
Abstract
Background:
Noninvasive encapsulated follicular variant papillary thyroid carcinoma (EFVPTC) was reclassified as “noninvasive follicular thyroid neoplasm with papillary-like nuclear features” (NIFTP) in 2016. Most existing studies that examined outcomes included patients managed as EFVPTC and only retrospectively reclassified as NIFTP. This is the first study to evaluate the clinicopathologic, molecular, and surveillance characteristics of patients diagnosed with NIFTP at the time of surgery and managed based on this diagnosis.
Methods:
We performed a retrospective cohort study of consecutive cases diagnosed as NIFTP from June 2016 to October 2021 identified from electronic medical records at a large tertiary care institution. Patients with coexisting low-risk thyroid cancers ≥1.0 cm in size or any size aggressive histology were excluded, and review of demographic, clinical, imaging, cytologic, and molecular genetic data was performed. Initial care was delivered according to existing clinical guidelines, with a consensus institutional plan for five-year follow-up after surgery.
Results:
Among 79 patients with 84 nodules diagnosed as NIFTP after surgery, 83.5% (66/79) were women and the mean age was 51 years (range, 21–84). Mean NIFTP size was 2.4 cm (range 0.15–8.0). On ultrasound, the majority of nodules were categorized as thyroid imaging, reporting and data system TI-RADS 3 (55.3%, 42/76), and TI-RADS 4 (36.8%, 28/76). On cytology, they were typically diagnosed as Bethesda III (69.1%, 47/68) or Bethesda IV (23.5%, 16/68). Molecular testing was performed on 62 nodules, and molecular alterations were found in 93.5% (58/62). The most common alterations identified in NIFTP were RAS mutation (75.4%, 43/57), THADA fusion (12.3%, 7/57), and BRAFK601E mutation (7.0%, 4/57). Fifty-two (65.8%) patients underwent lobectomy and 27 (34.2%) total thyroidectomy, and no patient received completion thyroidectomy. Twenty-one patients (26.5%) had coexisting papillary or follicular microcarcinoma. None of the patients received radioiodine ablation. On a mean follow-up of 28.5 months (range, 6–69 months), no structural or biochemical recurrences were observed.
Conclusions:
In this large cohort of patients with NIFTP diagnosed at the time of surgery and managed typically by lobectomy with no radioiodine ablation, no evidence of tumor recurrence was identified on a limited follow-up. This finding supports indolent clinical course of NIFTP.
Introduction
Thyroid tumors have traditionally been classified into benign and malignant, with no recognized intermediate, preinvasive forms such as carcinoma in situ, which occur in the majority of other organs. This changed in 2016 with the reclassification of noninvasive encapsulated follicular variant of papillary thyroid cancer (EFVPTC) to “noninvasive follicular thyroid neoplasm with papillary-like nuclear features” (NIFTP). 1 This new entity is considered a precursor for invasive EFVPTC, a tumor sharing its molecular profile and histopathology appearance with NIFTP except for the presence of invasion. The aim of nomenclature revision was to reduce overtreatment of a neoplastic entity that did not necessarily need to be classified as cancer based on its noninvasive nature, largely indolent behavior, and apparently miniscule propensity for recurrence after resection. 2
Indeed, among the 109 patients with noninvasive EFVPTC in the initial study, including 67 treated with lobectomy alone and without radioactive iodine (RAI), no recurrences were detected after 13 years median follow-up. 1 In contrast, among 101 invasive EFVPTC, 12 patients registered an adverse event including 5 who developed distant metastases, of whom 2 died of disease. The reclassification set the stage for de-escalated management of noninvasive tumors that had previously been managed as conventional papillary thyroid carcinoma (PTC), 3,4 and not only improved evidence-based management of these lesions, but also played an important role in decreasing financial burden and allaying anxiety related to a “cancer” diagnosis. 5,6
Since the original nomenclature revision, the diagnostic criteria for NIFTP were refined in 2018 in a revision that eliminated the acceptance of “less than 1% papillae” as a criterion for NIFTP and modified it to “no well-formed papillae” to avoid misdiagnosis of classic PTC in tumors with an otherwise prominent follicular pattern. 7 In addition, this change included “secondary criteria” namely lack of high-risk mutations (BRAFV600E , TERT, TP53, etc.) not expected in NIFTP.
NIFTP as a new entity was included in the WHO Classification of Tumors of Endocrine Organs 8 and in 2017 was endorsed for use by the American Thyroid Association (ATA) Guidelines on the Management of Thyroid Nodules and Differentiated Thyroid Cancer Task Force. 4 The latter suggested that NIFTP patient management should follow recommendations for low-risk differentiated thyroid cancer, that is, lobectomy would be sufficient, remnant ablation not recommended, and thyrotropin (TSH) target 0.5–2 mIU/L.
Furthermore, the ATA guidelines recommended that occasional monitoring with serum thyroglobulin and neck ultrasound can be considered, with the intensity of follow-up to be determined when more long-term data are available. 4 Since then, several observational studies have described NIFTP clinicopathologic characteristics, extent of invasion, and recurrence. 2,9 –11 An important limitation of these studies is the primary inclusion of patients who were initially diagnosed as noninvasive EFVPTC on histology and later reclassified as NIFTP, and therefore such patients had cancer-directed management including total thyroidectomy and not uncommonly radioiodine ablation.
Shortly after the nomenclature revision, our institution's multidisciplinary thyroid group adopted an institutional approach to NIFTP patients that included abandonment of completion thyroidectomy and radioiodine ablation, and follow-up after surgery similar to surveillance for low-risk differentiated thyroid cancer (Table 1). The primary aim of this study was to assess the recurrence rate in a consecutive cohort of patients diagnosed with NIFTP at the time of resection and managed under a prospective clinical algorithm. Secondary aims were to evaluate the sonographic, clinicopathologic, and molecular features of nodules that yielded the diagnosis of NIFTP at the time of surgery.
University of Pittsburgh Medical Center Recommendations for Postsurgical Follow-Up of Noninvasive Follicular Thyroid Neoplasm with Papillary-Like Nuclear Features Patients
NIFTP, noninvasive follicular thyroid neoplasm with papillary-like nuclear features; PCP, primary care provider; Tg panel, thyroglobulin and thyroglobulin antibodies; TSH, thyrotropin; US, ultrasound.
Materials and Methods
Under University of Pittsburgh Quality Improvement Review Committee (QRC) approval (QI 3259, retrospective study, patient consent waiver), we performed a retrospective cohort study of consecutive NIFTP cases that were identified by searching for the relevant diagnosis code (D49.7) from the electronic medical records of adult endocrinology and endocrine surgery clinics at the University of Pittsburgh Medical Center. The period of search was from June 2016 to September 2021; we selected the start time as June 2016 as it coincided with the initial nomenclature revision study. 1
Surgical pathology reports were reviewed to confirm that NIFTP diagnosis occurred at the time of surgery, and any cases that had been retrospectively classified from a prior diagnosis of noninvasive EFVPTC were excluded. Other exclusion criteria were the presence of coexisting papillary or follicular cancer ≥1.0 cm in size, coexisting papillary or follicular microcarcinoma (<1.0 cm) with angiolymphatic invasion or extrathyroidal extension at the time of diagnosis, or coexisting medullary or anaplastic carcinoma of any size. Coexisting papillary or follicular microcarcinoma (<1.0 cm) without any angiolymphatic invasion or extrathyroidal extension at the time of diagnosis was not considered an exclusion criterion, as these incidental lesions almost always carry an excellent prognosis and do not warrant additional treatment other than what would have been carried out for the primary lesion (NIFTP).
Data were extracted from clinical notes, fine-needle aspiration (FNA) cytology reports, surgical pathology reports, molecular testing reports, and surveillance laboratory and radiologic reports. Histopathology slides were reviewed by thyroid pathologists at the University of Pittsburgh. NIFTP was diagnosed after examination of the entire tumor and capsule, using the revised criteria including encapsulation, follicular growth pattern, nuclear features of PTC, no well-formed papillae, and no invasion. 7 Available ultrasound images were reviewed by two endocrinologists experienced in performing and reporting thyroid ultrasounds. When necessary, nodules were classified using the thyroid imaging, reporting and data system (TI-RADS). 12 Most patients had molecular testing on FNA samples using ThyroSeq Genomic Classifier (TSv2 until October 2017, TSv3 after November 2017). Thyroglobulin and thyroglobulin antibody levels were measured using the Beckman Coulter chemiluminescent method.
Recurrence after resection was defined as evidence of structural disease on neck examination or imaging, or the presence of an elevated thyroglobulin level after total thyroidectomy (unstimulated TSH thyroglobulin >2 ng/mL in the absence of thyroglobulin antibodies). Thyroglobulin levels after lobectomy were not considered in assessment of recurrence. Data collection and calculation of percentages and means was performed using Microsoft Excel.
Results
Case selection and demographics
Although record search resulted in 90 consecutive patients with NIFTP diagnosis from June 2016 to October 2021, we excluded 3 patients who had been reclassified to NIFTP retrospectively. In addition, we excluded eight patients who did not meet other selection criteria stated previously. The remaining 79 patients had 84 histologic NIFTP lesions managed prospectively (Fig. 1). Among these, the mean age was 51 years (range, 21–84) and 66 patients (83.5%) were women.
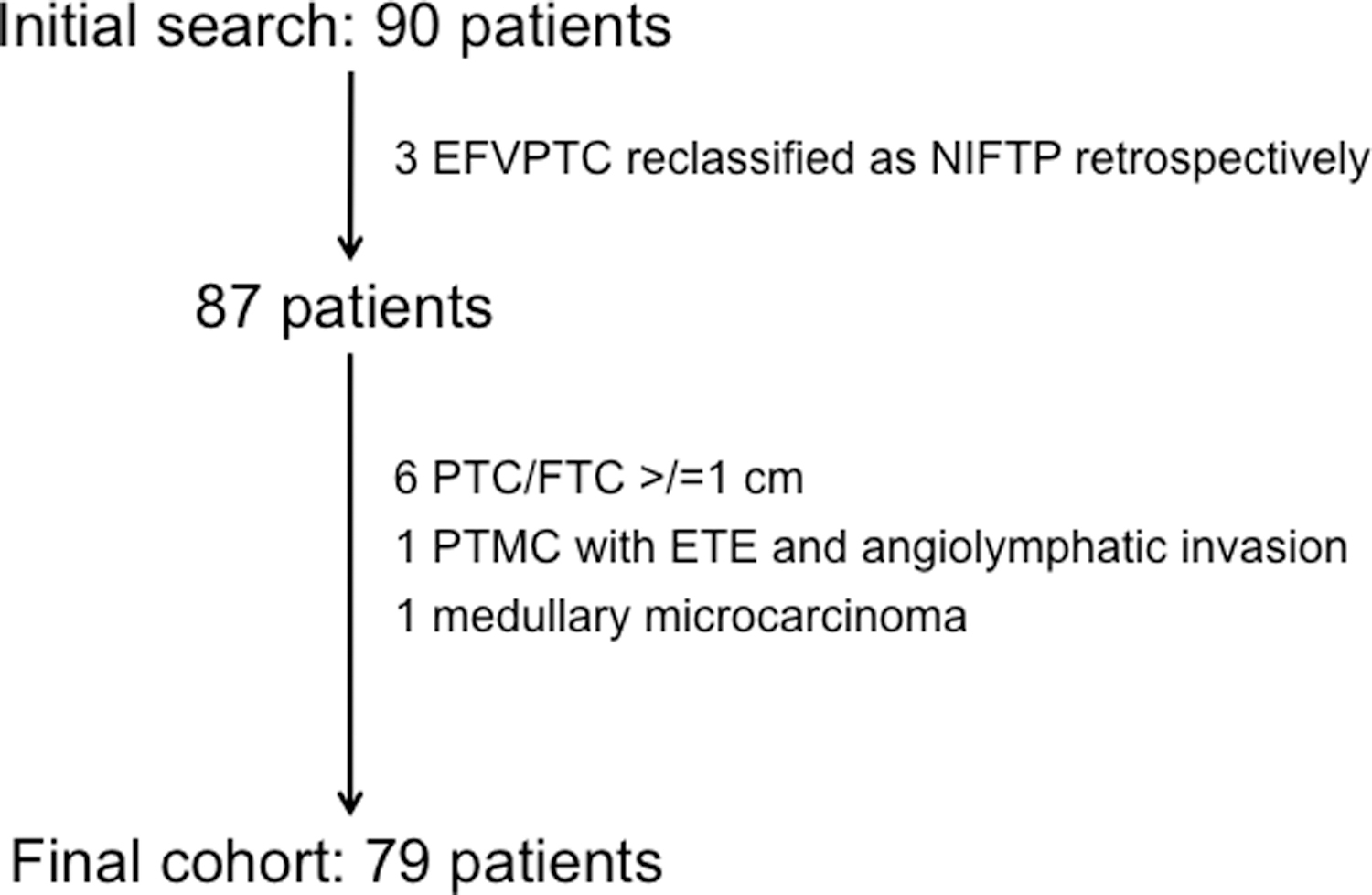
Flowchart depicting patient selection and exclusion criteria. EFVPTC, encapsulated follicular variant papillary thyroid carcinoma; ETE, extrathyroidal extension; FTC, follicular thyroid carcinoma; NIFTP, noninvasive follicular thyroid neoplasm with papillary-like nuclear features; PTC, papillary thyroid carcinoma; PTMC, papillary thyroid microcarconima (<1.0 cm).
Nodule characteristics and molecular profiles
Thyroid ultrasound images were reviewed for 76/84 NIFTP nodules; the remaining 8 either did not have available imaging, or had NIFTP incidentally diagnosed on surgical pathology without preoperative identification by ultrasonography. The nodules ranged in size from 0.9 to 8.2 cm (mean 2.8) and were typically solid, hypoechoic, or isoechoic, with smooth margins corresponding to the presence of an intact capsule (Fig. 2). Overall, the most common radiologic categories were TI-RADS 3 (mildly suspicious) or TI-RADS 4 (moderately suspicious), together accounting for 70 of the 76 cases (92.1%) (Table 2).
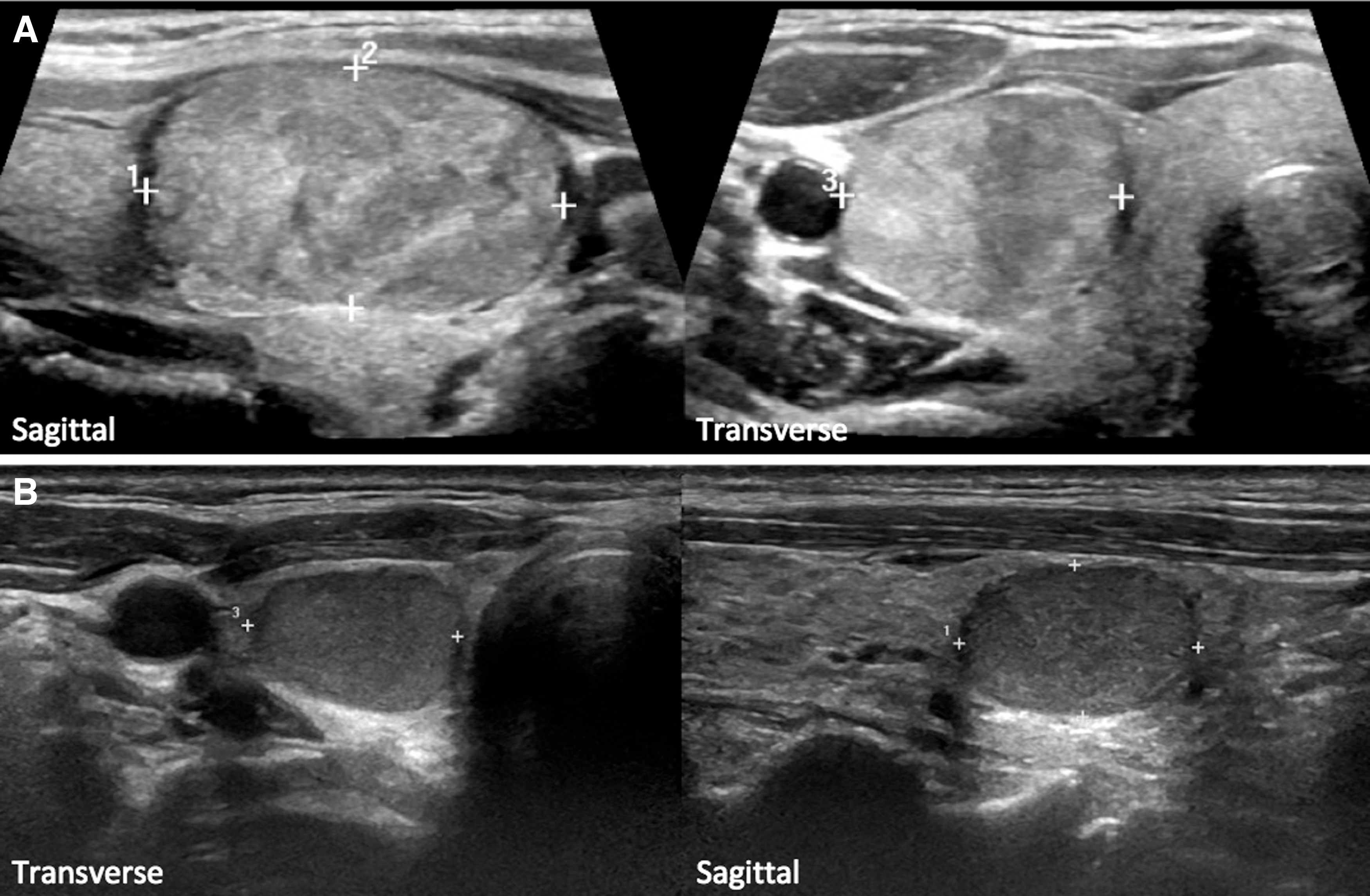
Typical ultrasound appearance of NIFTP nodules. Solid, isoechoic (
Demographic and Clinicopathologic Data
AUS/FLUS, atypia of undetermined significance/follicular lesion of undetermined significance; FN/SFN, follicular neoplasm/suspicious for follicular neoplasm; TI-RADS, thyroid imaging, reporting and data system.
FNA cytology results were available for 68/84 nodules. The most common NIFTP cytologic diagnosis was atypia of undetermined significance/follicular lesion of undetermined significance occurring in 47/68 nodules (69.1%), followed by follicular neoplasm/suspicious for follicular neoplasm in 16 (23.5%) (Table 2). Three NIFTP nodules (4.4%) were categorized as benign, and 1 (1.5%) each as nondiagnostic and suspicious for malignancy. Patients with nondiagnostic or benign cytology underwent thyroidectomy because of large nodule size (>4.0 cm).
Molecular testing was performed in 62/84 nodules (73.8%). One sample was tested using Afirma Gene Expression Classifier and the remainder by ThyroSeq Genomic Classifier. Molecular testing showed positive results in 58/62 NIFTP cases (93.5%) with specific genetic information available in 57 cases. The most common mutation observed was RAS—either alone or in combination with other low to intermediate risk alterations, which accounted for 43 of the 57 positive samples (75.4%). Other alterations observed at lower frequencies were IGF2BP3-THADA fusion, BRAFK601E mutation, and gene expression alterations (Table 3). No BRAFV600E or other BRAFV600E -like alterations or high-risk mutations (TERT, TP53, etc.) were observed in these samples.
Mutational Testing of Fine-Needle Aspiration Samples
CNA, copy number alterations; GEA, gene expression alterations.
Patient management and surgical pathology findings
Of the 79 patients, 52 (65.8%) underwent lobectomy, 27 (34.2%) total thyroidectomy, and no patient received completion thyroidectomy. The indications for and extent of thyroidectomy followed current medical and surgical guidelines, 4,13 including consideration of coexisting pathology, hyperthyroidism, and substernal goiter. No patient received RAI postoperatively.
The mean size of NIFTP lesions was 2.4 cm (range, 0.15–8.0). Sixteen of 84 lesions (19.0%) were ≥4.0 cm, while 11 (13.1%) were <1.0 cm. Five patients (6.3%) had multifocal NIFTP (each with two NIFTP foci), one of whom had bilateral lesions. Twenty-one patients (26.5%) had coexisting papillary (n = 20) or follicular (n = 1) microcarcinoma in the examined specimen, without evidence of angiolymphatic invasion or extrathyroidal extension.
Clinical course
The mean follow-up period after resection of NIFTP was 28.5 months (range, 6–69). All patients received at least one office visit and neck examination. Sixteen patients (20.3%) were lost to follow-up. Thyroglobulin levels were checked at least once during surveillance in 50 patients (63.3%), while at least one neck ultrasound was completed during follow-up in 49 patients (62%). A total of 63 patients (79.7%) had either a thyroglobulin level or neck ultrasound in addition to neck examination. Upon reviewing the results of the stated modalities for assessment of recurrence, none of the 63 patients with available follow-up had any evidence of structural or biochemical recurrence of thyroid tumor.
Discussion
Several studies have reported clinical features and outcomes in patients with noninvasive EFVPTC that was retrospectively reclassified as NIFTP after nomenclature revision. However, these patients, at least before reclassification, would have been managed similarly to conventional thyroid cancer. To our knowledge, this is the first study of a large cohort of patients with NIFTP diagnosis established at the time of surgery, who were prospectively managed based on their NIFTP diagnosis typically with thyroid lobectomy and no radioiodine ablation.
Most existing studies corroborate findings of the initial report that NIFTP has an indolent clinical behavior with an extremely low likelihood of nodal or distant metastases. A recent meta-analysis including 1242 cases diagnosed or reclassified as NIFTP and followed for 16–134 months reported a 1.8% rate of neck lymph node metastasis and 0.08% rate of distant metastasis. 2
Earlier reports published soon after nomenclature revision reported a small percentage of cases meeting criteria for NIFTP that had nodal or distant metastases at the time of diagnosis or on follow-up. 10,11,14 –16 Many of these tumors contained some well-formed papillary structures and/or were positive for BRAFV600E mutation, which are findings that typically exclude the diagnosis of NIFTP. Such reports have demonstrated that too-broad interpretation of the NIFTP criterion allowing for “less than 1% papillae,” used in the initial study to account for single ill-formed papillary structures, may result in incorrect diagnosis of some classic papillary carcinomas as NIFTP. 11,14 This finding provided the rationale for the 2018 revision of the diagnostic criteria that replaced the “less than 1% papillae” criterion with “no well-formed papillae.” 7
At our institution, thyroid pathologists had the advantage of being well aware of the intent and scope of the initial <1% papillae criterion, so that early application of this criterion would be expected. This in part is confirmed by the lack of cases positive for BRAFV600E mutation in the study, a mutation almost exclusively limited to classic papillary carcinoma.
Some studies note patients with tumors that may meet criteria for reclassification as NIFTP but who had lymph node metastases. These cases had coexisting papillary microcarcinoma, creating uncertainty about the origin of the tumor in the lymph nodes. 2 In addition, some of these studies are limited by the lack of molecular testing, as the presence of BRAFV600E mutation would have resulted in reconsideration of the NIFTP diagnosis. Similarly, the effects of NIFTP multifocality and bilaterality on prognosis need to be better understood. 9
Our cohort had 26.5% (21/79) patients with coexisting papillary or follicular thyroid microcarcinoma, and 6.3% (5/79) with multifocal NIFTP (4 patients with unilateral, 1 with bilateral lesions). Despite the relatively high incidence of thyroid microcarcinoma in our cohort, its presence was not associated with recurrence/metastasis during follow-up. Multifocality of NIFTP in our cohort is also lower compared with existing studies, which could potentially be explained by higher rates of lobectomy than total thyroidectomy in our population. 2,9,17 The lack of recurrence/metastasis in our cohort can also partly be explained by the strict application of the NIFTP diagnostic criteria by specialized thyroid pathologists at our institution. 1,7
The one reported patient with lung metastasis who accounted for the 0.08% distant metastasis rate in the meta-analysis of cases retrospectively reclassified as NIFTP had a 6.4 cm primary tumor. 14 Our cohort included 16 patients (20.3%) with a primary NIFTP tumor ≥4.0 cm, the largest lesion being 8.0 cm, and with a mean follow-up period of 31 months (range 7–69) there were no recurrences observed.
In this study, the preoperative characteristics of NIFTP nodules were similar to those widely reported in EFVPTC studies. 1,2,18 –21 First, radiologically most NIFTP were solid, isoechoic, or hypoechoic with smooth, intact margins and without high-risk ultrasonographic features (TI-RADS 3 or TI-RADS 4). The observed rarity of cases with TI-RADS 5 score correlates well with prior observations 20 –22 and is expected, because by virtue of being encapsulated and nonpapillary, NIFTP are not likely to score for high-risk features related to margins and echogenic foci. Second, on cytology, NIFTP nodules were typically diagnosed as Bethesda III and IV. Fewer than expected number of NIFTP in this study had Suspicious for Malignancy (Bethesda V) cytology, which is likely owing to mostly moderately developed nuclear features of PTC in these cases, which would correspond to nuclear score 2 in the initial reclassification report. 1
The higher rate of Bethesda V cytology in earlier studies could again be explained by the inclusion of tumors with minimal papillary structures, which would be expected to have more pronounced nuclear features of papillary carcinoma. 18,20,21 Overall, the present findings confirm previous reports that cytologically, NIFTP is likely to be distinguished from classic papillary carcinomas, which are typically Bethesda VI or Bethesda V, but not from follicular-patterned thyroid tumors and particularly from invasive EFVPTC that have similar cytologic features and differ only in invasion. 19,23,24
Molecular profiles of NIFTP demonstrated that they are predominantly clonal neoplasms driven by RAS-like alterations. Indeed, RAS mutations represented the most common genetic event in these tumors, found in three-fourth of the cases. Other observed changes included RAS-like alterations such as THADA fusions, BRAFK601E mutation, and gene expression alterations. 25,26 Overall, the molecular profiles identified in NIFTP patients were similar to those found in noninvasive EFVPTC in the initial reclassification study and in subsequent series of reclassified cases. 1,27,28 The absence of BRAFV600E or other high-risk mutations in the present cohort supports the accuracy of the NIFTP diagnoses, in keeping with the revised secondary criteria for diagnosis. 7 Overall, among the nodules that had preoperative molecular testing, most (93.4%, 58/62) had a positive test. Even among the four nodules that were negative on molecular testing, two harbored low-risk mutations such as PTEN and GNAS, typically seen in benign adenomas.
One additional case had a very low-level NRAS mutation not significant enough to meet the malignancy/NIFTP threshold needed for a positive test, which was likely owing to limited tumor sampling. Overall, the results of this study are reassuring that most NIFTP should be positive on preoperative testing using currently available molecular tests. However, although preoperative molecular analysis can distinguish NIFTP from classic papillary carcinomas (based on the lack of BRAFV600E and like alterations) and potentially, from high-risk cancers (based on the lack of TERT, TP53 and other high-risk mutations), it cannot differentiate NIFTP from invasive EFVPTC or benign follicular adenomas that are also driven by RAS mutations and RAS-like alterations and share histopathologic characteristics with NIFTP including encapsulation and follicular growth pattern. For that reason, lobectomy is still required to exclude invasion in such nodules, which is required for NIFTP diagnosis.
In our cohort of patients with NIFTP diagnosis established at the time of surgery whose follow-up was provided under an institutional surveillance algorithm, none had evidence of biochemical or structural recurrence in short-term follow-up with a mean of 28.5 months. Almost 80% patients had either neck ultrasound, thyroglobulin level, or both checked during follow-up, in addition to neck examination. Our institutional strategy for postsurgical surveillance of patients with NIFTP is generally consistent with the ATA recommendations to manage these patients as for low-risk differentiated thyroid cancer, 4 as well as with recommendations by others suggesting that some form of active surveillance should be considered especially for patients undergoing lobectomy, given the potential risk of contralateral lesions and multifocality. 17 Additional data on longer-term follow-up are needed to generate evidence-based guidelines for the intensity and length of following patients with NIFTP after surgery.
The patients in this study were predominantly treated with lobectomy and none received completion thyroidectomy after NIFTP diagnosis. Another key design difference of this study compared with existing NIFTP reports was that the postsurgical management was conducted based on the NIFTP diagnosis and as a result, no patient received RAI postoperatively. In the EFVPTC reclassification studies, there were invariably patients who had received RAI as they had been treated for “conventional thyroid cancer.” Our findings strengthen the evidence that NIFTP patients do well when managed with lobectomy and without RAI, as is gradually becoming the standard of care for these patients.
This study has several limitations. First, it is retrospective in nature, although the diagnosis of NIFTP was established at the time of surgery. Second, the follow-up period was relatively short. Considering that thyroid cancer recurrences may occur after a long latency, studies with more extended follow-up are needed to assess long-term outcomes of the NIFTP diagnosis. Third, 20% were lost to follow-up, and 38% patients had no ultrasound imaging during follow-up. Although all patients received neck examination during follow-up, the sensitivity and reliability of such an assessment is limited.
Another limitation is that the investigation was conducted at a single academic institution with a subspecialized model of care for patients with thyroid nodules (i.e., a multidisciplinary thyroid center with dedicated pathologists, endocrinologists, and surgeons providing coordinated care), so the findings may not be fully generalizable to all clinical settings. In addition, as detailed previously we observed incomplete programmatic compliance with the clinical algorithm for postoperative surveillance, which is likely attributable to an implementation phase, but which can potentially influence the results of the study.
In summary, the results of this study of a large cohort of patients prospectively diagnosed with NIFTP at the time of surgery demonstrate that the ultrasonographic, cytologic, and molecular characteristics of these tumors are similar to those expected following the nomenclature change. Of importance, when diagnosed using the accepted histopathologic criteria, no evidence of recurrent disease during follow-up was observed, although most of the patients were treated with lobectomy and none receive adjuvant radioiodine in management. Although studies with longer follow-up are required for further confirmation, these findings provide support for the highly indolent behavior of NIFTP tumors.
Footnotes
Authors' Contributions
C.T.: Conceptualization, data curation, formal analysis, investigation, methodology, writing—original draft, writing—review and editing. L.Y.: Methodology, writing—review and editing. E.M.M.: Writing— review and editing. R.S.: Writing—review and editing. S.I.C.: Writing—review and editing. N.P.O.: Writing—review and editing. S.E.C.: Formal analysis, writing—review and editing. M.N.N.: Conceptualization, writing—review and editing. Y.E.N.: Conceptualization, formal analysis, methodology, supervision, writing—original draft, writing—review and editing. E.K.-F.: Conceptualization, formal analysis, methodology, supervision, writing—review and editing.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This study did not receive any financial support from any funding agency in the public, commercial, or not-for-profit sectors. S.E.C. receives general support from the William and Susan Johnson Fund for Endocrine Surgery Research.