
Abstract
Background:
Untreated adult hypothyroidism may be associated with cognitive and emotional impairment, but the precise underlying neuropathological mechanism is unknown. We investigated the brain morphological and functional abnormalities associated with cognition and emotion in hypothyroidism.
Methods:
This is a cross-sectional observational study. Forty-four newly diagnosed adult hypothyroid patients and 54 well-matched healthy controls (HCs) were enrolled. All participants underwent three-dimensional T1-weighted imaging and resting-state functional magnetic resonance imaging (MRI). Morphological and seed-based functional connectivity (FC) analyses were performed to compare the intergroup differences. Neuropsychological tests, including the Montreal Cognitive Assessment (MoCA) Scale, 24-item Hamilton Depression Rating Scale (HAMD-24), and Hamilton Anxiety Rating Scale (HAMA) were administered. Thyroid function test and blood lipid levels were measured. Correlations were computed between neuropsychological and biochemical measures with neuroimaging indices. Sensitive morphological or functional neuroimaging indicators were identified using receiver operating characteristic (ROC) analysis.
Results:
Compared with HCs, hypothyroid patients demonstrated lower total and subdomain scores on the MoCA and higher HAMD-24 and HAMA scores. Morphological analysis revealed the hypothyroid patients had significantly reduced gray matter (GM) volumes in the right superior frontal gyrus, superior temporal gyrus, left dorsolateral superior frontal gyrus, middle frontal gyrus, and supplementary motor area as well as significantly increased GM volumes in the bilateral cerebellar Crus I and left precentral gyrus. Furthermore, seed-based FC analysis of hypothyroid patients showed increased FC between the right cerebellar Crus I and left precentral gyrus, triangular part of the inferior frontal gyrus, and angular gyrus of the inferior parietal lobe. The language scores of the MoCA were positively correlated with Jacobian values of the left supplementary motor area (r = 0.391, p = 0.046) and precentral gyrus (r = 0.401, p = 0.039). ROC analysis revealed FC value between cerebellar Crus I and angular gyrus could differentiate groups with relatively high accuracy (sensitivity: 75%, specificity: 77.8%, area under the curve: 0.794 [CI 0.701–0.888], p < 0.001).
Conclusions:
Untreated adult-onset hypothyroidism may be associated with impaired cognition and anxiety or depression. GM morphological alterations and FC of the cerebellum with subregions of the frontal and parietal lobes may represent key neuropathological mechanisms underlying the cognitive deterioration and mood dysregulation observed in hypothyroid adults. Clinical Trial Registration Number: chiCTR2000028966.
Introduction
Hypothyroidism, which is a global health problem with a prevalence of 1–2% in iodine-sufficient countries, 1 is characterized by elevated serum levels of thyrotropin (TSH) and decreased levels of thyroid hormones (THs). 2 Since THs are essential for maintaining normal mature brain function, 3 adult patients with hypothyroidism often exhibit neurological and psychiatric symptoms, which include impaired memory, inattention, and emotional dysregulation. 2,4,5 Hypothyroidism may be associated with an increased risk of developing dementia 6 and affective disorders, 7 which may substantially diminish quality of life. However, the exact neuropathophysiological mechanisms underlying cognitive and emotional impairment in hypothyroidism remain poorly understood.
The cerebral impairment of hypothyroidism is difficult to detect because of the lack of typical neurological manifestations and sensitive objective indicators. Magnetic resonance imaging (MRI) is a simple and noninvasive tool that can appraise subtle changes in structural alterations and functional activities in the brain. 8,9 MRI techniques have recently been applied to assess the brain changes associated with hypothyroidism. Morphological studies of hypothyroid patients have revealed a significant reduction of gray or white matter volume in the precentral and postcentral gyrus, inferior and middle frontal gyrus, occipital gyrus, temporal gyrus, hippocampus, and cerebellum. 10,11 Task-based functional MRI study has demonstrated task-induced deactivation within the default mode network (DMN) during working memory processing in hypothyroidism, suggesting a correlation between abnormal neural activity and hypothyroidism-related cognitive function. 12 Furthermore, a study using resting-state functional MRI (rs-fMRI) also reported that hypothyroid patients showed decreased functional connectivity (FC) among regions belonging to the resting-state networks, namely the right frontoparietal network, medial visual network, and motor network, suggesting corresponding neurocognitive changes in these regions. 13 However, these studies relied mainly on unimodal imaging techniques that reflected either morphological or functional changes. No studies to date have comprehensively combined structural and functional MRI methods to elucidate the precise pathophysiological mechanism underlying cerebral impairment in hypothyroidism.
Deformation-based morphometry (DBM) is a comparatively novel image analysis technique that captures regional structural changes in the entire brain by recording information about deformations, including not only local volume changes, but also deformation size, direction, and intensity. 14 Compared with voxel-based morphometry (VBM), DBM has benefited from improvements in image registration methods and is not necessarily dependent on the segmentation of tissues or brain parcellation, can match images locally based on similarities in contrast and intensity, making it more sensitive than VBM to subtle differences to provide a precise voxel-level assessment of atrophy. 14 –16 DBM has been applied to investigate abnormal morphological alteration in various cognitive disorders, such as Alzheimer's disease and Parkinson's disease, 17,18 however, it has not been used to evaluate the morphological alterations in hypothyroid patients so far.
In addition, rs-fMRI is an effective method of studying brain functional activities with blood oxygen level-dependent (BOLD) signals. 19 In contrast to task-based functional MRI, rs-fMRI allows to detect the intrinsic functional organization of the brain without the need for complex task designs or individual performance differences in finishing the task. 20 Moreover, while functional MRI during tasks may reveal cognition-related brain activity, functional MRI during wakeful rest can identify more directly endogenous processes. 21 Seed-based FC analysis is one of the most commonly used methods in rs-fMRI. It is a hypothesis/data-driven approach that correlates the BOLD time course in a predefined “seed” region with the time course from all other brain regions. It is suitable for functional analysis of the human brain because of its simplicity and directness. 19
Accordingly, this study applied DBM based on three-dimensional T1-weighted imaging (3D T1WI) combined with FC analysis based on rs-fMRI to explore whether patients with adult-onset hypothyroidism exhibit morphological and functional abnormalities. Given the exploratory nature of this study, we hypothesized that morphological or functional alterations may exist in the hypothyroid brain, especially the frontal lobe and cerebellum, because these regions contain abundant TH receptors 22,23 and are closely related to higher-order cognitive or emotional processing. 24 –27 We additionally hypothesized that alterations in these regions would be correlated with the decreased cognitive function and/or increased anxious/depressed symptoms observed in these patients.
Materials and Methods
Participants
From September 2019 to December 2021, 52 newly diagnosed untreated patients with overt hypothyroidism were recruited from the Outpatient Department of Endocrinology, Gansu Provincial Hospital. Over the same period, 64 healthy controls (HCs) matched for age, sex, and education level, were also recruited from the local community. All participants were of Chinese Han ethnicity.
The inclusion criteria of the hypothyroid group were as follows: (1) a clinical diagnosis of hypothyroidism based on the Guidelines for Diagnosis and Management of Hypothyroidism in adults (2017 Edition). 28 The specific biochemical criteria were an elevation of serum TSH levels above the reference range (0.35–4.94 mIU/L) and reduced serum-free thyroxine (fT4) levels below the reference value (9.01–19.05 pmol/L); (2) age 18–60 years; and (3) a minimum education level of 6 years (to ensure participants could independently complete neuropsychological scales).
The exclusion criteria were as follows: (1) history of neurological or psychiatric diseases (e.g., multiple sclerosis, epilepsy, dementia, major depression, and schizophrenia); (2) history of brain diseases (e.g., stroke, brain tumors, and traumatic brain injury); (3) prior endocrine disorders (e.g., diabetes mellitus and prediabetes) or nonthyroid autoimmune disease; (4) cardiovascular diseases or some other major chronic diseases; (5) severe visual impairment or severe hearing impairment; (6) history of alcohol or psychoactive substances abuse; (7) current pregnancy, lactation, or oral contraceptive use in women; (8) contraindications to MRI examination (e.g., claustrophobia, placement of cardiac pacemakers, neurostimulators, syringe injection pumps, cochlear implants, or any metal implant); (9) scores <24 points on the Mini-Mental State Examination (MMSE) 29 ; and (10) left-handedness or ambidexterity. The HCs had no history of thyroid diseases nor current somatopathy and met inclusion criteria (2–3) and all exclusion criteria.
This study was approved by the Medical Ethics Committee of Gansu Provincial Hospital (Approval No. 2019-196). Informed consent was obtained from all participants.
Clinical variables and neuropsychological tests
For all subjects, medical history and all current medications were recorded in questionnaires. Venous blood was collected after overnight fasting for thyroid function and blood lipid tests. Thyroid function tests included serum triiodothyronine (T3), thyroxine (T4), free triiodothyronine (fT3), fT4, and TSH, which were measured using chemiluminescent microparticle immunoassay (Abbott Laboratories). Blood lipids tests included serum triglyceride (TG), cholesterol, low-density lipoprotein cholesterol (LDL-C), and high-density lipoprotein cholesterol, measured using the Ci 1620 automatic biochemical immune analysis system (Abbott Laboratories). The detailed assay characteristics are presented in the Supplementary Methods section.
All participants underwent neuropsychological testing using the following instruments: the Chinese version of MMSE 29 was used to evaluate the general cognitive state of the patients. Scores range from 0 to 30, with lower scores indicative of a greater degree of cognitive impairment. Participants with MMSE scores <24 points were considered consistent with cognitive impairment 30 and were thus excluded. The Montreal Cognitive Assessment (MoCA, Beijing version) 31 scale was applied for the rapid evaluation of seven cognitive subdomains, namely visuospatial/executive function, naming, memory and delayed recall, attention, language, abstraction, and orientation. The total score of MoCA was 30 points with a score of <26 thought to signify mild cognitive impairment and above; otherwise, it indicated normal cognitive function. For participants receiving ≤12 years of education, their score was adjusted by addition of 1 point to reduce a possible education level bias effect. 32 Depression and anxiety symptoms were evaluated using the 24-item Hamilton Depression Rating Scale (HAMD-24) 33 and Hamilton Anxiety Rating Scale (HAMA), 34 with HAMD-24 scores <8 and HAMA scores <7 considered to be normal. All neuropsychological tests, which were conducted in Chinese on the day of the MRI scan, were performed by clinicians with specialty training in the neuropsychological scale assessment under the guidance of the chief physician from the department of psychiatry. Only one HC participant had missing HAMD-24 and HAMA scale data on the day of the MRI scan.
MRI image acquisition
A 3.0 Tesla Magnetom Skyra scanner (Siemens Healthcare, Erlangen, Germany) with a 32-channel head coil was used to obtain brain MRI images. Routine scans (T1WI, T2WI, and T2-FLAIR) were performed to exclude neurological or structural abnormalities. All subjects then underwent rs-fMRI and high-resolution 3D T1WI scanning, the scanning parameters are summarized in the Supplementary Table S1.
DBM analysis
First, the original Digital Imaging and Communications in Medicine file was converted to Neuroimaging Informatics Technology Initiative (NIfTI, file extension .nii), and then each T1WI image was manually checked and anterior and posterior commissures (AC and PC) of the corpus callosum were manually identified in the T1 weighted anatomical images of each participant and the anatomical images were rotated to the AC-PC plane. Computational Anatomy Toolbox (CAT12) running within Statistical Parametric Mapping (SPM12) was used to preprocess 3D T1WI images.
The preprocessing steps included denoising, correction for intensity inhomogeneity, and linear intensity scaling. Each participant's map of the spatial deformation of each voxel was created using the nonlinear transformation information of structural images from individual space to the typical Montreal Neurological Institute space. The deformation was used to conduct statistical analysis and to quantify the map of local volume changes. 35 Finally, a 6-mm full-width-half-maximum Gaussian kernel was used to smooth the DBM data.
Preprocessing of resting-state fMRI data
The preprocessing of rs-fMRI data was performed using the DPABI V5.1 36 based on the SPM12 on the MATLAB R2018a platform. Detailed steps of rs-fMRI data preprocessing can be found in the Supplementary Methods section.
Seed-based FC analysis
DPABI V5.1 software was used for seed-based FC analysis. The seed regions were defined using the peak values of the significant brain voxels based on the results of the DBM analysis (Fig. 2). Detailed information about the seed-based FC analysis is showed in the Supplementary Methods section.
Statistical analysis
Group differences in demographic, clinical variables, and neuropsychological scores were analyzed using SPSS 25.0 software. The two-sample t-test was performed for normally distributed continuous variables, Mann–Whitney U test for non-normally distributed continuous variables, and chi-square test for categorical variables. In addition, we also used a nonparametric approach (chi-square) to compare intergroup differences for MoCA, HAMD-24, and HAMA scores. p < 0.05 was considered statistically significant and p < 0.007 was considered a significant difference in MoCA subdomain scores after Bonferroni correction.
First, the Jacobian values from the gray matter (GM) deformation infographic were extracted as morphological parameters for comparing the intergroup difference using the two-sample t-test in the SPM12 statistical module. The voxel threshold was set at p < 0.001 to identify statistically different sets of pixels clusters, with age, sex, and educational level serving as covariates for whole-brain analysis. Second, seed-based FC values were tested using the two-sample t-test, where age, sex, educational level, and head movement parameters were included as covariates in the group comparison. Gaussian Random Field (GRF) theory was used for multiple comparison correction (voxel-wise of p < 0.001 and cluster-wise of p < 0.05). We conducted a post hoc power analysis using G*Power (V3.1.9.7), 37 with an alpha level of 0.05, one-tailed using the mean and standard deviation of abnormal brain regions.
Once clusters with significant intergroup differences were identified, the Jacobian and FC values were extracted from the hypothyroid group to further calculate the two-tailed Spearman's correlation coefficients with thyroid function, blood lipid indicators, and neuropsychological test scores, respectively, and false discovery rate (FDR) correction were performed with R language (V4.1.1). Moreover, a receiver operating characteristic (ROC) analysis was also applied to assess the positive and negative predictive values for cerebral impairments in hypothyroidism.
Results
Clinical variables and neuropsychological tests
Eight hypothyroid patients and 10 HCs were excluded due to excessive head movement (mean frame-wise displacement >0.2 mm) 38 and/or incomplete images (rs-fMRI image slices ≠33), for a final sample of 44 in the hypothyroid and 54 in the HCs group (Fig. 1). The groups did not differ in age, sex, and education level, but they did significantly differ in thyroid function indicators, blood lipid indicators, and neuropsychological test scores (Table 1). Neuropsychological test results indicated that although MMSE scores of all participants were within the normal range (>24), 16 of 44 (36.4%) hypothyroid patients exhibited MoCA total scores <26. Furthermore, 19 of 44 (43.2%) and 13 of 44 (29.5%) hypothyroid patients exhibited depressive or anxious symptoms, respectively. In contrast, none of the HCs group showed either cognitive or depressive/anxious symptoms. The group differences are shown in Tables 2–4.

A flowchart shows participant selection. HC, healthy control; mFD, mean frame-wise displacement; rs-fMRI, resting-state functional magnetic resonance imaging.
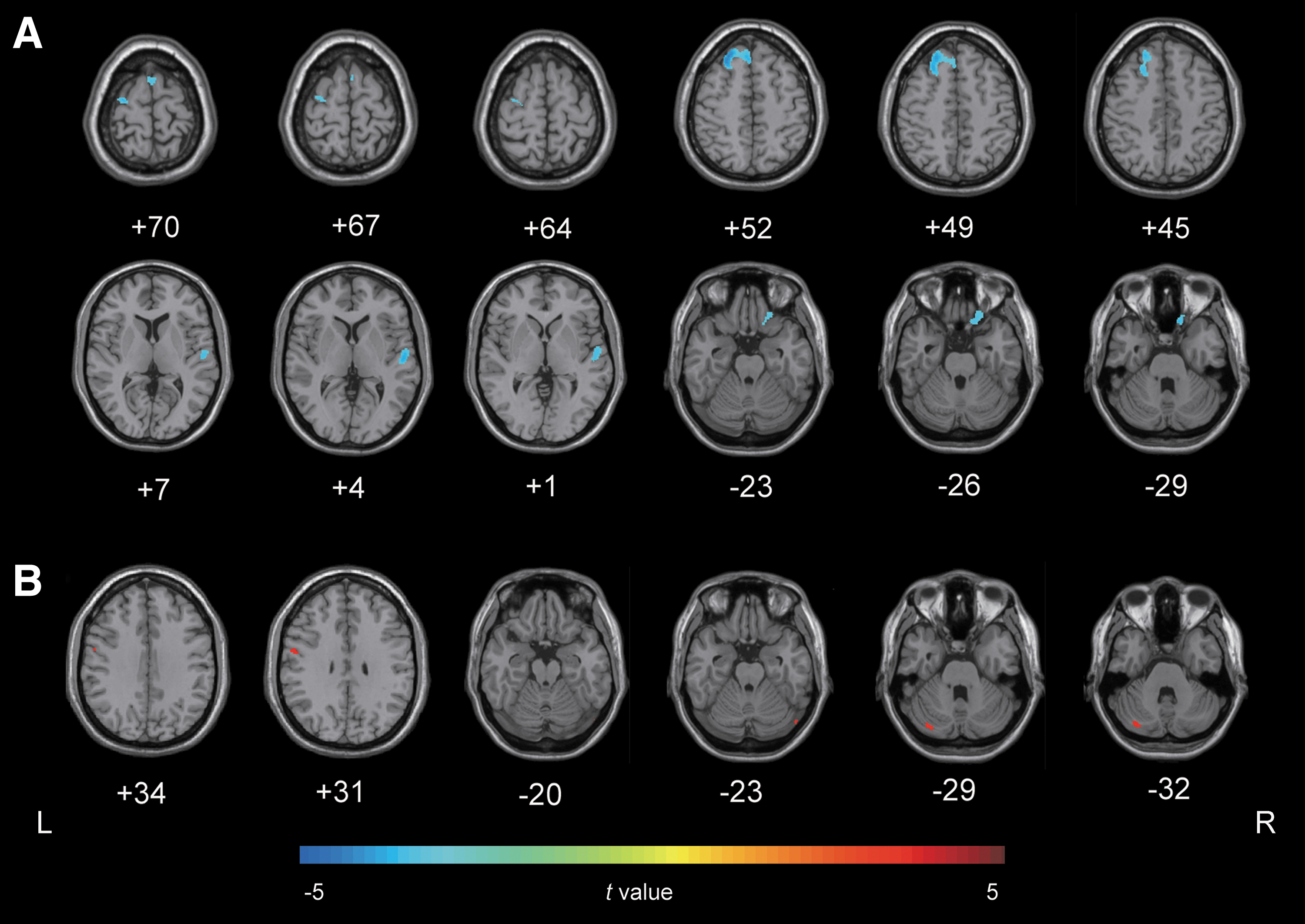
Regions showing significantly altered GM volume in the hypothyroid group compared with HCs. (
Demographics, Clinical Variables, and Neuropsychological Tests of Hypothyroid Patients and Healthy Controls
Represents the χ2 value (chi-square test).
Represents the t value (two-sample t-test).
Represents the z value (Mann–Whitney U test).
Indicates that in the hypothyroid and HC group, there were 17 and 12 participants with an education level ≤ 12 years respectively, therefore, 1 point was added to their MoCA total score reduce the possible education level bias effects.
Indicates that only one HC participant had missing HAMD-24 and HAMA scale. Since the data did not obey the normal distribution, the missing data were supplemented by the median.
p < 0.05 is considered statistically significant.
p < 0.007 is considered significant after Bonferroni correction.
CHOL, cholesterol; fT3, free triiodothyronine; fT4, free thyroxine; HAMA, Hamilton Anxiety Rating Scale; HAMD-24, 24-item Hamilton Depression Rating Scale; HC, healthy control; HDL-C, high-density lipoprotein cholesterol; IQR, interquartile range; LDL-C, low-density lipoprotein cholesterol; MMSE, Mini-Mental State Examination; MoCA, Montreal Cognitive Assessment Scale; OH, overt hypothyroidism; SD, standard deviation; T3, triiodothyronine; T4, thyroxine; TG, triglyceride; TSH, thyrotropin.
Comparison of the Montreal Cognitive Assessment Result Between Hypothyroidism and Healthy Control Group with Chi-Square Test
p < 0.05 is considered statistically significant.
OH, overt hypothyroidism.
Comparison of the 24-Item Hamilton Depression Rating Scale Result Between Hypothyroidism and Healthy Control Group with Chi-Square Test
p < 0.05 is considered statistically significant.
Comparison of the Hamilton Anxiety Rating Scale Result Between Hypothyroidism and Healthy Control Group with Chi-Square Test
p < 0.05 is considered statistically significant.
Intergroup morphological differences in DBM
Compared with HCs, the hypothyroid group had reduced GM volumes in the left middle frontal gyrus, left dorsolateral superior frontal gyrus, left supplementary motor area, orbital part of the right superior frontal gyrus, and right superior temporal gyrus (voxel-p < 0.001, cluster size = 100, uncorrected). In contrast, the hypothyroid group had increased GM volumes in the bilateral cerebellar Crus I and left precentral gyrus (voxel-p < 0.001, cluster size = 5, uncorrected) (Table 5 and Fig. 2). The results of post hoc power analysis of the above abnormal brain regions are presented in the Supplementary Results section and Supplementary Table S7.
Brain Regions with Altered Gray Matter Volume in Hypothyroid Patients Compared with Healthy Controls
OH<HC, brain regions of reduced gray matter volume; OH>HC, brain regions of increased gray matter volume. X, Y, and Z, coordinates of primary peak locations in MNI space. Peak T value, the T value of the voxel with maximum effect estimate within the identified cluster. The threshold was set at p < 0.001 (uncorrected).
Cerebellum_Crus I_L, left cerebellar Crus I; Cerebellum_Crus I_R, right cerebellar Crus I; Frontal_Mid_L, left middle frontal gyrus; Frontal_Sup_L, left dorsolateral superior frontal gyrus; Frontal_Sup_Orb_R, orbital part of the right superior frontal gyrus; MNI, Montreal Neurological Institute; Precentral_L, left precentral gyrus; Supp_Motor_Area_L, left supplementary motor area; Temporal_Sup_R, right superior temporal gyrus.
Intergroup differences in seed-based FC
Compared with the HCs group, the hypothyroid group exhibited increased FC between the right cerebellar Crus I and left precentral gyrus, triangular part of the inferior frontal gyrus, and angular gyrus of the inferior parietal lobe (GRF correction, voxel-p < 0.001, cluster-p < 0.05) (Table 6 and Fig. 3). The results of post hoc power analysis of these brain regions are presented in the Supplementary Results section and Supplementary Table S7. No significant FC alterations were observed between the groups in the remaining regions of interest, namely the orbital part of the right superior frontal gyrus, right superior temporal gyrus, left middle frontal gyrus, left dorsolateral superior frontal gyrus, left supplementary motor area, left cerebellar Crus I, and left precentral gyrus.
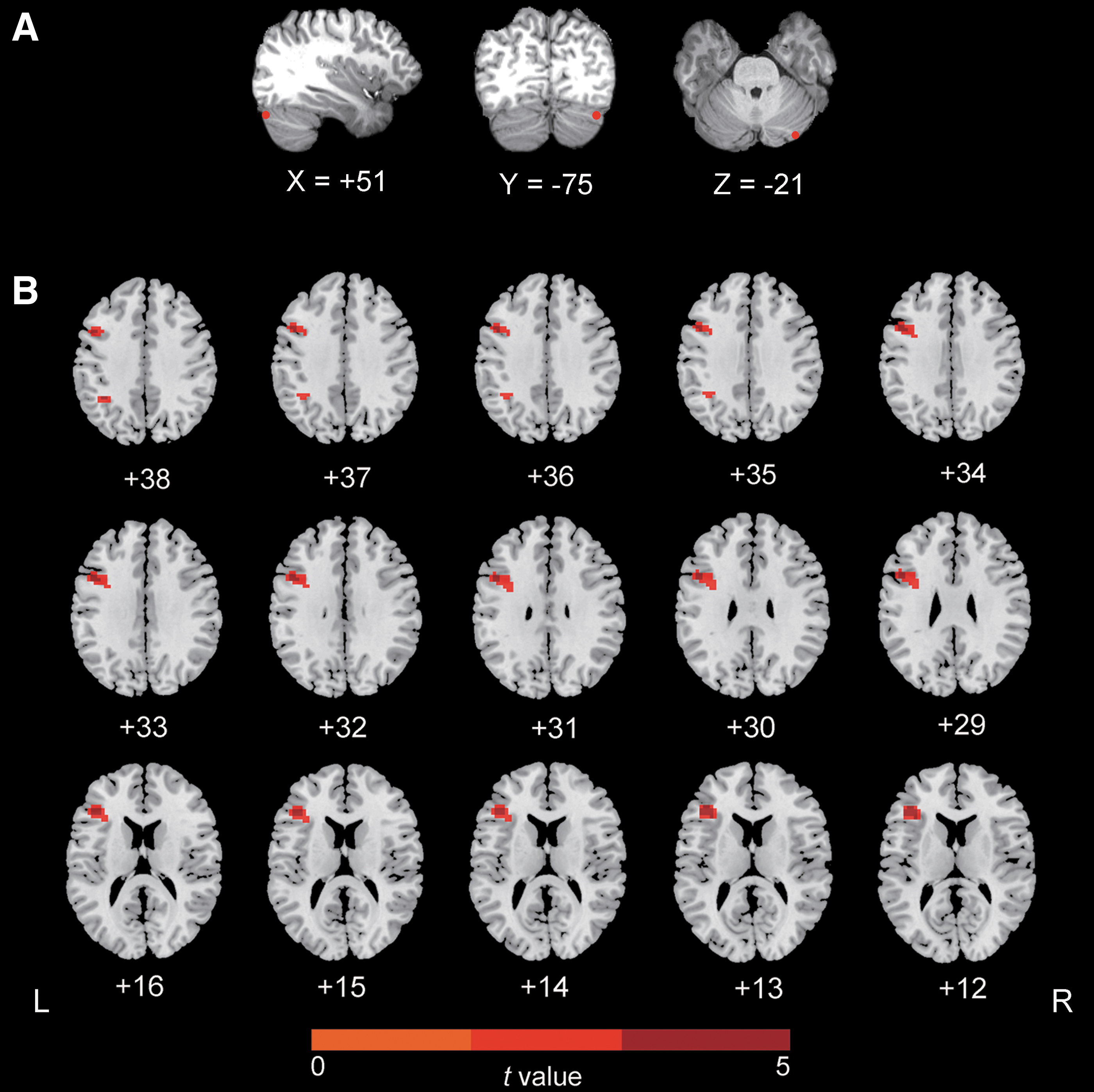
Regions showing significantly increased FC with the right cerebellar Crus I in the hypothyroid group compared with HCs. (
Brain Regions with Increased Functional Connectivity in Hypothyroid Patients Compared with Healthy Controls
X, Y, and Z, coordinates of primary peak locations in MNI space. Peak T value, the T value of the voxel with maximum effect estimate within the identified cluster. The threshold was set at p < 0.001 (GRF correction).
Frontal_Inf_Tri_L, triangular part of the left inferior frontal gyrus; GRF, Gaussian Random Field; Parietal_Inf_L, angular gyrus of the left inferior parietal lobe.
Correlations between significantly altered brain regions with clinical variables and neuropsychological scores
Language scores on the MoCA were positively correlated with morphological Jacobian values of the left supplementary motor area (r = 0.391, FDR-corrected two-tailed p-value = 0.046) and the left precentral gyrus (r = 0.401, FDR-corrected two-tailed p-value = 0.039) (Fig. 4 and Supplementary Tables S2–S4). No other significant correlation was found between the Jacobian values or FC values of other significant altered brain regions and thyroid function, blood lipids levels, MoCA, HAMD-24, or HAMA scores.
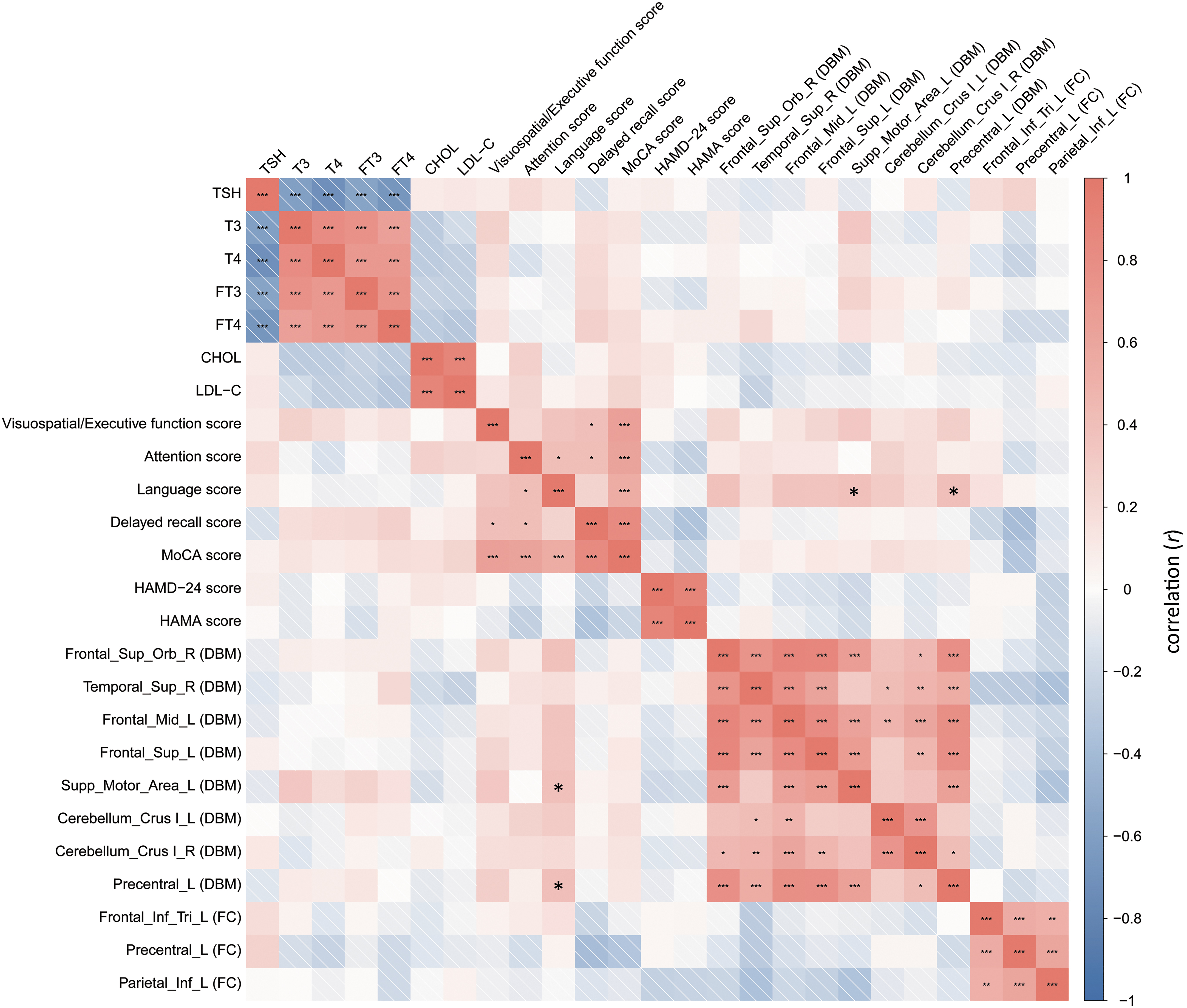
Correlations between the abnormal brain regions in hypothyroid patients and neuropsychological test scores or clinical variables. The language scores were positively correlated with morphological Jacobian values of left supplementary motor area (r = 0.391, p = 0.046) and left precentral gyrus (r = 0.401, p = 0.039), respectively.
Correlations between neuropsychological scores and clinical variables
As shown in Figure 4 and Supplementary Tables S5 and S6, there was no significant correlation between neuropsychological test scores and thyroid function tests (|r| < 0.3, FDR-corrected two-tailed p-value >0.05) or blood lipid levels (|r| < 0.3, FDR-corrected two-tailed p-value >0.05).
ROC results
The sensitivity and specificity of morphological and functional alterations of the brain in hypothyroid patients and HCs are displayed in Table 7 and Figure 5. Among them, the FC value between the right cerebellar Crus I and left angular gyrus demonstrated the highest area under the curve (AUC) value of 0.794 (p < 0.001 [CI 0.701–0.888]), with a sensitivity of 75% and specificity of 77.8%.
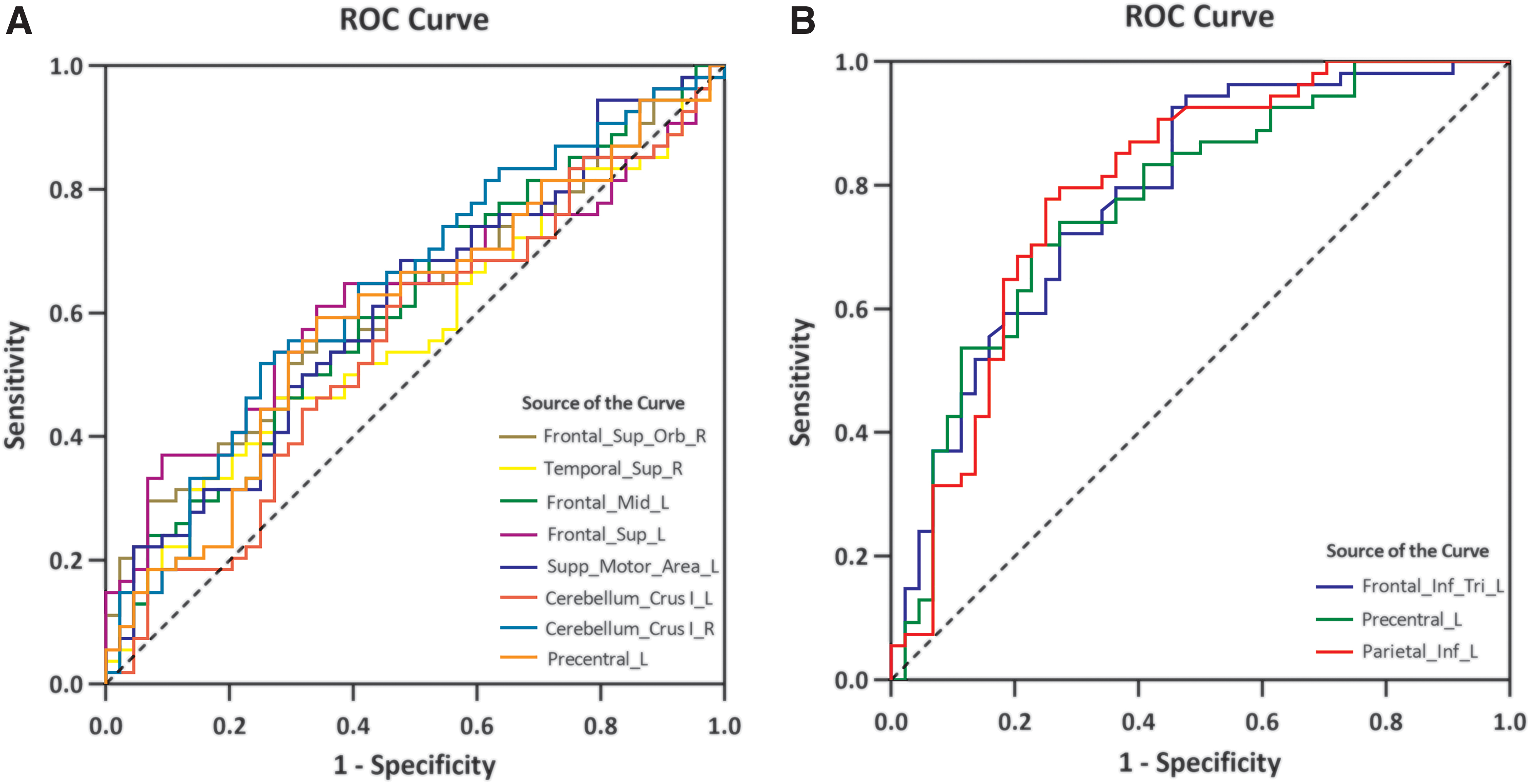
ROC curve analysis of the cerebral morphological and functional alterations in hypothyroid patients and HCs.
Results of Receiver Operator Characteristic Curve Analysis of the Parameters of Cerebral Morphological and Functional Alterations
AUC, area under the curve; CI, confidence interval; DBM, deformation-based morphometry; FC, functional connectivity.
Discussion
In this study, we investigated the hypothyroid-related cerebral morphological and functional alterations using a combination of DBM and resting-state seed-based FC analytic approaches. Our results revealed that hypothyroid patients exhibited reduced GM volumes in the orbital part of the right superior frontal gyrus, left dorsolateral superior frontal gyrus, left middle frontal gyrus, left supplementary motor area, and right superior temporal gyrus and enlargement of the bilateral cerebellar Crus I and left precentral gyrus. The additional seed-based FC analysis provided more details about abnormal connections between the right cerebellar Crus I and the left precentral gyrus, triangular part of the inferior frontal gyrus, and angular gyrus. Furthermore, significant correlations were observed between the abnormal brain regions and language scores on the MoCA. Notably, the hypothyroid patients exhibited lower cognitive scores, and higher depressive and anxious scores, which might reflect a complicated mechanism involving a metabolic disturbance as well as abnormalities in the morphology and function of the brain.
Analyses of clinical information and laboratory data revealed a common feature of hypothyroid patients, namely blood lipid metabolism disorders in addition to elevated TSH and decreased THs. TSH affects brain function and plays a crucial role in cognitive function, whereby higher TSH levels are linked to poorer memory, visuospatial/visual construction skills, and slower psychomotor speed. 39,40 Furthermore, these findings are consistent with a postmortem study demonstrating the presence of TSH receptor (TSHR) in large neuronal cell bodies in limbic regions of the human brain. 41 Also in TSHR knockout mice, TSH-TSHR dysregulation led to poorer performance on spatial learning and memory tasks, 42 as well as behavioral and neurological phenotypes of attention-deficit/hyperactivity disorder, related to monoaminergic nervous systems. 43 These findings could potentially suggest that TSH may influence brain structure or function related to cognition and mood, to some extent.
Decreased THs levels are involved in the pathophysiological mechanism of neurocognitive function. As reported in the literatures, in the developing brain, THs could regulate the balance of production of oligodendrocytes and astrocytes; 44 moreover, in the mature brain, THs are also essential for adult neurogenesis and the maintenance of normal brain function. 3 The deficiency of THs in adulthood could affect cognitive function. Indeed, a postmortem study showed low levels of serum T3 in patients with a high burden of neurofibrillary tangles. 45 Reduced THs could result in hyperphosphorylation of tau protein, increased levels of pro-inflammatory cytokines, 46 and affected glutamate synthesis 47 in the hippocampus, all of which are associated with impaired spatial memory, learning, and attention, as well as influenced hippocampal synaptic plasticity.
Dyslipidemia, as noted in our hypothyroid patients, may be involved in the pathogenesis of cognitive impairment. The metabolic disorder of total cholesterol (TC) and TG could also interfere with normal neurological function, thereby significantly altering the equilibrium of Aβ production, metabolism, and clearance, leading to impairing cognitive function; 48,49 in particular, increased LDL-C, TC, and TG levels were associated with decreased executive function, attention, and processing speed. 50 Thus, alterations of THs levels and blood lipid metabolism disorders may contribute to cognitive impairment in hypothyroidism.
The frontal lobe is thought to be responsible for higher-order cognitive function 51 and emotional processing 52 and is widely connected to the superior temporal gyrus, 53 a crucial structure in more basic aspects of cognitive function. 54 –56 In this study, reduced GM volumes were observed primarily in the frontal lobe and superior temporal gyrus in patient group. A previous VBM-based investigation also revealed a significant reduction in white matter volumes in the inferior/middle frontal gyrus and right temporal gyrus in hypothyroid patients, 10 supporting our findings.
Moreover, significantly decreased regional cerebral blood flow in the frontal lobe and temporal lobe were found by using neuroimaging techniques, 57,58 which could be the pathological basis for the reduction of GM volumes in the frontal or temporal lobe of untreated hypothyroidism. A magnetic resonance spectroscopy study revealed that TH replacement could increase the energy metabolism as measured by the increased ratio of phosphocreatine to inorganic phosphate in the frontal cortex of hypothyroid patients. 59 This may suggest that the frontal cortex is sensitive to THs levels, further supporting our results.
Furthermore, the alteration of GM volumes in the frontal cortex correlated with the decreased language scores in this study, suggesting a potentially important role of the frontal lobe in the higher-order cognitive processing. Taken together, these findings may help to explain the cognitive decline and emotional dysregulation associated with hypothyroidism. However, contrary to our expectations, no correlations were observed between the altered frontal lobe and the level of TSH or THs, possibly related to the relatively small sample size. Therefore, studies with larger sample sizes are required to verify our findings.
Accumulating evidence and recent data suggest that the cerebellum plays an important role in cognitive and emotional processes in addition to fine motor coordination and balance. Herein, increased GM morphology of bilateral cerebellar Crus I was demonstrated, and increased FC between the right cerebellar Crus I and left precentral gyrus, triangular part of the inferior frontal gyrus, and angular gyrus were found in hypothyroidism, indicating the involvement of the cerebellar Crus I in the pathophysiological processes of the hypothyroid state.
A study of hypothyroid mice and rats showed that deficiency of THs could hinder the differentiation of Purkinje cells and the migration of granular cells in the cerebellum. 60 Moreover, TH receptors TRα1/TRβ1 are continuously expressed in pyramidal and Purkinje cells in the adult cerebellum. 61 The biological effects of THs in a mature brain could be exerted through the control of the expression of specific genes mediated by TH receptors. 62
In addition, clinical MRI studies have identified changes in cerebellar GM volume 10 and abnormal FC between the cerebellum and DMN (the medial prefrontal cortex, the precuneus, and the bilateral angular gyri) 63 in adults with hypothyroidism, which is consistent with our findings. Notably, the cerebellum participates in the prefrontal–thalamic–cerebellar circuit, 64 which plays a key role in the higher-order cognitive and affective processing. The cerebellar Crus I is closely connected to the DMN in humans, 65 which has been confirmed in studies investigating major depressive disorder 66 and bipolar disorder. 67,68
The altered morphology and FC of cerebellar Crus I, as determined in this study, indicate that disrupted morphology and cerebellar–cerebral connectivity could be associated with hypothyroid-related cognitive deterioration. Interestingly, the FC value between the right cerebellar Crus I and left angular gyrus displayed the highest AUC in the ROC analysis, which indicates a potentially valuable imaging biomarker for early detection of cognitive decline in hypothyroidism.
While studies focusing on patients with depression or anxiety have reported that an altered cerebellum is may be associated with emotional symptoms and is a key structure involved in mood regulation, 69,70 we did not observe any significant correlations between cerebellar abnormalities and the anxiety or depression scores. Thus, it is unclear whether the observed cerebellar changes may be attributed to the hypothyroidism or the adverse emotion and larger studies needed to examine this issue.
The main strength of our study is the combination of morphological and functional approaches with highly homogeneous newly diagnosed adult-onset hypothyroid patients. However, our study also has several limitations: First, the sample size is limited, although it is comparable with or larger than that of prior research using similar methodology. Generally, the reliability, sensitivity, and positive predictive value of findings obtained with a sample size of at least 40 participants per group may be considered stable in rs-fMRI research. 71 Second, this is a cross-sectional study from the time of diagnosis before treatment. Therefore, we do not know the treatment outcomes with levothyroxine therapy and future longitudinal studies are needed.
Third, we were unable to determine the relationship between the disease duration and the brain alterations due to hypothyroidism. Fourth, the heterogeneity of the underlying causes of hypothyroidism may affect the results, although the majority of patients in this study had Hashimoto's thyroiditis. Fifth, the resting state was difficult to control, even though participants were instructed to try not to focus on any specific matter while performing rs-fMRI scanning. Sixth, due to the exploratory aims of this study, DBM analysis was undertaken without corrections being made for multiple comparisons. Seventh, since language scores on the MoCA were tested based on repeated presentation of sentences, which might involve the motor component, the effects on cognition should be interpreted cautiously. Unexpectedly, we did not observe any significant correlations between the MoCA subscales and the abnormal brain regions except the language scores. The correlation results of our study should be interpreted with caution and may not directly infer causality. Eighth, although the cognitive rating scale, MoCA scale, used in this study could directly assess the general cognitive function, it cannot adequately describe various aspects of the cognitive domain, such as semantic memory, episodic memory, working memory, and processing speed. Subsequent studies should assess cognitive status more comprehensively.
Ninth, we could not determine whether the abnormalities in brain regions were attributable to hypothyroidism itself or, in part, due to the anxious/depressive symptoms; therefore, future research should include a comparison group of depressed individuals without hypothyroidism. Tenth, the partially missing neuropsychological scale data in the HCs group were supplemented with the median since they did not follow normal distribution. And finally, task-based functional MRI was not performed in this study and future studies with task-based functional MRI would be of interest.
In conclusion, hypothyroid patients may be at risk of cognitive deterioration, depression, and anxiety. In this study, which combined rs-fMRI and 3D T1WI techniques, we observed morphological GM volume alterations in the frontal, temporal lobe, and cerebellum, as well as impaired cerebellar–cerebral FC, and correlates with cognitive subdomain function in hypothyroid patients. Moreover, the findings from the ROC analysis indicated the FC value between the cerebellar Crus I and the angular gyrus might serve as a potential biomarker for the early detection of brain abnormality in hypothyroidism. These abnormal brain regions have the potential as regions of interest for further investigation or candidate therapeutic targets for cerebral impairments in hypothyroid patients in the future. Overall, our findings provide valuable insights into understanding the pathophysiological mechanism of the cognitive and emotional deterioration associated with adult-onset hypothyroidism.
Footnotes
Acknowledgments
We thank the participants and investigators in this study.
Authors' Contributions
Writing—original draft, writing—review and editing, and formal analysis by W.S. Study idea and design, and writing—review and editing by L.Z. Formal analysis by S.B. Data curation by R.Q., T.Z., and Y.H. MRI data processing by J.C. and J.T. Data collection by C.C., Q.S., G.Q., and F.S. Study idea and design by L.T.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This study was supported by the National Natural Science Foundation of China (No. 82060152), the Natural Science Foundation of Gansu Province (20JR5RA156 and 21JR7RA593), and the “Young Scholars in Western China” project of The Chinese Academy of Sciences in 2020.
Supplementary Material
Supplementary Data
Supplementary Table S1
Supplementary Table S2
Supplementary Table S3
Supplementary Table S4
Supplementary Table S5
Supplementary Table S6
Supplementary Table S7