
Abstract
Background:
Studies have shown that thyroid autoimmunity (TAI) is associated with increased risks of adverse pregnancy outcomes. The aim of this study was to investigate the associations between TAI and embryo quality in euthyroid women undergoing in vitro fertilization or intracytoplasmic sperm injection (IVF/ICSI).
Methods:
This retrospective cohort study included euthyroid infertile women with and without TAI (defined as a serum thyroperoxidase concentration ≥34 IU/mL or a thyroglobulin concentration ≥115.0 IU/mL) who underwent their first complete IVF/ICSI treatment cycles at a tertiary referral center between April 2016 and February 2022. Embryo quality measurements and clinical outcomes were compared between women with (TAI positive) and without TAI (TAI negative). The high-quality cleavage embryo rate and cumulative live birth rate (cLBR) were the primary outcomes.
Results:
A total of 499 TAI-positive and 2945 TAI-negative women were included in this study, and their mean (standard deviation) ages were 31.6 (4.5) and 30.9 (4.4) years, respectively (p = 0.001). The overall analysis showed no significant differences between TAI-negative and TAI-positive women in the high-quality cleavage embryo rate (n/N: 11,139/22,553 vs. 1971/3820; adjusted rate: 52.8% vs. 53.4%, p = 0.66) and cLBR (1917/2945 vs. 327/499; 53.4% vs. 56.2%, p = 0.31). Moreover, no significant differences were observed between TAI-negative and TAI-positive women in the rates of oocyte retrieval (35,078/51,978 vs. 5853/8628; 69.1% vs. 69.4%; p = 0.65), fertilization (23,067/34,197 vs. 3902/5728; 61.1% vs. 62.2%, p = 0.34), embryo utilization (18,233/22,553 vs. 3156/3820; 80.2% vs. 80.8%, p = 0.61), blastocyst formation (7051/13,721 vs. 1192/2330; 48.5% vs. 48.4%, p = 0.97), and high-quality blastocysts (4819/13,721 vs. 799/2330; 29.9% vs. 29.4%, p = 0.73). Furthermore, no significant differences were observed between TAI-negative and TAI-positive women in the clinical pregnancy rate (1524/2808 vs. 248/482; 46.7% vs. 44.6%, p = 0.40), early pregnancy loss rate (156/1524 vs. 23/248; 13.5% vs. 11.5%, p = 0.44), and LBR (1338/2808 vs. 218/482; 37.4% vs. 36.0%, p = 0.55) of the first transfer cycle.
Conclusions:
This study demonstrated that TAI in women was not associated with embryo quality or the cLBR following IVF/ICSI. Future large studies are warranted to confirm these findings.
Introduction
Thyroid autoimmunity (TAI) refers to the presence of antibodies against thyroperoxidase (TPO-Ab) or thyroglobulin (Tg-Ab). 1 The prevalence of TAI in women of reproductive age has been reported to be 8–18% across different studies. 1 –3 The associations between TAI and pregnancy outcomes have long been investigated, and several meta-analyses have shown increased risks of pregnancy loss and preterm birth in women with TAI. 4 –7 However, recently published population-based studies have not supported any detrimental effects of TAI on pregnancy outcomes following assisted reproductive technology (ART). 8 –11 These results were supported by two recent meta-analyses. 3,12
Moreover, two randomized controlled trials, namely, the TABLET and POSTAL trials, that were published in 2019 13,14 reported no beneficial effects of levothyroxine (LT4) treatment on the clinical pregnancy rate (CPR) or live birth rate (LBR) and no reduction in pregnancy loss in euthyroid women with TAI. Therefore, further studies are warranted to confirm the associations between TAI in women and pregnancy outcomes.
In 2021, the European Thyroid Association Guideline suggested the use of intracytoplasmic sperm injection (ICSI) as the preferred fertilization method to improve the fertilization rate of in vitro fertilization (IVF) treatment in women with TAI, as well as the consideration of LT4 treatment for infertile women with TAI and thyrotropin (TSH) levels >2.5 mIU/L on a case-by-case basis to allow for optimized embryo development. 15 However, this recommendation is based on evidence from only a few small observational studies. In 2011, Monteleone et al conducted a small retrospective study (14 TAI patients and 17 control subjects) that showed a significantly lower fertilization rate (63% vs. 72%) and grade A embryo rate (25% vs. 48%) in TAI patients than in control subjects. 16 A subsequent study of 90 patients with TAI and 676 controls in 2012 also showed significantly lower fertilization rate, implantation rate, and CPR in the TAI group. 17
Subsequently, three other small studies evaluated the effect of TAI on embryo quality, but the results of these studies were inconsistent. 18 –20 These discrepancies may be attributable to differences in the study design, patient selection, or methodological issues. Limited sample sizes prevented the full control of potential confounders in these previous studies; as embryogenesis is a complex process, this may have affected the accuracy of the results. Therefore, studies with larger sample sizes that fully consider confounders are warranted to elucidate the effects of TAI.
In this study, our aim was to evaluate the relationship between TAI and embryo development in a large cohort of infertile female patients who had undergone IVF/ICSI.
Materials and Methods
Study population and design
This was a retrospective cohort study conducted at the First Affiliated Hospital of Kunming Medical University from April 2016 to February 2022. The study protocol was approved by the ethics committee of the hospital (Approval No. 2022L60). Informed consent was waived due to the retrospective study design.
Infertile couples who had received IVF/ICSI treatment during the study period were potentially eligible for inclusion in this study. Patients were included in this study if: (1) their first oocyte retrieval cycle had resulted in at least one live birth after a fresh or consecutive frozen embryo transfer or had failed to result in a live birth after all embryos with autologous sperm and oocytes had been transferred; (2) both the female and male partners had TSH, free triiodothyronine (fT3), and free thyroxine (fT4) concentrations within the normal ranges and had complete TPO-Ab and Tg-Ab data; (3) the female partners were aged 20–40 years; and (4) at least one oocyte had been retrieved in each cycle.
Cycles (couples) were excluded if: (1) the female or male partner had received LT4 supplementation before or during ovarian stimulation; (2) the female or male partner had a chromosomal abnormality; (3) the female partner had been diagnosed with endometriosis or a uterine abnormality; (4) pregnancy loss had occurred ≥2 times; (5) cycles had been performed with frozen sperm or sperm from testicular/epididymal aspiration; or (6) the female partner had another immune disorder, such as systemic lupus erythematosus, rheumatoid arthritis, or Sjögren's syndrome. Only the first oocyte retrieval cycle was included in this study. The patients' demographic and clinical information and treatment details were recorded in an ART database, as described in our previous studies. 2,21
Thyroid function and anti-Mullerian hormone measurement
Patients were tested for thyroid function before the initiation of IVF/ICSI treatment. Thyroid functional parameters, including the serum TSH, fT3, fT4, TPO-Ab, and Tg-Ab concentrations, were measured by chemiluminescent immunoassay using a Cobas analyzer (E601) provided by Roche Diagnostics GmbH (Mannheim, Germany), as previously described. 2 Patients with TPO-Ab concentrations ≥34 IU/mL or Tg-Ab concentrations ≥115.0 IU/mL were diagnosed with TAI. 2 Serum anti-Mullerian hormone (AMH) concentrations were measured using an enzyme-linked immunosorbent assay kit with a sensitivity of 0.06 ng/mL (Kangrun Biotech, Guangzhou, China) as previously described. 2 The reference ranges and intra-/interassay coefficients of variation of thyroid function parameters and AMH are reported in Methods Supplement 1.
Ovarian stimulation, fertilization, embryo culture, and embryo transfer
The processes of ovarian stimulation, follicle monitoring, oocyte retrieval, and fertilization are described in Methods Supplement 2. Cleavage embryo morphology was evaluated on day 3 following fertilization and graded as I to IV depending on the number, size, and shape of the blastomeres and the degree of fragmentation. 21 The blastocysts were scored on days 5–6 using the Gardner and Schoolcraft morphological criteria 22 ; blastocysts with grades higher than 4BB were categorized as high quality. One or two fresh or frozen embryos were transferred per cycle, depending on the patient's condition.
Outcome measures
The primary outcomes in this study were the high-quality cleavage embryo rate and the cumulative live birth rate (cLBR). The secondary outcomes were the rates of oocyte retrieval, fertilization, embryo utilization, blastocyst formation, and good-quality blastocysts, and the clinical outcomes of the first transfer cycles. The oocyte retrieval rate was defined as the ratio of the total number of oocytes retrieved to the number of follicles punctured (≥10 mm in diameter) on the day of oocyte retrieval. 23 The fertilization rate was calculated as the number of normally fertilized oocytes (two pronuclei) divided by the number of oocytes used for insemination (IVF cycle) or injection (ICSI cycle). 21 The embryo utilization rate was defined as the number of grade I–III embryos divided by the total number of embryos evaluated on day 3 after fertilization.
The high-quality cleavage embryo rate was calculated as the percentage of grade I–II embryos among all of the embryos evaluated on day 3. 21,24 The blastocyst formation rate was defined as the number of embryos that reached the blastocyst stage on day 5/6 divided by the number of two pronuclei embryos subjected to blastocyst culture. 25,26 The high-quality blastocyst rate was calculated as the number of blastocysts rated as grade 4BB or higher divided by the total number of embryos that underwent blastocyst culture. 26 The CPR was calculated as the number of cycles with the presence of at least one gestational sac on ultrasound, divided by the number of transfer cycles. Early pregnancy loss was defined as a spontaneous miscarriage that occurred before 12 weeks of gestation.
A live birth was defined as a live-born baby after 28 weeks of gestation. 21,26 The cLBR was calculated as the number of oocyte retrieval cycles resulting in at least one live birth in fresh or subsequent frozen embryo transfer cycles, divided by the number of oocyte retrieval cycles. If multiple live births were achieved in one oocyte retrieval cycle, only the first live birth was included in the analysis. 27
Data analysis
Data are presented as the mean (standard deviation [SD]) when normally distributed, or as the median (interquartile range) otherwise. Demographic and clinical data were compared between TAI-negative and TAI-positive women using Student's t-test, the Mann–Whitney U test, or the chi-square test, as appropriate.
The effects of female TAI on embryo quality measurements and clinical outcomes were analyzed using generalized linear models, with an identity link function for the analysis of continuous outcomes and a logistic link function for the analysis of binomially distributed measurements. 25,28 The models were adjusted for female age, body mass index (BMI), TSH, and AMH concentrations, primary or secondary infertility, infertility diagnosis, ovarian stimulation protocols, and the year of oocyte retrieval when analyzing the oocyte retrieval rate. The models were further adjusted for male age, male BMI, and the type of fertilization (IVF or ICSI) when analyzing laboratory outcomes and the cLBR. The models were additionally adjusted for the type of embryo transfer (fresh or frozen), stage of the embryo at transfer (cleavage or blastocyst), and the number of transferred embryos when analyzing the clinical outcomes of the first transfer cycle (CPR, early pregnancy loss rate [ePLR], and LBR).
To explore whether the effect of TAI on embryo quality and clinical outcomes differed according to patient age, TSH concentration, TAI subtype, and IVF or ICSI treatment, subgroup analyses of cycles were performed according to female age (<35 or ≥35 years), 2 TSH concentration (<2.5 or ≥2.5 mIU/L), TPO-Ab/Tg-Ab status (TPO-Ab[−]/Tg-Ab[−], TPO-Ab[+]/Tg-Ab[−], TPO-Ab[−]/Tg-Ab[+], or TPO-Ab[+]/Tg-Ab[+]), and treatment cycle (IVF or ICSI).
Data analysis was performed using SPSS 25.0 (SPSS, Inc., Chicago, IL). All tests were two-tailed, and p < 0.05 was considered to indicate statistical significance.
A post hoc power calculation was performed for the cLBR. Detailed information about the power calculation is provided in Methods Supplement 3.
Results
Of the 6239 couples who completed their first oocyte retrieval cycle, 3444 cycles (2945 were TAI negative and 499 were TAI positive) met the inclusion criteria and were included in the final analysis, representing 1917 live births in the TAI-negative group and 327 live births in the TAI-positive group, as presented in Figure 1. The mean ages of the TAI-positive and TAI-negative women were 31.6 (SD 4.5) and 30.9 (SD 4.4) years, respectively (p = 0.001). TAI-positive women had significantly higher TSH concentrations than TAI-negative women (median: 2.40 mIU/L vs. 2.21 mIU/L, p = 0.005). Other demographic and clinical characteristics were not significantly different between the two groups (all p > 0.05, Table 1).
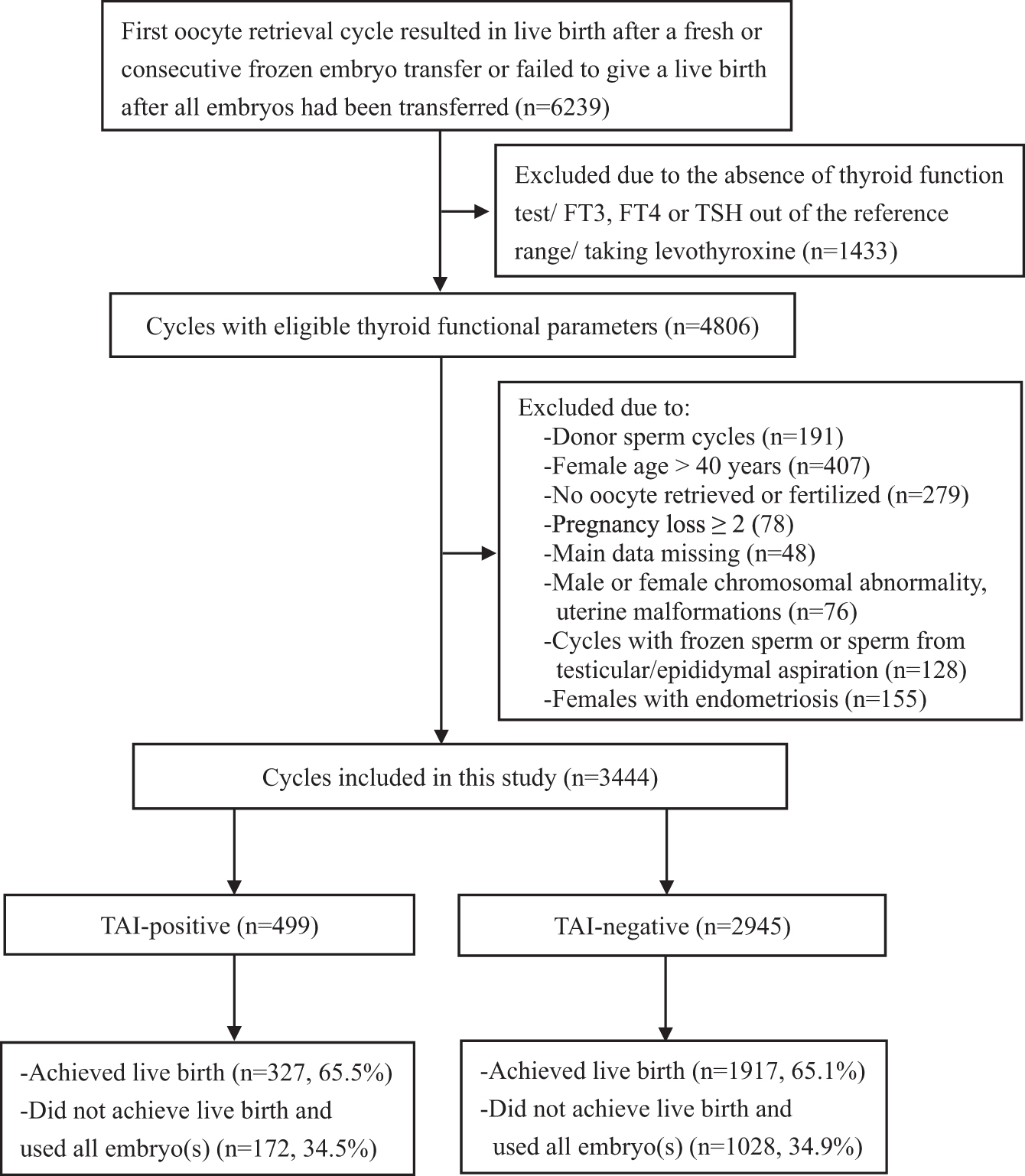
Flowchart of the participant selection in this study. TAI positive is defined as a serum thyroperoxidase concentration ≥34 IU/mL or a thyroglobulin concentration ≥115.0 IU/mL. TAI negative is defined as a serum thyroperoxidase concentration <34 IU/mL and a thyroglobulin concentration <115.0 IU/mL. TAI, thyroid autoimmunity.
Characteristics of the Included Participants
p-Value in bold represents significant difference.
AMH, anti-Mullerian hormone; BMI, body mass index; fT3, free triiodothyronine; fT4, free thyroxine; ICSI, intracytoplasmic sperm injection; IQR, interquartile range; IVF, in vitro fertilization; SD, standard deviation; TAI, thyroid autoimmunity; TSH, thyrotropin.
The overall analysis showed that the high-quality cleavage embryo rate (n/N: 11,139/22,553 vs. 1971/3820; adjusted rate [confidence interval]: 52.8% [49.3 to 56.2] vs. 53.4% [49.2 to 57.6], p = 0.66) and cLBR (1917/2945 vs. 327/499; 53.4% [49.0 to 57.8] vs. 56.2% [49.9 to 62.3], p = 0.31) were not significantly different between TAI-negative and TAI-positive women. Similarly, the rates of oocyte retrieval (35,078/51,978 vs. 5853/8628; 69.1% [67.4 to 70.7] vs. 69.4% [67.3 to 71.5], p = 0.65), fertilization (23,067/34,197 vs. 3902/5728; 61.1% [58.7 to 63.6] vs. 62.2% [59.1 to 65.3], p = 0.34), embryo utilization (18,233/22,553 vs. 3156/3820; 80.2% [77.5 to 82.8] vs. 80.8% [77.5 to 84.0], p = 0.61), blastocyst formation (7051/13,721 vs. 1192/2330; 48.5% [43.1 to 54.0] vs. 48.4% [42.3 to 54.6], p = 0.97), and high-quality blastocysts (4819/13,721 vs. 799/2330; 29.9% [25.0 to 34.8] vs. 29.4% [23.9 to 34.9], p = 0.73) were not also significantly different between TAI-negative and TAI-positive women.
Furthermore, no significant differences were observed in the CPR (1524/2808 vs. 248/482; 46.7% [41.9 to 51.6] vs. 44.6% [38.3 to 51.0], p = 0.40), ePLR (156/1524 vs. 23/248; 13.5% [9.3 to 19.2] vs. 11.5% [6.8 to 18.8], p = 0.44), and LBR (1338/2808 vs. 218/482; 37.4% [32.8 to 42.3] vs. 36.0% [30.2 to 42.3], p = 0.55) of the first embryo transfer cycle between the TAI-negative and TAI-positive groups (Table 2).
Associations Between Thyroid Autoimmunity and In Vitro Fertilization/Intracytoplasmic Sperm Injection Outcomes
Oocytes or embryos or pregnancies were pooled in each group for calculation.
Rates were calculated individually for each cycle. Generalized linear regression models were used for the data analysis. The models were adjusted for female age, BMI, TSH, and AMH concentrations, primary or secondary infertility, infertility diagnosis, ovarian stimulation protocols, and the year of oocyte retrieval when analyzing the oocyte retrieval rate. The models were further adjusted for male age, male BMI, and the type of fertilization when analyzing laboratory outcomes and the cLBR. The models were additionally adjusted for fresh or frozen embryo transfer, the stage of the embryo transfer, and the number of transferred embryos when analyzing the clinical outcomes of the first transfer cycle.
CI, confidence interval; cLBR, cumulative live birth rate; CPR, clinical pregnancy rate; ePLR, early pregnancy loss rate; LBR, live birth rate.
In the subgroup of women aged <35 years, 2286 and 361 cycles were characterized as TAI negative and TAI positive, respectively. In the subgroup of females aged ≥35 years, 659 and 138 cycles were characterized as TAI negative and TAI positive, respectively. None of the embryo quality measurements or the clinical outcomes was significantly different between TAI-negative and TAI-positive women in both age subgroups (all p > 0.05), as shown in Table 3. In the subgroup of women with TSH concentrations <2.5 mIU/L, 1809 and 263 cycles were characterized as TAI negative and TAI positive, respectively. In the subgroup of women with TSH concentrations ≥2.5 mIU/L, 1136 and 236 cycles were characterized as TAI negative and TAI positive, respectively. After adjustment for confounders, no significant differences in embryo quality measurements and clinical outcomes were observed between women with and without TAI (all p > 0.05) in both the TSH <2.5 and ≥2.5 mIU/L subgroups, as shown in Table 4.
Associations Between Thyroid Autoimmunity and Embryo Quality in Different Female Ages
Data were presented as adjusted rate [CI]. Generalized linear regression models were used for the data analysis. The models were adjusted for female age, BMI, TSH, and AMH concentrations, primary or secondary infertility, infertility diagnosis, ovarian stimulation protocols, and the year of oocyte retrieval when analyzing the oocyte retrieval rate. The models were further adjusted for male age, male BMI, and the type of fertilization when analyzing laboratory outcomes and the cLBR. The models were additionally adjusted for fresh or frozen embryo transfer, the stage of the embryo transfer, and the number of transferred embryos when analyzing the clinical outcomes of the first transfer cycle.
Associations Between Thyroid Autoimmunity and Embryo Quality at Different Thyrotropin Concentrations
Data were presented as adjusted rate [CI]. Generalized linear regression models were used for the data analysis. The models were adjusted for female age, BMI, TSH, and AMH concentrations, primary or secondary infertility, infertility diagnosis, ovarian stimulation protocols, and the year of oocyte retrieval when analyzing the oocyte retrieval rate. The models were further adjusted for male age, male BMI, and the type of fertilization when analyzing laboratory outcomes and the cLBR. The models were additionally adjusted for fresh or frozen embryo transfer, the stage of the embryo transfer, and the number of transferred embryos when analyzing the clinical outcomes of the first transfer cycle.
In addition, no differences in these outcomes were observed between women with TAI negativity, isolated TPO-Ab positivity, isolated Tg-Ab positivity, or combined TPO-Ab and Tg-Ab positivity (all p > 0.05, Supplementary Table S1). The embryo quality measurements and clinical outcomes were also not significantly different between TAI-positive and TAI-negative women in both the IVF and ICSI treatment subgroups (all p > 0.05, Supplementary Table S2).
Discussion
In this study, we found no significant differences between TAI-positive and TAI-negative euthyroid women in terms of fertilization rates, embryo quality, and cLBR following IVF/ICSI. These results suggest that female TAI does not affect the oocyte or embryo quality or the corresponding pregnancy outcomes.
TAI may reflect a decrease in thyroid functional capacity that becomes apparent during states of increased demand for thyroid hormone synthesis, such as early pregnancy. 29 TAI may also be considered a manifestation of general autoimmunity, and it may be complicated by connective tissue diseases. 30,31 As early as 2009, a TAI-positive mouse model-based study showed that TPO-Ab bound to preimplantation embryos, affected postimplantation embryo development, and eventually led to fetal loss and reduced litter size. 32 This finding raised the question of whether TPO-Ab and Tg-Ab are present in human follicles and can affect folliculogenesis. In 2017, Monteleone et al reported for the first time that TPO is present in the cytoplasm of human granulosa cells, indicating that the human ovarian follicle may independently produce thyroid hormones. 33
Another two studies demonstrated the existence of TPO-Ab and Tg-Ab in human follicular fluid and that their concentrations in follicular fluid are positively associated with their concentrations in serum. 16,34 The authors hypothesized that these antibodies may disrupt the function of TPO, generate an inflammatory response, and alter the milieu of the maturing oocyte. 35 This hypothesis was supported by other studies that reported lower fertilization and high-quality embryo rates in women with TAI than in women without TAI. 16,18,19 However, these results were inconsistent with those of two recent cohort studies that showed no significant association between TAI and the fertilization rate or embryo quality. 11,20 The results of the current study indicate that female TAI has no significant effect on embryo quality or pregnancy outcomes, as measured by the cLBR. Our findings are in agreement with a previous study that also reported no differences in the cLBR between women with and without TAI. 8
We used the cLBR per oocyte retrieval to evaluate the effect of TAI on pregnancy outcomes, as this variable may better reflect the effect of TAI on embryos. Our results did not support a detrimental effect of TAI on pregnancy outcomes after IVF/ICSI, which is consistent with the findings of previous studies showing similar pregnancy, miscarriage, and LBRs in couples undergoing intrauterine insemination 9 or IVF/ICSI. 35 However, our results were in contrast to those of a meta-analysis published in 2016, which showed a 35% decrease in the LBR (309 women with TAI) and a 1.44-fold increase in the miscarriage rate (330 women with TAI) in women with TAI relative to women without TAI. 5 These discrepancies may be attributable to differences in the sample size and patient characteristics between studies or to the increasingly widespread use of ICSI in recent studies.
In the current study, we excluded patients with recurrent pregnancy loss (≥2 times), as such patients have been reported to be more susceptible to TAI. Two studies focusing on patients with unexplained recurrent pregnancy loss showed that TPO-Ab positivity was associated with a significantly lower LBR than TPO-Ab negativity and that TPO-Ab-positive women with LT4 supplementation had a similar LBR to TPO-Ab-negative women, 36,37 demonstrating that TAI plays a critical role in recurrent pregnancy loss that may be attenuated by LT4 treatment. Therefore, TAI may contribute to the etiology of unexplained recurrent pregnancy loss, but it may not be associated with the outcomes of the general population of patients with infertility following IVF/ICSI.
This study has several strengths. First, it is a large cohort study on the effect of TAI on embryo quality. It is also the first study to investigate the association between TAI and the cLBR, defined as the rate of live births per oocyte retrieval cycle, which is a comprehensive and objective index that reflects the oocyte and embryo quality in a specific oocyte retrieval cycle. Second, as the study was conducted in a single center, fertilization, embryo culture, and embryo grading were performed under the same conditions, which minimized variability.
However, this study also has some limitations. The first limitation is the retrospective design. The second limitation is the use of manufacturer-recommended reference ranges for the thyroid function parameters, as region-specific reference ranges were not available. As the third limitation, type II errors could not be excluded because the subgroup analyses were performed with relatively small sample sizes. In addition, we did not perform a stratified analysis based on infertility diagnosis because the sample size was not sufficiently large. However, this variable may be important, as TAI itself has been reported to contribute to the etiology of infertility. For example, TAI is more prevalent in women with polycystic ovary syndrome, 38 primary ovarian insufficiency, 39,40 and idiopathic infertility 41 than in their healthy counterparts.
In conclusion, we observed no association of female TAI with embryo quality or the cLBR in couples who underwent IVF/ICSI treatment. These findings need to be confirmed in large prospective studies.
Footnotes
Acknowledgments
We thank Dr. Qingyan Peng (from the first affiliated hospital of Kunming Medical university) for her guidance and help with statistical analysis. We thank all of the patients who participated in our study. We acknowledge the professional article editing services of Armstrong–Hilton Ltd. AsiaEdit (asiaedit.com).
Data Availability
Some or all data sets generated and/or analyzed during the current study are not publicly available, but are available from the corresponding author on reasonable request.
Authors' Contributions
M.R., S.Z., and L.T. designed the study. Q.Z., C.S., and Z.Y. collected the data. M.R., Z.Z., and Q.Z. performed the data analysis and wrote the article. Z.Z. contributed to the interpretation of the results. All authors contributed intellectually to revising the article and approved the final version.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This study was supported by Joint Funding from the Science & Technology Department of Yunnan Province and Kunming Medical University (2019FE001-142), the Basic Research Project of the Yunnan Province-Outstanding Youth Foundation (No. 202101AW070018), and the “1000 Talent Plan” of Yunnan Province (No. RLQN20200001).
Supplementary Material
Methods Supplement 1
Methods Supplement 2
Methods Supplement 3
Supplementary Table S1
Supplementary Table S2