
Abstract
Background:
Due to the excellent prognosis and relatively high incidence of small low-risk thyroid cancers, more conservative management strategies such as active surveillance (AS) or hemithyroidectomy (HT) may be preferable to total thyroidectomy (TT) for patients seeking to balance long-term survival rates with the potential adverse effects of overtreatment. The aim of this review was to synthesize key factors or variables that inform patient decision making about treatment for low-risk thyroid cancer, from current primary investigations that presented participants with information facilitating this choice.
Methods:
Studies were identified from the Medline, Cochrane, and Embase databases up until March 2022. Study characteristics were extracted into a pre-piloted form. Factors were hypothesized to include treatment-related risks and possible outcomes and identified from a review of studies with consensus by discussion.
Results:
The search identified 444 unique studies: 397 were excluded on review of abstract and title with 47 studies undergoing a full text review and 6 studies identified to be eligible. Four were cross-sectional: one a prospective cohort study and one a mixed-methods study with both a prospective observational and qualitative component. The decisions addressed included: the choice between AS versus surgery (HT and/or TT) and HT versus TT and enrolled participants ranging from healthy volunteers to thyroid cancer patients. Treatment choice was the primary outcome in five studies. Across the studies, participants who were given the option of AS or surgery predominately chose the more conservative pathway, with a range of 70–84%. The major factors represented by information provision in the studies were risk of cancer recurrence or spread, need for hormone replacement therapy, and voice change.
Conclusions:
A framework of key factors informing patient treatment choice may be derived from current studies involving information provision for low-risk thyroid cancer management. Further research evaluating the efficacy and optimal timing for decision support interventions would help inform the design and clinical use of these tools to promote shared decision making.
Introduction
Traditionally, total thyroidectomy (TT) has been the standard of care for thyroid cancer patients, followed by radioactive iodine therapy. This management paradigm has substantially minimized the risk of recurrence or morbidity for patients with tumors ≥1 cm (1). However more recently, the increased detection of well-differentiated small low-risk thyroid tumors due to improvements in the quality of cancer imaging technology (2) has called for a re-evaluation of this one-size-fits-all treatment standard.
More recent studies have shown that survival rate is not tangibly affected by whether patients choose to undergo TT versus hemithyroidectomy (HT) for tumors 1–4 cm in size (3). Due to the excellent prognosis and relatively high incidence of most small thyroid cancers, more conservative management strategies such as active surveillance (AS) or HT have become established treatment options and may be preferable for patients seeking to balance long-term survival rates with the potential adverse effects of overtreatment (4).
Such evidence has led to the American Thyroid Association endorsing a choice of either HT or TT for low-risk differentiated thyroid cancer of 1–4 cm, and AS as a viable alternative for selected patients, especially for those with papillary thyroid micro carcinomas (5).
When deciding on treatment, patients and clinicians have to balance the slightly higher recurrence rate among patients who have pursued HT (6), against the higher rate of surgical complications and potential subsequent lower quality of life from TT (7). Moreover, the psychological challenges of potentially carrying a small cancer may make AS an unviable pathway for some (8). As a result, patient decision after the diagnosis of low-risk thyroid cancer is a complex one that must consider both demographic and diagnostic factors, as well as individual patient preference and risk tolerance.
Many clinicians use written or visual information to explain to patients the treatment options and from this review we sought to understand what information is presented to participants in research studies that have evaluated treatment choice.
The aim of this scoping review was to synthesize the key factors that inform patient decision making about treatment for low-risk thyroid cancer, from current primary investigations that presented participants with information facilitating this choice. We also sought to evaluate the effect and efficacy of different modes of information provision and identify any gaps in the evidence.
This knowledge will crucially inform the future design of decision support tools for addressing this nuanced choice within thyroid cancer management and may guide various practicing physicians to incorporate the unique factors of their own health care contexts, such as varied follow-up practices and cultural considerations, within an existing framework.
Methods
Review question
“What factors inform individual treatment choice for AS, HT and TT for low-risk thyroid cancer?”
Protocol
The scoping review was performed according to the Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) reporting guidelines for scoping reviews (9). A PRISMA checklist for this review is available in Supplementary Appendix SA1. This study was initially designed as a systematic review with the title “A systematic review of decision aids for low-risk thyroid cancer patients deciding between active surveillance, hemithyroidectomy and total thyroidectomy” and the review question “What are the factors which inform patient decision on active surveillance and hemithyroidectomy versus total thyroidectomy for low-risk papillary thyroid cancer?.” The study was changed to a scoping review after reviewing the included studies, with the realization that the definition of the term “decision aid” was initially misunderstood by the senior author. The protocol for the initial systematic review was prospectively registered with PROSPERO registration number: CRD42021286083.
Search
An inclusive list of search terms was developed in consultation with a literature search specialist from the University of Sydney Medical School Library (Supplementary Appendix SA2) and with authors (J.W., B.N.). The search strategy was partially adapted from a previous systematic review exploring decision aids for early breast cancer that had a comprehensive search strategy for recalling records concerned with decision support tools and decision making (10). The search was conducted in Medline, Embase, and Cochrane databases, retrieving records from inception up to March 2022 (by authors J.W., M.T., A.G.).
The gray literature was reviewed by a search of Google Scholar. Reference lists were also searched for articles that were missed by the database search. After removing duplicates, abstracts and titles were screened for eligibility (by authors J.W., M.T.). After this, full text screening was conducted by two independent study authors (J.W., M.T.) to curate a collection of original research articles for inclusion. Differences were resolved via discussion by all authors.
Inclusion and exclusion criteria
Studies were included if they were primary investigations that presented participants with information surrounding two or more treatment options for low-risk thyroid cancer, their associated risks, and potential benefits, and they prompted a treatment choice. Studies were needed to address the initial treatment decision for at least one of AS, HT, or TT. Moreover, eligible studies needed to report participant outcomes in relation to the factors provided.
Factors were hypothesized to include treatment-related risks and potential outcomes of each treatment and defined from an independent review of studies by authors J.W., M.T., and A.G. and a discussion by these authors to identify the factors presented to participants in each study.
Studies were excluded if there was no assessment of the impact of information provision on treatment choice and if the studies were reviews, commentaries, or editorials. Protocols where outcomes were not reported were also excluded. Detailed inclusion and exclusion criteria are presented in Supplementary Appendix SA3.
Data were extracted with use of a pre-piloted form in Excel. The following characteristics were extracted for eligible studies: location where the study was performed, type of decision support, treatment modalities presented, comparator group, study design, number of participants, population description, and outcomes/results. Studies were not assessed by formal critical appraisal of bias or validity by using a systematic assessment tool due to the heterogeneity of the studies. The heterogeneity of studies, and their respective outcomes did not support the pooling of results and no meta-analysis was performed.
Results
Study characteristics
The initial search yielded 495 records. After removing 51 duplicates, 444 unique studies were identified (Fig. 1). Three hundred and ninety-seven of these were excluded based on title and abstract, leaving 47 records to be assessed. Full text screening resulted in the inclusion of six original research articles for analysis, with excluded articles outlined in Supplementary Appendix SA4. No additional studies were discovered from a review of the gray literature.
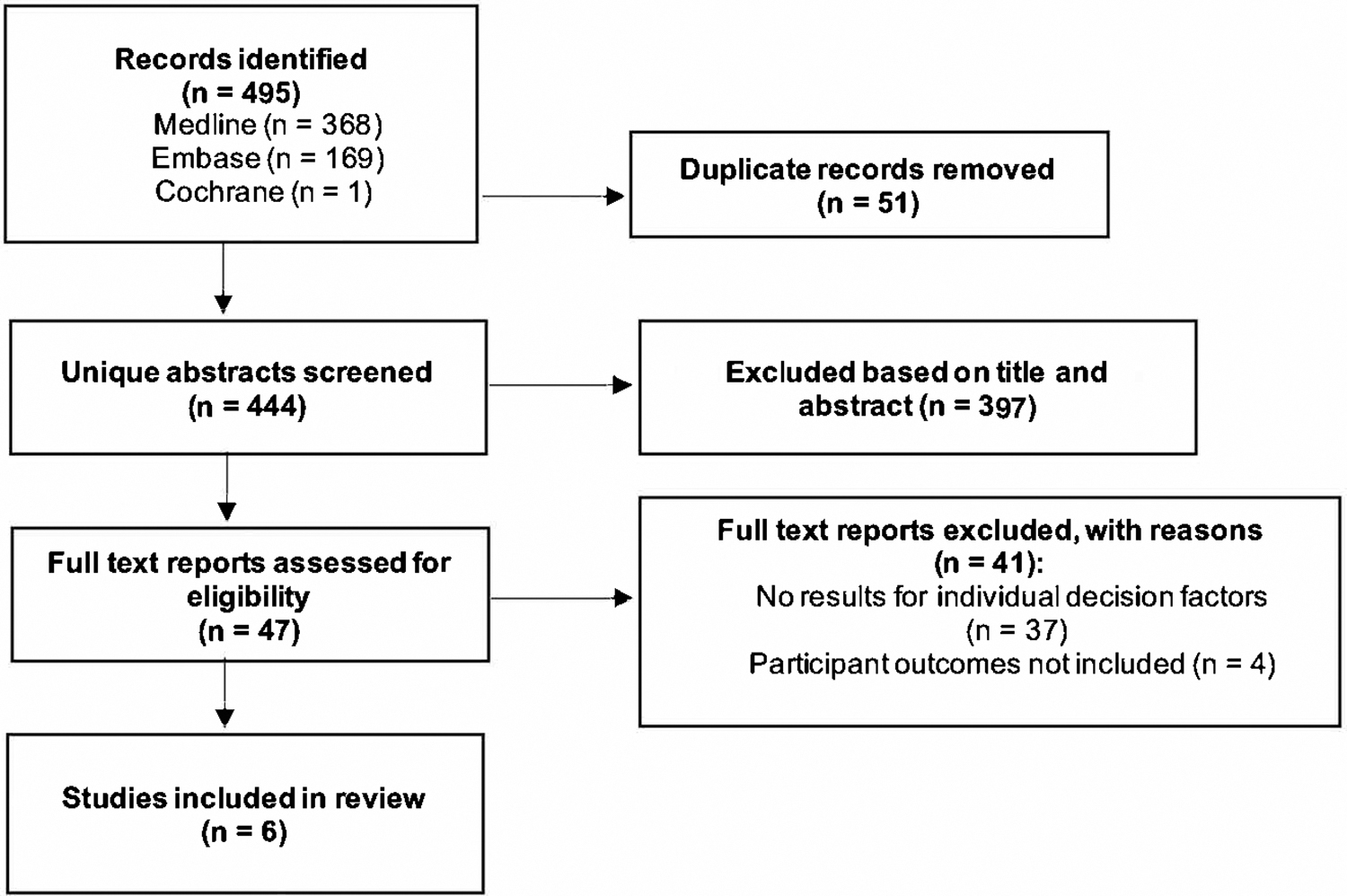
PRISMA flow diagram. PRISMA, Preferred Reporting Items for Systematic reviews and Meta-Analyses.
The study populations varied, with three studies utilizing healthy volunteers making hypothetical decisions and three studies including patients with a diagnosis of thyroid cancer and/or patients undergoing surgery for thyroid nodules. The characteristics of included studies are summarized in Table 1 for healthy volunteers and Table 2 for studies using patients diagnosed with thyroid cancer or thyroid nodules. Of the studies, four were cross-sectional, one was a prospective cohort study, and one was a mixed-methods study involving both a prospective observational and a qualitative component.
Study Characteristics and Outcomes for Healthy Volunteers
AS, active surveillance; CI, confidence interval; CrI, credible interval; DCE, discrete choice experiment; HT, hemithyroidectomy; MRS, marginal rate of substitution; PTC, papillary thyroid cancer; SD, standard deviation; TT, total thyroidectomy.
Study Characteristics and Outcomes for Patients with Thyroid Cancer or Thyroid Nodules
Five studies addressed the choice between AS and surgery. Three of the five studies differentiated between the modalities of HT and TT: Two assisted the participants in deciding between all three options, and the other between AS and HT (Tables 1 and 2). The final study addressed the choice between the two surgical modalities.
Outcome measures
Treatment choice was the primary outcome measure in five studies and the sole outcome measure of three. Sawka et al. (11) was the sole paper to report on the usefulness of the information presented as an outcome measure. In Dixon et al. (12), an approach was taken where the preference weight placed on the cancer disease label was compared with that of other attributes, to determine its role in patient decision making. The two online surveys by Nickel et al. (13,14) also considered the effect of cancer terminology on treatment choice and anxiety.
Information provision
Information presentation and clinical usage
Information presented to study participants took varied forms, both physical and digital. Most studies incorporated multimedia elements such as diagrams and graphs to illustrate statistical information. Brito et al. designed a conversation aid pamphlet to be used during clinical consultation (15). As a conversation aid, it was intended to trigger discussion between clinician and patient rather than solely act as a repository of information.
Accordingly, the paper-based format was determined most suitable for this function, although patient evaluation of this format was not explicitly assessed. Further, a decision-board style was utilized, with four panels each focusing on one aspect of patient concern: options available, physical effects of treatment, cancer growth and spread, and lifestyle impacts.
Online-based surveys also took a variety of formats. The online surveys by Dixon et al. and Nickel et al. were designed to be completed by a randomly sampled pool of predominantly healthy respondents (12 –14). As such, the online infographic format was employed, with each foregrounded by a hypothetical scenario that participants were to envision.
Dixon et al. presented the information in three successive panels: the first detailing the hypothetical scenario, the second providing statistics on the risks of each treatment option, and the third prompting participant choice for a particular scenario. Nickel et al. primarily relied on a table format to present more detailed statistical information in both a discrete choice experiment (DCE) and randomized crossover style survey, with minimal use of image aids (13,14).
Also utilizing an online DCE survey format, Ahmadi et al. combined use of infographics within a table format to prompt choice between two treatment options (16). This study was conducted on patients considering thyroid surgery. Finally, Sawka et al. presented patients with written information about low-risk papillary thyroid cancer prognosis, and the options of surgery or AS (11). This information was provided in conjunction with the opportunity to clarify questions in person with the study physician. All patients had already participated in a thyroid surgery consultation before enrollment in the study.
Information presented to participants
Information considered in each study is summarized in Table 3, with the level of risk attributed to each factor also included, where provided. As the written information presented to patients in Sawka et al. was not available, the factors considered in the study were omitted from this section of results. Factors in informing patient decision, as determined by the studies, were the risk of requiring hormone replacement therapy, cancer recurrence/spread, and voice change. These factors were considered in all five studies.
Information Considered in Each Study

Collectively, the risk of cancer recurrence/spread was presented to be between 0% and 7% after pursuing HT and 0% and 10% after pursuing AS. The risk of needing hormone replacement therapy after HT was presented to be between 20% and 50%.
For voice change, in Ahmadi et al. the risk after either HT or TT was presented to be between 1% and 14% (16). In Nickel et al., this risk was defined as 1–5% for HT and at 2–25% for TT (14). Brito et al., Dixon et al., and Nickel et al. differentiated between the short- and long-term risks to voice damage by informing patients about the likelihood of temporary hoarseness of voice as opposed to permanent voice change after surgery (12,13,15). The risk of temporary voice change was presented to be between 4% and 25%. The risk of permanent voice change was represented to be 2–5%. Other factors reported in studies were frequency of follow-up practices, risk of hypocalcemia, and chance of dying from thyroid cancer. Across the studies, the risk of death was presented as <1%.
The factors of scar appearance and the psychological impact of carrying cancer were considered in three and two studies, respectively. The chance of suffering from medicine side effects was also considered in two studies. Both Dixon et al. and Nickel et al.'s surveys investigated the effect of disease label on patient decision (12,14). These involved “cancer” and “tumor” as opposed to “nodule,” “abnormal cells,” and “lesion.” The other factors were reported in relation to these terminology frames.
Effect/efficacy of information
Treatment choice
Participants who were given the option of AS or surgery overwhelmingly chose the more conservative option throughout the studies, with a range of 70–84%. For thyroid cancer patients (Table 2), this was reflected in Brito et al. where 84% of patients overall opted for AS, a choice made more likely by the use of a conversation aid paper pamphlet (relative risk = 1.16, confidence interval [1.04–1.29]) (15). Similarly, in Sawka et al., the majority of patients preferred AS over surgery (70%) although no comparator group was included for analysis (11). Similar results were seen with healthy volunteers (Table 1).
Nickel et al. found that regardless of the terminology used, the initial treatment preference for AS was high at 72% (13). Ahmadi et al. investigated patient preference between HT and TT and similarly found that the average patient preferred the more conservative treatment, given that the chance of needing a second surgery remained below 30% (16).
Ahmadi et al. found that between HT and total TT, 35% of patient decisions could be explained by the risk of cancer recurrence, 28% by the risk of requiring a second surgery, and 19% by the risk of recurrent laryngeal nerve damage (16). Both risk of recurrence and voice change were risks represented across all the studies; however, the risk of requiring a second surgery was only considered in two. Nickel et al. additionally found that an increased chance of needing lifelong thyroid medication, hypocalcemia, high out-of-pocket costs, and frequent follow-up practices were factors for participants when considering treatment options (14).
Effect of terminology
In studies that considered the effect of cancer terminology on patient decision (n = 3), all of which focused on healthy volunteers, findings were varied. From the online DCE survey, Nickel et al. reported that the terminology used to describe the disease process did not significantly impact the relative influence of all attributes on treatment preferences with a few exceptions: the chance of needing lifelong thyroid medication, financial cost, and the risk of developing invasive thyroid cancer (14).
On the other hand, Nickel et al.'s randomized crossover style survey found that a higher proportion of participants (19.6%) chose TT when the cancer terminology was used as opposed to when the papillary lesion or abnormal cell terminology was used (10.5% and 10.9%, respectively) (13). Dixon et al. also found that the cancer disease label considerably affected participant decision making. Respondents accepted a four-percentage increase in the risk of progression/recurrence to avoid labeling their disease as cancer. Moreover, notably, preference for the nodule label was similar in magnitude to preference for AS over surgery (12).
Usefulness of information presented
One study considered the efficacy of information presented and health communication was reported to be enhanced by the factors presented (11). Sawka et al. quantified patient confidence in making the decision and ultimate decision satisfaction via the Decision Self-Efficacy Scale and Satisfaction with Decision Scales, respectively (11). Patients reported a high level of both decision self-efficacy (mean score of 94.3, where 100 reflected maximum confidence) and final decision satisfaction (mean score of 28.3 out of 30, where scores above 24 indicated a high level of satisfaction) across the board.
Discussion
Shared decision making for low-risk thyroid cancer is a complex process that must consider diagnostic factors, as well as individual patient preference and the ethos, experience, and outcomes of the treating medical team. The uniqueness of this review stems from being the first study to synthesize the primary literature surrounding factors informing choice for thyroid cancer specifically, focusing on the initial treatment decision between AS, HT, and TT for the low-risk thyroid cancer patient. Common factors conveyed by the studies were risk of needing thyroid hormone replacement therapy, cancer recurrence/spread, and voice change.
This review complements other studies on clinician decision-making factors and patient decision-making factors for low-risk thyroid cancer that do not present information regarding treatment choice (17,18).
From this review, we found that participants who were given the option of AS or surgery overwhelmingly chose the more conservative pathway, evidenced in Brito et al. (83%), Sawka et al. (70%), and Nickel et al. (72%). These results suggest that people may be more inclined to consider conservative treatment options when presented with adequate information. This corroborates with the evidence that major barriers to implementing AS are related to a lack of clinical consensus surrounding surveillance protocols, and lack of knowledge about the guidelines, impairing physician ability to comfortably recommend AS to patients (19).
The psychological impact of carrying a small cancer was raised by several of the studies, which may have been a factor deterring some patients from AS. This may be exacerbated by the cancer label itself, found to significantly raise participant mean anxiety and TT preference when compared with alternative terminologies in the randomized crossover survey by Nickel et al. (13). However, it is worth considering that levels of cancer worry experienced by patients undergoing AS in a Japanese study have been found to reduce over time, suggesting that psychological impacts are not necessarily prohibitive to AS success (20).
Moreover, Nickel et al. also found that participants who chose surgery reported higher levels of anticipated treatment-related anxiety compared with those who chose AS, suggesting that psychological effects of both pathways may be comparable (13).
Standardizing management strategies may improve patient-centered decision making; however, due to the imperfect nature of current risk stratification processes, clinical practices exhibit significant variability (21). Physicians must integrate factors from their respective local practice contexts alongside the general framework provided by factors raised in these studies to deliver the most effective care.
This is demonstrated in a study of benign thyroid nodular disease by Sabaretnam et al. that took into account culture-specific factors in a video-based decision tool for HT decision making in India (22). Socioeconomic differences in medical care worldwide can also significantly affect conventional practices between different countries, demonstrated in Japan where HT was adopted as the standard therapy over TT earlier than other countries (23).
Moreover, the quality of disease surveillance programs, patient economic status, education, and convenience of accessing medical resources may all impact patient adherence to AS follow-up programs, significantly impacting its suitability as a safe alternative to immediate surgery (24).
This review highlights the importance of clinicians and units knowing and reporting their outcomes to allow patient choice. It has been shown that for thyroid surgery, surgical outcomes are related to individual unit volume (3). Rates of permanent nerve injury quoted in some studies such as up to 5% in studies with healthy volunteers would be of concern for many thyroid surgeons in cases involving low-risk thyroid cancer, where a rate of less than 1% would be an aim (13,14,25).
Other local context-specific factors that could be included in decision support tools include the higher prevalence of multinodular thyroid disease in areas affected by iodine deficiency (26). This may lend itself to TT recommendation to avoid the need for follow-up and potential biopsies of contralateral nodules (27).
Another area of considerable practice variation surrounds completion thyroidectomy, necessitated by unexpected pathological findings such as angioinvasion or extrathyroidal extension found intraoperatively or postoperatively. Decision making presenting the HT alternative should inform the patient of this downstream risk, as it could significantly impact choices. Tuttle et al. have devised a useful framework that integrates three major domains of preoperative imaging/clinical findings, medical team characteristics, and patient characteristics to stratify patient suitability for conservative management strategies, which has the potential to be adapted for a variety of clinical contexts (28).
From the results of this study, we would propose that a better understanding of practice variation and local practice contexts could be obtained by the reporting of information in future research, which will help inform clinical practice as outlined in our proposed framework (Fig. 2). This framework has been synthesized from the results of this project and is presented by disease and treatment information provided with risks or likely outcome if a treatment choice decision study was to be performed in the authors' clinical institution. This framework is not intended to be used for patients when making treatment decisions but to provide an easy-to-access context of the information provided for other clinicians and researchers to better understand the outcomes of studies.
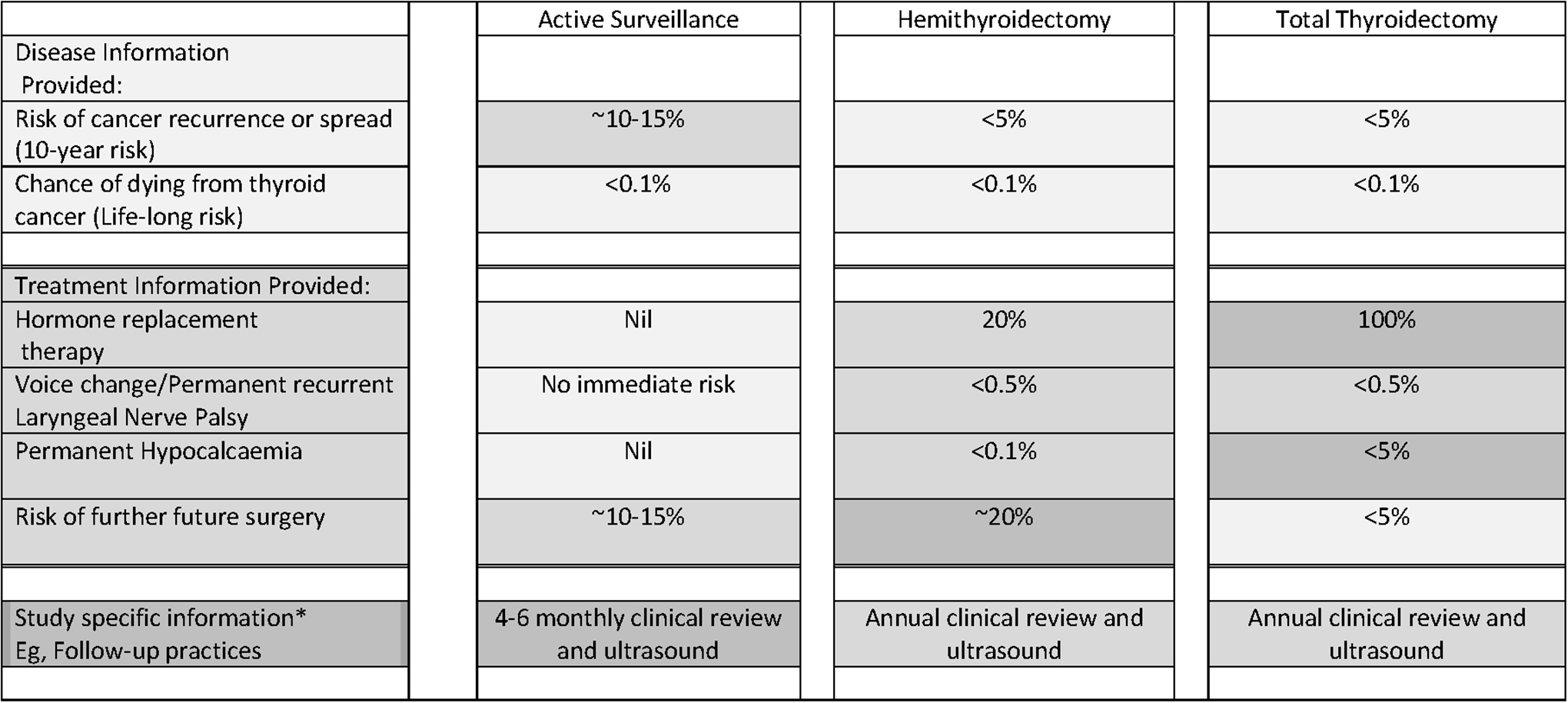
Proposed framework for presenting hypothetical information on treatment choices to patients with low-risk thyroid cancer. Values provided are hypothetical and would depend on institution treatment practices and study groups chosen. Darker colors have been used for presentation purposes to present higher risk or a more frequent event. *Future study-specific factor/s depending on study, cultural and location practices and could include factors such as cost, availability of treatment, waiting times, disease labels, and other information specific to future studies.
Of the studies reviewed, only one considered patient satisfaction with the study process, suggesting that more evidence is needed to determine which presentation attributes are the most useful for reducing decisional conflict, decisional regret, and empowering patient confidence. These factors could involve: the clinical context in which decision-making tools are used, prior patient knowledge, characteristics of the patient population, and time available to make decisions.
The limited randomized controlled trial evidence around thyroid cancer decision making points to the need for more high-quality evidence to inform both current and future practice. From the studies reviewed, only Brito et al.'s conversation aid was explicitly designed to be used as a decision aid. Further, three studies were conducted on predominantly healthy respondents in an online survey format rather than patients diagnosed with thyroid cancer, possibly limiting clinically relevant conclusions.
This draws attention to a gap in the literature for more comprehensive studies addressing authentic and country-specific patient groups. In addition to this, the timing of information presentation was also variable between studies; some studies were performed in consultation, whereas others were designed to model a pre-consultation context, or did not standardize this factor. Additional evidence is required to assess the optimal timing for information provision, to inform the design and use of future decision-making tools. For future studies, outcomes should incorporate knowledge gained, decisional conflict, and decision regret, to more holistically evaluate the utility of decision support tools (29).
With regards to the generalizability of these results and the outcomes presented, it is important to note that three of the six studies included participants who were healthy volunteers. As these participants have not received a diagnosis of thyroid cancer but had been asked to imagine a diagnosis, this has the potential to bias the results found. A thyroid cancer diagnosis will potentially change treatment decision-making factors due to the psychosocial impact of the diagnosis itself and due to their interactions with the health care providers (30). However, a study on healthy participants may be useful in modeling the perspective of a patient first learning about their diagnosis before consultation and discussion with clinicians.
Limitations of this review arise from the limited number of studies that precluded a systematic review and the studies' heterogeneity, so no formal systematic assessment of bias or validity was performed. Subsequently, results had to be synthesized qualitatively. The small pool of studies included indicates a need for further research in this emerging area to best empower patients and physicians to engage in appropriately risk-stratified and preference-sensitive decisions.
This is highlighted by our finding that this study was initially developed as a systematic review focusing on decision aids and the lack of research in this area for low-risk thyroid cancer offers the potential for further research. Due to the search criteria, other studies that directly assess the impact of factors such as family history of cancer and clinician influence on patient choice may not have been included in this review if information provision was not a feature of the experimental design.
To allow for a better understanding of patient decision-making studies and future research in this area, we have proposed factors that have been represented in the reviewed studies that could be reported in future studies (Fig. 2). This would allow a better understanding of the information that was provided to participants so that future studies can be better designed, replicated, and/or compared and the results potentially translated more easily to clinical practice.
Conclusion
In this review, we have identified the key factors informing patient treatment choice surrounding low-risk thyroid cancer. Decision-making tools offer great promise to help patients and clinicians manage nuanced decision making, potentially encouraging patients to choose more conservative options after being presented with a balanced benefit-and-risk analysis. However, more high-quality evidence is required to further evaluate the efficacy of decision support interventions, and the most suitable clinical contexts and timing in which they should be used to enhance shared decision making in thyroid cancer management.
Footnotes
Authors' Contributions
J.W.: Methodology, data collection, formal analysis, writing—original draft, writing—reviewing and editing; M.T.: Data collection, writing—reviewing and editing; B.N.: Methodology, writing—reviewing and editing; A.G.: Supervision, conceptualization, methodology, writing—reviewing and editing. All the authors were responsible for the final approval of the article.
Author Disclosure Statement
All the authors have no conflicts of interests to disclose.
Funding Information
A.G. is supported by a Cancer Institute NSW Early Career Fellowship (2019/ECF1081) for this project. B.N. is supported by a National Health and Medical Research Council (NHMRC) Emerging Leadership Research Fellowship (1194108).
Supplementary Material
Supplementary Appendix SA1
Supplementary Appendix SA2
Supplementary Appendix SA3
Supplementary Appendix SA4