no significant difference in patient survival between the TI intervention and control groups.
The incidence of 18FDG-PET/CT TIs in the literature (2–3%) is comparable to the current study result of 1.9% (18,19). The FNAC analyses showed Bethesda V or VI group in 21% of the patients subjected to an ultrasound and biopsy, which is lower when compared with previous studies (26–50%) (20). The under-investigation may have led to a lower malignancy rate compared with other populations described in literature. The most frequent malignant histological subtype was papillary thyroid carcinoma (53%), which is comparable to previous studies (21 –24).
The incidence of TI increases in Western countries and has been described in a number of previous studies analyzing different diagnostic modalities. The current literature revealed four systematic reviews concerning 18FDG-PET TI (21 –24). Most of the reviewed studies were retrospective in nature and included a small number of patients with TIs. Two reviews concluded that focal hypermetabolic thyroid nodules were associated with a higher prevalence of malignancy (21,22). The general advice extracted from available literature is that health care institutions should make their own TI management strategies with the aim of avoiding unnecessary investigations and surgery (23,24).
In our center, different types of treatment strategies were applied. The prognosis of most patients was dependent on the underlying malignancy type. Pattison et al. focused on the clinical relevance of investigating 18FDG-avid TI in cancer patients. They emphasized the perspective of a broader clinical context before the investigation of 18FDG-avid TIs (25). The amount of FDG-uptake in the index malignancy and the disease stage of the primary nonthyroidal malignancy were all statistically significant predictors of mortality (25). These results are consistent with our study observations, although the amount of FDG-uptake in the index malignancy was not verified.
The overall mortality of patients with 18FDG-avid TI undergoing 18FDG-PET/CT in this tertiary cancer referral center was relatively high (42%). This is probably due to the fact that the study was performed in a tertiary oncology referral center. In 38% of the analyzed patients, the cause of death was related to their nonthyroid primary cancer, in 4% to a noncancer related event, and one patient (0.1%) died from medullary thyroid cancer. Stratification for type of primary nonthyroidal malignancy showed a poor prognosis for lung, urothelial, and colon cancer patients whereas breast cancer patients had a favorable survival outcome. The nonthyroidal primary malignancies with an unfavorable prognosis were predominant in the control group. This strongly suggests that physicians in our cancer center select their patients for further 18FDG-avid TI diagnostic workup and possible treatment based on the expected survival time of their main oncologic diagnosis. The propensity-weighted analysis implies that the decision to not perform additional TI diagnostic tests does not harm patient survival and is a safe strategy for our study population.
The strengths of this study include the comprehensive assessment of the relevance of performing TI diagnostic evaluations in cancer patients. Further, the large size of 800 patients and long duration of follow-up add to the validity of this study. A limitation of this study is the retrospective nature and the exclusion of 20% of the patients due to lack of follow-up data. However, the retrospective nature of the study did enable us to have a long follow-up period of a rare pathology. The post hoc analyses should be considered hypothesis-generating and require independent validation.
Another limitation is that the decision to perform further investigation of a TI was made by the physician responsible for the primary nonthyroid cancer care. This also led to a lack of ultrasound evaluation in a large proportion of patients. The group of patients without additional ultrasound investigation is likely to harbor possible thyroid malignancies, but follow-up data show that these possible missed malignancies did not become clinically relevant. Further, a minority of patients underwent thyroid surgery and therefore had a final histological diagnosis available. Although FNAC has a high sensitivity, it is possible that malignancies were missed (26).
In conclusion, the incidence of TI in this tertiary cancer referral center was comparable to current literature. Further thyroid diagnostic analyses were performed in less than half of the patients, and only a minority of patients underwent thyroid surgery. Our current study did not identify relevant clinical predictors to select cancer patients with an 18FDG-avid TI for further diagnostic workup or surgery other than the type of the primary nonthyroidal malignancy and its associated survival. Since only one patient died from thyroid cancer, the strategy to withhold thyroid diagnostic workup and treatment seems valid for a large group of patients with a 18FDG-avid TI and a nonthyroid cancer diagnosis. In the presence of a treatable underlying malignancy, a full diagnostic workup according to the recent ATA guidelines and, if indicated, followed by surgery can be discussed in these patients (27). Thus, actively pursuing a TI might benefit a subgroup of patients in whom the primary nonthyroidal malignancy or disease is successfully treated or presumably stable. A wait-and-see policy with ultrasound follow-up could be an alternative strategy. These considerations should be part of the shared decision making in cancer patients with a TI.
Footnotes
Authors' Contributions
I.M.C.V.d.P. designed this project and supervised throughout the project. M.W.P. performed the analysis of the data and wrote the final article with input from all the authors. R.K. contributed to analytical calculations and verified the analytical methods. J.P.d.B., M.R.V., R.S.v.L., M.S., K.J.H., and F.V.D. contributed to the analysis of the results and to the writing of the article.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.