
Abstract
Background:
Operations for pediatric thyroid nodules are more complicated, and usually lead to longer scars, which may impair life quality in the long term. Bilateral axillo-breast approach robotic thyroidectomy (BABA RT) may provide a better alternative to conventional open thyroidectomy (COT) for pediatric thyroid nodules. Our study aimed at comparing the surgical and oncological outcomes of BABA RT and COT in pediatric patients.
Methods:
The data of 49 pediatric patients who consecutively underwent BABA RT or COT (20:29) between July 1998 and November 2021 in our center were retrospectively analyzed, including demographics, surgery extent, surgical outcomes, pathological characteristics, and oncological outcomes.
Results:
All BABA RT procedures were completed successfully without conversion to open operation. The BABA RT group consisted of 5 benign and 15 malignant cases, while the COT group consisted of 19 benign and 10 malignant cases. The operation time, drain removal time, and number of lymph nodes harvested by central lymph node dissection or lateral lymph node dissection were equivalent in the BABA RT and COT groups. Notably, the postoperative hospital stay of the BABA RT group was shorter than that of the COT group (8.5 [interquartile ranges (IQRs): 3] vs. 11 [IQR: 8] days, p = 0.008). The aesthetic score of the BABA RT group was much higher than that of the COT group (9 [IQR: 1] vs. 6 [IQR: 1], p < 0.001). There was no significant difference between the BABA RT and COT groups in hypoparathyroidism rate (transient, 5 vs. 4; permanent, 1 vs. 0). There was one case of chyle leakage in the COT group and no other complications in any group, such as recurrent laryngeal nerve injury. With a median follow-up of 101 (IQR: 189) months, one case of local relapse and one case of pulmonary metastasis in the COT group were documented.
Conclusion:
In the hands of experienced surgeons, robotic BABA thyroidectomy can be a safe and effective option for both benign and malignant thyroid nodules in children, including those with lymph node metastasis. Robotic BABA thyroidectomy can offer a better and faster postoperative course and a much better cosmetic result, which is crucial for pediatric thyroid patients.
Introduction
Thyroid nodules incidence is much lower in children than in adults. In contrast, the malignancy rate of thyroid nodules diagnosed in children is much higher (22–26% vs. 5–10%), and the morbidity of pediatric thyroid cancer has been increasing rapidly in recent decades. 1,2 Accounting for more than 90% of pediatric thyroid cancer, papillary thyroid cancer (PTC) in children and adolescents is likely to have more regional lymph node involvement, extrathyroidal extension (ETE), pulmonary metastasis, and a higher risk of recurrence. 3 –7
Thus, thyroidectomy for children is usually more complicated because of the dissection of larger tumors and more central and lateral lymph nodes. As a concern of many patients, conventional open thyroidectomy (COT) leaves a permanent cervical scar that indicates privacy of surgery history and may lead to deficiency in employment in special fields, decrease the quality of life, and even cause depression. 8 –10 Moreover, the scar is even longer in children who undergo lateral lymph node dissection (LND).
Many innovative surgery methods have been made to diminish or conceal the surgical scar for children, such as minimally invasive video-assisted thyroidectomy (MIVAT), 11 –13 endoscopic or robotic thyroidectomy through axillary, 14,15 retroauricular, 14 or transoral approaches 16,17 (Table 1). However, since the American Thyroid Association (ATA) guidelines recommend a more aggressive operation for children and adolescents with PTC, all these surgical approaches have limited indications.
Innovative Methods of Thyroidectomy in Pediatric Patients
CND, central neck dissection; MIVAT, minimally invasive video-assisted thyroidectomy; MRND, modified radical neck dissection; RA, retroauricular approach; TAA, transaxillary approach; TOETVA, transoral endoscopic thyroidectomy via the vestibular approach; TT, total thyroidectomy.
Robotic bilateral axillo-breast approach (BABA) thyroidectomy is eligible to dissect bilateral glandular lobes and lymph nodes with covert incisions. It is, thus, more qualified to perform total thyroidectomy (TT) and bilateral central or lateral cervical lymph node dissection. 18,19 Based on the vast experience of robotic BABA thyroidectomy in adults in our center, we performed BABA robotic thyroidectomy for children with thyroid nodules, 50.0% of whom underwent TT with central lymph node dissection (CND) and LND. In this study, we first analyzed the surgical outcomes of BABA robotic thyroidectomy (BABA RT) and COT in children retrospectively.
Materials and Methods
Patients
Forty-nine patients younger than the age of 18 who consecutively underwent thyroidectomy in the 960th Hospital of the Chinese People's Liberation Army were retrospectively analyzed in our study. The study flowchart is shown in Figure 1. Twenty-nine patients underwent COT from July 1998 to November 2021, and 20 underwent BABA RT from January 2014 to November 2021.

Study flow chart.
Neck ultrasound (US) and fine-needle aspiration (FNA) under US guidance were conducted to assess thyroid nodules and cervical lymph nodes, as well as computed tomography if necessary. For the subset of children who had been diagnosed with PTC with FNA preoperatively or frozen section pathology during surgery, TT with ipsilateral prophylactic CND was routinely recommended. 20 For PTC cases with suspicious lymph nodes in the lateral neck by US, FNA and thyroglobulin measurements of FNA washout were performed to confirm metastasis. Once confirmed, therapeutic LND of levels Ⅱ, Ⅲ, and Ⅳ was recommended. The contraindications of BABA RT were as reported in our previous study. 21
The study was approved by the medical ethics review committee of our hospital (no. 20190606). Before surgery, all patients and their parents were informed of the possible therapeutic options for their thyroid nodules or cancers, including both advantages and disadvantages of COT and BABA RT. Based on their preference, the parents of the patients signed informed consent for surgery after deliberation with the patients.
Surgical technique
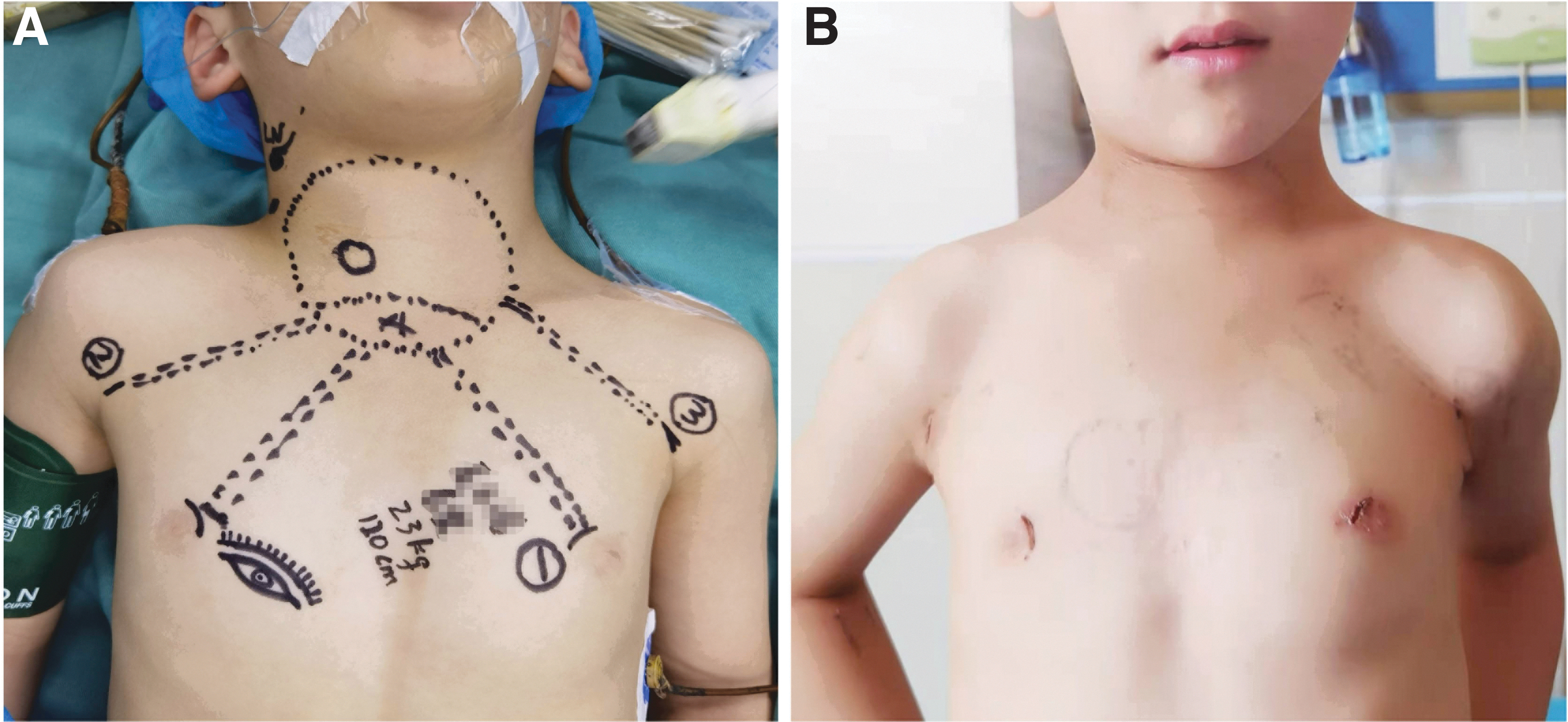
After receiving general anesthesia, the patient was placed in a supine position with the neck slightly extended. Two incisions in the bilateral peri-areolars and another two in the bilateral axillary creases were made to insert the trocars (Fig. 2A). Thyroidectomy and lymph node dissection (Fig. 3) were performed similarly to the COT that has been reported in our previous study. 21
Robotic thyroidectomy using the BABA for a 6-year-old boy. (
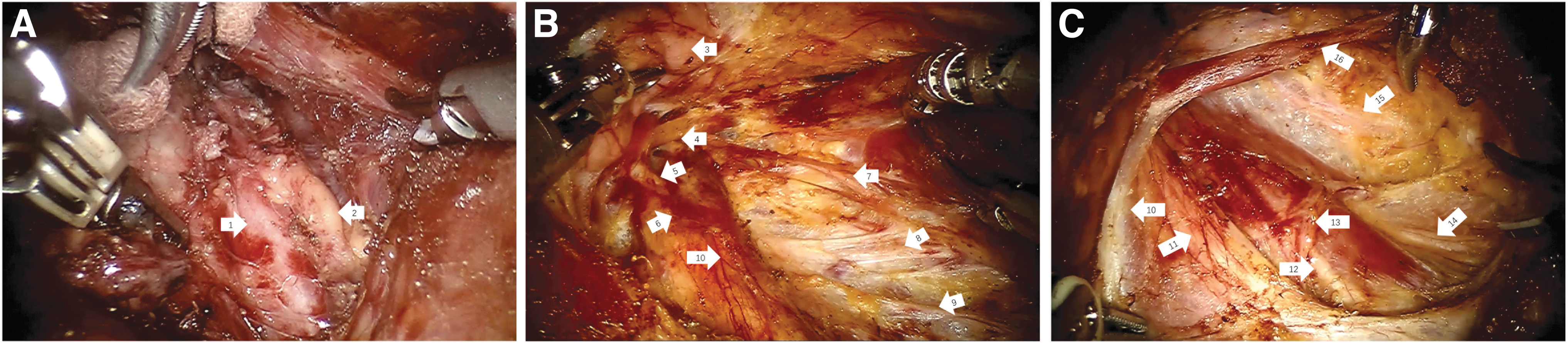
Pediatric robotic thyroidectomy and lateral neck dissection using the BABA. (
Clinical data collection
The following clinical parameters were collected and analyzed: clinical characteristics, operation type, operation time, drain removal time, days of postoperative hospital stay, aesthetic score, pathological characteristics, complications, follow-up time, recurrence, and metastasis.
Postoperative follow-up
Follow-up information was collected through outpatient consultation or telephone inquiry. Parathyroid hormone (PTH) and serum calcium were routinely tested 1 day after surgery for patients who had undergone TT. After surgery, transient hypoparathyroidism was diagnosed if PTH had been <15 ng/mL (normal range 15–65 ng/mL) and/or serum calcium had been under 2.35 mmol/L (normal range 2.35–2.75 mmol/L). If PTH and/or serum calcium remained low for more than 6 months, permanent hypoparathyroidism was diagnosed.
The RLN function was assessed for all patients by a visual laryngoscope before surgery. If hoarseness occurred after thyroidectomy and vocal cord palsy was confirmed by a visual laryngoscope, RLN injury was diagnosed. If the phonation abnormality relieved in 6 months, transient RLN injury was documented. Otherwise, permanent RLN injury was documented. The postoperative aesthetic effect was evaluated in June 2022 by the Visual Analog Scale, with a score of 0–10. As two patients diagnosed with benign nodules were lost to follow-up, the aesthetic score results obtained by the latest valid follow-up were used.
Statistical analysis
If continuous quantitative variables conformed to a normal distribution, they were expressed as the mean ± standard deviation, and a t test was used for their contrast. Otherwise, they were expressed as medians with interquartile ranges (IQRs), and the Mann–Whitney U test was used. Categorical variables were compared by Fisher's exact or chi-square test according to sample size. The difference was considered statistically significant when p < 0.05. Statistical analyses were performed using Statistical Product and Service Solutions (SPSS) software version 26.0 (IBM Corp., Armonk, NY).
Results
Demographics and clinical characteristics
Among the 49 pediatric patients (11 males and 38 females; sex ratio 1:3.45) younger than 18 years, 20 received BABA RT, while 29 received COT. All surgeries were completed successfully without conversion to other approaches. The mean age was 15.13 ± 3.08 years (range, 6–18), and the average body mass index (BMI) was 21.46 ± 5.06 kg/m2 (range, 14.48–37.12). The sex ratio, age, and BMI were equivalent between the BABA RT and COT groups.
There was no history of radiation exposure in either group. Among the 20 patients in the BABA RT group, 15 were diagnosed with PTC (75.0%), and 5 were diagnosed with benign tumors (25.0%), including 3 adenomas and 2 multinodular goiters. Among the 29 patients in the COT group, 10 were diagnosed with PTC (34.5%), and 19 were diagnosed with benign tumors (65.5%), including 7 adenomas and 12 multinodular goiters. The demographics and clinical characteristics of the two groups are presented in Table 2.
Demographics and Clinical Characteristics of the Bilateral Axillo-Breast Approach Robotic Thyroidectomy and Conventional Open Thyroidectomy Groups
BABA RT, bilateral axillo-breast approach robotic thyroidectomy; BMI, body mass index; CI, 95% confidence interval; COT, conventional open thyroidectomy.
Surgical extent and outcomes
The surgical extent and outcomes of the two groups are shown in Table 3. For patients who were diagnosed with benign nodules, 4 (80.0%) and 1 (20.0%) patients in the BABA RT group and 16 (84.2%) and 3 (15.8%) in the COT group underwent lobectomy and TT, respectively (p = 1.000). For patients who were diagnosed with PTC, 1 (6.7%) received lobectomy with ipsilateral CND, 1 (6.7%) received TT, 3 (20.0%) received TT with CND, and 10 (66.7%) received TT with CND and LND in the BABA RT group. In comparison, 1 (10.0%) received lobectomy with ipsilateral CND, 1 (10.0%) received lobectomy with ipsilateral CND and LND, 2 (20.0%) received TT with CND, and 6 (60.0%) received TT with CND and LND in the COT group.
Comparisons of Surgical Extent and Outcomes Between the Bilateral Axillo-Breast Approach Robotic Thyroidectomy and Conventional Open Thyroidectomy Groups
CND, central lymph node dissection; IQR, interquartile range; LND, lateral lymph node dissection; RLN, recurrent laryngeal nerve.
The operation times of the BABA RT and COT groups were equivalent [217.5 (IQR: 129.25 [95% confidence interval (CI): 174.34–254.66]) vs. 175 (IQR: 185.5 [CI: 169.03–260.35]) minutes, p = 0.946]. The median drain removal time of the two groups [5 (IQR: 2 [CI: 4.58–5.52]) vs. 5 (IQR: 3 [CI: 4.03–5.28]) days, p = 0.423] did not show any significant difference. The postoperative hospital stay was significantly shorter in the BABA RT group than in the COT group [8.50 (IQR: 3 [CI: 7.74–9.96]) vs. 11.00 (IQR: 8 [CI: 11.01–17.82]) days, p = 0.008].
Moreover, the postoperative aesthetic score of the BABA RT group was significantly higher than that of the COT group [9 (IQR: 1 [CI: 8.48–8.92]) vs. 6 (IQR: 1 [CI: 6.07–6.82]), p < 0.001] (Figs. 2B and 4).

Picture of skin incision from COT on the postoperative 8-year follow-up. COT, conventional open thyroidectomy.
Complications occurred in 6 (30.0% [CI: 8.0–52.0%]) and 5 (17.2% [CI: 2.6–31.9%]) cases in the BABA RT and COT groups (p = 0.293), including 5 (25.0% [CI: 4.2–45.8%]) and 4 (13.8% [CI: 3.9–311.7%]) transient hypoparathyroidisms, respectively, in the BABA RT and COT groups. One (5.0% [CI: 0.1–24.9%]) permanent hypoparathyroidism occurred in the BABA RT group, and 1 (3.4% [CI: 0.1–17.8%]) chyle leakage occurred in the COT group.
No tracheal leakage, hematoma of the surgical area or chest wall tunnels, seroma, transient or permanent RLN injury, wound infection, or Horner's syndrome occurred in any of the patients. Moreover, no iatrogenic implantation metastasis occurred in surgical tunnels or fields in the BABA RT group.
Pathological characteristics
The pathological characteristics and TNM stage of patients diagnosed with PTC in both groups are shown in Table 4. The mean cancer foci diameter of all PTCs was 1.5 ± 1.0 cm, 1.3 ± 0.8 cm, and 1.7 ± 1.1 cm in the BABA RT and COT groups, respectively, without a significant difference (p = 0.353). Two (13.3%) and 4 (40.0%) patients were found to have multiple cancer foci in the BABA RT and COT groups, respectively (p = 0.175).
Comparison of Pathologic Characteristics and TNM Stage Between the Bilateral Axillo-Breast Approach Robotic Thyroidectomy and Conventional Open Thyroidectomy Groups
ETE, extrathyroidal extension; LNs, lymph nodes; PTC, papillary thyroid cancer.
One (6.7%) and 2 (20.0%) patients were found to have bilateral cancer foci in the BABA RT and COT groups, respectively (p = 0.543). One (6.7%) and 2 (20%) patients were found to have gross ETE in the BABA RT and COT groups, respectively (p = 0.543), while 6 (40.0%) and 3 (30.0%) patients were found to have micro ETE in each group (p = 0.691). Although the number of harvested lymph nodes in the BABA RT group was slightly less than that in the COT group [37 (IQR: 27 [CI: 21.75–43.05]) vs. 39.5 (IQR: 26 [CI: 24.35–66.85]), p = 0.338], there was no significant difference. The mean number of metastatic lymph nodes harvested in each group was 6 (IQR: 16 [CI: 3.55–13.38]) vs. 19 (IQR: 26 [CI: 7.35–26.45]), p = 0.177. In particular, the number of harvested and metastatic lymph nodes in central or lateral dissection for each side was equivalent in the BABA RT and COT groups (p > 0.05).
According to the 8th American Joint Committee Cancer (AJCC) TNM staging manual, one patient in each group was classified as stage II [(6.7% [CI: 0.2–31.9%]) in the BABA RT group vs. (10.0% [CI: 0.3–44.5%]) in the COT group], and the others were all classified as stage I.
Follow-up results
Although two patients diagnosed with benign thyroid nodules were lost to follow-up, the median follow-up time of the remaining patients was 101 (IQR: 189, range: 7–287) months. The median follow-up time of patients diagnosed with PTC was 47 (IQR: 72, range: 7–287) months. The follow-up time of the BABA RT group was significantly shorter than that of the COT group (32.2 ± 18.4 months vs. 139.4 ± 94.2 months, p < 0.001). Among the PTC patients in the COT group, 1 (10.0% [CI: 0.3–44.5%]) was found to have pulmonary metastasis 63 months after surgery, and another (10.0% [CI: 0.3–44.5%]) was found to have lateral lymph node relapse 27 months postoperatively. However, none of the patients in the BABA RT group showed local recurrence or distant metastasis.
Discussion
To the best of our knowledge, this is the first case series to report robotic thyroidectomy through a BABA in the pediatric population and compare its surgical outcomes with COT. Our study showed that robotic thyroidectomy by BABA provided excellent cosmetic results and oncologic outcomes comparable to those of open surgery for thyroid carcinomas in children and adolescents, even with lateral lymph node metastasis (LNM). It can be recommended as an alternative to conventional open procedures for selected children with PTC and lateral LNM.
Compared with adults, pediatric thyroid cancer is rare and characterized by frequent regional LNM, ETE, and more often, pulmonary metastasis. Even for pediatric PTC patients with clinically negative lymph nodes, the rate of LNM could be as high as 75%, 22 and the rate of lateral LNM was 42.4–50%. 23,24 However, despite its aggressiveness and frequent metastasis, it has better survival. Pediatric patients, especially PTC with lateral LNM, need more aggressive surgical intervention, and this will inevitably leave a long and noticeable scar in the visible cervical area, which could lead to severe cosmetic concerns.
An obvious anterior cervical scar is significantly associated with lower quality of life, depression, and loss of confidence in social situations. 8 –10 Moreover, younger children and adolescents have an increased risk for hypertrophic scars. 25 Excellent and meticulous surgical decisions should consider the treatment of physical diseases and the improvement of postoperative psychological conditions for patients with good survival. Therefore, it is crucial to avoid surgical scars in the cervical area after thyroid surgery for pediatric patients.
In recent decades, several attempts have been made to develop scarless thyroidectomy in children, with the advancement and evolution of endoscopic and robotic techniques. However, all these approaches have some limitations. MIVAT still leaves a 1.5–2 cm incision in the lower neck and allows for TT and, when necessary, prophylactic central neck dissection, 13 so it has relatively narrow indications for surgery. TOETVA is considered a precisely minimally invasive procedure due to a shorter dissection distance to reach the thyroid region from the oral vestibule. 16,17
Still, it is not suitable for patients with larger tumor sizes or with LNM, both of which are quite common in pediatric thyroid cancer. 26 Robotic trans-axillary thyroidectomy has a wider working space, which makes it easier to perform thyroidectomy and lateral neck dissection. 14,15 In contrast, dissection of the contralateral thyroid lobe and access to the upper neck area is rather technically challenging, and contralateral neck LND is impossible. 27 –29 Moreover, brachial plexus injury has always been reported in this approach. 30
Many studies have demonstrated that robotic thyroidectomy through BABA is safe and technically feasible for treating thyroid diseases in adult populations. 21,31 –36 Its surgical completeness and oncologic outcomes are comparable to open procedures, and it offers improved cosmetic outcomes. BABA has several obvious superiorities. BABA is a midline approach and it offers a symmetric view of both thyroid lobes, enabling TT and bilateral lateral neck dissection more easily. BABA has a shorter learning curve and can achieve better cosmesis.
Consequently, BABA RT has been performed frequently and has become a good surgical alternative in adult patients even with advanced thyroid cancer. 21,32,37 The advantages of BABA RT in adult patients also apply to the pediatric population, most of whom have relatively advanced thyroid cancer and do not suit other approaches. In our study, since we began to perform BABA RT in 2014, 85% of children and adolescents with benign thyroid diseases or PTC have chosen this neck-scarless procedure. The high acceptance rate indicated that most pediatric patients and their parents placed great emphasis on the influences of the cervical scar.
The safety of thyroidectomy is commonly evaluated based on complications. Compared with adults, complications of thyroidectomy are higher in the pediatric population. 38 The complication rates of RT were comparable to those of COT in terms of vocal cord palsy and hypoparathyroidism, which were in agreement with previous studies. 21 In the COT group, transient hypoparathyroidism was observed in four cases (13.8%), and no permanent hypoparathyroidism occurred.
In the BABA RT group, transient hypoparathyroidism was observed in five cases (25.0%), and permanent hypoparathyroidism was observed in one case (5.0%). There were no cases of vocal cord paralysis or hematoma in either group. Thus, with a complication rate comparable to COT, BABA RT appears safe and feasible in pediatric patients.
Oncologic completeness is also an important factor in evaluating the surgical outcomes for patients with thyroid cancer, especially for children with a higher recurrence rate. The most reliable parameters of surgical completeness are the number of retrieved lymph nodes and long-term follow-up. 32 In the present study, the number of retrieved and metastatic central or lateral lymph nodes in PTC patients was similar between the BABA RT and COT groups.
Further, only two patients were found to have recurrence or metastasis in the COT group, whereas there was no recurrence or mortality in the BABA RT group. These data showed that the oncologic outcomes of BABA RT with cervical neck dissection are comparable to those of open procedures without sacrificing surgical safety parameters.
According to the ATA guidelines, 3 due to a higher incidence of multifocal and bilateral disease and an increased risk for recurrence and subsequent second surgical procedures for most patients with PTC, TT is the recommended initial surgical approach, especially for children with high-risk factors such as radiation exposure or family history. For some small unilateral lesions that are confined to the gland, and without cervical LNM, hemithyroidectomy can be selected. However, close follow-up and monitoring are required after surgery, and patients should be advised regarding the possibility of completion.
Prophylactic CND for pediatric patients with PTC is still a controversial issue. For patients with cN0 PTC, it may reduce local recurrence and increase disease-free survival. However, it does not enhance overall survival rates but increases the risk of RLN injury and hypoparathyroidism. According to the 2015 ATA guideline, 3 prophylactic CND may be selectively considered for PTC patients without clinical evidence of gross ETE and/or locoregional metastasis.
However, considering the high postoperative recurrence rate and the significantly increased difficulty of reoperation, routine prophylactic CND was recommended by the Chinese expert consensus on thyroid nodules and differentiated thyroid cancer (DTC) for children. 20 In our study, all children with PTC underwent CND, and the rate of LNM was 79.1%, which is consistent with other studies. 22,23
Our study has some limitations. First, this is a single-center and retrospective study with an inherent bias. Second, the sample size enrolled in our study was small, and the follow-up period was too short to fully evaluate the recurrence outcomes of pediatric patients with PTC. Therefore, prospective, large-sample, multicenter controlled studies with long-term follow-up are required to determine the surgical outcomes and oncologic completeness of BABA RT for the pediatric population.
In conclusion, for experienced surgeons, robotic thyroidectomy using the BABA approach can be a safe and effective alternative for children with benign thyroid diseases or DTC even with lateral lymph nodes metastasis and offers an opportunity to improve cosmetic and surgical outcomes.
Footnotes
Authors' Contributions
C.L. and Y.G. participated in the design of the study, data collection, and article writing. P.Z., T.Y., and J.X. participated in the article writing and statistical analysis. C.S. and Y.L. participated in the data collection. D.Z. participated in the data collection and helped draft the article. Q.H. participated in the study's design and helped to revise the article. X.L. participated in the design of the study, the data analysis, and the article review. All authors read and approved the final article.
Acknowledgment
The authors are grateful to Jing Yuan, PhD (the 960th Hospital of People's Liberation Army) for her professional assistance in statistical analysis.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This research was funded in part by the National Key Research and Development Program of China (2019YFC0119205), the National Natural Science Foundation of China (81702448), and the Clinical Science and Technology Innovation Program of Jinan (202019010).