
Abstract
Background:
Thyroid peroxidase antibodies (TPO-Abs) play an important role in autoimmune thyroid disease, but are also prevalent in healthy individuals. However, it is unclear what determinants may influence the occurrence of TPO-Abs in healthy individuals and how TPO-Abs may affect health outcomes in these individuals. We aimed to identify determinants of TPO-Abs in a large, prospective population-based cohort of middle-aged and elderly individuals and to subsequently assess the association between TPO-Abs and risk of overall and cause-specific mortality.
Methods:
We performed binomial and multinomial logistic regression analyses to obtain odds ratios (ORs) and 95% confidence intervals [95% CIs] for the association of potential determinants based on previous literature with TPO-Ab positivity (>35 kU/L), TPO-Ab detectability (>5 kU/L), and TPO-Ab categories. Cox proportional hazards regression analyses were performed to obtain hazard ratios (HRs) and CIs for the association between TPO-Abs and mortality risk.
Results:
In 9685 participants (57% women, median baseline age 63.3 years, median follow-up time 10.1 years), we identified female sex (OR = 2.47 [CI 2.13–2.86]) and current smoking (OR = 3.10 [CI 2.66–3.62]) as determinants of TPO-Ab positivity and TPO-Ab detectability, respectively. Higher age (OR = 0.98 [CI 0.97–0.98]) and all categories of alcohol consumption (ORs ranging from 0.71–0.78) were associated with lower odds of TPO-Ab detectability. TPO-Ab detectability was associated with a higher risk of overall (HR = 1.09 [CI 1.01–1.17]), cancer-related (HR = 1.18 [CI 1.01–1.38]), and cardiovascular mortality (HR = 1.21 [CI 1.01–1.45]). Interestingly, this was more prominent in men compared with women (HR for cardiovascular mortality 1.50 vs. 0.99, respectively).
Conclusions:
In community-dwelling middle-aged and elderly individuals, female sex and current smoking are the most important determinants associated with TPO-Ab levels in the detectable and positive range, whereas alcohol consumption is associated with lower odds of TPO-Abs. The clinical importance of detectable TPO-Ab levels is illustrated by the association with an increased mortality risk, mainly in men. Our results warrant further exploration of the clinical applicability of detectable TPO-Ab levels, potentially as a marker for low-grade inflammation. The Rotterdam Study has been entered into the Netherlands National Trial Register (NTR;
Introduction
Thyroid peroxidase (TPO) is a thyroid enzyme involved in thyroid hormone synthesis through iodination. TPO is also expressed in extrathyroidal tissues, such as the skin, breast, and heart, although it is unclear what its role in these tissues is (1). In vitro, stimulation of human mononuclear cells with TPO led to an inflammatory response with production of various proinflammatory cytokines. This response was enhanced by the addition of immunoglobulin G (IgG) antibodies directed against TPO (TPO-Abs) (2). TPO-Abs are produced during the development of autoimmune thyroid disease (1). However, TPO-Abs have been detected in disease-free individuals from the general population as well (3,4).
Previous smaller studies have described potential determinants of TPO-Ab positivity in healthy individuals, including female sex, older age, Caucasian ethnicity, obesity, and diet (5 –10). Studies concerning the effect of smoking are conflicting, but most report lower odds of TPO-Ab positivity in smokers or no association at all (7,11 –16). Alcohol consumption was less frequent in autoimmune hypothyroid women compared with euthyroid controls, suggesting a protective effect of alcohol on TPO-Ab development (17).
Inconclusive results were found for the association of various cardiovascular markers with TPO-Ab positivity (18 –21). However, these previous studies had mostly small sample sizes and did not assess multiple potential determinants within the same study population. Studies furthermore focused on TPO-Ab positivity based on assay-specific cutoff levels instead of TPO-Ab levels across the whole measurable (detectable) range.
The presence of TPO-Abs may be clinically relevant as well, regardless of thyroid disease status. In a cohort of mainly euthyroid women with diminished ovarian reserve or unexplained infertility, TPO-Ab positivity was associated with a lower antral follicle count (22). Furthermore, in pregnant women from the general population, TPO-Ab positivity was associated with an increased risk of premature delivery and a lower child intelligence quotient independent of thyroid function (23,24). TPO-Ab positivity has been reported in various nonthyroidal conditions as well, including autoimmune diseases (25).
On the contrary, higher TPO-Ab levels were associated with a decreased risk of breast cancer and more favorable tumor characteristics (26 –28). Results on the association between TPO-Ab positivity and cardiovascular disease were conflicting (29 –32). One population-based study did not find an association between TPO-Ab positivity and all-cause mortality (33).
Despite previous studies highlighting the potential importance of TPO-Abs in individuals without thyroid disease, much remains unknown. No large population-based studies so far have provided an overview of multiple potential determinants of TPO-Abs while also taking a wide range of potential confounders into account. Furthermore, previous studies were limited to TPO-Ab positivity, whereas inclusion of the entire measurable range of TPO-Ab levels may be much more informative. Studies reporting on the association between TPO-Abs and clinical outcomes were often retrospective and patient-based, rendering the significance of TPO-Abs in individuals from the general population undisclosed.
We therefore aim to explore potential determinants of TPO-Abs in a large prospective population-based cohort, subsequently linking TPO-Abs to risk of overall and cause-specific mortality. To this end, we will include multiple categories of TPO-Abs and will distinguish between detectable and positive TPO-Ab levels.
Materials and Methods
Study population
This study is embedded in the Rotterdam Study (RS), a large prospective population-based cohort study of middle-aged and elderly citizens from Ommoord, Rotterdam, the Netherlands. For this study, we included participants of three independent RS cohorts (I-3, II-1, and III-1) with TPO-Ab measurements and written informed consent for follow-up. For RS I and II, all inhabitants of the study district who were aged 55 and older were invited to participate, whereas for RS III, inhabitants of the study district aged 45 and older were invited. Details can be found in the Supplementary Data and elsewhere (34). The RS has been approved by the Medical Ethics Committee of the Erasmus MC (registration number MEC 02.1015) and by the Dutch Ministry of Health, Welfare and Sport (Population Screening Act WBO, license number 1071272-159521-PG). The RS Personal Registration Data collection is filed with the Erasmus MC Data Protection Officer under registration number EMC1712001.
Assessment of TPO-Abs and thyroid function
Blood was drawn at the research center in Ommoord between 1997 and 2008 and the moment of blood drawing was considered the study baseline. TPO-Abs were determined through an electrochemiluminescence immunoassay “ECLIA” for TPO-Abs (COBAS, Roche Diagnostics GmbH, Germany). The assay had a measuring range of 5–600 kU/L, and values above 35 kU/L were regarded positive according to the manufacturer's recommendations. The assay's lower detection limit was 5 kU/L, and TPO-Ab levels >5 kU/L were regarded detectable.
We further categorized TPO-Ab levels into undetectable (<5 kU/L), low detectable (5–15 kU/L), high detectable (15–35 kU/L), and positive (>35 kU/L). The distinction between low and high detectable was based on a previous study within the RS that reported a rise in thyrotropin (TSH) and a decrease in free thyroxine (fT4) levels at a TPO-Ab level of 15 kU/L (35). TSH and fT4 were measured with ECLIA, and had reference ranges of 0.4–4.0 mU/L and 11–25 pmol/L, respectively.
Assessment of covariates
Potential determinants and confounders were selected based on previous literature, biological plausibility, and availability in our study cohort. We included baseline measurements of body mass index (BMI), alcohol consumption, smoking status, hypertension, diabetes mellitus, serum cholesterol, and C-reactive protein (CRP). The assessment methods are included in the Supplementary Data. Baseline use of thyroid function-altering medication was determined through linkage with computerized records of pharmacies in the study district and comprised amiodarone, systemic corticosteroids, levothyroxine, propylthiouracil, carbimazole, thiamazole, and/or iodine.
Assessment of mortality
Information on all-cause mortality and cause-specific mortality was collected from medical records of general practitioners, nursing homes, and hospitals. Two independent research physicians classified the events according to the International classification of primary care and International statistical classification of diseases and related health problems 10th revision (ICD-10) coding systems. The coded events were subsequently reviewed by a medical expert in the field.
Cardiovascular mortality comprised mortality due to coronary heart disease, cerebrovascular disease, and other atherosclerotic disease in accordance with previously set clinical criteria (36). Cancer-related mortality comprised mortality due to all solid and hematological malignancies (ICD-10 codes C00-D48). The follow-up for all-cause mortality has been completed until May 24, 2018, and the follow-up for cause-specific mortality has been completed until January 1, 2015.
Statistical analyses
To assess the association of potential determinants with TPO-Ab detectability and TPO-Ab positivity, we performed binomial logistic regression analyses to obtain odds ratios (ORs) with 95% confidence intervals (CIs). To assess the association of potential determinants with TPO-Ab categories, we performed multinomial logistic regression analyses to obtain ORs with CIs. We applied two models for both logistic regression analyses. The first model was univariate (unadjusted), and the second model was adjusted for the other determinants, TSH and fT4.
Cox proportional hazards regression analyses were performed to obtain hazard ratios (HRs) with CIs for the association of continuous TPO-Ab levels, TPO-Ab detectability, and TPO-Ab positivity with all-cause, cardiovascular, and cancer-related mortality. Furthermore, we also investigated the association between TPO-Ab tertiles and mortality risk.
We applied two models to all Cox analyses. The first model included age, sex, TSH, and RS cohort. The second model additionally included smoking status, BMI, alcohol consumption, hypertension, diabetes mellitus, serum CRP, and cholesterol. We performed competing risk regression analyses to obtain 10-year absolute risks of cardiovascular and all other (noncardiovascular) mortalities for men and women. Competing risk analyses were adjusted for age, TSH, RS cohort, smoking status, BMI, alcohol consumption, hypertension, diabetes mellitus, serum CRP, and cholesterol.
For all analyses, the multivariate models were reported in the results. Detailed statistical methods including predefined stratification and sensitivity analyses are included in the Supplementary Data. All analyses were performed in R version 4.0.2 (The R Foundation for Statistical Computing, Vienna, Austria).
Results
Baseline characteristics
We included 9685 participants with a median age of 63.3 years, of whom 56.8% were women. The median TPO-Ab level was 7.6 kU/L and almost half of our study population had TPO-Abs in the low detectable range (5–15 kU/L). Median levels of TSH and fT4 were 1.9 mU/L and 15.6 pmol/L, respectively. An overview of baseline characteristics is shown in Table 1. Sex-stratified baseline characteristics are shown in Supplementary Table S1. Subtle but significant differences were seen between men and women for most covariates. Most notably, TPO-Ab positivity and use of thyroid function-altering medication were more prevalent in women (Supplementary Table S1).
Baseline Characteristics of 9685 Participants with Thyroid Peroxidase Antibodies and Given Informed Consent
Ten gram alcohol/day is equivalent to one alcoholic beverage according to the WHO guidelines.
Encompasses amiodarone, systemic corticosteroids, levothyroxine, propylthiouracil, carbimazole, thiamazole, and/or iodine.
BMI, body mass index; CRP, C-reactive protein; fT4, free thyroxine; IQR, interquartile range; SD, standard deviation; TPO-Abs, thyroid peroxidase antibodies; TSH, thyrotropin; WHO, the World Health Organization.
Determinants of TPO-Ab positivity
Female compared with male sex was associated with higher odds of TPO-Ab positivity (i.e., TPO-Ab levels >35 kU/L) (OR = 2.47 [CI 2.13–2.86]). No associations were seen of age, BMI, alcohol consumption, and smoking status with TPO-Ab positivity (Table 2). When stratified by sex, no associations were seen for age, BMI, and alcohol consumption in either sex. However, female current smokers had higher odds of TPO-Ab positivity than female never-smokers (OR = 1.24 [CI 1.01–1.52]) (Supplementary Table S2). Excluding users of thyroid function-altering medication did not affect effect estimates (Supplementary Table S3).
Association Between Determinants and Thyroid Peroxidase Antibody Positivity and Detectability
TPO-Ab positivity comprises values >35 kU/L, TPO-Ab detectability comprises values >5 kU/L.
Multivariate model is adjusted for age, sex, BMI, alcohol consumption, smoking status, Ln(TSH), and fT4.
CI, 95% confidence interval; Ln(TSH), natural logarithm of thyrotropin; OR, odds ratio.
Determinants of TPO-Ab detectability
Higher age was associated with lower odds of TPO-Ab detectability (i.e., TPO-Ab levels >5 kU/L) (OR per 1-year increase = 0.98 [CI 0.97–0.98]). All categories of alcohol consumption compared with nondrinking were associated with decreased odds of TPO-Ab detectability as well (OR for heavy drinking = 0.71 [CI 0.59–0.85]). On the contrary, higher odds of TPO-Ab detectability were reported in women compared with men (OR = 1.35 [CI 1.22–1.49]) and current compared with never-smokers (OR = 3.10 [CI 2.66–3.62]) (Table 2). We reported a small positive association between BMI and TPO-Ab detectability (OR per one kg/m2 increase = 1.02 [CI 1.01–1.03]) (Table 2).
Stratification by sex revealed a stronger and significant negative association of moderate (OR = 0.76 [CI 0.59–0.97]) and heavy alcohol consumption (OR = 0.62 [CI 0.47–0.81]) with TPO-Ab detectability in women. No other notable sex differences were seen (Supplementary Table S2). Excluding users of thyroid function-altering medication did not affect effect estimates (Supplementary Table S3).
Determinants of TPO-Ab categories
Higher age was associated with lower odds of TPO-Ab levels in the positive range and with particularly lower odds of TPO-Ab levels in the detectable range (Table 3; Fig. 1). Female sex was associated with higher odds of high detectable (OR = 1.51 [CI 1.28–1.79]) and positive (OR = 2.71 [CI 2.31–3.18]) TPO-Abs (Table 3; Fig. 1). BMI was weakly associated with detectable TPO-Ab levels (ORs 1.02 and 1.03 for low, respectively, high detectable TPO-Abs).
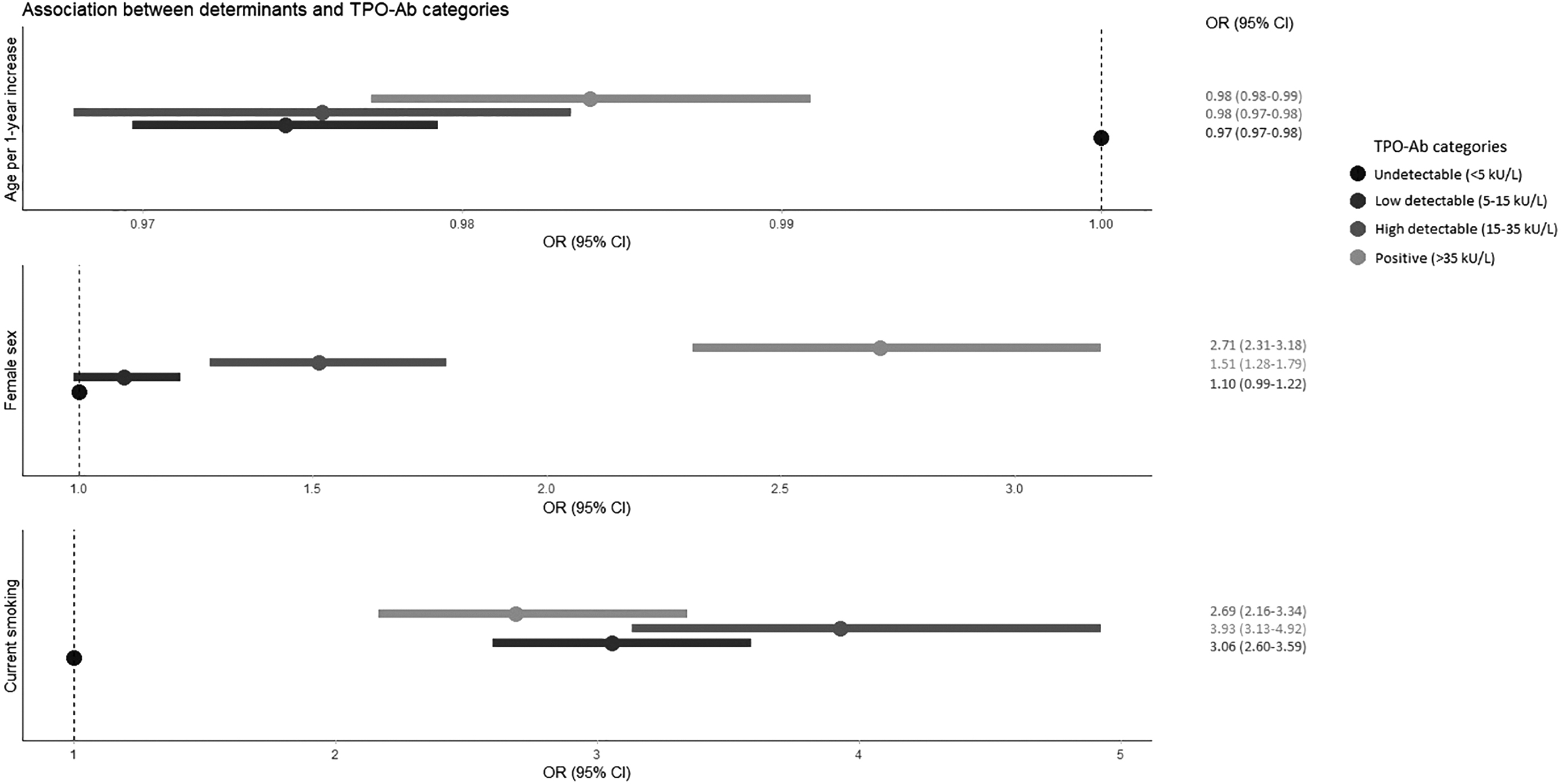
Forest plot for identified clinically relevant determinants of TPO-Ab categories. Displayed are ORs (dots) and corresponding CIs (lines) for the association between determinants and TPO-Ab categories. The dot with the dashed line depicts the reference category of undetectable TPO-Abs. ORs are adjusted for age, sex, BMI, alcohol consumption, smoking status, Ln(TSH), and fT4. BMI, body mass index; CI, 95% confidence intervals; fT4, free thyroxine; Ln(TSH), natural logarithm of thyrotropin; OR, odds ratio; TPO-Abs, thyroid peroxidase antibodies.
Association Between Determinants and Thyroid Peroxidase Antibody Categories
Multivariate model is adjusted for age, sex, BMI, alcohol consumption, smoking status, Ln(TSH), and fT4.
Mild and heavy alcohol consumption was associated with lower odds of both detectable and positive TPO-Ab levels (ORs ranging from 0.70 to 0.81) (Table 3). No association was seen between former smoking and TPO-Ab categories, but current smoking was associated with three- to fourfold higher odds of detectable TPO-Abs and 2.7-fold higher odds of TPO-Abs in the positive range (Table 3; Fig. 1).
In the sex-stratified analyses, mild and heavy alcohol consumption were associated with lower odds of TPO-Ab positivity in women only. No other differences between men and women were noted (Supplementary Table S4). Exclusion of thyroid function-altering medication users yielded similar results as in the main analyses (Supplementary Table S5).
Association between TPO-Abs and mortality
TPO-Ab detectability was associated with an increased risk of all-cause, cardiovascular, and cancer-related mortality (HRs ranging from 1.09 to 1.21), independent of thyroid function. No associations were seen between TPO-Ab positivity and mortality risk (Table 4).
Association Between Thyroid Peroxidase Antibodies and Mortality
Model 1 is adjusted for age, sex, RS cohort, and (Ln)TSH. Model 2 is adjusted for model 1, smoking status, BMI, alcohol consumption, DM, serum CRP, serum cholesterol, and hypertension.
Natural logarithm of TPO-Ab level.
DM, type 2 diabetes mellitus; HR, hazard ratio; RS, Rotterdam Study.
When stratified by sex, higher TPO-Ab levels in men were associated with all-cause mortality (HR per unit increase in log-transformed TPO-Ab level = 1.07 [CI 1.02–1.13]) and cardiovascular mortality (HR per unit increase in log-transformed TPO-Ab level = 1.15 [CI 1.01–1.32]) (Table 5). When taking competing risks into account, the 10-year absolute risk of cardiovascular mortality was higher in men compared with women, and this risk increased with higher TPO-Ab levels in men, while remaining constant in women (risk difference at a TPO-Ab level of 403 kU/L ∼3.1%) (Fig. 2A).
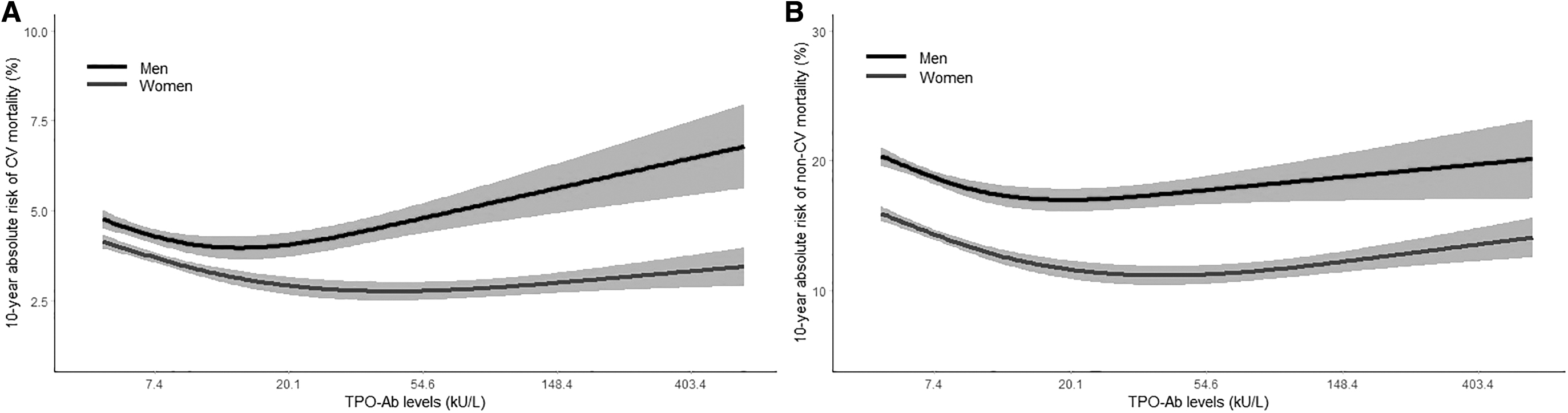
Absolute risk plots for the association between TPO-Ab levels and mortality stratified by sex. (
Association Between Thyroid Peroxidase Antibodies and Mortality Stratified by Sex
Adjusted for age, RS cohort, (Ln)TSH, smoking status, BMI, alcohol consumption, DM, serum CRP, serum cholesterol, and hypertension.
Natural logarithm of TPO-Ab level.
For noncardiovascular mortality, the 10-year absolute risk did not change across TPO-Ab levels, but was consistently higher in men than women (Fig. 2B). Furthermore, TPO-Ab detectability was associated with a higher risk of all-cause and cardiovascular mortality in men as well (HR = 1.19, respectively 1.50). No associations were seen between TPO-Ab positivity and risk of any mortality in either sex (Table 5).
Exclusion of thyroid function-altering medication users did not change effect estimates (Supplementary Table S6). When analyzing TPO-Abs in tertiles, the middle and highest tertiles were associated with an increased risk of all-cause, cardiovascular, and cancer-related mortality. Mortality risk was highest and reaching significance for the middle tertile (TPO-Ab level 5.4–10.8 kU/L) compared with the lowest tertile (TPO-Ab level <5.4 kU/L) (Supplementary Table S7).
When stratified by sex, both the middle and particularly the highest TPO-Ab tertiles were associated with an increased risk of all-cause mortality (HR for highest tertile = 1.21 [CI 1.06–1.37]) and cardiovascular mortality (HR for highest tertile = 1.58 [CI 1.16–2.17]) in men. No significant associations were seen in women (Supplementary Table S8).
Discussion
We assessed the association between potential determinants and TPO-Abs and subsequently associated TPO-Abs with risk of overall and cause-specific mortality in a large prospective, population-based cohort of middle-aged and elderly individuals. Age, sex, smoking status, and alcohol consumption were identified as determinants of TPO-Abs in the detectable and/or positive range.
Higher age was associated with lower odds of TPO-Abs in the detectable and positive range, which was not in line with the results of previous studies. However, previous studies had included relatively young participants and only reported descriptive statistics in 5- or 10-year age categories rather than performing regression analyses with age as a continuous variable, and some only reported age differences when stratified by sex (5,6,37). A Greek cross-sectional study found fluctuating percentages of TPO-Ab positivity across 10-year age categories ranging from 12 to >80 years. This study had a relatively small sample size and did not formally assess the association between age and TPO-Abs either (38). Although the age distribution of autoimmune diseases varies greatly, most occur in young adult or middle-aged individuals rather than at older age (39). Diminished autoimmunity throughout aging may be explained by a reduced immune response. TPO-Abs are predominantly produced by thyroid infiltrating lymphocytes and the TPO-Ab titer reflects the extent of lymphocytic infiltration of the thyroid gland (40). Several studies reported an age-related decline in various subsets of T and B lymphocytes (41 –44), which could result in reduced lymphocytic infiltration of the thyroid gland and subsequently a lower TPO-Ab production at older age.
Female sex was associated with higher odds of TPO-Ab detectability and particularly of TPO-Ab positivity. This confirms the results of previous studies reporting higher percentages of TPO-Ab positivity in women compared with men (3 –5,38). However, we reported notable sex differences in the detectable TPO-Ab range as well. Other nonthyroidal autoantibodies are also more common in women than in men (45 –47). Possible explanations include a stimulating effect of estrogens on autoantibody production, sex-specific differences in microbiota influencing immunophenotype, or increased immune reactivity in women (47 –49). More research is needed to explore these hypotheses.
Alcohol consumption was associated with lower odds of detectable and positive TPO-Abs, most notably in female heavy drinkers (>20 g alcohol per day). In previous population-based studies, alcohol consumption was associated with lower odds of overt autoimmune hypothyroidism (17,50). Previous studies further established a dose-dependent association of higher alcohol consumption with lower odds of rheumatoid arthritis and systemic lupus erythematosus (51,52), suggesting immunomodulating properties of alcohol. In vitro and in vivo experiments showed that alcohol consumption either stimulates or inhibits the function of immune cells, including T and B lymphocytes, depending on the dose (moderate or heavy) and duration (acute or chronic) (53).
Current smoking more than tripled the odds of TPO-Ab detectability and to a lesser extent was associated with TPO-Ab levels in the positive range as well. Most previous studies reported no association or a negative association between smoking and TPO-Abs (7,11,12,14 –16). However, these studies only included TPO-Ab positivity as defined by the assay's manufacturer in their analyses, instead of TPO-Ab levels across the entire measurable range. Compared with our study population, the previous studies had furthermore included relatively young participants (mean age 30–50 years), and most studies had included mainly or exclusively women in their study population. We propose that smoking may cause a subtle shift in TPO-Ab levels, mainly leading to detectable TPO-Abs, due to inflammation. Smoking is known to activate the nuclear factor kappa-light-chain-enhancer of activated B cells (NF-κB) pathway, a pathway that among various other biological functions regulates the expression of TPO (54,55).
We established that detectable TPO-Abs were associated with an increased risk of all-cause, cardiovascular, and cancer-related mortality, independent of thyroid function. No association was seen between TPO-Ab positivity and mortality risk, which corresponds with the results of a previous Dutch population-based study (33). Detectable TPO-Abs could reflect chronic low-grade inflammation. TPO-Abs are mostly IgG antibodies and it is known that IgG glycosylation patterns change at older age increasing its proinflammatory potential (56,57). Chronic low-grade inflammation is associated with an increased risk of all-cause and cardiovascular mortality (58,59).
The absence of an association between TPO-Ab positivity and mortality risk could be explained by more extensive medical surveillance and treatment of individuals with overt thyroid disease (i.e., Hashimoto's disease) resulting in improved prognosis. However, results after exclusion of thyroid function-altering medication users were comparable, rendering this explanation less likely. Alternatively, the relatively low number of events within the TPO-Ab-positive group could pose a power problem to detect significant associations.
When including TPO-Ab tertiles, increasing statistical power in the higher TPO-Ab groups, we indeed found stronger and significant effect estimates for the highest TPO-Ab tertile (TPO-Ab level ≥10.8 kU/L) than in the TPO-Ab positivity analyses in men. However, this highest TPO-Ab tertile also included participants with detectable TPO-Ab levels. Future studies with more mortality events in participants with positive TPO-Ab levels are needed to confirm whether the differences in mortality risk between TPO-Ab detectability and positivity are due to power issues or other underlying factors.
When stratified by sex, we only reported significant associations of TPO-Abs and TPO-Ab detectability with all-cause and cardiovascular mortality in men. We also reported a stronger association between TPO-Abs and absolute 10-year risk of cardiovascular mortality in men compared with women. Similar sex differences have previously been reported for the association between thyroid hormones and mortality risk as well (60 –62). It is unclear whether these sex differences could imply different clinical consequences of TPO-Abs in men compared with women. As shown before, women have higher odds of detectable and positive TPO-Abs, which suggests that in women the threshold for clinically significant TPO-Ab levels may be higher than in men. It is also possible that men have certain unmeasured or unknown risk factors that explain the higher mortality risk. Although we adjusted for a wide range of well-documented/-phenotyped confounders, residual confounding cannot be ruled out in observational studies. Further research is warranted to investigate the sex differences in associations between thyroid parameters and mortality.
Our biggest strength is that we are the first to identify potential determinants of TPO-Ab levels across the entire measurable (both detectable and positive) range in a large population-based cohort of middle-aged and elderly individuals. We furthermore assessed the association between TPO-Abs and risk of all-cause and cause-specific mortality to explore the clinical implications of TPO-Abs in healthy individuals. We had access to a wide range of potential confounders and long-term follow-up with extensive ascertainment of covariates and mortality events. We furthermore repeated all our analyses after exclusion of users of thyroid function-altering medication and retrieved similar results. This addition to the fact that we adjusted for TSH and fT4 levels implies that the identified determinants of TPO-Abs and the reported associations with mortality risk are independent of thyroid function.
An important limitation of our study is that TPO-Ab measurements were only available at one time point (at baseline), preventing assessment of the association with potential determinants over time and identification of determinants that may have a bidirectional association with TPO-Abs (e.g., cardiovascular serum markers and diabetes mellitus). Future studies with repeated measurements of TPO-Abs and potential determinants should address this. Finally, our study population consists of mainly Caucasian individuals, which may limit extrapolation of our findings to other ethnicities.
Conclusion
In middle-aged and elderly individuals from the general population, female sex and smoking are associated with TPO-Abs in the detectable and positive range. Higher age and alcohol consumption are associated with lower odds of detectable or positive TPO-Abs. TPO-Ab detectability, rather than TPO-Ab positivity, is also associated with an increased risk of all-cause, cardiovascular, and cancer-related mortality, especially in men. Our results highlight the clinical importance of detectable TPO-Abs as a potential biomarker for low-grade inflammation.
Footnotes
Authors' Contributions
Conceptualization: S.R.K., R.P.P., P.M.v.H., V.D., and L.C. Methodology: S.R.K. and L.C. Formal analysis and investigation: S.R.K. Writing—original draft preparation: S.R.K. Writing—review and editing: S.R.K, R.P.P., P.M.v.H., V.D., and L.C. Supervision: R.P.P., P.M.v.H., V.D., and L.C. Funding acquisition: V.D.
Author Disclosure Statement
All authors have no competing interests or personal financial interests to disclose.
Funding Information
V.D. received an unrestricted investigator-initiated research grant from Takeda Pharmaceutical Company Limited (IIR-NLD-002671).
Supplementary Material
Supplementary Data
Supplementary Table S1
Supplementary Table S2
Supplementary Table S3
Supplementary Table S4
Supplementary Table S5
Supplementary Table S6
Supplementary Table S7
Supplementary Table S8