
Abstract
Background:
Failure to escape from the Wolff–Chaikoff effect (WCE) causes hypothyroidism.
Methods:
This is the first report of myxedema coma after iohexol administration. The failure of the escape phenomenon in this patient was longer than existing reports.
Results:
The patient received 42,000 mg of iodine in iohexol cumulatively and developed myxedema coma after 16 days. She was subsequently found to have pre-existing primary hypothyroidism that was treated with levothyroxine 50 μg daily, but had defaulted treatment. She was discharged with levothyroxine 100 μg daily and this was weaned to 50 μg daily over 12 months.
Conclusions:
Iodine-based contrast media (ICM) can aggravate primary hypothyroidism. In severe cases, it may precipitate myxedema coma. Patients with thyroid disorders should be informed to monitor for aggravation of their symptoms after ICM administration. Long-term follow-up of thyroid function may be needed in patients who fail to escape from the WCE.
Introduction
The National Institutes of Health recommends daily iodine consumption of 150 μg for adults, 220 μg for pregnant females, and 290 μg for lactating females (1). When iodine consumption is excessive and serum iodine exceeds 50 to 350 μg/L (2), hyperthyroidism may develop, but is prevented by several physiological mechanisms. These mechanisms are collectively known as the Wolff–Chaikoff effect (WCE). The WCE is typically short lived and failure to escape from it causes hypothyroidism. We describe a patient who developed myxedema coma within 16 days of iohexol administration followed by a prolonged recovery period. This is the first reported case of myxedema coma after iohexol administration.
Institutional research ethics board approval is not required for a case report in the National University Health System of Singapore. Written informed consent was obtained from the patient.
Patient Information
A 65-year-old woman was admitted for recurrent pyogenic cholangitis. She reported a history of thyroid disorder but was unable to provide further details. She was clinically and biochemically euthyroid on admission (free thyroxine [fT4] 9.8 pmol/L, thyrotropin [TSH] 3.84 mIU/L). She underwent computed tomography mesenteric angiogram, image-guided biliary drainage, endoscopic retrograde cholangiopancreatography, and repeat image-guided biliary drainage within five days of admission. Iohexol (containing 350 mg/mL of iodine) was used for these. She received a cumulative dose of 42,000 mg of iodine within 5 days.
Events leading to myxedema coma
She became acutely confused 16 days after admission. Repeat thyroid function test showed a central hypothyroid picture (fT4 < 5.0 pmol/L, TSH 4.58 mIU/L). No additional causes were found to explain her confusion. Levothyroxine 25 μg daily was started by the internist. She became drowsy two days later. She was hypothermic and bradycardic: rectal temperature 35.6°C, pulse rate 58/min, respiratory rate 20/min, and blood pressure 119/73 mmHg. She appeared puffy and jaundiced. Her voice was croaky. She was diagnosed with myxedema coma and was referred to the endocrinologist.
Endocrinological evaluation and treatment
Corroborative history revealed no features of hypopituitarism, prior thyroidectomy, or family history of thyroid disorders. She had no goiter or temporal visual field deficits. She was found to have hypogonadotropic hypogonadism (Supplementary Material). No other pituitary hormone deficiency was found. Serum lithium was not detectable. Magnetic resonance imaging of the pituitary gland was normal. She was treated with a no-iodine diet, hydrocortisone, levothyroxine, liothyronine, and supportive measures in the intensive care unit. She was discharged with levothyroxine 100 μg daily.
Outpatient evaluation
Her pituitary hormone levels were normal three months after discharge from hospital. Hydrocortisone was subsequently stopped based on a robust response to the Synacthen® test.
Thyroxine replacement therapy
Her levothyroxine dose was gradually reduced from 100 μg daily to 50 μg daily over 12 months. Further reduction of levothyroxine led to a fall in her fT4 to the lower limit of normal (fT4 9.4 pmol/L, TSH 3.57 mIU/L).
History of thyroid dysfunction
It was discovered much later that she was diagnosed with Graves' disease in February 2001 and underwent radioactive iodine ablation in September 2002 and January 2005. She was lost to follow-up after February 2006. She was referred to an endocrinology clinic in May 2014 as she had experienced weight gain and cold intolerance. Her blood tests in May 2014 showed undetectable fT4 and mildly elevated TSH (fT4 < 3.2 pmol/L, TSH 6.64 mIU/L). Her pituitary hormone levels and thyroid autoimmune antibodies were normal in June 2014. She was treated with levothyroxine 50 μg daily since October 2014 but defaulted treatment after May 2015.
Her progress between February 2001 and December 2021 is summarized in the time line in Figure 1. Her thyroid function tests are summarized in Table 1.
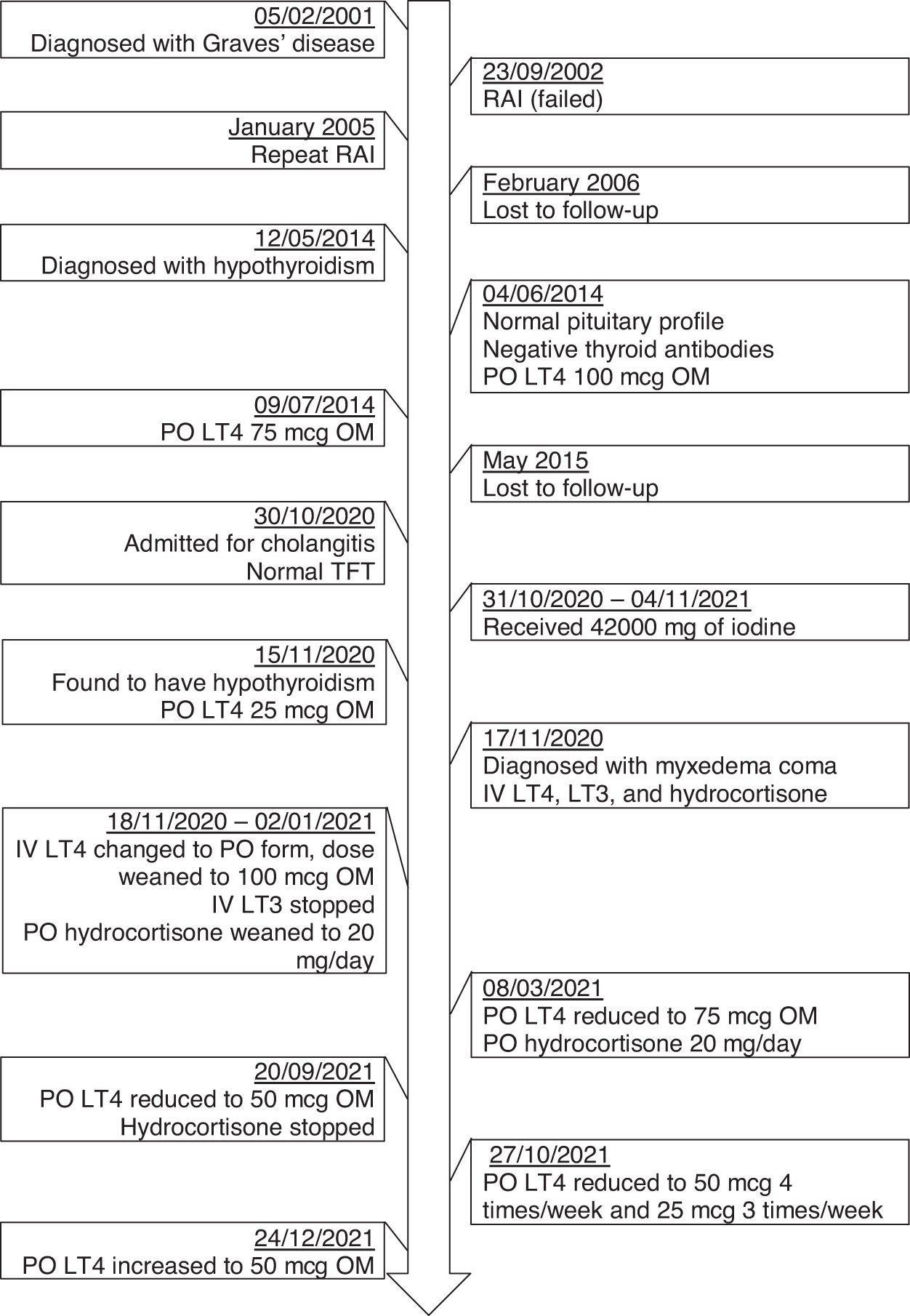
Time line of events between 2001 and 2021. Anti-TPO Ab, antithyroid peroxidase antibody; E2, estradiol; FSH, follicle stimulating hormone; fT4, free thyroxine; LH, luteinizing hormone; TRAb, thyrotropin receptor antibody; TSH, thyrotropin.
Laboratory Tests at Important Time Points Between 2001 and 2021
Further considerations
Her thyroid function tests in May 2014 and November 2021 suggest partial TSH deficiency. The TSH releasing hormone test may be helpful in assessing her TSH reserve, but this could not be done as she could not be weaned off levothyroxine.
Discussion
The WCE was first described in vitro in 1944 by Morton et al. (3). The in vivo effects were subsequently described by Wolff and Chaikoff in 1948 (4). It occurs between 48 hours and 10 weeks after acute iodine excess (5 –8). Clinically significant hypothyroidism due to the WCE has been attributed to iodine-based contrast media (ICM) use in coronary angiography (9), lipiodol contrast use in lymphography (5), saturated solution of potassium iodide use in the treatment of cutaneous mycoses (6,10), antiseptic solution use on wounds and peritoneal dialysis catheters (11 –13), iodine-containing expectorant consumption (14), and amiodarone therapy.
We described the first case report of myxedema coma arising from iohexol-induced WCE. The patient developed severe hypothyroidism after 16 days from iodine administration and lapsed into myxedema coma. This report highlights the need to be aware of potential hypothyroidism after ICM use, especially in people with partial thyroid insufficiency. The WCE may diminish the residual thyroid function in these people and a higher dose of thyroxine replacement may be needed until the escape phenomenon occurs.
The odds ratio of developing overt hypothyroidism after ICM administration was 3.05 (95% confidence interval [CI] 1.07–8.72) (15). The adjusted hazard ratio reported in a retrospective cohort study from Taiwan showed this risk to be 2.00 (CI 1.65–2.44). The risk for hypothyroidism increases with age, female gender, and with repeated ICM exposure (16). The risk for iodine-induced hypothyroidism may be higher in people living in iodine-replete areas (17).
The WCE eventually wears off even if iodine excess persists. This adaptive process is termed the escape phenomenon, and it occurs between 2 days and 5 months after iodine withdrawal (4 –6,8,11,18). The escape phenomenon occurs secondary to a reduction in transcription of the sodium iodide symporter gene and consequently reduced follicular iodine uptake (19 –23). Failure of the escape phenomenon can arise from failure in downregulation of the sodium iodide symporters and iodine organification (7).
This patient took an unusually long period to escape from the WCE. Her thyroxine replacement dose could only be weaned to precrisis level (0.8 μg/kg body weight per day) after 12 months. This case highlights the variability in duration taken for the escape phenomenon to occur. It casts uncertainty in the duration needed to monitor the thyroid function after development or aggravation of hypothyroidism in such patients. Markou et al. recommended long-term follow-up of such patients as they believe many of them will progress to permanent hypothyroidism (24). This recommendation is not substantiated by prospective studies. The European Thyroid Association Guidelines for the management of ICM-induced thyroid dysfunction did not provide any recommendation on this (25).
This patient has underlying Graves' disease and received two courses of radioactive iodine previously. This is a risk factor for failure of the escape phenomenon (26). Other risk factors include nodular goiter (27 –29), chronic systemic diseases, positive thyroid autoantibodies, history of subacute thyroiditis, history of postpartum thyroiditis (30), history of interferon-alpha-induced thyroid dysfunction, Hashimoto's thyroiditis (31), and renal impairment (32,33).
It is unknown whether certain ICMs are safer in people with thyroid dysfunction. The European Thyroid Association Guidelines for the management of ICM-induced thyroid dysfunction compared various ICMs but made no comments on the safety of these agents (25). Iohexol is a nonionic water-soluble ICM that was found to be well tolerated between 125 and 1500 mg of iodine/kg of body weight (34,35).
This patient developed hypothyroidism after receiving 700 mg of iodine/kg of body weight. In comparison, iopromide, a monomeric nonionic ICM, was found not to cause thyroid dysfunction in two small pediatric studies [1 cohort study including 20 infants (36) and 1 retrospective observational study including 23 infants and young children (37)]. The small number of study subjects and observational design of these studies restrict the generalizability of these findings to the adult population.
Conclusions
ICMs can induce the WCE and aggravate existing primary hypothyroidism. In severe cases, it may precipitate myxedema coma. ICMs should be used cautiously in patients with thyroid disorders. It may be prudent to monitor the thyroid function of patients with partial thyroid insufficiency after ICM administration. Iopromide may be safer than iohexol in this group of patients. We recommend screening for a history of thyroid dysfunction before ICM administration. The outcome of patients who have prolonged WCE is not known and long-term follow-up of thyroid function may be needed in patients with failure of the escape phenomenon.
Footnotes
Authors' Contributions
E.-L.T. acquired and interpreted the data, drafted and revised the article, approved the final version of the article for publication, and agree to be accountable for all aspects of the study in ensuring that questions related to the accuracy or integrity of any part of the study are appropriately investigated and resolved. A.T.A. contributed to the acquisition of data, revised the article, approved the final version of the article for publication, and agree to be accountable for all aspects of the study in ensuring that questions related to the accuracy or integrity of any part of the study are appropriately investigated and resolved. N.C. contributed to the acquisition of data, revised the article, approved the final version of the article for publication, and agree to be accountable for all aspects of the study in ensuring that questions related to the accuracy or integrity of any part of the study are appropriately investigated and resolved.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.
Supplementary Material
Supplementary Material