
Abstract
Introduction:
Pediatric papillary thyroid carcinomas (PTCs) are more invasive than adult PTCs. No large, contemporary cohort study has been conducted to determine whether younger children are at higher risk for advanced disease at presentation compared to adolescents. We aimed to describe pediatric PTC and contextualize its characteristics with a young adult comparison cohort.
Methods:
The National Cancer Database was interrogated for pediatric and young adult PTCs diagnosed between 2004 and 2017. Clinical variables were compared between prepubertal (≤10 years old), adolescent (11–18 years old), and young adult (19–39 years old) groups. Multivariable logistic regression modeling for independent predictors of metastases was conducted. A subanalysis of microcarcinomas (size ≤10 mm) was performed.
Results:
A total of 4860 pediatric (prepubertal n = 274, adolescents n = 4586) and 101,159 young adult patients were included. Prepubertal patients presented with more extensive burden of disease, including significantly larger primary tumors, higher prevalence of nodal and distant metastases, and increased frequency of features such as lymphovascular invasion, and extrathyroidal extension (ETE). Prepubertal age was an independent predictor of positive regional nodes (adjusted odds ratio [AOR] = 1.36 [95% confidence interval {CI} 1.01–1.84], p = 0.04) and distant metastatic disease (AOR = 3.12 [CI 1.96–4.96], p < 0.001). However, there was no difference in survival between groups (p = 0.32). Prepubertal age independently predicted lymph node metastases for microcarcinomas (AOR = 2.19 [CI 1.10–4.36], p = 0.03). Prepubertal (n = 41) versus adolescent (n = 937) patient age was associated with gross ETE (p = 0.004), even with primary tumors ≤1 cm in size.
Conclusions:
Patients aged <11 years old present with more advanced disease than adolescents, with a higher likelihood of nodal and distant metastatic disease at time of diagnosis, although survival is high. Prepubertal children undergo more extensive treatment, likely reflective of more invasive disease at the outset, even in the setting of a subcentimeter primary tumor.
Introduction
Pediatric differentiated thyroid carcinoma (DTC) is rare, although its incidence has increased over time, with 6.4 cases per 1,000,000 diagnosed between 1997 and 2008 and 11.0 cases per 1,000,000 diagnosed between 2009 and 2018. 1 While pediatric DTC only accounts for 1% of pediatric cancer cases in prepubertal children, the disease comprises 7% of adolescent cancer cases for patients aged 15–19 years old. 2 More than 90% of pediatric DTCs are papillary thyroid carcinomas (PTCs), as follicular carcinoma is uncommon in children. 3 –5 Survival is high, with a cause-specific mortality of only 1% at 30 years. 6 Children are ultimately less likely to die of the disease than adults, even in the presence of distant metastases, and 30-year recurrence rates are comparable. 6
PTC has been reported to present more extensively in children compared to adults. Historically, studies have demonstrated that up to 57% of pediatric PTCs are multifocal and 30% are bilateral. 7 –11 Children have traditionally presented with more distant and locally advanced disease as well, with pulmonary metastases diagnosed in up to 25% of cases. 3,7,8,11 –14 One of the only large analyses conducted for pediatric PTC studied 740 Belarusian children, 92% of whom were exposed to radiation as a consequence of the Chernobyl nuclear disaster, and found that younger age was associated with recurrent nodal disease and pulmonary metastases. 15 Much of the historic data were obtained in the context of a significant proportion of these patients having undergone ionizing radiation to the head and neck before diagnosis. 16 Now only 3% of patients present with a history of ionizing radiation. 17
The American Thyroid Association (ATA) published its first set of guidelines for pediatric DTC in 2015. 18 Based on the data characterizing pediatric PTC as more invasive, total thyroidectomy was recommended as the initial surgical approach for almost all pediatric PTC patients, with a prophylactic central neck dissection to be considered at the time of surgery. 18 At the time the guidelines were written, the ATA stated that it was unclear whether younger patients are at higher risk. 18 More recent studies have further described contemporary pediatric PTC and have attempted to investigate whether outcomes differ for younger children compared to adolescents. These analyses have found that closer to 35% of pediatric patients present with multifocal disease, 19,20 although estimated rates of distant metastases at presentation still range from 5% to 19%. 6,20 –25
The literature also suggests that for pediatric PTC, younger age at presentation is associated with recurrence, 26,27 distant metastases, 6,21,22,27,28 extrathyroidal extension (ETE), 27,28 lymphovascular invasion (LVI), 5 and regional lymph node positivity. 27 –29 One recent study demonstrated that prepubertal compared to pubertal patients had a greater extent of DTC as evaluated by the ATA risk classification; however, there were only 54 patients in total, 9 of whom were prepubertal. 30 Pediatric PTC remains a rare disease, and these analyses are based on retrospective, single-institution reviews of small cohorts of patients, which may undermine their conclusiveness and generalizability. Although additional studies have been published in the intervening years since the guidelines were written, as reviewed here, large-scale analysis of prepubertal PTC patients is needed to help guide management and support or refute the existing data.
We aimed to validate the existing literature with respect to the presentation of pediatric PTC using a large, diverse, generalizable patient cohort, as well as compare disease severity at time of diagnosis to that of young adults with PTC. In addition, we strove to determine whether prepubertal children present with more extensive disease than adolescents. The goal of this study was to further our understanding of the relationship between age and progressive PTC to improve management of pediatric patients. We used the National Cancer Database (NCDB), a comprehensive clinical oncology database sponsored by the American College of Surgeons and the American Cancer Society, to address our aims. 31
Materials and Methods
Study population and definitions
The NCDB was queried for all pediatric (≤18 years old) and young adult (19–39 years old) patients diagnosed with PTC between 2004 and 2017 using the primary site code of C73.9, and papillary histology codes as defined by the International Classification of Diseases for Oncology, third revision. Patients with benign disease (134), nonpapillary histology (10,050), and who were diagnosed at the reporting facility but treated elsewhere (2577) were excluded (Supplementary Fig. S1). Pediatric patients were classified as prepubertal (≤10 years old) or adolescent (11–18 years old). The NCDB extracts patient variables, including patient demographics, cancer staging and treatment, and overall survival from >70% of newly diagnosed cancer cases in the United States from 1500 Commission on Cancer-accredited facilities. 31
The NCDB faithfully captures pediatric patients, with a coverage rate of 68% of all pediatric (<19 years old) and 79% of all adolescent and young adult (15–39 years old) cancer diagnoses in the United States. 32 LVI was reported for patients diagnosed between 2010 and 2017, while ETE was coded for patients diagnosed from 2004 to 2015. Noncoded data were excluded for those variables as detailed in Tables 2 and 3. Missing data were otherwise detailed. The thyroid is not considered a paired organ in the NCDB; as such, bilaterality is not a coded variable.
A prophylactic lymphadenectomy was defined as one performed in the setting of a clinical N0 nodal stage, while a therapeutic lymphadenectomy was defined as one in which the patient was diagnosed as clinically stage N1. “Neck dissection, NOS” describes a patient who underwent a lymphadenectomy but for whom clinical nodal stage was not coded or unknown. The clinical stages for the NCDB registry are coded by the physician or registry staff based on the medical record and the AJCC Cancer Staging Manual edition in use during the year in which the case was diagnosed. The Weill Cornell Medicine Institutional Review Board designated this analysis as exempt, given the use of publicly available deidentified data.
Statistical analysis
Demographic, tumor, and treatment variables were first compared between prepubertal and adolescent patients, and then between all three groups (prepubertal, adolescent, and young adult; denoted as “all” preceding the p-value) using Pearson's chi-squared test for categorical variables and the Kruskal–Wallis test or Wilcoxon's rank-sum for continuous nonparametric data, as appropriate. Multivariable logistic regression modeling for independent predictors of positive regional lymph node and distant metastases in pediatric patients (≤18 years old) was performed. Sex, race, ethnicity, tumor size, LVI, ETE, and multifocality were found to predict metastases to lymph nodes and distant organs at an alpha level of 0.01 on univariate analysis and were included in the multivariable models. Adjusted odds ratios (AORs) are reported. Kaplan–Meier analysis for overall survival for all three groups was executed.
Finally, a subanalysis of tumor and treatment characteristics for microcarcinomas (tumor size ≤10 mm) was conducted. Multivariable regression modeling for independent predictors of regional lymph node metastases in the pediatric (≤18 years old) cohort was performed for the microcarcinoma subgroup. Sex, ethnicity, LVI, ETE, and multifocality predicted regional lymph node disease on univariate analysis at an alpha level of 0.01 and were included in the multivariable model for the microcarcinoma cohort. A multivariable model for distant metastatic disease in the microcarcinoma cohort could not be constructed as sample sizes were insufficient. All statistical tests were performed using Stata software, version 16.1 (Stata Corp., College Station, TX). Significance was evaluated at the 0.05 alpha level and hypothesis tests were two-sided.
Results
This analysis included 4860 pediatric (prepubertal n = 274, adolescent n = 4586) and 101,159 young adult patients for a total sample size of 106,019. Clinicodemographics differed significantly between pediatric and young adult cohorts (Table 1). The median ages for each group were as follows: prepubertal 9 years old (interquartile range [IQR] 7–10), adolescent 16 years old (IQR 15–18), and young adult 32 years old (28–36) (all p < 0.001).
Clinicodemographics Summary of Pediatric and Young Adult Cohorts
Data are presented as n (%) or median (IQR). Bolded numbers represent statistically significant p-values.
Prepubertal age group versus adolescent age group.
Prepubertal age group compared to adolescent group and to young adult group.
Area-based measure of rurality and urban influence, using the typology published by the USDA Economic Research Service.
Median distance traveled for treatment for overall cohort was 11.2 mi.
IQR, interquartile range; USDA, United States Department of Agriculture.
Female sex comprised 82.0% (n = 3760) of the adolescent group and 82.6% (n = 83,546) of the young adult group, which differed from the only 64.6% (n = 177) of female patients in the prepubertal group (all p < 0.001). A higher proportion of prepubertal patients were Hispanic (n = 58, 21.2%) compared to the adolescent (n = 680, 14.8%) and young adult (n = 11,706; 11.6%) groups (all p < 0.001). Prepubertal patients were least likely to undergo treatment in a rural county (all p < 0.001) and had to travel further to obtain care (all p < 0.001).
Prepubertal patients present with more extensive disease than either adolescent patients or young adult patients (Table 2). Children younger than the age of 11 years presented with larger primary tumors, with 22.6% (n = 62) of prepubertal patients presenting with tumors >4 cm in size. Only 13.5% (n = 620) of adolescent children and 8.3% (n = 8363) of young adults presented with such large tumors (all p < 0.001). In addition, prepubertal compared to adolescent patients more frequently presented with LVI (n = 74, 57.8% vs. n = 898, 36.1%, p < 0.001), and gross ETE (n = 108, 47.4% vs. n = 933, 24.9%, p < 0.001). There was no difference in the frequency of multifocal tumors between prepubertal and adolescent children (n = 102, 37.2% vs. n = 1628; 35.5%, p = 0.56).
Tumor Pathologic and Treatment Characteristics by Patient Age at Presentation
Data are presented as n (%), or median (IQR). Bolded numbers represent statistically significant p-values.
Prepubertal age group versus adolescent age group.
Prepubertal age group compared to adolescent group and to young adult group.
LVI reported for patients diagnosed 2010–2017.
ETE reported for patients diagnosed 2004–2015.
ETE, extrathyroidal extension; LVI, lymphovascular invasion; NOS, not otherwise specified; RAI, radioactive iodine therapy.
Young adult patients, on the contrary, presented with multifocal tumors more frequently than either pediatric group (n = 39,274; 38.8%, all p < 0.001). Prepubertal patients were much more frequently diagnosed with regional lymph node (n = 184, 67.2% vs. n = 2399; 52.3%, p < 0.001), and distant metastatic (n = 31, 11.3% vs. n = 101, 2.2%, p < 0.001) disease compared to adolescent patients. Conversely, in comparison, 32.1% (n = 32,503) of young adult patients presented with positive regional lymph nodes and 0.5% (n = 520) presented with distant metastases. When a lymphadenectomy was performed, the median number of lymph nodes examined for prepubertal patients was 14 (IQR 2–42) compared to adolescent patients, who had a median of 4 (IQR 1–17) examined (p < 0.001).
Prepubertal children had a higher median number of positive metastases to regional lymph nodes on examination than adolescent patients (8 [IQR 1–18] vs. 2 [IQR 0–9], p < 0.001). The yield of positive lymph nodes was 87% for prepubertal, 78% for adolescent, and 64% for young adult patients. Prepubertal age compared to adolescent age was an independent predictor of both regional lymph node (AOR = 1.36 [95% confidence interval {CI} 1.01–1.84], p = 0.04) and distant metastatic (AOR = 3.12 [CI 1.96–4.96], p < 0.001) disease on multivariable regression modeling (Fig. 1).
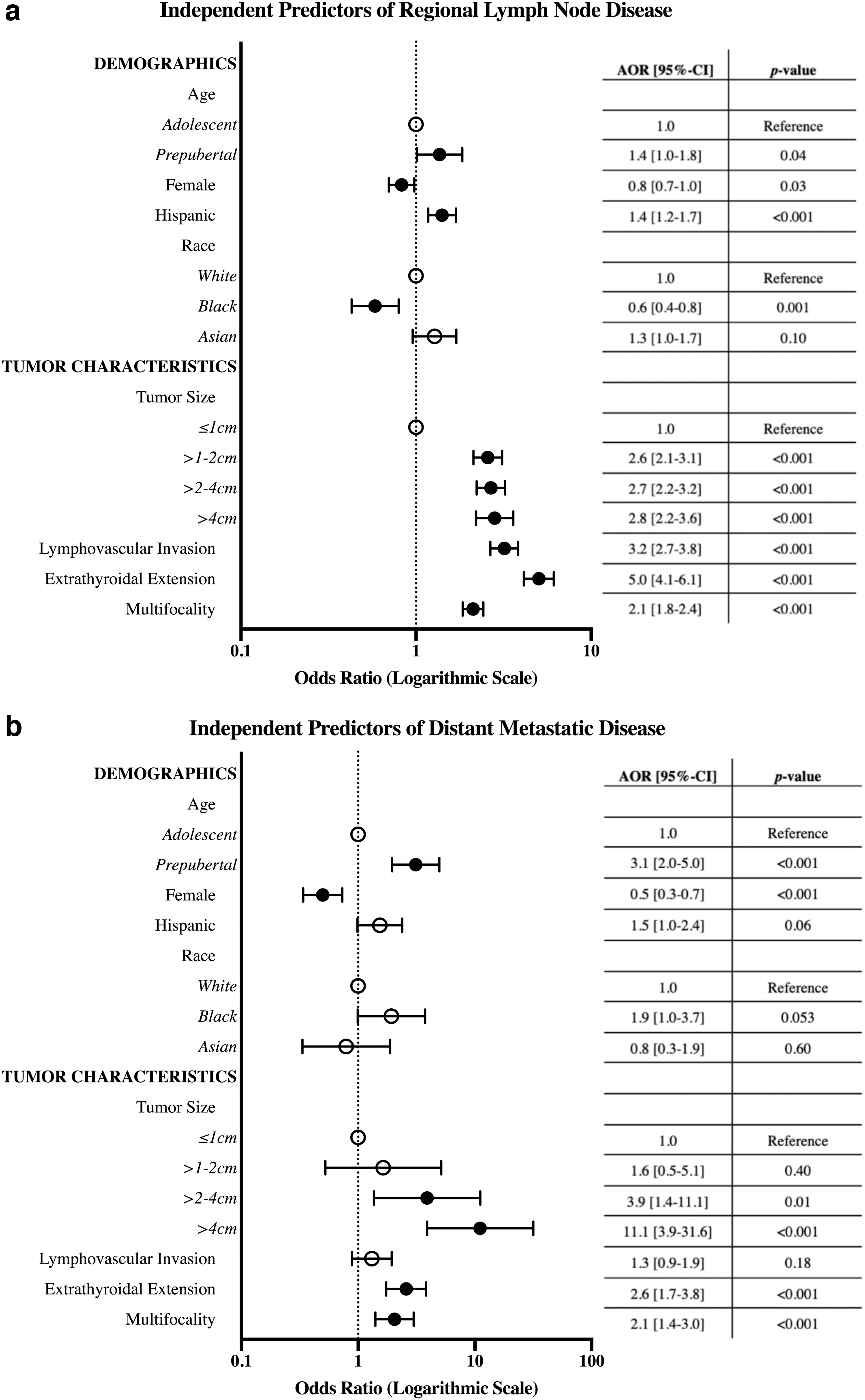
Multivariable logistic regression analysis of independent predictors for regional lymph node metastases (
Pediatric patients underwent more extensive thyroid cancer treatment (Table 2). The majority of pediatric patients underwent total thyroidectomy, in line with current management guidelines, although 7.2% (n = 329) of adolescent patients were managed with hemithyroidectomy, compared to 4.0% (n = 11) of prepubertal children (p = 0.001). A high proportion of young children and adolescents underwent adjuvant radioactive iodine therapy (n = 172, 62.8% vs. n = 2719, 59.3%, p = 0.25). Prepubertal patients less frequently underwent prophylactic lymphadenectomies than adolescent patients (n = 51, 18.6% vs. n = 1377, 30.0%), but more often required therapeutic lymphadenectomies (n = 85, 31.0% vs. n = 901, 19.6%, p < 0.001). Fewer young adult patients required therapeutic lymphadenectomies (n = 11,329, 18.2%, all p < 0.001).
Approximately 63% of patients who underwent a prophylactic lymphadenectomy had lymph node metastases on final pathology, regardless of age at presentation. Nevertheless, overall survival did not differ based on patient age and was high (Fig. 2). Median follow-up was 68.8 months (5.7 years). Five-year survival data were reported for 151 prepubertal, 2454 adolescent, and 53,420 young adult patients. Five-year survival was 99.1% for prepubertal patients, 99.2% for adolescent patients, and 99.1% for young adult patients (all p = 0.32). Median survival-time was not reached for any group.
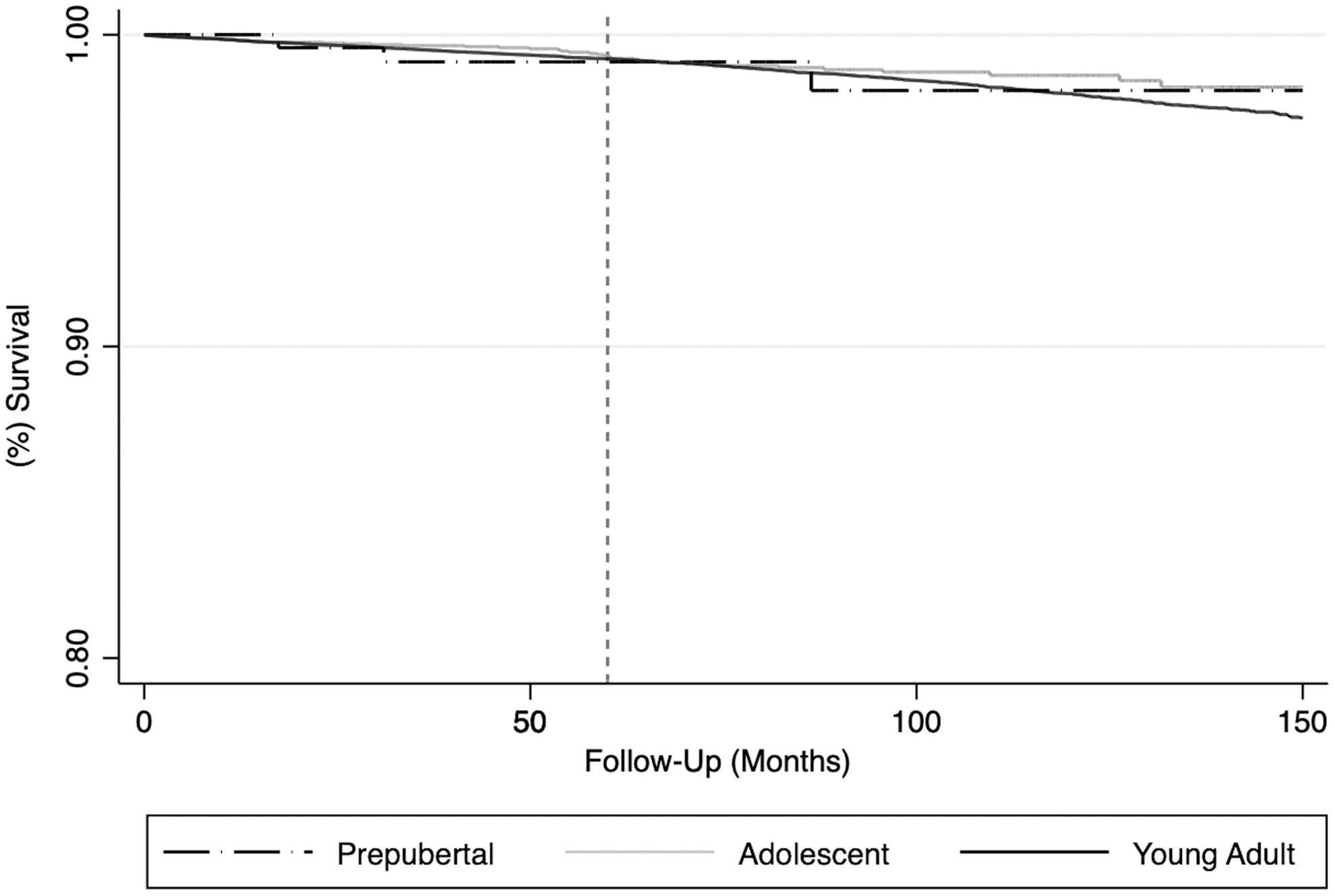
Overall survival in pediatric and young adult papillary thyroid carcinoma patients stratified by age at presentation and represented by Kaplan–Meier curves. y-Axis begins at 75% survival to facilitate discernment. x-Axis denotes survival in months (dashed line at 5 years).
Prepubertal age was associated with more advanced disease even when the cohort was restricted to patients who presented with small primary tumors (≤10 mm) (Table 3). This included 41 prepubertal patients, 937 adolescent patients, and 33,950 young adult patients. Prepubertal compared to adolescent patients still had a higher frequency of gross ETE (n = 6, 20.7% vs. n = 53, 6.7%, p = 0.004), positive regional lymph nodes (n = 21, 51.2% vs. n = 253, 27.0%, p = 0.001), and distant metastases (n = 1, 2.4% vs. n = 3, 0.3%, p = 0.04), although sample size was limited for the latter comparison.
Subgroup Analysis of Tumor and Treatment Characteristics for Patients Diagnosed with Microcarcinomas (≤10 mm) Stratified by Age at Presentation
Data are presented as n (%) or median (IQR). Bolded numbers represent statistically significant p-values.
Prepubertal age group versus adolescent age group.
Prepubertal age group compared to adolescent group and to young adult group.
LVI reported for patients diagnosed 2010–2017.
ETE reported for patients diagnosed 2004–2015.
Prepubertal age at presentation was associated with higher regional lymph node metastatic burden as well, with a higher median number of positive lymph nodes on examination compared to adolescent patients (1 [IQR 0–8.5] vs. 0 [IQR 0–2], p = 0.002). Young adult patients had the highest frequency of multifocal microcarcinomas (n = 11,702, 34.5%) compared to prepubertal (n = 10, 24.4%) and adolescent patients (n = 265, 28.3%) (all p < 0.001). On multivariable regression modeling of the pediatric microcarcinoma cohort, prepubertal age compared to adolescent age remained an independent predictor of regional lymph node metastases (AOR = 2.19 [CI 1.10–4.36], p = 0.03) (Fig. 3).
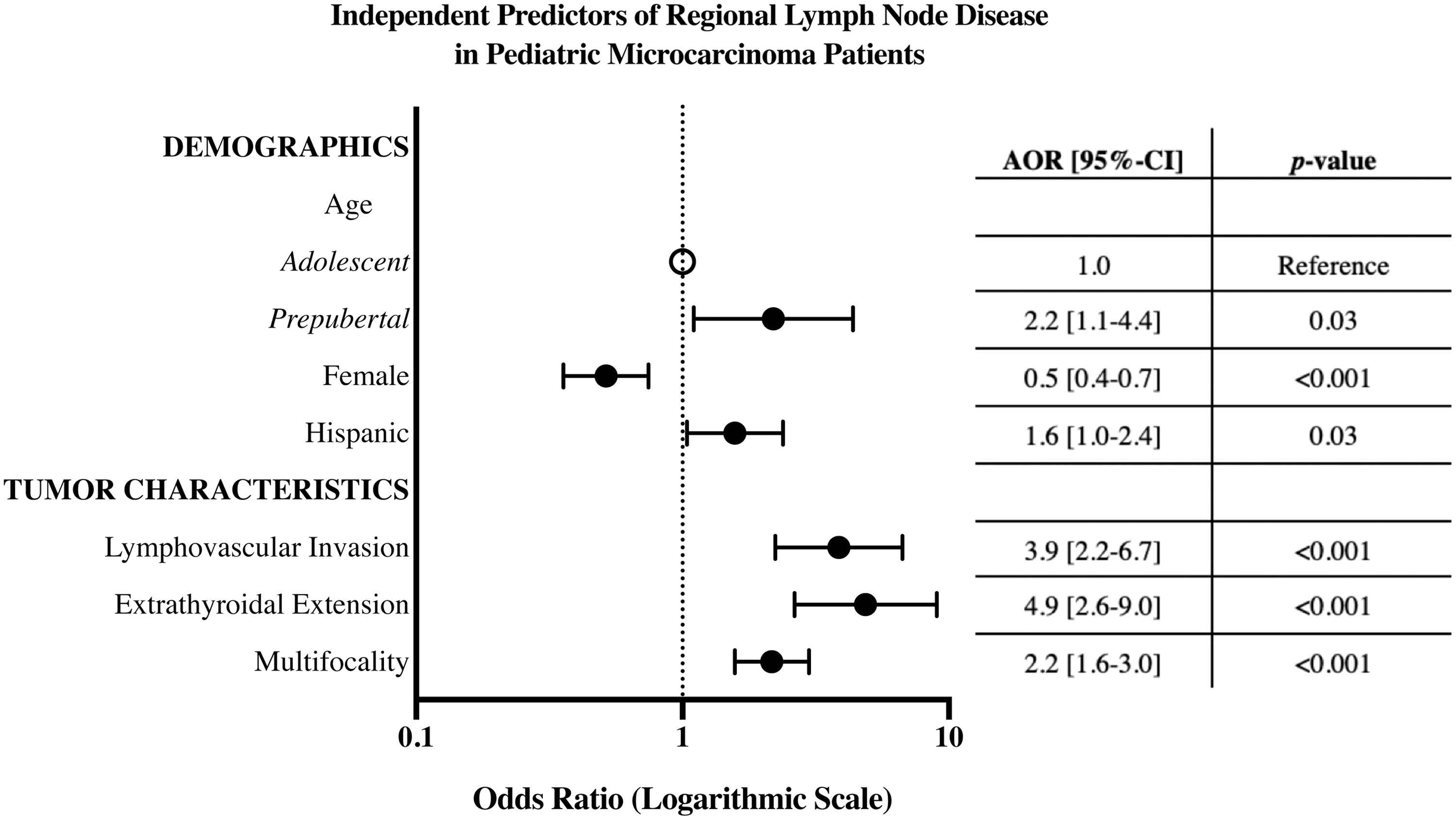
Multivariable logistic regression analysis of independent predictors for regional lymph node metastases in the pediatric microcarcinoma cohort (n = 978). ORs and 95% CIs are indicated. Filled-in circles represent statistically significant values.
Discussion
This analysis of pediatric PTCs is a cohort study that captures ∼70% of all pediatric thyroid cancer diagnoses in the United States and characterizes the association between patient age with respect to onset of puberty and presenting stage of disease. It is the largest study of pediatric PTC since the Belarusian analysis, which found that younger age at diagnosis in patients with a history of ionizing radiation was associated with recurrent nodal disease and pulmonary metastasis. 15 We report a spectrum of disease severity for pediatric PTC, wherein prepubertal children present with the most extensive disease and young adults present most favorably, with adolescents assuming an intermediate profile.
Specifically, prepubertal children are most likely to have lymph node disease, ETE, LVI, and distant metastases at the time of diagnosis, even in the setting of a small primary tumor (≤10 mm). Adolescent children, in turn, present with these disease characteristics more frequently than young adults. On multivariable regression modeling, controlling for potentially confounding factors, prepubertal age compared to adolescent age was found to be an independent predictor of nodal and distant metastatic disease.
Some small, institutional retrospective analyses have reported similar conclusions that younger children generally present with more invasive disease than adolescents, with specific emphasis on higher propensity for distant metastatic disease. 5,21,26 –30 With respect to the influence of extent of disease on patient outcomes, one study found that age as a continuous variable was not related to disease-free survival (DFS) or distant metastasis-free survival (DMFS); yet, children <15 years old had distinct clinical manifestations such as lymph node metastases and ETE, which did predict both DFS and DMFS. 33 The authors concluded that a cutoff age of 14 would be more appropriate for diagnosis of “pediatric” PTC 33 essentially supporting the notion of two distinctive phenotypes currently represented in the <18 years of age cohort.
The more invasive phenotype of PTC observed in prepubertal children compared to adolescents and young adults, especially with regard to its propensity to metastasize distantly, implies differing tumor biology. Molecular studies have shown that point mutations in BRAF and RAS, which are very commonly detected in adult PTCs, are significantly more rare in pediatric tumor specimens. 34 –36 Gene rearrangements involving receptor tyrosine kinases such as RET, NTRK1, NTRK3, and ALK, on the contrary, are highly prevalent in pediatric PTCs, and are associated with more aggressive clinical disease than fusion gene-negative PTCs. 34 –38 One study aimed to explore the molecular mechanisms underlying distant metastatic disease in PTC and found that these same gene fusions (RET, ALK, or NTRK1) are independently associated with metastases on multivariate analysis. 39
Another study of 106 pediatric Korean patients by Lee et al demonstrated that fusion oncogenes were specifically more prevalent in PTC patients aged <10 years old. 40 Our data demonstrate that the female sex preponderance observed in adult PTC patients holds for the adolescent population (82%), but only 65% of prepubertal patients diagnosed with PTC are female (p < 0.001). Future studies should continue to investigate this genomic landscape to ultimately facilitate a precision approach to treatment.
Current management guidelines for pediatric PTC recommend total thyroidectomy for almost all patients, in part, because children are considered to have a higher likelihood of multifocal and bilateral disease than adults. 7,41 We found that young adult PTCs were just as frequently multifocal, even for patients with primary microcarcinomas. Literature suggests that of those patients with multifocal disease, 69% will have bilateral nodules. 20 Another review found that 38.4% of pediatric patients younger than the age of 17 years presented with bilateral disease. 42 As such, they concluded that total thyroidectomy should still be the standard of care for most pediatric PTC patients. 42 Neither of these studies included an adult comparison cohort for contextualization.
Although the frequency of multifocal disease is high based on our data, it is similar to that of young adult patients, who are often safely managed with lobectomy in the appropriate clinical context. Indeed, a few recently published retrospective studies have suggested that lobectomy might be safely considered for some early-stage pediatric PTCs. 43,44 However, given that patients aged <11 years old generally present with the more advanced disease phenotype, even in the setting of T1 tumors, they are likely to continue to require more aggressive management and surveillance.
There are limitations to this study. As a retrospective analysis of the NCDB, it is reliant on accurate coding of patient and treatment variables for reliable analysis. 31 As discussed, bilaterality is not a coded variable. Tumor size was used as a proxy for the clinical T stage of each patient, as this variable was not reliably coded for cases diagnosed before 2008. Moreover, the NCDB does not collect data on DFS or cancer recurrence. Relatedly, median follow-up time for survival was only 6 years, which does not approach median survival time. In addition, facility type data are not collected for pediatric patients, which preclude stratification of treatment with respect to cancer center type.
Significantly, there is no information collected by the NCDB regarding tumor mutational profiles. Multivariable regression modeling for independent predictors of distant metastatic disease was unable to be performed for the microcarcinoma cohort secondary to small sample size. Finally, there is no strict age cutoff for the onset of puberty, and there are developmental differences in the timing of maturation between female and male patients.
Conclusions
Pediatric PTC patients present with more extensive disease than adult PTC patients, but age <11 years old is an independent predictor for high regional disease burden and distant metastases at the time of presentation, even for those with small primary tumors. Pediatric PTCs are no more frequently multifocal than those diagnosed in young adults. Additional research is needed to determine whether adolescent patients may be safely managed less conservatively than younger children with PTCs and to further elucidate the specific molecular derangements that underlie this divergence in presentation.
Footnotes
Authors' Contributions
J.W.T.: Conceptualization, data curation, methodology, formal analysis, writing-original draft, and writing-review and editing. C.E.E. and J.A.G.: Data curation and writing-review and editing. T.B.: Methodology, formal analysis, and writing-review and editing. R.Z.: Supervision and writing-review and editing. T.J.F.: Conceptualization, methodology, supervision, and writing-review and editing. B.M.F.: Conceptualization, methodology, formal analysis, supervision, and writing-review and editing.
Author Disclosure Statement
All authors have no related conflicts of interests to declare and have approved the final article for submission.
Funding Information
There are no external funding sources to report.