
Abstract
Background:
Little is known about the role of emotions in treatment decisions for thyroid cancer. We aimed to characterize the emotional content of patient–surgeon communication during decision-making about low-risk thyroid cancer treatment.
Methods:
We audio-recorded conversations about treatment for clinically low-risk thyroid cancer or biopsy suspicious for thyroid cancer between patients (n = 30) and surgeons (n = 9) in two diverse, academic hospitals in the United States. Inductive and deductive content analyses were used to characterize the emotional content in verbatim transcripts.
Results:
Patients' expression of emotion focused on primarily on their diagnosis and treatment outcomes. Patients commonly expressed negative emotions like fear and anxiety about “the C-word” and worried about the cancer growing or spreading. In response, most surgeons used education, as opposed to empathy or validation, to reassure patients, often highlighting low probabilities of adverse events. Surgeons emphasized the “slow-growing” nature and excellent prognosis of thyroid cancer compared with other malignancies. When discussing treatment options, surgeons often described alternatives in terms of their emotional outcomes. Some described total thyroidectomy as providing “peace of mind” or a “sense of completeness,” warning that cancer or thyroid tissue remaining in the body with active surveillance or lobectomy might “worry” or “bother” patients. Surgeons supported deliberation by reassuring patients that there are “two right answers” and “no rush” to decide.
Conclusions:
Patients express negative emotions during treatment decision-making. In response, surgeons often miss opportunities to provide empathy in addition to education. Surgeons and patients both acknowledge patient fear and anxiety as a reason to choose thyroidectomy instead of active surveillance. Peace of mind gained by patients and surgeons as a result of thyroidectomy may lead to overtreatment of patients with low-risk thyroid cancer.
Introduction
The majority of patients with low-risk thyroid cancer undergo total thyroidectomy, the treatment option with the greatest morbidity (1 –3). More recently, thyroid lobectomy and active surveillance have been shown to offer equivalent long-term survival in appropriately selected patients with significantly reduced morbidity (2,4). Yet, the majority of patients with low-risk thyroid cancer in the United States continue to undergo total thyroidectomy (5).
When diagnosed with low-risk thyroid cancer, patients must weigh the benefits, harms, and risks of treatment alternatives, consider their goals and preferences, and choose a treatment option that is right for them (6,7). This decision is complex and not solely based on cognitive processing of risk. Theories of decision-making demonstrate that emotions heavily influence choice and can bias perceptions of risk leading to decisions that do not align with one's preferences and values (8 –10).
At present, little is known about the role of emotions in treatment decisions for low-risk thyroid cancer. The aim of this study was to characterize the emotional content of patient–surgeon communication during decision-making about treatment for low-risk thyroid cancer or nodule suspicious for cancer. Because contemporary models of decision-making recognize that emotions can cause behavior to diverge from what makes sense rationally, this study provides a novel view into decisions that potentially over treat low-risk thyroid cancer (8,11).
Methods
Participants and setting
We conducted this study at two academic hospitals in the United States (Madison, WI; New York, NY) to increase geographic, institutional, and practice variability. We invited all attending surgeons who perform thyroidectomy at both institutions to participate. Participating surgeons provided written consent before patient recruitment to participate in a study about “how surgeons and patients communicate about treatment decisions for thyroid cancer.” Adult patients (>17 years old) were eligible to participate if they were being treated by a consented surgeon, English-speaking, and had low-risk thyroid cancer defined as a biopsy proven papillary thyroid cancer or cytology suspicious for papillary thyroid cancer (Bethesda V or VI), size <4 cm, no evidence of suspicious lymphadenopathy on physical examination or ultrasound, and no evidence of extrathyroidal extension. Patients with a history of thyroid surgery were excluded. Patients and surgeons were both blinded to the study's goal to characterize the emotional content of communication. The Institutional Review Board at each institution approved this study.
Data collection
Eligible patients were invited to participate by mail or immediately before their visit. Written consent to participate in a study about “how surgeons and patients talk and make decisions about thyroid cancer treatment” was obtained by trained research team members in person before the visit. Preoperative patient–surgeon consultations (with family members, if present) were audio-recorded and transcribed verbatim. All identifiers were removed from transcripts before analysis. Participants (surgeons and patients) did not have access to study data or results. Data collection continued until no new themes emerged and data saturation was reached. Patients also completed a brief survey before and after the visit that included demographics, a validated Cancer Worry scale adapted by replacing the word “breast” with “thyroid,” and the intended treatment choice (12,13). The Cancer Worry scale assessed level of worry about being diagnosed with thyroid cancer on a 5-point scale ranging from not at all (1) to almost all the time (5) and the impact of worry on mood and daily functioning on a 4-point scale ranging from not at all (1) to a lot (4). Surgeons completed a brief demographic survey at the time of consent.
Analysis
We used a hybrid model of inductive and deductive content analysis to analyze each transcript. The Risk as Feelings framework guided our deductive analysis (8). This well-known model describes the following: (1) how emotions and cognition work in concert to determine behavior and (2) how emotions exert a strong and powerful influence on cognition when emotional and cognitive evaluations of risk diverge. Coding was completed by a diverse team with backgrounds in endocrine surgery (S.C.P.), social psychology (C.I.V.), sociology (M.C.S.), and education (A.R., not a co-author) and included a member with a history of thyroid cancer. At least three team members coded each transcript and discussed codes and emergent themes until consensus was reached. The coding taxonomy was iteratively revised throughout the analytic process. NVivo 12 software (QSR International) was used to catalog data.
Higher level analysis examined quotes coded as “patient expression of emotion” or “surgeon response to emotion” and included analytical memos about subthemes within these categories. To characterize the role emotion plays in decision-making, we queried additional codes related to “anticipating future outcomes,” “reacting to potential outcomes,” “painting a picture, “patient typology,” and “treatment preference” and mapped out the timing of emotional expression (i.e., prediagnosis, diagnosis, treatment decision-making, and anticipated future emotions). The research team met throughout the analytic process to discuss memos and summaries of the data. Patient quotes are identified by study number, self-reported sex, and age. Surgeons are not identified to preserve anonymity.
Results
Patients (n = 30) had a median age of 48.5 years (range 20–71). Most were white (86.7%) and women (80.0%). Surgeons (n = 9) had been in practice 2–50 years; 66.7% were men and 66.7% white (Table 1). Overall, 81.0% of patients worried about their cancer often or sometimes. Worry somewhat affected the mood of 42.1% of patients and somewhat affected the ability to perform daily activities of 10.5%.
Demographic Data
In the conversations, patients and surgeons both expressed and acknowledged the role of emotion in treatment decisions. Expression of emotion occurred around specific themes as explained hereunder.
Patient expression of emotion
During the consultations, emotions expressed by patients focused on two aspects of care: (1) diagnosis and (2) treatment outcomes. Temporally, these emotions represented those currently being experienced by patients as well as emotions patients anticipated experiencing in following treatment. Some patients expressed emotions about the treatment options themselves and other aspects of care, but these were less prominent.
Diagnosis
With respect to diagnosis, patients commonly expressed fear, worry, and uncertainty about “the C-word.” Some patients expressed emotions overtly by stating, “I'm worried…” or “It's scary…” (P4, female, 48) and explicitly named their emotion: “anxiety,” “nervous,” “concern,” “foggy,” “stress,” “thrown off,” or feeling “dire.” Other patients expressed emotions indirectly with statements like, “I've got something in me that shouldn't be there” (P6, female, 54) or by asking questions, such as, “Is it possible this could be in my lymph nodes?” (P26, female, 53). These types of questions appeared cognitive on the surface, but also indicated worry about the stage or extent of the cancer. Emotions expressed indirectly included shock; surprise; the need for reassurance, certainty, or safety; and feeling overwhelmed by their diagnosis, the amount of information provided, or misinformation on the internet. Patients also described symptoms of distress, such as difficulty sleeping or eating (Table 2).
Domains and Examples of Patient Expression of Emotion

Treatment outcomes
Patients additionally expressed worry about anticipated treatment outcomes, such as the cancer growing or spreading if the cancer was not removed quickly. Patients commonly described this concern directly stating, “My biggest concern is spreading…” (P17, female, 50). Patients also expressed concerns about scarring; gaining weight after thyroidectomy; potential complications, such as voice changes; cancer outcomes, including recurrence and survival; the possibility of completion thyroidectomy; and the need for thyroid hormone (Table 2). The concern about outcomes was sometimes related to general health and well-being. For example, patient 18 stated, “My biggest concern is what it is going to be like after. Like, will I feel normal eventually?” (female, 33).
Other aspects of care
Although the majority of patient emotions were expressed about diagnosis or anticipated treatment outcomes, they did express emotions about other aspects of care (Table 2). Patients expressed worry and anxiety about their recent biopsy, treatment options, the need to make a decision, timing of surgery, and anesthesia. Misbeliefs about cancer and past experiences with cancer also influenced patients' emotions (Table 2). The effect of past experiences depended on the nature of the experience; some provided reassurance, whereas others increased anxiety or the intensity of the emotion.
Surgeon response to patient emotion
During the conversations, surgeons' responses to patients' emotions often provided reassuring information that required cognitive processing, leading them at times to miss the opportunity to directly provide empathy. Some surgeons also addressed emotions they believed the patient might experience, but had not been expressed by the patient during the visit, or expressed their own concerns.
Reassurance with information
Surgeons most frequently responded to patients' current emotions with information intended to be reassuring (Table 3). They often highlighted that thyroid cancer is “slow-growing,” very “curable” or “one of the best cancers to have.” One surgeon compared thyroid cancer, the “small c” with other cancers, the “big C,” whereas another used a metaphor describing thyroid cancer as a turtle or snail, compared with other cancers that were more like birds or rabbits (Table 3). Surgeons also used probabilities, risk estimates, and quoted research to convey the low likelihood or rarity of an event (Table 3). For example, one surgeon stated, “The death rate for thyroid cancer is ridiculously low. It's, like, 1 in hundreds of thousands of people.” Other commonly used qualitative descriptors included “rare,” “unlikely,” or “teeny, tiny little fraction.”
Surgeon Response to Emotion
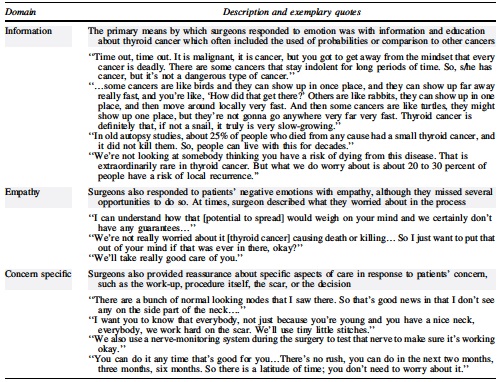
Response with empathy
Some surgeons responded to patients' emotions with empathy and validation, although this was less frequent. Surgeons acknowledged that a cancer diagnosis can be “scary,” that “nobody likes to hear the C-word,” and named patient's “anxiety” or “worry.” One emphasized that there is “no such thing as a good cancer” and acknowledged when “you hear the word ‘cancer’…4-letter words come out of your mouth.” Surgeons also provided empathy through nonabandonment, resources, and physical contact (Table 3). For example, one surgeon stated, “I'm going to get you that [support group] stuff, and I'm going to give you a hug because we've got this. Okay? We are going to get you through it.” Surgeons rarely directly asked patients how they were feeling or coping.
Other expression of surgeon emotion
Surgeons also expressed their own emotions during the decision-making conversations independent of patient expression of emotion. These instances primarily occurred when surgeons were educating patients about complications and shared their “worry” or “concern” about a potential adverse event (Table 3). Some used rhetorical questions like, “Do you know what I worry about?”
Emotion in decision-making
In addition to patients' expression and surgeons' responses, emotions played a significant role during decision-making, particularly with respect to anticipated outcomes and emotions.
Patient decision-making
Anxiety and worry (negative emotions) were the dominant emotions expressed by patients during treatment decision-making about low-risk thyroid cancer. Patients made assertions such as, “I would prefer just to do all of it. Just get it done and not worry about it” (P21, female, 54). They often expected thyroidectomy (lobectomy or total) and removal of cancer would resolve their anxiety and worry they were experiencing (Table 4). Patients anticipated that removal of the cancer would provide them with peace of mind, reassurance, and a sense of certainty. This emotional forecasting was often reinforced by surgeons. Patient-initiated discussion of worry about recurrence was rare.
Discussion of Emotions During Decision-Making About All Three Treatment Options for Low-Risk Thyroid Cancer
When discussing active surveillance, patients most commonly expressed worry about the cancer progressing. For example, one patient said, “I think I personally would want it removed because knowing that I have cancer inside of me and that it can grow, and I already have anxiety” (P22, female, 55). However, some patients expressed a dislike of surgery and indicated comfort with the idea of active surveillance (Table 4). Of note, some patients who initially expressed anxiety about surveillance eventually chose monitoring in lieu of immediate surgery when they were reassured by the surgeon.
Surgeon decision-making
When discussing treatment options, surgeons often described or framed the alternatives in terms of their anticipated emotional outcomes (benefits or drawbacks) regardless of whether patients expressed emotions or preferences about treatment options first. When describing total thyroidectomy, surgeons often emphasized that the procedure has the potential to resolve negative emotions by eliminating the cancer (Table 4). For example, one surgeon stated, “Reasons to take the whole thyroid out are number one, some people like the sense of completeness…” Another surgeon said, “…a lobectomy may not give you the peace of mind you're looking for,” and emphasized potential, “worry…about watching the other lobe.” Some surgeons also favored selecting total thyroidectomy because of worry about remaining contralateral nodules. One surgeon explained, “Whenever there are many nodules…we take the whole thyroid out, because that other nodule will keep haunting you.” This belief about contralateral nodules was not universal. Another surgeon stated, “Reasons to consider a lobectomy, it takes out the cancer and the worrisome nodules obviously, [but] I'm not really worried about those [contralateral nodules].” Worry about recurrence was also described by surgeons as a reason for total thyroidectomy. One surgeon stated: “The advantage to taking the whole thing is that it's easier to monitor you if you're worried about recurrence.”
When discussing less extensive treatment options, surgeons also described anticipated emotional outcomes (Table 4). Some warned that cancer or thyroid tissue remaining in the body after a lobectomy or during active surveillance might “worry” or “bother” patients, and stated that it was reasonable to choose a more extensive option if the patient thought a less extensive treatment would be too stressful. One surgeon addressed patients' potential worry by stating, “You may ask ‘well, what if, in the period I'm watching it, it spreads all over my body and I can no longer remove it anymore?’ That just has not been the case.” Some surgeons who encouraged active surveillance also talked about how patients would not have to “worry” about thyroid hormone replacement, scarring, or poor surgical outcomes. They highlighted that surgery remained an option during surveillance if the cancer grew, spread, or the patient experienced excessive anxiety. For example, one surgeon stated, “If you do progress [on surveillance], then [we] will refer you back for surgery… we have not ever regretted the delay in the surgery.”
When it was time to make a treatment decision, surgeons frequently provided reassurance by emphasizing that there is “no rush” to make a decision (Table 3). One surgeon stated, “I tell people we've got two right answers… If you're torn, you don't have to rush into surgery… you can think about it. There's no emergency.” Another expressed, “There's no wrong choice.” Patients appeared to respond positively to this approach to supporting deliberation.
Discussion
Emotions are known to influence how people interpret information and make decisions (8 –10). In this qualitative study performed at two institutions, emotions played a profound role in patient–surgeon decision-making about low-risk thyroid cancer treatment. Patients and surgeons both acknowledged that negative emotions, such as fear and anxiety, experienced by patients in response to diagnosis with thyroid cancer, represent a reason to choose thyroidectomy (lobectomy or total) over active surveillance. Total thyroidectomy was often framed as treating or preventing negative emotions, whereas active surveillance was described as potentially increasing or inducing negative emotions. Peace of mind from removing the cancer was often seen by patients and surgeons as an anticipated benefit of thyroidectomy, making it both a patient- and surgeon-centered outcome. These emotions expressed during decision-making about low-risk thyroid cancer treatment appear to support decisions that potentially overtreat these cancers while representing a barrier to lobectomy or active surveillance.
This study is the first to qualitatively characterize the influence of currently experienced and anticipated emotions on decisions about low-risk thyroid cancer treatment in recently diagnosed patients. Previous studies on emotion in those with thyroid cancer have primarily been cross-sectional, quantitative, and focused on worry in survivors (14 –17). According to behavioral theory, both current and anticipated emotions exert a dominant effect over cognition in the decision-making process by biasing perceptions of risk and other cognitive inputs (8). Our finding that surgeons commonly use information and probabilities as reassurance in response to patients' fear and anxiety is important, because this strategy may leave patients unsupported and allow their emotions to overly influence decisions.
Previous studies suggest that patients with thyroid cancer have unmet psychosocial support needs at the time of diagnosis despite 92% of physicians who treat thyroid cancer reporting that their patients are at least somewhat worried (18 –22). Therefore, providing increased empathy and emotional support may be an effective strategy to meet patients' needs and increase patient preference for less invasive management. A mixed-methods study assessing the experience of those undergoing less invasive management with active surveillance in Japan showed that levels of worry were relatively low among participants (23). In addition, 60% of participants reported lower worry than prediagnosis (23). Because worry is an emotion that is experienced in response to anxiety or a concern about an issue (whether real or imagined) and a natural response to an anticipated future problem, adequate emotional support may be a strategy to reduce worry in those with thyroid cancer undergoing active surveillance or survivors following surgery (24).
Emotions have similarly been shown to influence treatment decisions in patients with low-risk breast and prostate cancer (10,11,25 –29). Women with breast cancer who have higher levels of fear and anxiety are more likely to undergo contralateral prophylactic mastectomy despite the lack of a survival benefit and increased risk of complications (30,31). Men with low-risk prostate cancer with increased anxiety are more likely to choose active treatment over active surveillance despite risks like impotence, urinary incontinence, and decreased quality of life (32). Findings in these patient populations similarly point toward the influence of peace of mind gained from more extensive treatment (29,33 –35). Beliefs about cancer in the general population and past experiences likely contribute greatly to the similarities among the three diseases (36).
One important finding of our study was that peace of mind also appears to be a surgeon-centered outcome. Following total thyroidectomy, uncertainty about cancer recurrence is reduced because physicians can monitor thyroglobulin levels. This benefit may come at the expense of patient quality of life and increased risk for complications. Additional research is needed in this area as physician recommendations heavily influence patient choice and may support overtreatment (37). Physicians should remain cognizant of the potential effect of their own biases and beliefs on clinical decision-making.
Emotions and their intensity have also been shown to decrease information recall and increase perceptions of disease severity (38,39). Therefore, recognizing and addressing patients' concerns has the potential to improve their comprehension and ability to participate in shared decision-making. For low-risk thyroid cancer, such improvements may lead to different treatment decisions and increased uptake of less extensive management options. Studies are needed to investigate the effect of emotional support on recall and treatment decisions in this population.
Strengths of this study include the multi-institutional design and heterogeneity of surgeon training and practices. This study also has limitations. Audio recordings were completed at two high-volume, academic institutions whose practices may not reflect other settings, and whose patients were predominantly White and may not represent the general population. Patients may have had previous discussions with their endocrinologist and family/friends or performed independent research that influenced their mindset at the time of consultation. Dynamics of the patient–surgeon relationship related to race, ethnicity, gender, or sex may also have impacted the discussions. Studies have shown that demographic concordance or lack thereof affects communication, patient participation, and satisfaction (40). The background and theoretical orientation of the research team may also have impacted the interpretation of data. Although awareness of audio recording may have influenced conversation content or emotion expression, studies show that audio recording physicians have minimal or no effect on their behavior (41). The combined inductive and deductive approach attempted to mitigate researcher bias.
Conclusions
These data demonstrate that negative emotions play a significant role in treatment decision-making for low-risk thyroid cancer. These findings are critically important because better emotional support at the time of diagnosis and during treatment decision-making have the potential to decrease unnecessarily extensive surgery and promote active surveillance for appropriate patients. Interventions that provide peace of mind without thyroidectomy by increasing the ability of patients to cope with their diagnosis have the potential to reduce overtreatment and promote active surveillance for low-risk thyroid cancer. Such patient-oriented interventions could be either directly aimed at patients or mediated by medical professionals.
Footnotes
Acknowledgments
The study team thanks Alexandra Rosser, BS for her assistance coding. A portion of this study was presented virtually at the 42nd Annual Meeting of the Society for Medical Decision Making on October 20, 2020. The abstract is published online at:
Authors' Contributions
All authors have reviewed and approved this article and meet the International Committee of Medical Journal Editors (ICMJE) criteria for authorship.
Author Disclosure Statement
The authors have no competing or personal financial interests to disclose.
Funding Information
This study was funded by K08CA230204 the National Institutes of Health/National Cancer Institute. PI: Dr. Susan Pitt. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health. Effort on this grant was provided by a Research Career Scientist award to Dr. Voils from the Health Services Research and Development Service of the Department of Veterans Affairs (RCS 14-443). Dr. Roman is supported in part by the Cancer Center Support Grant P30 CA008748 from the National Institutes of Health/National Cancer Institute.