
Abstract
Background:
Subacute thyroiditis (SAT) is a thyroid disease initiated by viral infection. Whether severe acute respiratory syndrome coronavirus 2 infection can cause SAT is unclear. This study investigated changes in the nationwide incidence of SAT during the coronavirus disease 2019 (COVID-19) pandemic.
Methods:
This is a retrospective, cross-sectional population-based study. Data regarding SAT and related viral diseases, including COVID-19, from 2017 to 2020 were collected from the National Health Insurance Service and Korea Disease Control and Prevention Agency databases.
Results:
In a total of 15,447 patients, 2484 men and 12,963 women diagnosed with SAT from 2017 to 2020 were included in this study. The incidence of SAT was significantly higher in 2020 than in 2017–2019 (8.30 vs. 7.27 per 100,000 persons, p < 0.001), while the incidence of SAT-related respiratory viral diseases, except for COVID-19, markedly decreased in 2020. The peak age of SAT incidence in 2020 was 50–59 years, and the women-to-men ratio was 5.4 (similar to that in 2017–2019). Corticosteroids were prescribed more often (72% vs. 58%, p < 0.001), and the prescription rate exceeding 1 month was significantly higher (45% vs. 40%, p < 0.01) in 2020 than in 2017–2019.
Conclusions:
The incidence of SAT increased in 2020 in association with COVID-19. A diagnostic approach to COVID-19 needs to be considered in patients with SAT during the COVID-19 pandemic.
Introduction
Subacute thyroiditis (SAT), also known as de Quervain thyroiditis, is a self-limiting thyroid disease initiated by viral infections or post-viral inflammatory processes. It is typically characterized by a triphasic clinical course, including thyrotoxicosis, hypothyroidism, and a return to normal thyroid function. Clinically, SAT presents with neck pain, frequently radiating to the ears, and various systemic symptoms, including fever, asthenia, and malaise. Many patients also present with clinical and/or biochemical manifestations of mild-to-moderate thyrotoxicosis, such as tremors and palpitations in the initial phase. 1
Several respiratory viruses, including coxsackievirus, 2 mumps, 3 Epstein–Barr virus, 4 cytomegalovirus, 5 and influenza virus, 6 are reportedly associated with SAT development. 7 However, diagnostic evaluations aimed at identifying the viral etiology are not generally performed in these patients since most cases do not require specific antiviral treatment. Direct and indirect data support the viral infection-based pathogenesis of SAT. Epidemiological data showed an overlap between seasonal infectious diseases and SAT outbreaks. 3,8 Patients with SAT reportedly have high titers of virus-specific antibodies or virus-positive swabs, and SAT has been linked to the presence of antibodies to specific viruses. 2,3,9 However, virus cultures from thyroid tissue and viral RNA identification from thyroid cytological samples have yielded conflicting results. 10 –12 In addition, whether follicle damage in SAT results from direct viral infection of the gland or the immunological response of the host to the viral infection is unclear.
The effects of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) on the thyroid have been suggested in terms of both clinical manifestations and complications of the coronavirus disease 2019 (COVID-19) pandemic. SAT was one of the thyroid-related COVID-19 complications reported in some case reports, 13 –15 followed by several original articles, editorials, and reviews. 16 –20 A recent review summarized 27 SAT cases associated with COVID-1921 and concluded that clinical presentation of SAT in patients with COVID-19 is similar to that of general SAT; nevertheless, the sample sizes and quality of published data are limited.
This study aimed to investigate changes in the national SAT incidence during the COVID-19 pandemic. The nationwide databases of the Korean National Health Insurance Service (NHIS) and Korea Disease Control and Prevention Agency (KDCA) were used to evaluate the annual incidence of SAT and SAT-related viral diseases, including COVID-19, from 2017 to 2020.
Methods
Data source and study population
This is a retrospective, cross-sectional population-based study. The NHIS database in South Korea, from January 2017 to December 2020, was used for health insurance claims data research. Approximately 97% of the country's population is enrolled in the NHIS program; therefore, NHIS data provide information on the health care use of the entire South Korean population. The NHIS data include all citizens' qualifications and insurance premiums, medical examination results, medical history (ICD-10 diagnostic codes), test items, drug prescriptions, hospitalizations, outpatient clinic visits, and registration information for cancer and rare incurable diseases. KDCA maintains the nationwide infectious disease statistics based on the reported data from each clinic and hospital. KDCA integrates data and calculates statistics on infectious diseases yearly, as published on its website (
Since SAT is presumed to be caused by a viral infection, 7 we investigated the annual incidence of respiratory viral infections, including enterovirus, adenovirus, parainfluenza, mumps, influenza, and COVID-19 from the annual statistics provided by the KDCA Infectious Disease Portal. 22 SAT has been considered a seasonal incidence, with a higher prevalence in spring and fall since it is caused by upper respiratory infections. 23,24 The monthly incidence of SAT per 100,000 persons was analyzed.
Given that the first COVID-19 case in South Korea was detected in January 2020, 25 data from 2017 to 2020 were collected from the NHIS and KDCA and divided into two groups: data from 2017 to 2019 (before the COVID-19 pandemic) and data from 2020 alone (during the COVID-19 pandemic). The study protocol was approved by the institutional review board (IRB) of Chung-Ang University Hospital (IRB 1911-031-16294). The requirement for obtaining informed consent was waived due to the study's retrospective nature and anonymized data usage. This study adheres to the tenets of the Declaration of Helsinki.
Operational definition of disease and SAT clinical data collection
SAT was defined as a case in which the diagnostic code of SAT (E061) was claimed more than twice within 6 months, and an erythrocyte sedimentation rate test code (B1030, 1033, 1034, D0100) was claimed more than once during the same period. A total of 15,447 SAT cases were identified from the total population covered by Korean NHIS, from 51,230,704 in 2017, 51,300,879 in 2018, 51,337,423 in 2019, to 51,349,259 in 2020 (Fig. 1).
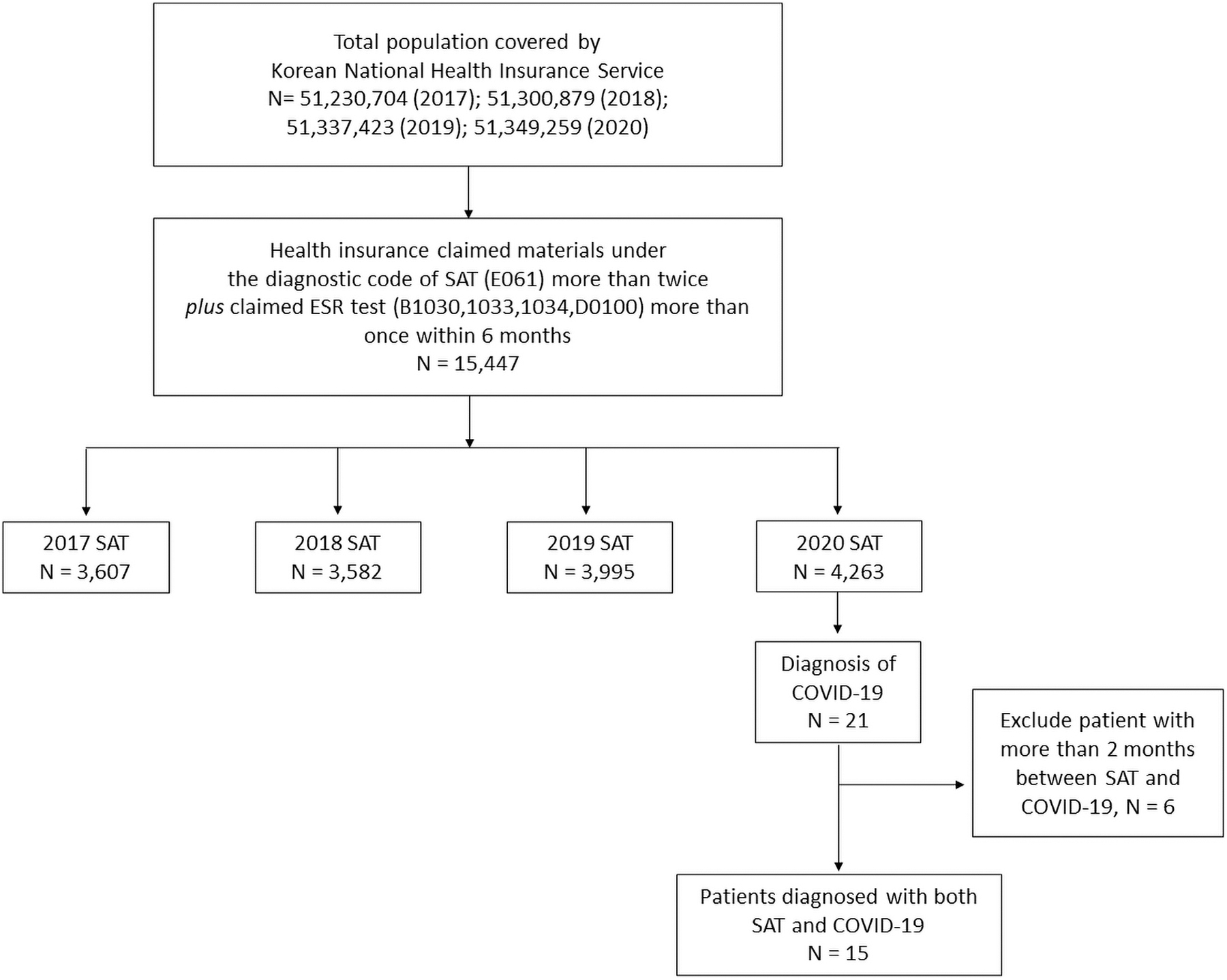
Flowchart for study participants. COVID-19, coronavirus disease 2019, SAT, subacute thyroiditis.
SAT with molecularly confirmed COVID-19 was defined as a case in which all of the following conditions were satisfied: (1) SAT defined as per the above criteria in 2020 and (2) the diagnostic code of COVID-19 (U071, U072) claimed from 2 months before to 2 months after SAT diagnosis. Of the 21 patients diagnosed with COVID-19 among SAT patients in 2020, 15 patients met the criteria of synchronized diagnosis of both SAT and COVID-19 (Fig. 1).
Data regarding age, sex, and time of SAT and/or COVID-19 diagnosis were collected. Moreover, data on prescribed medication history after SAT diagnosis were collected. Corticosteroid use was analyzed annually to assess disease severity. In the later phase of SAT, hypothyroidism requiring levothyroxine treatment is often observed, which may be mostly transient or rarely permanent. Therefore, levothyroxine use was also analyzed. Thus, data on the prescription rate and duration of corticosteroid use (prednisolone [217001ATB] and methylprednisolone [193302ATB]) and levothyroxine (183607ATB, 183611ATB, 183608ATB, 183602ATB, 183601ATB, 183610ATB, 183604ATB, 183606ATB, 183609ATB, 183603ATB, 184402ATB, and 296800ATB) were collected.
Statistical analyses
The annual incidence of SAT per 100,000 persons was calculated by dividing the number of patients with SAT by the resident population registered each year. We compared the average incidence of each viral infection, including SAT, before (2017–2019) and after (2020) the COVID-19 outbreak. Moreover, subgroup analyses were performed for sex and age by decade. Considering the seasonal variation in incidence rates commonly observed in respiratory infectious diseases, we calculated the monthly incidence rate of each virus. Comparisons of incidence rates between groups were performed using the chi-square test, and the Mantel–Haenszel test was used for trend analysis. Statistical significance was set at p < 0 · 05. Statistical analyses were performed using the SPSS software package (IBM Corp., Version 26).
Results
The increased annual incidence of SAT in the COVID-19 era
The population-based annual incidences of SAT from 2017 to 2020 were 7.04, 6.98, 7.78, and 8.30 per 100,000 persons, respectively, with a significantly higher incidence in 2020 than in 2017–2019 period (p < 0.001, Table 1). Contrarily, the incidence of respiratory viral diseases, except COVID-19, significantly decreased in 2020 compared with that in the 2017–2019 period (Table 1 and Supplementary Fig. S1A, B). SAT also increased in 2019 compared with that in 2017–2018 (Supplementary Fig. S2). The rise between April and June appears to result from an unusual peak of influenza from March to May 2019. Another SAT increase incidence in October 2019 was due to the parainfluenza infection between July and September. SAT incidence increased in 2020—the first year of the newly emerged COVID-19—while the incidence of other respiratory viral diseases that can play pathogenic roles in the occurrence of SAT had robustly decreased.
Number of Patients with Subacute Thyroiditis and Respiratory Tract Infections from 2017 to 2020
p-Value for the comparison between “2017–2019” and “2020.”
CIR, crude incidence rate per 100,000 persons; COVID-19, coronavirus disease 2019; N, no; SAT, subacute thyroiditis; Y, yes.
Clinical characteristics of SAT in the COVID-19 era
Demographic findings
Age, sex, and seasonal variations in SAT were compared between the 2017 to 2019 period and 2020 to explore clinical characteristics of SAT during the COVID-19 era. The peak SAT incidence rate was observed in the 50- to 59-year age group, both in the 2017 to 2019 period and 2020. Meanwhile, the largest increase from before the 2017 to 2019 period to 2020 was observed in the 30- to 39-year age group (17.3%, p < 0 · 001), followed by the 60- to 69-year age group (17.0%, p < 0 · 001) (Fig. 2). Interestingly, the peak COVID-19 incidence in 2020 occurred in patients in the 60- to 69-year age group in South Korea (Supplementary Fig. S3).
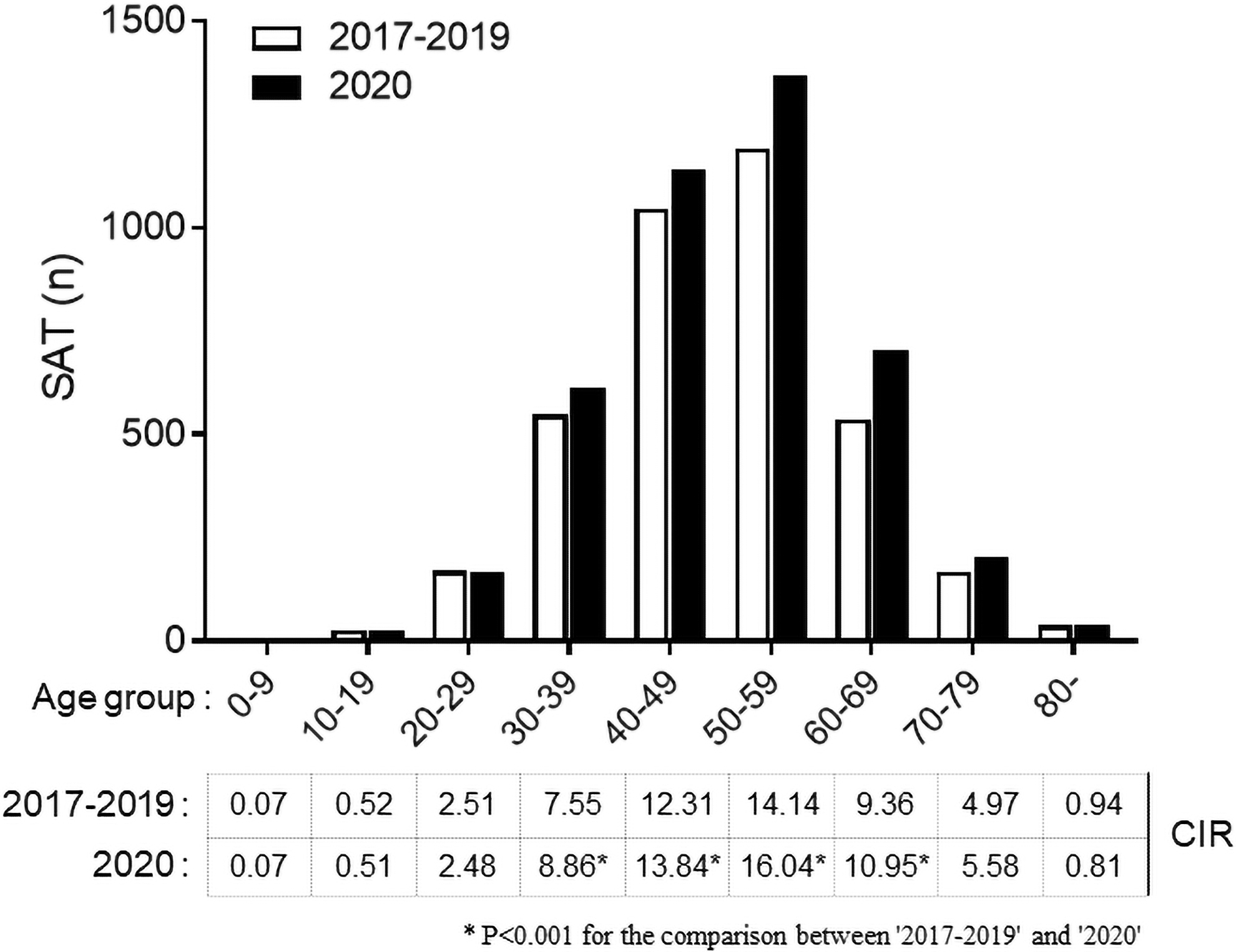
Incidence of SAT by age group. The number of SAT cases is presented in the graph (upper), and CIRs per 100,000 persons are presented in the table (lower). *p < 0.01, comparison between 2017–2019 and 2020. CIR, crude incidence rate per 100,000 persons.
The incidence rates per 100,000 persons for women in 2017, 2018, 2019, and 2020 were 11.9, 11.6, 12.9, and 14.0, respectively; for men, they were 2.2, 2.3, 2.6, and 2.6, respectively. A significantly higher incidence rate of SAT was observed in women in 2020 than in the 2017 to 2019 period (14.0 vs. 12.1, p < 0.001), but no significant difference was observed in men (2.6 vs. 2.4, p = 0.088). The women-to-men ratio was similar each year, with a mean ratio of 5.1 in the 2017–2019 period and 5.4 in 2020 (p = 0.186) (Supplementary Table S1).
Seasonal variations
The mean monthly SAT incidence from June to September was significantly higher than that from October to May in the 2017–2019 period (0.66 ± 0.01 vs. 0.58 ± 0.01, p = 0.007) and in 2020 (0.64 ± 0.08 vs. 0.80 ± 0.05, p = 0.003). The seasonal difference was 2.1-fold higher in 2020 than in 2017–2019 (Fig. 3A). Additionally, the monthly SAT incidence from May to July and from September to December was significantly higher in 2020 than in 2017–2019. Interestingly, the two periods of increased SAT incidence in 2020 were 1–2 months after the first and second COVID-19 outbreaks (Fig. 3B).
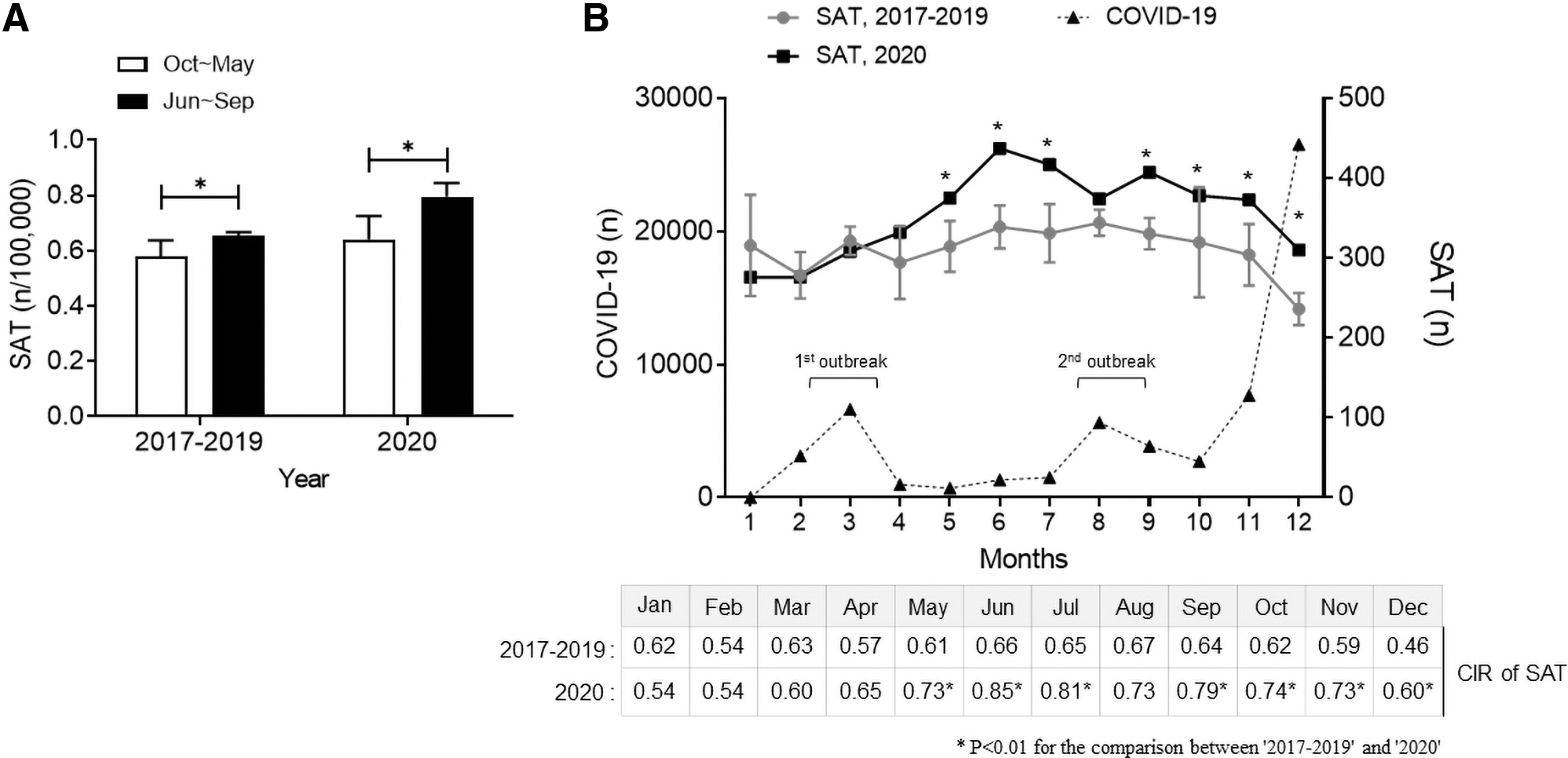
Seasonal occurrence of SAT. (
Treatment
Among all patients with SAT, total corticosteroid use was significantly higher in 2020 than in the 2017–2019 period (72% vs. 58%, p < 0.001, Fig. 4A). Additionally, among the patients who used corticosteroids, the number of prescriptions exceeding 1 month was significantly higher in 2020 than in 2017–2019 (45% vs. 40%, p < 0.01, Fig. 4B). Overall, corticosteroid use for SAT treatment in 2020 was more frequent, with a duration longer than that in 2017–2019, suggesting a possible increased disease severity of SAT in 2020.

Corticosteroid prescription number in SAT. (
In 2020, among 4263 patients with SAT, 24.6% received levothyroxine therapy—a rate similar to the 2017–2019 period. In 2020, the mean duration of levothyroxine prescription was 256 ± 164 days, and the mean time from SAT diagnosis to levothyroxine prescription was 76 ± 73 days (Supplementary Table S2).
SAT with molecularly confirmed COVID-19
Among the patients with confirmed SAT in the 2020 NHIS data, 15 had COVID-19 in the same year (Table 2). The mean age at diagnosis was 44.0 ± 14.8 years, and 86.7% were women. Eleven of these patients had SAT after COVID-19; 10 were diagnosed with SAT within 30 days of COVID-19 diagnosis, and the remaining patient between 31 and 60 days. Interestingly, four patients had SAT within 2 months before COVID-19 molecular diagnosis. Among the 15 patients with confirmed SAT with COVID-19 in the same year, 13 (86.7%) were prescribed steroids, and the mean duration of steroid use was 60.9 ± 47.0 days. Additionally, four (26.7%) patients were prescribed levothyroxine after SAT diagnosis. The mean duration of levothyroxine use was 351 ± 32 days, and the mean time from SAT diagnosis to levothyroxine prescription was 88.3 ± 59.1 days.
Demographics, Clinical Characteristics, and Outcome of Subacute Thyroiditis with Molecularly Confirmed COVID-19
RT-PCR, reverse transcriptase-polymerase chain reaction; SD, standard deviation.
Discussion
The present study demonstrated an increased SAT incidence in 2020, the year the COVID-19 pandemic began, by assessing claims data from the NHIS in South Korea. The annual incidence of SAT-related viral infections, apart from COVID-19, robustly decreased in the same year. Therefore, we suggest that the SAT increase in 2020 was associated with the COVID-19 pandemic, although molecular confirmation of COVID-19 in patients with SAT in 2020 was <0.5%. Aside from 2020, the annual incidence of SAT in 2019 was significantly higher than that in 2017 and 2018 (Supplementary Fig. S2). This was explained by a significant increase in SAT-associated viral infections—such as enterovirus, adenovirus, and parainfluenza—in 2019 compared with that in 2017 and 2018 (Supplementary Fig. S1A). To our best knowledge, this is the first nationwide report on the annual incidence of SAT in the COVID-19 era.
A previous epidemiological study from the Rochester Epidemiology Project in Olmsted County, Minnesota, showed that the annual incidence of SAT was 12.1 cases per 100,000 between 1970 and 1997. 24 The peak incidence was in the fifth decade of life, showing women's preponderance. 24 They also speculated seasonal variations of SAT; more cases occurred in fall and spring but did not show statistical significance. 24 The annual incidence and clinical features of SAT before COVID-19 (2017–2019) in this study were similar to those of a previous study. The annual incidence was 7.27 cases per 100,000, and the peak incidence age was 50–59 years, with a higher women-to-men ratio.
Additionally, seasonal variations in SAT were confirmed in this study. The monthly SAT incidence was significantly higher from June to September (early summer to early autumn) than from October to May. Demographic and clinical characteristics of SAT in 2020 were analyzed after confirming the concordance of the present and previous studies' findings. As an indicator of SAT severity, we compared corticosteroid prescription rates. However, corticosteroids can also be used for COVID-19 treatment, and not only for SAT. Therefore, it is necessary to identify the disease for which corticosteroid was prescribed. In 2020, only 15 patients with SAT were simultaneously diagnosed with COVID-19, and since these were mild COVID-19 cases without hospitalization, corticosteroids were considered for SAT treatment.
Among 4263 SAT cases in 2020, 15 (0.35%) were molecularly confirmed to coincide with COVID-19. This was a much smaller number than expected since the annual incidence of SAT was significantly increased in 2020, even though the incidence of all other SAT-related viral infections—except for COVID-19—was markedly decreased. Currently, we cannot clearly explain whether the increased SAT incidence in 2020 was related to the COVID-19 pandemic. SAT, as a comorbidity, can be underestimated, given that the diagnostic approach and medical care provided to patients with COVID-19 are generally focused on respiratory symptoms and systemic inflammatory response syndrome. Indeed, a recent focus has been on COVID-19-related “painless” SAT. 1
Early analgesics use, including nonsteroidal anti-inflammatory drugs and intensive care unit care, is the main reasons for masking neck pain, a diagnostic marker of SAT. 26,27 The possibility of true painless SAT has also been suggested. 1 However, these are merely possibilities for underestimating SAT incidence during the COVID-19 pandemic and not an explanation for the discrepancy observed between the increased annual incidence of SAT and marked less frequent cases of COVID-19-positive SAT in this study. We evaluated the cases of 15 patients with COVID-19-positive SAT in South Korea to gain insight into COVID-19-associated SAT.
Previously, systematic reviews, including individual case reports or series, were performed and concluded that the clinical features of SAT in patients with COVID-19 were similar to those in SAT that occurred before the COVID-19 era. 21,28 The mean patient age was ∼40 years, which was common in women. Corticosteroid therapy was needed in 86% of the patients, and 27% subsequently had hypothyroidism. The present study showed characteristics similar to those of previous reports (Table 2). 21,28
One interesting finding from the case reviews is that SAT can be the initial and/or only COVID-19 presentation. Among the 27 cases assessed in a previous study, 1 patient had SAT that was diagnosed 47 days before the molecular diagnosis of COVID-19, without any respiratory symptoms or fever but with pneumonic infiltration on chest radiography. 15 Similarly, our study included four cases of SAT that were diagnosed 2 months before the molecular diagnosis of COVID-19. These results provide a clue to explaining the increased incidence of SAT without a molecular diagnosis of COVID-19.
If SAT is the initial or only presentation of COVID-19, the molecular diagnosis of COVID-19 can be underestimated in these patients. Because ACE receptor is expressed in the thyroid gland, 29 thyroid infection might precede respiratory infection, or infection might occur only in the thyroid gland, which can be considered an explanation for this phenomenon. However, we cannot conclude that this can fully explain the discordance between the increased annual SAT incidence and markedly less frequent cases of COVID-19-positive SAT. This finding suggests that a diagnostic approach to COVID-19 is needed for patients with SAT in the COVID-19 era. Previously, in general practice, identification of the causative viral organism was not performed in patients with SAT, given that most cases were self-limiting; however, COVID-19 has a potential risk for poor clinical outcomes.
Our study has several limitations. First, it is unknown whether other infectious diseases have decreased. The decline in other infectious diseases in 2020 is likely due to social distancing, hand hygiene, and wearing a facial mask. Conversely, other infectious diseases might have decreased because people did not visit the hospital with mild symptoms. Second, only a very small number of patients tested positive for COVID-19 because the retrospective study design prevented testing all patients with SAT. The COVID-19 test will be required for patients with suspected SAT since coronavirus is still prevalent.
Third, since patients with SAT were extracted from the claims data using the operation definition, it is impossible to see the laboratory results, and the risk of error due to claims data omission cannot be excluded. No cases of SAT-related hospitalization were observed between 2017 and 2020, possibly due to diagnostic code omission at the time of hospital admission and claim. In severe cases of SAT, hospitalization for heart failure or hepatic decompression is possible, 30 as in these cases, focus is more on serious medical problems than on SAT itself.
Eventually, additional studies on SAT occurrence in 2021 and additional validation with cohort data from other countries are needed to generalize our study results.
In conclusion, the annual SAT incidence in 2020 was higher than that in 2017 to 2019 period, while COVID-19-positive SAT was rarely documented. Since SAT-related viral infections markedly decreased in 2020, the increased SAT incidence in 2020 could be associated with COVID-19. Additionally, SAT can be the initial presentation of COVID-19; therefore, diagnostic tests for COVID-19 should be considered in patients with SAT during the COVID-19 pandemic.
Footnotes
Authors' Contributions
H.Y.A.: conception and design of the work (equal), collection of data (lead), interpretation of data and article writing (equal), revising the article (lead), and final review (equal). H.S.C.: statistical analysis of data (equal). S.H.: extraction and collection of data from the source database (lead). S.W.C.: conception and design of the work (equal), analysis and interpretation of data (equal), article writing (lead), and final review (equal).
Author Disclosure Statement
S.W.C. is a co-founder and CEO of Cellus, Inc. The remaining authors have no conflict of interest.
Funding Information
The present study was supported by the Korean Thyroid Association (KTA). This study used the National Health Insurance Database (NHIS-2021-1-762) created by the National Health Insurance Service (NHIS). The authors declare no conflict of interest with the NHIS.
Supplementary Material
Supplementary Figure S1
Supplementary Figure S2
Supplementary Figure S3
Supplementary Table S1
Supplementary Table S2