
Abstract
Background:
Thyroid dysfunction is prevalent in reproductive-age women and has been identified as a risk factor for female infertility. However, it remains largely unclear whether subtle thyroid dysfunction, as estimated by moderately high thyrotropin (TSH) levels within the normal range, is associated with ovarian reserve in infertile women before assisted reproductive technology (ART) treatment.
Methods:
This cross-sectional study involved 3501 euthyroid infertile women, including 2189 women with TSH levels ≤2.5 μIU/mL and 1312 women with high-normal TSH levels (2.51–4.20 μIU/mL). Ovarian reserve markers were compared between women with low- and high-normal TSH levels. Correlation analysis and regression models were used to estimate the association of TSH levels with ovarian reserve. In addition, the association of subtle thyroid dysfunction with ovarian reserve was further evaluated after stratification for different infertility diagnoses and statuses of thyroid autoimmunity (TAI).
Results:
In the total population, women with high-normal TSH levels had significantly decreased anti-Müllerian hormone (AMH) concentrations (p < 0.001), a lower bilateral antral follicle count (AFC) (p < 0.001), and a higher prevalence of diminished ovarian reserve (DOR) (p = 0.018) than women with low-normal TSH levels. The TSH levels showed a negative association with both AMH levels (r = −0.050, p = 0.003) and bilateral AFC (r = −0.071, p < 0.001). Furthermore, the association of high-normal TSH levels with decreased AMH and AFC was more prominent in infertile women with ovulation dysfunction (p = 0.002, p = 0.002), unexplained infertility (p = 0.020, p = 0.028), or negative TAI (both p < 0.001).
Conclusions:
These data suggested that subtle thyroid dysfunction was associated with DOR in infertile women before ART treatment, which will add evidence that strengthens the systematic screening of TSH levels/TAI in infertile women and will contribute to the discussion of specific TSH cutoff values in predicting ovarian reserve.
Introduction
Thyroid dysfunction and thyroid autoimmunity (TAI) are prevalent in reproductive-age women and have independently been associated with multiple adverse reproductive outcomes, either in spontaneous conception or assisted reproductive technology (ART) treatment (1 –3). In particular, a higher prevalence of thyroid insufficiency has been reported in infertile women, especially those with idiopathic infertility (4). Consequently, both the recent European Thyroid Association (ETA) and American Thyroid Association (ATA) guidelines recommend screening for thyroid dysfunction and autoimmunity as a routine part of the initial workup for infertile women attempting pregnancy (3,5).
Ovarian reserve mainly encompasses the quantity and quality of oocytes. It is vital for reproductive function and determines a woman's reproductive potential and, subsequently, her reproductive life span and age at menopause onset. As an important contributor to female infertility, the factors accounting for the high risk of diminished ovarian reserve (DOR) have not been fully elucidated. The detrimental impact of severe thyroid dysfunction on ovarian function has been widely reported (6).
Expression of thyroid hormone receptors and thyrotropin (TSH) receptors has been reported on granulosa cells and oocytes in the ovary, which functions through direct impact or synergistic action with follicle-stimulating hormone (FSH) on follicular growth and development (7). In addition, thyroid dysfunction may disrupt the gonadotropin-releasing hormone (GnRH) function, which then results in dysregulation of the hypothalamic–pituitary–gonadal axis (6,8,9).
Thyroid insufficiency represents a continuum of impaired thyroid function, rather than a dichotomous state. Even mild thyroid insufficiency with moderately elevated TSH levels has been considered as one of the plausible causes of reduced fertility and poor pregnancy outcomes due to the importance of thyroid hormones (2,3,6,10). Nonetheless, the association reported was not consistent, which can partly be explained by different cutoffs used to define the upper limit of normal TSH concentration.
Subclinical hypothyroidism was variably defined in the literature as TSH levels >2.5 μIU/mL, >4.5 μIU/mL, or above the upper limit of the assay-specific reference range (3,11). Indeed, optimizing preconception upper reference TSH values for euthyroidism in a distinct population of subfertile or infertile women is under debate. In women undergoing ART treatment, the prevalence of moderately elevated TSH levels (2.5–4.5 μIU/mL) was 20–26%, much higher than the prevalence of 5% in the general population (12,13). Some advocated that TSH values >2.5 μIU/mL in subfertile women could indicate insufficient capacity for reproductive functions such as oocyte quality, ovulation, fertilization, and implantation (14,15).
However, studies that assessed the impact of moderately elevated TSH levels or the potential dose-dependent effects of TSH levels within the normal reference range on ovarian reserve are sparse. In particular, even the limited evidence yielded conflicting results (12,16,17). Michalakis et al. (12) found a significant increase in the frequency of DOR with increasing TSH levels, whereas Rao et al. (17) concluded no significant differences in anti-Müllerian hormone (AMH) levels and antral follicle counts (AFCs) between patients with TSH levels <2.5 mIU/mL and high-normal TSH levels.
Heterogeneity existed among the different studies, including small sample numbers, poor study design, the selection of causes of infertility, and different assays using varying reference cutoff levels for TSH, which might explain the contradictions. Collectively, as a milder precursor stage within a spectrum of impaired thyroid function, whether occult/incipient thyroid insufficiency predisposes patients toward DOR remains unclear.
In this retrospective cross-sectional study, we aimed to understand whether subtle thyroid dysfunction, as estimated by moderately high TSH levels within the normal range, is associated with DOR in infertile women before undergoing ART treatment. Different indicators of ovarian reserve were compared between euthyroid women with low-normal and high-normal TSH levels, and the association of high-normal TSH levels with indicators of ovarian reserve and prevalence of DOR, either stratified by different causes of infertility or TAI status, was further evaluated.
Our results will add additional informative evidence for routine screening for thyroid disease in the workup of infertile women.
Material and Methods
Ethical approval
The study was approved by the Institutional Review Board of the Center for Reproductive Medicine, Shandong University. A written informed consent form was obtained from each participant.
Participants
Patients who were referred to the fertility clinic of the Hospital for Reproductive Medicine Affiliated to Shandong University between January 2015 and June 2020 were retrospectively screened. All electronic records were individually reviewed to ensure that all participants met our inclusion and exclusion criteria. Infertile women aged 20–40 years with normal thyroid function before treatment were included. Infertility was defined as failure to achieve a clinical pregnancy after 12 months or more of regular unprotected sexual intercourse.
The exclusion criteria included (i) a history of thyroid disease, thyroid hormone/antithyroid medication, or thyroid surgery; (ii) a history of chemotherapy, radiotherapy, or ovarian surgery; (iii) X chromosome abnormalities; and (iv) a lack of results of ovarian reserve or thyroid function/autoimmunity.
According to the TSH cutoff value of 2.5 μIU/mL, the participants were divided into two groups: a low-normal group with a TSH cutoff of 0.27–2.50 μIU/mL and a high-normal group with a TSH cutoff of 2.51–4.20 μIU/mL (Fig. 1).
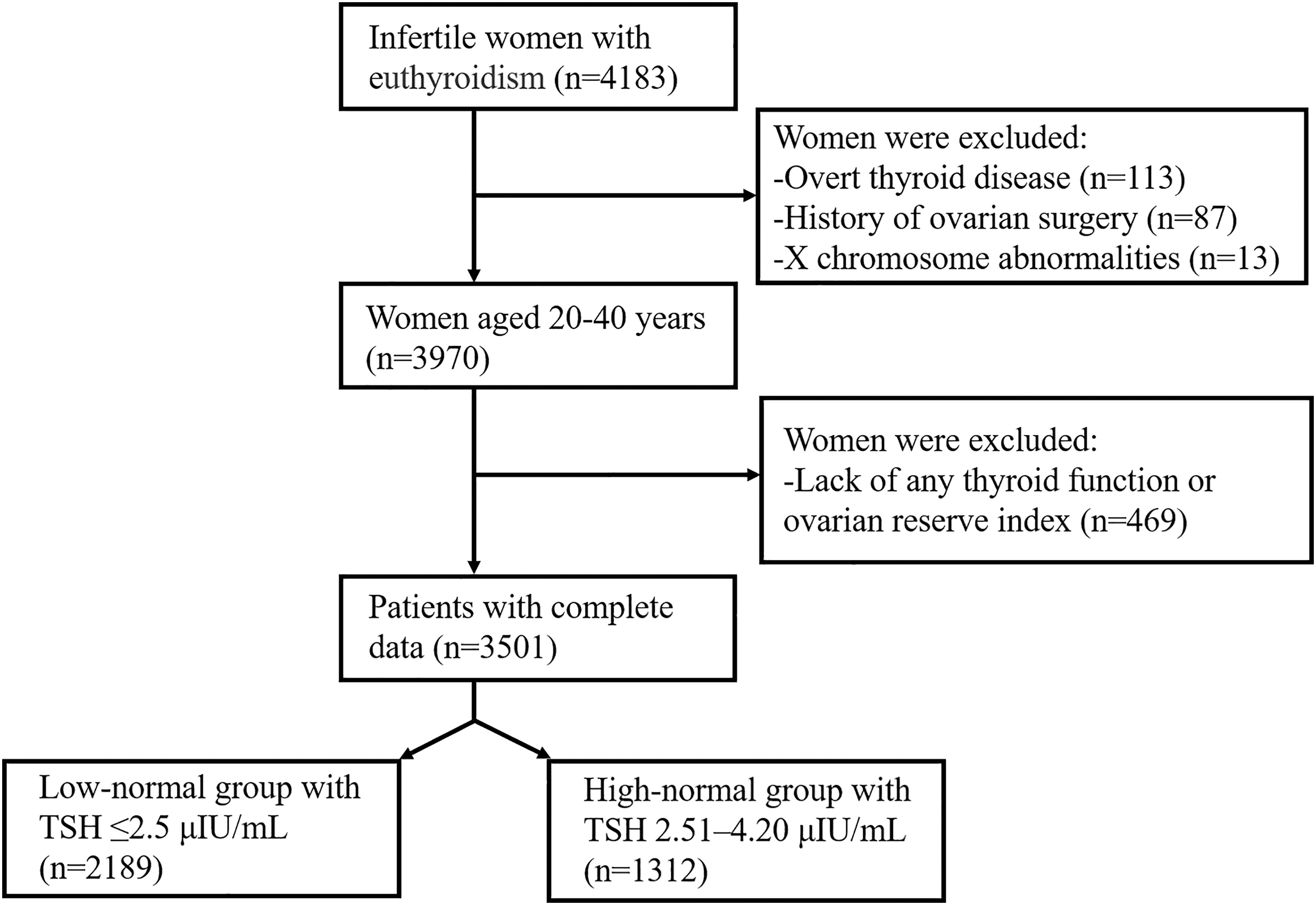
Flow chart of study population selection. TSH, thyrotropin.
Biochemical measures and ultrasonography
All diagnostic testing was performed as part of routine clinical care. Endocrine hormones, including FSH, luteinizing hormone (LH), estradiol, prolactin, and testosterone, were measured on days 2–4 of the menstrual cycle by chemiluminescence immunoassays. AMH levels were assayed using an ultrasensitive enzyme-linked immunosorbent assay.
The serum baseline TSH, free triiodothyronine (fT3), free thyroxine (fT4), thyroid peroxidase antibody (TPOAb), and thyroglobulin antibody (TGAb) levels were detected by automatic chemiluminescence immunoassays. The intra- and interassay coefficients of variation were <10% and <15%, respectively. Reference ranges were recommended as follows: 0.27–4.20 μIU/mL for TSH levels, 3.1–6.8 pmol/L for fT3 levels, and 12–22 pmol/L for fT4 levels. TPOAb and TGAb levels were defined as positive if the titer was >34 or >115 IU/mL, respectively. Positive TAI was considered as the presence of TPOAb and/or TGAb positivity.
DOR was defined as basal FSH levels ≥12 IU/L, along with AMH levels <1.2 ng/mL or an AFC <5, consistent with our previous study (18). The AFC was recorded as the number of antral follicles (2–10 mm in diameter) in the early follicular phase through transvaginal ultrasound.
IVF procedure and pregnancy outcomes
A standardized ovarian stimulation protocol was used, as reported in our previous study, including a natural protocol, a GnRH agonist short/long protocol, a GnRH antagonist protocol, and an ultralong protocol (18). When ≥2 antral follicles had reached a mean diameter ≥18 mm, human chorionic gonadotropin (hCG) was injected, followed by oocyte retrieval guided by transvaginal ultrasonography 34–36 hours later. Based on the sperm quality, oocytes were fertilized through intracytoplasmic sperm injection or conventional insemination. Luteal-phase support was initiated on the day of oocyte retrieval until 12 weeks after conception.
Biochemical pregnancy was confirmed with the serum hCG level >25 IU/L at 14 days after embryo transfer. Clinical pregnancy was confirmed with the observation of a gestational sac on ultrasonography. Live birth was defined as the delivery of at least one live-born infant after 28 weeks of gestation. Pregnancy loss was defined as a fetal loss in spontaneous abortion or therapeutic abortion that occurred at any point during gestation.
Statistical analyses
Data analyses were conducted using the Statistical Package for the Social Sciences (SPSS) and GraphPad Prism 9. The Kolmogorov–Smirnov test and quantile–quantile plot were combined to test for normality. Continuous variables with a normal distribution are presented as the mean ± standard deviation and compared using Student's t-test. Non-normally distributed continuous variables were compared with the Mann–Whitney U-test and presented as the median (interquartile range).
Categorical variables were analyzed by chi-square or Fisher's exact test, as appropriate, and are presented as the number of observations (percentage). The comparison of the DOR prevalence and infertility diagnosis was analyzed by the χ2 test with Bonferroni correction for categorical variables expressed as proportions.
The association of high-normal TSH levels with indicators of ovarian reserve and the prevalence of DOR were analyzed using multivariable linear regression models or binary logistic regression models, and the correlation of TSH levels with ovarian reserve was analyzed using correlation analysis after adjusting for the woman's age, body–mass index (BMI), infertility diagnosis, and TAI positivity.
A value of p < 0.05 on a two-tailed test was considered statistically significant.
Results
Baseline characteristics
A total of 3501 euthyroid women with infertility were recruited and they had a mean age of 32.63 ± 3.83 years and a mean TSH level of 2.26 ± 0.88 μIU/mL. Among these patients, 62.52% had a TSH level ≤2.5 μIU/mL and 37.48% were included in the high-normal subgroup with the TSH cutoff of 2.51–4.20 μIU/mL. No significant difference was observed in terms of age, BMI, or type of infertility between the two groups (all p > 0.05).
Based on the infertility diagnosis, tubal factor, uterine factor, ovulation dysfunction, male factor, and unexplained infertility accounted for 20.74%, 11.25%, 40.16%, 16.91%, and 10.94%, respectively. Interestingly, the causes of infertility diagnoses were significantly different between the two groups (p < 0.001). Compared with women with high-normal TSH levels, there were more women who were infertile due to ovulation dysfunction and fewer women with unexplained infertility in the low-normal TSH group (p = 0.011, p < 0.001).
As expected, patients with TSH levels >2.5 μIU/mL had slightly decreased levels of fT3 and fT4 compared with those with TSH levels ≤2.5 μIU/mL (p = 0.029, p = 0.002). In addition, the percentage of either TAI positivity or single TPOAb/TGAb positivity was significantly increased within the high-normal subgroup (p < 0.001, p = 0.019, p < 0.001) (Table 1).
Baseline Characteristics of the Participants
Data are presented as mean ± standard deviation or n (%).
BMI, body–mass index; fT3, free triiodothyronine; fT4, free thyroxine; TAI, thyroid autoimmunity; TGAb, thyroglobulin antibody; TPOAb, thyroid peroxidase antibody; TSH, thyrotropin.
Ovarian reserve indicators and reproductive outcomes in euthyroid women with low-normal and high-normal TSH levels
To evaluate the impact of slightly high TSH levels on ovarian reserve, different indicators of ovarian reserve and function were first compared between women with low-normal and high-normal TSH levels. The median AMH concentration and bilateral AFC were significantly lower in women with high-normal TSH levels than in those with low-normal TSH levels (2.63 [1.40, 4.96] ng/mL vs. 2.99 [1.58, 5.51] ng/mL, p < 0.001; 11 [7, 16] vs. 12 [7, 17], p < 0.001), whereas no difference of FSH, LH, E2, or T was found between the two groups (all p > 0.05).
Furthermore, the prevalence of DOR was also significantly increased in women with high-normal TSH levels (5.11% vs. 3.47%, p = 0.018) (Table 2).
Ovarian Reserve Indicators Between Euthyroid Women with Low-Normal and High-Normal Thyrotropin Levels
Data are presented as mean ± standard deviation or median (interquartile range).
AFC, antral follicle count; AMH, anti-Müllerian hormone; DOR, diminished ovarian reserve; E2, estradiol; FSH, follicle-stimulating hormone; LH, luteinizing hormone; T, testosterone.
Given that ovarian reserve is an important determinant of successful pregnancy, the reproductive outcomes were further analyzed. A total of 4632 transplantation cycles were available.
Intriguingly, women with high-normal TSH levels had a lower live birth rate (54.26% vs. 57.41%, p = 0.038) and a higher frequency of biochemical pregnancy loss (9.71% vs. 7.63%, p = 0.037) compared with women with low-normal TSH levels, while there were no significant between-group differences in the rates of clinical pregnancy (64.32% vs. 66.83%, p = 0.083) and clinical pregnancy loss (8.83% vs. 8.60%, p = 0.825) (Supplementary Table S1).
The association of moderately high TSH levels with ovarian reserve
Given the significant differences in AMH levels, bilateral AFCs, and the prevalence of DOR between women with high-normal and low-normal TSH levels, the impact of slightly high TSH levels on ovarian reserve was further determined using multivariable linear regression models after adjusting for confounding factors in terms of age, BMI, infertility diagnosis, and TAI positivity.
Consistently, we found that patients with high-normal TSH levels had significantly decreased levels of AMH (mean difference = −0.39, p = 0.003) and bilateral AFC (mean difference = −1.26, p < 0.001) and a higher prevalence of DOR (mean difference = 1.60, p = 0.008) than those within the low-normal group.
Correlation of TSH levels with ovarian reserve
Based on the impact of slightly high TSH levels on ovarian reserve, we further analyzed the correlation of TSH levels as continuous variables with different ovarian reserve indicators. Interestingly, in the total study population, the concentration of TSH showed a significant negative association with both AMH level (r = −0.050, p = 0.003) and bilateral AFC (r = −0.071, p < 0.001) (Fig. 2).
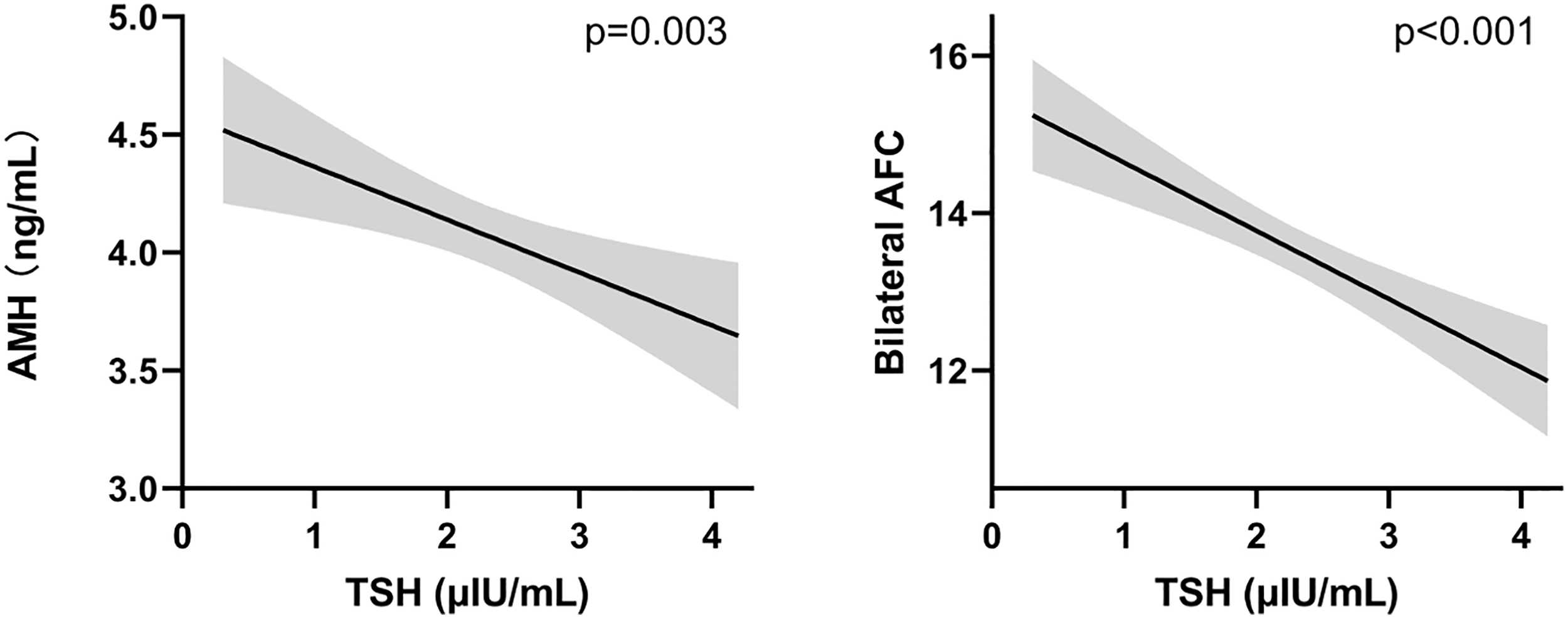
The correlation of TSH concentrations with levels of AMH and bilateral AFCs. Black line: the predicted mean value of AMH and bilateral AFC; gray area: the corresponding 95% confidence interval. AFC, antral follicle count; AMH, anti-Müllerian hormone.
Association of moderately high TSH level with ovarian reserve, stratified by infertility diagnosis
To investigate whether different causes of infertility affected the association between moderately high TSH levels and ovarian reserve, we performed a subgroup analysis after stratifying the patients by infertility diagnosis. Consistent with the data in the total population, no association was found with either FSH or E2 level in each subgroup (all p > 0.05).
Interestingly, in patients with ovulation dysfunction and unexplained infertility, a high-normal TSH level was significantly associated with lower AMH concentration (p = 0.002, p = 0.020) and decreased bilateral AFC (p = 0.002, p = 0.028). In the subgroups with tubal, uterine, and male factors, no significant association was observed (all p > 0.05) (Table 3).
The Association Between Slightly High Thyrotropin Levels and Ovarian Reserve in Euthyroid Women Stratified by Infertility Diagnosis
Data are presented as median (interquartile range).
The impact of moderately high TSH levels on ovarian reserve, stratified by TAI status
Considering that TAI per se could affect the ovarian reserve, all euthyroid subjects were further stratified based on the status of TAI positivity. Women with positive TAI, either within the low-normal or high-normal TSH group, showed decreased bilateral AFCs and a lower trend of AMH levels than those with negative TAI (p < 0.001, p = 0.114, p < 0.001, p = 0.601).
Of note, in women with negative TAI, both AMH levels and bilateral AFC values were significantly lower in the high-normal subgroup than in the low-normal subgroup (all p < 0.001). Surprisingly, there was no significant difference observed between the two subgroups when women were positive for TGAb and/or TPOAb (p = 0.307, p = 0.897) (Table 4).
The Impact of Slightly High Thyrotropin Levels on Ovarian Reserve in Euthyroid Women Stratified by Thyroid Autoimmunity Status
Data are presented as median (interquartile range).
Discussion
In this large, retrospective cohort study, we found that moderately high preconception TSH (>2.5 μIU/mL) within the normal range had a detrimental impact on ovarian reserve in infertile women attempting pregnancy, characterized by a significant decline in AMH level, decreased AFC, and increased prevalence of DOR. Furthermore, the association of subtle thyroid insufficiency with ovarian reserve was more prominent in infertile women with ovulation dysfunction and unexplained infertility.
In addition to the adverse effect of TAI on ovarian reserve, the subtle thyroid dysfunction was also associated with an increased risk of DOR in women negative for TAI. These results may contribute to further discussion of the impact of occult/incipient thyroid insufficiency on ovarian reserve in infertile euthyroid women before ART treatment and add evidence that strengthens the systematic screening of TSH levels/TAI in infertile women.
The recent guidelines recommend that all women seeking medical advice for subfertility should be screened for TSH and TPOAb/TGAb at the initial workup (3,5). Although it is well established that there are separate TSH goals for pregnant and nonpregnant women, whether the preconception upper reference TSH value to define euthyroidism in infertile women attempting conception by IVF should be 2.5 or 4.5 μIU/mL is under debate (19,20).
TSH cutoffs should not merely reflect a biochemical diagnosis, but ought to be linked with reduced fertility or adverse pregnancy outcomes. In fact, the prevalence of moderately elevated TSH levels (2.5–4.5 μIU/mL) was much higher in women pursuing ART treatment than in the general population (12). Nonetheless, evidence to advocate for a cutoff of 2.5 μIU/mL has been graded poor to fair, but it is argued that the potential benefits outweigh the potential risks (21).
Some data supported the idea that patients with high-normal TSH levels had an altered ovarian response or fewer mature oocytes (22). In addition, limited research has been conducted to explore whether treatment with LT4 has a beneficial effect on ovarian reserve, which found increasing AMH levels in women with TSH levels >2.5 μIU/mL and TAI after LT4 supplementation (23).
In the recent ETA guideline on thyroid disorders before and during assisted reproduction, Poppe et al. (3) also suggested that LT4 supplementation could be considered on a case-by-case basis in subfertile women with TSH >2.5 μIU/mL and TAI to achieve the optimal ovarian reserve. Therefore, it remains to be elucidated whether, within the normal range, TSH values can be distinguished between high-normal and low-normal TSH values and the status of ovarian reserve.
Both thyroid insufficiency and premature ovarian senescence represent a continuum of impaired function rather than a dichotomous state. The association of overt thyroid dysfunction with a decline in ovarian reserve, especially the most severe premature ovarian insufficiency (POI), has been widely suggested (24). However, the extent to which hypothyroidism is related to DOR, especially for infertile women attempting pregnancy through ART treatment, has yet to be established.
Previous studies on the impact of moderately elevated TSH levels or the potential dose-dependent effects of TSH within the normal reference range on ovarian reserve in subfertile women are sparse with conflicting results. Rao et al. (17) concluded that no difference in ovarian reserve was indicated by FSH, AMH, and AFC when a TSH cutoff value of 2.5 μIU/mL was used.
In contrast, Weghofer et al. (16) reported that in euthyroid patients with infertility, AMH levels were significantly lower in women with serum TSH levels >3.0 μIU/mL after adjustment for TAI and age. Another study also indicated a significant increase in the frequency of DOR with increasing TSH levels (12). Consistently, we also found a significant decline in AMH levels, decreased AFCs, and increased prevalence of DOR in infertile euthyroid women with moderately high preconception TSH levels.
The DOR was further supported by worse reproductive outcomes, including a lower live birth rate and a higher rate of pregnancy loss among biochemical pregnancies, in women with high-normal TSH levels. Intriguingly, the concentration of TSH was also found to be negatively associated with both AMH levels and bilateral AFCs, independently of the current classification of high- and low-normal TSH values, suggesting potential dose-dependent effects of TSH on ovarian reserve.
Collectively, these data suggested that thyroid dysfunction may exacerbate decreased ovarian reserve, which may be associated with a lower live birth rate and higher biochemical miscarriage rate, although the increase in risk in terms of absolute events is limited.
Further exploratory stratified analyses indicated that the association between thyroid dysfunction or TAI and ovarian reserve was considerably modified by the underlying infertility diagnosis (17,25). For example, thyroid function or TPOAb positivity was not associated with AFC when the infertility diagnosis was not taken into consideration. However, when analyses were stratified by infertility diagnosis, an association of lower fT3 levels and TPOAb positivity with lower AFCs was identified among women with either DOR or unexplained infertility (25).
Rao et al. (17) found that subtle hypothyroidism was associated with lower ovarian reserve in patients with only tubal factor and unexplained infertility, but not in those with other infertility diagnoses. In our study, we observed a positive association in women with either ovulation dysfunction or unexplained infertility, which is consistent with data from the study by Arojoki et al. (4).
Taken together, we can speculate that even mild variation in thyroid dysfunction within the normal range may be an important risk factor for DOR and idiopathic infertility. The discrepancies among these studies may be, at least partially, due to several parameters such as sample size, with some subgroups among different infertility diagnoses being too small to adequately quantify differences in effect estimates.
TAI is the most common autoimmune disorder in reproductive-age women and increases the risk of thyroid dysfunction. Accumulating evidence has demonstrated that TAI could independently impair the ovarian reserve and result in ovarian senescence in euthyroid women (3,26 –28). Therefore, the population was further stratified based on TAI status to determine whether TAI positivity would affect the association of TSH with ovarian reserve.
In contrast to the study by Osuka et al. (29), which found no differences in serum AMH levels between TPOAb- or TGAb-positive women and TAI-negative women, we found that women with positive TAI showed decreased AFCs and a lower trend of AMH levels. Interestingly, a strong correlation of moderately high TSH levels with decreased AMH levels or AFCs was observed in the TAI-negative subgroup rather than in the TAI-positive subgroup.
This result needs to be interpreted with caution and two possibilities are proposed. First, the sample sizes in subgroups with positive TAI might be a bit small, which could not ensure adequate power to detect statistical significance (about 200 cases in each TAI-positive subgroup). Second, the detrimental effect imposed on ovarian reserve by TAI might be more prominent than slightly increased TSH levels within the euthyroid status. The synergistic or additive effects between TAI and subtle thyroid dysfunction on ovarian function decline warrant further research.
To the best of our knowledge, this is the largest cross-sectional study to clarify the association of subtle thyroid insufficiency with ovarian reserve in infertile euthyroid women attempting conception before ART treatment. Our study provided new insights into the risk factors for a decline in ovarian reserve.
Our data, from the perspective of ovarian reserve, further supported the recent recommendation by ETA and ATA that women seeking pregnancy through ART treatment should undergo levothyroxine treatment of subtle hypothyroidism (TSH levels >2.5 μIU/mL) with the goal of achieving a TSH level <2.5 μIU/mL (28).
The reliability of the results was enhanced by in-depth analysis within a unified euthyroid population. First, participants were screened with strict inclusion and exclusion criteria. Any cases with missing data on thyroid function or ovarian reserve were excluded to avoid selection bias. Additionally, cases with known causes of low ovarian reserve (iatrogenic causes and karyotypic abnormalities) were also excluded. Second, our analysis of thyroid parameters in relation to ovarian reserve was performed for both continuous and categorical variables. Third, further stratification analysis by different causes of infertility and TAI status provided more evidence for individualized fertility counseling.
A few limitations are also noted. Even if the association between moderately high TSH and ovarian reserve persists when properly controlled for confounding variables, it remains challenging to claim causation due to the retrospective cross-sectional nature. In addition, experiments are warranted to comprehensively delineate the pathways of thyroid hormone action on ovaries and to thoroughly investigate the impact of thyroid insufficiency on fertility and ovarian function.
Conclusions
Overall, we demonstrated that subtle thyroid dysfunction was associated with an increased risk of adverse impacts on ovarian reserve, especially in women with ovulation dysfunction and unexplained infertility or those negative for TAI. Our data add evidence that strengthens the systematic screening of TSH/TAI-Abs in infertile women before ART treatment from the perspective of ovarian reserve status and may contribute to the discussion on the use of specific TSH cutoff values in predicting ovarian reserve.
Future well-designed prospective studies will help to determine the optimal cutoff value of TSH in the setting of infertility treatment and evaluate whether levothyroxine supplementation may improve the ovarian function in infertile women attempting pregnancy through ART treatment with TSH levels >2.5 μIU/mL.
Footnotes
Acknowledgments
The authors are grateful to the subjects for taking part in the research.
Authors' Contributions
N.L. was responsible for data extraction, statistical analysis, and manuscript writing. Y.L., P.S., and Z.L. performed the data extraction and scrutinized clinical electronic information. Y.Q. contributed to interpretation of results and manuscript editing. X.J. was responsible for the concept and design and writing of the manuscript.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This study is supported by the National Natural Science Foundation of China (82171651, 82125014, and 81971352) and Project of Medical and Health Technology Development Program in Shandong Province (202005010523).
Supplementary Material
Supplementary Table S1