
Abstract
Background:
The adverse impact of maternal negative TPOAb of gestational subclinical hypothyroidism (SCH-TPOAb−) on the development of the offspring has not yet been clearly identified. A lingering controversy exists over the treatment of SCH-TPOAb− diagnosed during pregnancy. Therefore, this study was designed to evaluate the intellectual development of children of mothers who had SCH-TPOAb−.
Methods:
A number of 139 children were recruited; 112 children were born to SCH TPOAb− and 27 children were born to euthyroid TPOAb− mothers. Based on the mothers' thyrotropin (TSH) levels during pregnancy and whether or not they received levothyroxine (LT4) treatment, the children were assigned to four groups: Group A (2.5 mIU/L < TSH ≤4.0 mIU/L, n = 31) and Group B (4.0 mIU/L < TSH ≤10.0 mIU/L, n = 26), whose mothers were treated with LT4 before eight gestational weeks, and Group C (2.5 mIU/L < TSH ≤4.0 mIU/L, n = 27) and Group D (4.0 mIU/L < TSH ≤10.0 mIU/L, n = 28), whose mothers received no treatment. A total number of 27 children whose mother's serum TSH was <2.5 mIU/L and were TPOAb− during their pregnancy served as the control group (Group E). The intellectual development of two-year-old children was assessed and compared using the Gesell Development Diagnosis Scale.
Results:
The developmental quotient (DQ) in Group D was 8.67 lower than this in Group E (p < 0.001). More specifically, gross motor quotient, fine motor quotient, adaptability quotient (ABQ), language quotient (LQ), and individual social behavior quotient (ISBQ) of DQ in Group D were significantly lower than those in Group E. No significant differences were observed in DQ among Group A, Group B, Group C, and Group E (p > 0.05). Spearman's rank correlation analysis showed that DQ, FMQ, ABQ, LQ, and ISBQ were significantly negatively correlated with the TSH level (r = −0.417, −0.253, −0.273, −0.436, and −0.272; p < 0.05). In addition, multivariate logistic regression analysis revealed that mothers' education (short education), mothers' education (medium education), and TSH level (4.0 mIU/L < TSH ≤10.0 mIU/L) were both risk factors affecting the intellectual development of the offspring (p < 0.05).
Conclusion:
The effects of the intellectual development of the offspring with SCH-TPOAb− are related to the level of TSH. Standardized treatment for SCH-TPOAb− pregnant women before eight gestational weeks, whose TSH level was from 4.0 to 10.0 mIU/L, may significantly improve the intellectual development levels of the approximately two-year-old offspring. Although our study was a historical cohort study, the data analyzed provide the foundation for further investigation. Further prospective intervention trials with large numbers of participants are needed to confirm our conclusions. The Clinical Trial Registration number is 2021-K-84-02.
Introduction
Subclinical hypothyroidism (SCH) is characterized by an elevated thyrotropin (TSH), accompanied by normal free thyroxine (fT4) levels. Results regarding whether a mildly elevated TSH concentration could increase adverse pregnancy outcomes have been vigorously debated (1,2). Therefore, the definitions of SCH in pregnancy have been changed in recent years. The 2011 “Guidelines of the American Thyroid Association (ATA) for the Diagnosis and Treatment of Thyroid Disease During Pregnancy and the Postpartum” recommended that the ideal upper limit of serum TSH was 2.5 mIU/L in early pregnancy (3), but a higher cutoff value of 4.0 mIU/L was recently proposed in the 2017 the ATA's guidelines (4).
Endocrinologists have not yet reached a consensus on whether to treat women with negative TPOAb of gestational subclinical hypothyroidism (SCH-TPOAb−). The Endocrine Society recommends therapy in all pregnant women with SCH, irrespective of their autoimmunity status (5). On the contrary, ATA supports the treatment of a specific subgroup of women with SCH who are TPOAb+ (SCH-TPOAb+) or TPOAb− but with TSH levels >10 mIU/L (4). However, no intervention trial has assessed the levothyroxine (LT4) impact, specifically in SCH-TPOAb− pregnant women. In 1999, scientific interest in undiagnosed maternal thyroid dysfunction was attracted by the results of studies suggesting an association between subclinical thyroid hypofunction and impaired fetal neuropsychological development (6,7).
Two large randomized controlled trials investigating the effect of treatment in women experiencing SCH have failed to show any improvement in the cognitive function of the offspring (8,9). It is worth noting that neither of the above-mentioned two randomized controlled trials described the TPOAb status. Therefore, the adverse impact of maternal SCH-TPOAb− on the development of the offspring has not yet been clearly identified. Therefore, this study was designed to evaluate the effect of maternal SCH-TPOAb− on possible intellectual deficits in the offspring.
Materials and Methods
Study population
This was a historical cohort study conducted at the Second Affiliated Hospital of Wenzhou Medical University (Wenzhou, Zhejiang, China) from June 2016 to June 2019. Women with a singleton gestation presenting for care before eight gestational weeks underwent thyroid and TPOAb screening. Women with a serum TSH concentration between 2.5 and 10 mIU/L and fT4 and TPOAb in the normal range were considered to be SCH-TPOAb−. Pregnant women with pregnancy complications including cardiac disease, hepatic disease, renal insufficiency, and abnormal hematopoietic system were excluded. All subjects signed written informed consent forms. A comprehensive questionnaire, including the demographics and reproductive, medical, and prenatal history, as well as the feeding patterns and parents' education level, was completed during a face-to-face interview.
LT4 treatment
Women in the SCH treatment group received LT4 ( Merck KGaA, Darmstadt, Germany) on the second day after the diagnosis with SCH. The median gestational age at the start of the LT4 treatment was six gestational weeks and four days. The thyroid function was reexamined every two weeks. Based on the examination results, the dosage was adjusted to maintain the TSH level between 0.5 and 2.0 mIU/L.
Assessment of intellectual development of children
The Chinese version of the Gesell Development Diagnosis Scale (GDDS) was used to evaluate the intellectual development of two-year-old infants. The GDDS was designed to diagnose the psychological development of children in the age range from four weeks to three years (10). The test was divided into five subtests. Each subtest examined a different aspect of developmental: gross motor quotient (GMQ), fine motor quotient (FMQ), adaptability quotient (ABQ), language quotient (LQ), and individual social behavior quotient (ISBQ). The mean values were expressed by the developmental quotient (DQ). The mean DQ was 100 points with a standard deviation (SD) of 15 points. A developmental score of above −1 SD (≥85) was regarded as average development, between 1 and 2 SDs below the average (85–70) was regarded as borderline development, and <2SD (≤69) as a significant developmental delay (11).
Cognitive performance tests were performed by expert psychologists at the Institute of Cognitive Sciences of the Second Affiliated Hospital of Wenzhou Medical University (Wenzhou, Zhejiang, China). The examiner was unaware of the result of mothers' thyroid function during pregnancy. The protocol was reviewed and approved by the Ethics and Research Committee of the Second Affiliated Hospital of Wenzhou Medical University.
Statistical analysis
Statistical analysis was performed using SPSS 26.0 for Windows. The measurement data are expressed as mean ± SD (x ± s). Analysis of variance was applied to find the significance of study parameters among three or more groups of patients for normally distributed data. In addition, a Fisher's LSD test was used for post hoc analyses. Categorical variables were assessed using Pearson's chi-squared test. Spearman's correlation test was adopted to evaluate the correlation among non-normally distributed data. Odds ratio (OR) was determined by ordered logistic regression analysis. A two-sided p-value <0.05 was considered to indicate statistically significant difference.
Results
Study population
From June 2016 to June 2019, a total of 5383 pregnant women underwent thyroid function tests (including thyroid antibody tests) before eight weeks of pregnancy. The median and reference ranges of serum TSH, free triiodothyronine (fT3), and fT4 for pregnant women in our hospital before eight weeks of pregnancy were 1.12 mU/L (0.11–4.07 mU/L), 3.16 pg/mL (2.49–4.63 pg/mL), and 1.26 ng/dL (0.99–1.98 ng/dL), respectively. The positive rate of TPOAb was 13.4%. A total of 4762 women (88.5%) had results that were considered to be normal, 41 (0.76%) had overt hyperthyroidism, 55 (1.02%) had overt hypothyroidism, 65 (1.21%) had SCH-TPOAb+, and 89 (1.65%) had other types of thyroid dysfunction. A total number of 371 women were diagnosed with SCH-TPOAb−. They voluntarily chose to receive LT4 on the second day after their diagnosis with SCH, or did not take LT4 during the whole gestation.
Among the 163 pregnant women in the SCH treatment group, 69 were excluded owing to treatment abandonment, failure to follow the doctor's advice to adjust the LT4 dose, or for other reasons. Meanwhile, among the 208 pregnant women in the SCH observation group, 111 were excluded owing to midway treatment, nonregular thyroid function screening, or other reasons. Eventually, the remaining 191 pregnant women met the inclusion criteria of our study. According to TSH levels and whether or not they received LT4 treatment, the SCH-TPOAb− pregnant women were divided into four groups: Group A (2.5 mIU/L < TSH ≤4.0 mIU/L, n = 53) and Group B (4.0 mIU/L < TSH ≤10.0 mIU/L, n = 41), who were treated with LT4 before eight gestational weeks, and Group C (2.5 mIU/L < TSH ≤4.0 mIU/L, n = 45) and Group D (4.0 mIU/L < TSH ≤10.0 mIU/L, n = 52), who received no treatment.
A number of 31 (58.5%), 26 (63.4%), 27 (60.0%), and 28 (53.8%) children completed the GDDS assessment at 24 months in groups A, B, C, and D, respectively (Fig. 1). There were no differences in the refusal rate among the four groups. Twenty-seven children whose mother's serum TSH was <2.5 mIU/L and were TPOAb− in their pregnancy served as the control group (Group E).
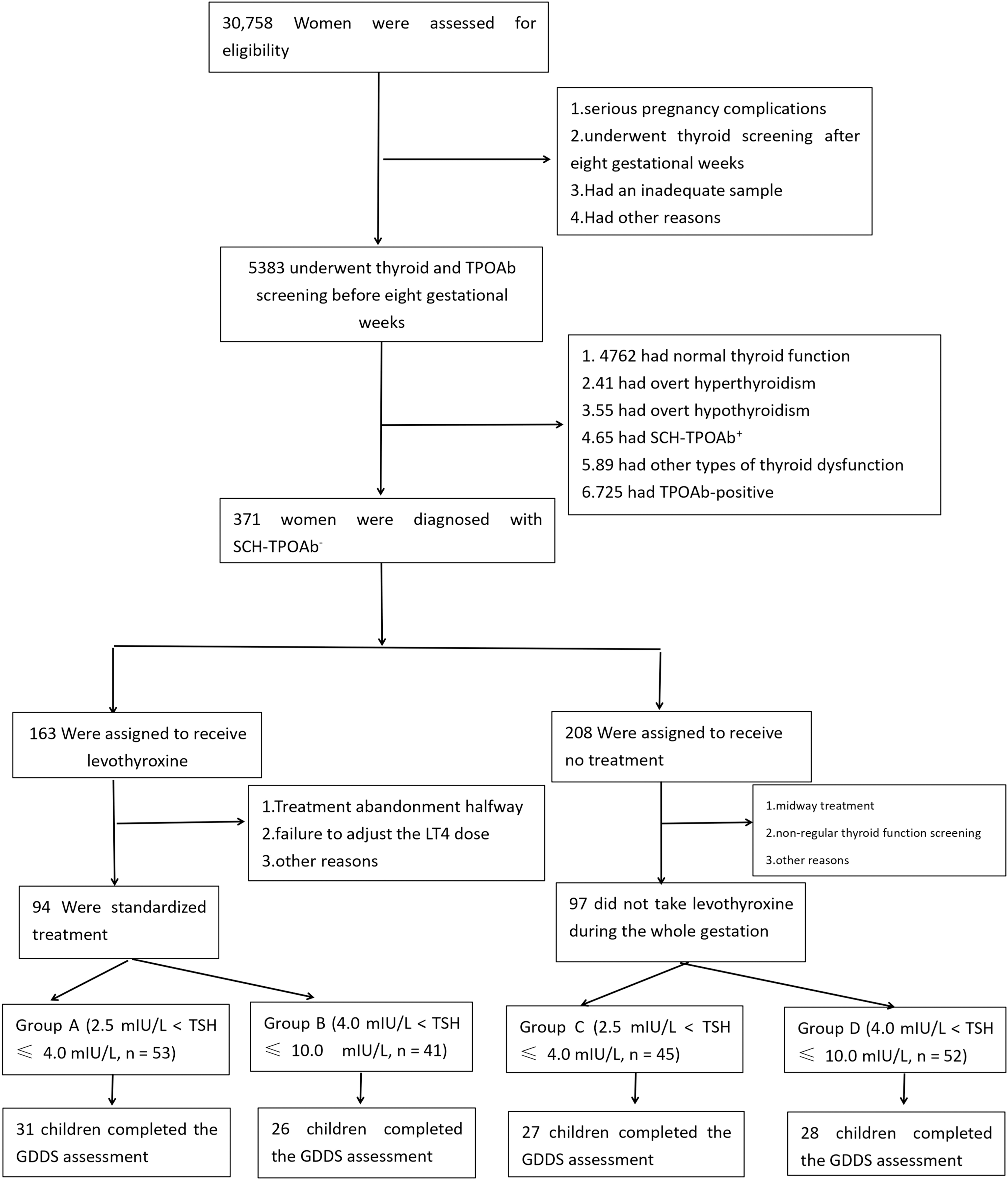
From June 2016 to June 2019, a total of 30,758 pregnant women assessed for eligibility. A total of 5383 pregnant women underwent thyroid function tests (including thyroid antibody tests) before eight weeks of pregnancy. The median and reference ranges of serum TSH, fT3, and fT4 for pregnant women in our hospital before eight weeks of pregnancy are 1.12 mU/L (0.11–4.07 mU/L), 3.16 pg/mL (2.49–4.63 pg/mL), and 1.26 ng/dL (0.99–1.98 ng/dL), respectively. The positive rate of TPOAb was 13.4%. A total of 4762 women (88.5%) had results that were considered to be normal, 41 (0.76%) had overt hyperthyroidism, 55 (1.02%) had overt hypothyroidism, 65 (1.21%) had SCH-TPOAb+, and 89 (1.65%) had other types of thyroid dysfunction. A total number of 371 women were diagnosed with SCH-TPOAb−. They voluntarily chose to receive LT4 on the second day after their diagnosis with SCH, or did not take LT4 during the whole gestation. Among the 163 pregnant women in the SCH treatment group, 69 were excluded owing to treatment abandonment, failure to follow the doctor's advice to adjust the LT4 dose or for other reasons. Meanwhile, among the 208 pregnant women in the SCH observation group, 111 were excluded owing to midway treatment, nonregular thyroid function screening or other reasons. Eventually, the remaining 191 pregnant women met the inclusion criteria of our study. According to TSH levels and whether or not they received LT4 treatment, the SCH-TPOAb− pregnant women were divided into four groups: Group A (2.5 mIU/L < TSH ≤4.0 mIU/L, n = 53) and Group B (4.0 mIU/L < TSH ≤10.0 mIU/L, n = 41), who were treated with LT4 before eight gestational weeks, and Group C (2.5 mIU/L < TSH ≤4.0 mIU/L, n = 45) and Group D (4.0 mIU/L < TSH ≤10.0 mIU/L, n = 52), who received no treatment. A number of 31 (58.5%), 26 (63.4%), 27 (60.0%), and 28 (53.8%) children completed the GDDS assessment at 24 months in groups A, B, C, and D, respectively. fT3, free triiodothyronine; fT4, free thyroxine; GDDS, the Gesell Development Diagnosis Scale; LT4, levothyroxine; TSH, thyrotropin.
Basic clinical characteristics of the parents
Highest attained educational level was divided into three categories according to the International Standard Classification of Education (ICSED) levels: short education (primary or upper secondary education), medium education (>4 years: vocational education), and long education (≥4 years: bachelor's or master's degree or a shorter cycle of higher education). The average age of pregnant women was 20–28 years. Breastfeeding was the most common feeding pattern of offspring aged within six months. The proportion of long-term education of parents in the offspring of the SCH treatment group (Group A and Group B) was higher than that of the observation group (Group C and Group D) and normal control group (Group E), but without a statistically significant difference. The effects of parental educational level, feeding pattern, and other factors on the intelligence of offspring were similar in our study, supporting the comparability of data among the five groups (Table 1).
Basic Clinical Characteristics of Parents in the Five Groups
Group A: Women with SCH-TPOAb−, whose TSH ranged from 2.5 to 4.0 mIU/L, treated with LT4 before eight gestational weeks. Group B: Women with SCH-TPOAb−, whose TSH ranged from 4.0 to 10.0 mIU/L, treated with LT4 before eight gestational weeks. Group C: Women with SCH-TPOAb−, whose TSH ranged from 2.5 to 4.0 mIU/L, received no treatment. Group D: Women with SCH-TPOAb−, whose TSH ranged from 4.0 to 10.0 mIU/L, received no treatment. Group E: normal control group.
Short education: primary or upper secondary education. Medium education: >4 years: vocational education. Long education: ≥4 years: bachelor's or master's degree or shortcycle higher education.
Data values are presented as mean ± SD. The prevalence of parents' educational level and feeding patterns were compared using chi-square tests. p < 0.05 was considered statistically significant.
LT4, levothyroxine; SCH-TPOAb−, negative TPOAb of gestational subclinical hypothyroidism; SD, standard deviation.
Perinatal outcomes of SCH-TPOAb−
In our study, no difference was found in the average gestational age of the five groups (39.13 ± 1.12, 38.17 ± 2.93, 39.14 ± 1.11, 39.07 ± 1.43, and 39.07 ± 1.43, p > 0.05). In the SCH groups (both the observation and treatment groups), adverse perinatal outcomes were rare regardless of the TSH level. We observed no significant difference in the incidence of adverse perinatal outcomes in the five groups (p > 0.05). The effects of preterm birth, neonatal asphyxia, and other factors on the intelligence of offspring were similar in our study, suggesting the comparability of data among the five groups (Table 2).
Perinatal Outcomes of SCH-TPOAb-
Group A: Women with SCH-TPOAb−, whose TSH ranged from 2.5 to 4.0 mIU/L, treated with LT4 before eight gestational weeks. Group B: Women with SCH-TPOAb−, whose TSH ranged from 4.0 to 10.0 mIU/L, treated with LT4 before eight gestational weeks. Group C: Women with SCH-TPOAb−, whose TSH ranged from 2.5 to 4.0 mIU/L, received no treatment. Group D: Women with SCH-TPOAb−, whose TSH ranged from 4.0 to 10.0 mIU/L, received no treatment.Group E: normal control group.
Birth asphyxia (low Apgar score), premature labor (delivery between 28th and 37th gestational week), postpartum hemorrhage (blood loss >500 mL after delivery within 24 hours) and low birth weight (newborn weight <2500 g).
Data values are presented as mean ± SD. The prevalence of cesarean section, birth asphyxia, premature birth, postpartum hemorrhage, low birth weight were compared using chi-square tests. p < 0.05 was considered as statistically significant.
Physical development of the offspring
Well-trained staff of the Second Affiliated Hospital of Wenzhou Medical University measured children's height and weight. The difference in the height and weight of each child was calculated according to the World Health Organization standards for infant and young child growth (12) and expressed as a t-value. Although the weight-for-age values and height-for-age values of children in five groups were slightly higher than those in the WHO standards, the differences among the five groups were not statistically significant (p > 0.05). In our study, no adverse effect was observed in SCH during pregnancy on short stature and weight loss of offspring (Table 3).
Physical Development of Offspring in the Five Groups
Group A: Women with SCH-TPOAb−, whose TSH ranged from 2.5 to 4.0 mIU/L, treated with LT4 before eight gestational weeks. Group B: Women with SCH-TPOAb−, whose TSH ranged from 4.0 to 10.0 mIU/L, treated with LT4 before eight gestational weeks. Group C: Women with SCH-TPOAb−, whose TSH ranged from 2.5 to 4.0 mIU/L, received no treatment. Group D: Women with SCH-TPOAb−, whose TSH ranged from 4.0 to 10.0 mIU/L, received no treatment. Group E: normal control group.
The difference in height and weight of each child was calculated according to the World Health Organization standards for child growth, and expressed as height t-value and weight t-value.
Data values are presented as mean ± SD. p < 0.05 was considered statistically significant.
Neurobehavioral development of the offspring
The value of DQ in Group D was 8.67 lower than that in Group E (p < 0.001). The difference of DQ between the Group D and the Group E was mainly reflected in the following aspects: GMQ was lower by 7.00 (p < 0.05), FMQ was lower by 8.33 (p < 0.05), ABQ was lower by 9.08 (p < 0.05), LQ was lower by 13.86 (p < 0.01), and ISBQ was lower by 8.34 (p < 0.05). There were no statistically difference in DQ including GMQ, FMQ, ABQ, LQ, and ISBQ among Group A, Group B, Group C, and Group E (p > 0.05) (Table 4).
Gesell Development Diagnosis Scale Scores of Offspring in the Five Groups
Group A: Women with SCH-TPOAb−, whose TSH ranged from 2.5 to 4.0 mIU/L, treated with LT4 before eight gestational weeks. Group B: Women with SCH-TPOAb−, whose TSH ranged from 4.0 to 10.0 mIU/L, treated with LT4 before eight gestational weeks. Group C: Women with SCH-TPOAb−, whose TSH ranged from 2.5 to 4.0 mIU/L, received no treatment. Group D: Women with SCH-TPOAb−, whose TSH ranged from 4.0 to 10.0 mIU/L, received no treatment. Group E: normal control group.
p < 0.05 was considered as statistically significant.
ABQ, adaptability quotient; DQ, developmental quotient; GDDS, the Gesell Development Diagnosis Scale; GMQ, gross motor quotient; FMQ, fine motor quotient; ISBQ, individual social behavior quotient; LQ, language quotient.
We chose Group A and Group C to assess the effects of LT4 treatment on the neurobehavioral development of the offspring of pregnant women with SCH-TPOAb−, whose TSH values were between 2.5 and 4.0 mIU/L. The DQ score in Group C was 0.89 lower than that in Group A (p > 0.05). The values of GMQ, FMQ, ABQ, LQ, and ISBQ of DQ were not statistically significant different between the two groups (p > 0.05) (Table 5).
Gesell Development Diagnosis Scale Scores of Offspring in Group A and Group C
Group A: Women with SCH-TPOAb−, whose TSH ranged from 2.5 to 4.0 mIU/L, treated with LT4 before eight gestational weeks. Group C: Women with SCH-TPOAb−, whose TSH ranged from 2.5 to 4.0 mIU/L, received no treatment.
p < 0.05 was considered as statistically significant.
We chose Group B and Group D to assess the effects of LT4 treatment on the neurobehavioral development of the offspring of pregnant women with SCH-TPOAb−, whose TSH values were between 4.0 and 10.0 mIU/L. The DQ score in Group D was 8.84 lower than those in Group B (p < 0.001). Specifically, the following differences in DQ between Group B and Group D was mainly reflected in the following aspects: ABQ was lower by 10.50 (p < 0.01), LQ was lower by 14.91 (p < 0.001), and ISBQ was lower by 9.47 (p < 0.01) (Table 6).
Gesell Development Diagnosis Scale Scores of Offspring in Group B and Group D
Group B: Women with SCH-TPOAb−, whose TSH ranged from 4.0 to 10.0 mIU/L, treated with LT4 before eight gestational weeks. Group D: Women with SCH-TPOAb−, whose TSH ranged from 4.0 to 10.0 mIU/L, received no treatment.
p < 0.05 was considered as statistically significant.
Correlation analysis of TSH level and DQ, GMQ, FMQ, ABQ, LQ, and ISBQ
The results of Spearman's rank correlation analysis showed that DQ, FMQ, ABQ, LQ, and ISBQ were significantly negatively correlated with TSH (r = −0.417, −0.253, −0.273, −0.436, −0.272; p < 0.05) (Fig. 2).
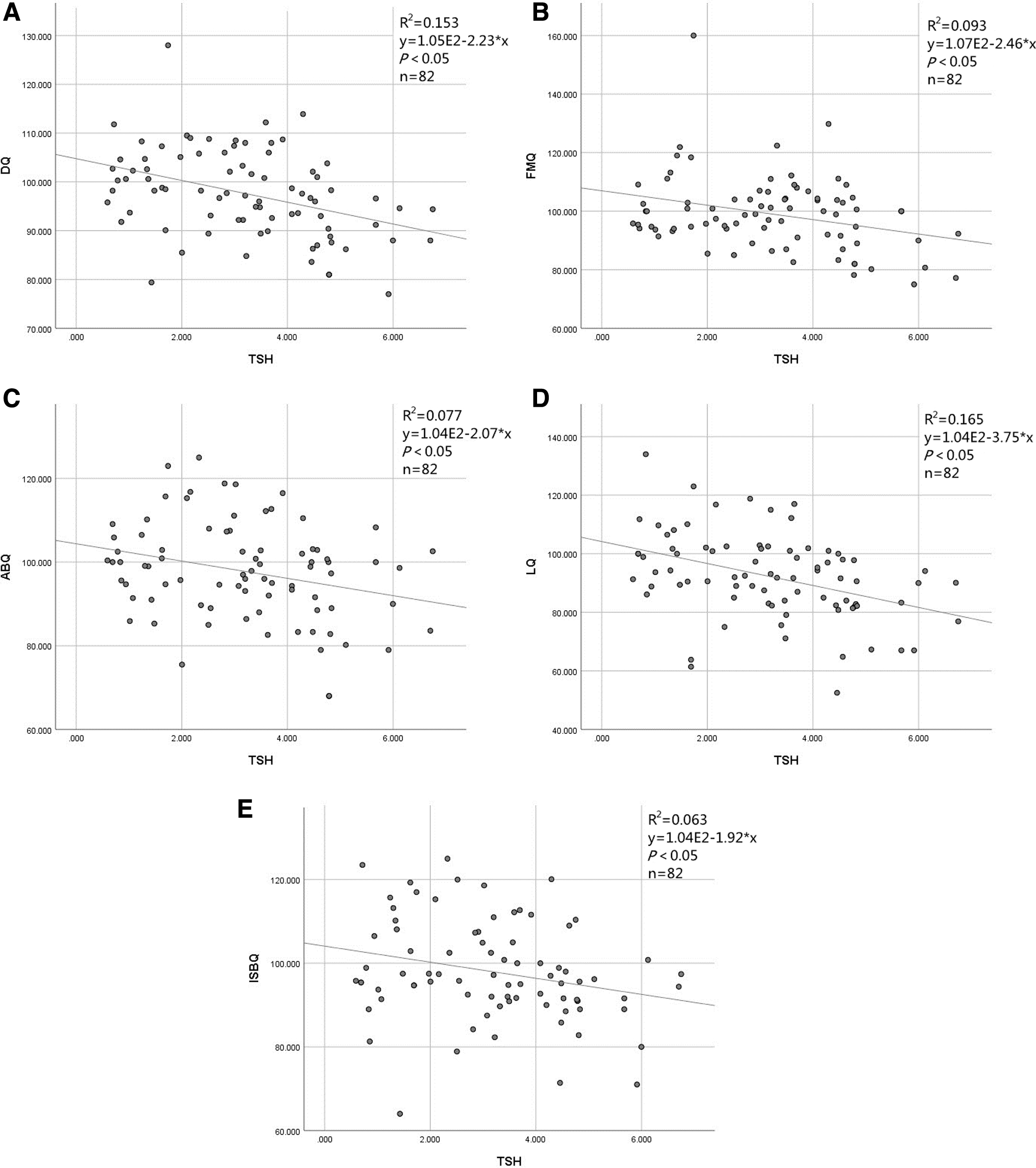
Correlation analysis of TSH level and DQ, GMQ, FMQ, ABQ, LQ, and ISBQ. (
Factors influencing the intelligence level of the offspring of SCH-TPOAb− mothers
The DQ values were categorized into three levels: 1 (>100 points), 2 (85–100 points), and 3 (<85 points). Parental education levels were also classified into three levels: 1 (short education), 2 (medium education), and 3 (long education). The feeding patterns in the first six months were divided into two categories: 1 (exclusive breastfeeding in the first six months) and 2 (milk powder feeding in the first six months or breastfeeding + milk powder). The feeding elders were divided into two levels, 1: parental feeding and 2: grandparent feeding or parental + group parental feeding. The TSH level was divided into three levels: 1 (4.0 mIU/L < TSH ≤10.0 mIU/L), 2 (2.5 mIU/L < TSH ≤4.0 mIU/L), and 3 (TSH ≤2.5 mIU/L).
In addition, the gender is categorized into two layers: 1 (male) and 2 (female). The Apgar score, birth weight, parental education level, feeding patterns, feeding elders, and gender were considered independent variables, and DQ was regarded as a dependent variable. Multivariate logistic regression analysis showed that mother's education (short education), mother's education (medium education), and TSH levels (4.0 mIU/L < TSH ≤10.0 mIU/L) were all risk factors affecting the intelligence level of the offspring (all p < 0.05), and ORs were 8.50, 3.82, and 12.48, respectively (Table 7). However, the birth status (based on Apgar score), birth weight, mothers' educational level (long education), fathers' educational levels, TSH level (TSH ≤4.0 mIU/L), breastfeeding or not in the first six months, parental feeding or not, and the gender were not risk factors affecting the intelligence level of the offspring (p > 0.05) (Table 7).
Influence Factors of Intelligence Level in the Offspring
DQ level = 1: DQ >100 points; DQ level = 2: DQ 85–100 points; mothers' education = 1: short education (primary or upper secondary education); mothers' education = 2: medium education (>4 years; vocational education); mothers' education = 3: long education (≥4 years: bachelor's or master's degree or a shorter cycle of higher education); fathers' education = 1: short education (primary or upper secondary education); fathers' education = 2: medium education (>4 years; vocational education); fathers' education = 3: long education (≥4 years: bachelor's or master's degree or a shorter cycle of higher education); TSH level = 1: 4.0 mIU/L < TSH ≤10.0 mIU/L; TSH level = 2: 2.5 mIU/L < TSH ≤4.0 mIU/L; TSH level = 3: TSH ≤2.5 mIU/L; feeding pattern = 1: exclusive breastfeeding in the first six months; feeding pattern = 2: milk powder feeding in the first six months or breastfeeding + milk powder; the feed elders = 1: parental feeding; the feed elders = 2: grandparent feeding or parental + group parental feeding; gender = 1: male; gender = 2: female.
OR = Exp (B); p < 0.05 was considered statistically significant.
B, regression coefficients; CI, confidence interval; OR, odds ratio.
Discussion
Thyroid hormone (TH) is essential for brain cell proliferation. Before gestational week 20, TH-dependent brain development fully or partly depends on maternal TH (13). A lingering controversy exists over the treatment of SCH diagnosed during pregnancy, questioning whether LT4 intervention may improve intelligence levels of the offspring. Conflicting results have been reported regarding the association between subclinical thyroid dysfunctions during pregnancy and the neurodevelopmental disorders in the offspring (7,14 –17). The following potential explanation for the uniform results can be considered: (i) Intervention time of LT4. No current evidence exists that LT4 treatment of pregnant women with SCH, especially when initiated after seven weeks of gestation, improves the neurocognitive functions in the offspring (8,9,18,19); (ii) Different trimester-specific reference upper limits for TSH; and (iii) Different thyroid peroxidase antibody status: more TPOAb+ impairment on the neurocognitive outcome in the offspring (20).
Investigations on the effect of maternal SCH-TPOAb− on the developmental status of the child have been rarely conducted. Moreover, the SCH diagnostic criteria have changed in recent years. The 2017 ATA guidelines (4) recommended revision of the upper reference limit of TSH for a prescription from 2.5 to 4.0 mIU/L. A previous study found that a cut-point of 4.0 mIU/L was suitable for diagnosing first-trimester gestational hypothyroidism in pregnant Chinese women (21). ATA supports LT4 treatment for a specific subgroup of women with SCH who are TPOAb− but with TSH levels >10 mIU/L, and no treatment is recommended for a TSH level between 2.5 and 4 mIU/L (4). Therefore, certain ambiguity is present concerning the feasibility of LT4 treatment for TSH levels between 4.0 and 10.0 mIU/L.
The key strength of this study is the assessment of the neurodevelopmental status of the offspring of SCH-TPOAb− women. We stratified using the TSH value and set up a control group without LT4 treatment and a normal control group. Our study results revealed that pregnant women with SCH-TPOAb− had a TSH of 4.0–10.0 mIU/L and the DQ value of their offspring was 8.67 points lower than that of the normal control group, without standard treatment before eight weeks of pregnancy. DQ was significantly lower in GMQ, FMQ, ABQ, LQ, and ISBQ. Conversely, early standardized treatment for these pregnant SCH-TPOAb− women (4.0 mIU/L < TSH ≤10.0 mIU/L) significantly improved the neurobehavioral development of their offspring, with no statistically significant difference in DQ between the values in GMQ, FMQ, ABQ, LQ, and ISBQ and those in the normal control group.
No significant differences were observed in DQ between the offspring of the SCH-TPOAb− mothers whose TSH values ranged from 2.5 to 4.0 mIU/L and that of the normal control group. In addition, our study also assessed the physical development of the offspring of SCH-TPOAb− women, revealing no statistically significant differences in the body weight or body length among the offspring of all studied subjects. Spearman's rank correlation analysis showed that DQ, FMQ, ABQ, LQ, and ISBQ were significantly negatively correlated with the TSH level. Certainly, the effect on the intellectual development is multifactorial. Our multivariate logistic regression analysis showed that mothers' education (short education), mothers' education (medium education), and TSH level (4.0 mIU/L < TSH ≤10.0 mIU/L) were both risk factors affecting the intellectual development of the offspring. We also performed adjustments for maternal age, parental education level, and fetal birth weight in each group.
The following limitations of this study should be acknowledged. First, this was a retrospective analysis, not a randomized trial. Therefore, the women who were diagnosed with SCH-TPOAb− voluntarily choose to receive or not receive treatment, and, although we did our best to adjust for the most obvious potential confounders, unknown confounders might have influenced our findings. Second, a potential selection bias might exist owing to the high rate of follow-up refusal and the small number of women included in the control group. Third, we measured the IQ of the children at a young age. Therefore, the children follow-up needs to be further improved. Finally, our study was single-center, and our sample size was not sufficiently large, which has affected its representativeness. Future multicenter studies with larger sample sizes and prospective approaches are thus warranted.
In summary, the intellectual development of the offspring with SCH-TPOAb− is related to the level of TSH of the mothers. The standardized treatment of pregnant SCH-TPOAb− women before eight gestational weeks whose TSH level is from 4.0 to 10.0 mIU/L may significantly improve the intellectual development levels of the approximately two-year-old offspring. Although this was a historical cohort study, our data provide supportive evidence for further investigation. Further multicenter studies with larger sample sizes and prospective approaches are needed to confirm and extend our findings.
Footnotes
Authors' Contributions
J.J.C.: Study design, execution, analysis, article drafting, and critical discussion. J.Z.: Study design and critical discussion. X.P.H.: Study design and analysis. S.Z.Z.: Study conception and design, interpretation of data, and critical revision. H.Q.X., P.P.Z. and T.Z.: data collection. Z.Y.X.: Study design, execution, analysis, manuscript drafting, and critical discussion. We declare that all authors participated sufficiently in the work and take public responsibility for its content.
Author Disclosure Statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Funding Information
This work was supported by a grant from the National Natural Science Foundation of China (No. 81771555) and the Science and Technology Project of Wenzhou City (No. Y20210326).