
Abstract
Background:
More than 40 years have passed since the introduction of newborn screening (NBS) for congenital hypothyroidism (CH), and many early diagnosed patients have reached adulthood. Their thyroid morphology and function have been little studied. This cross-sectional, observational study was conducted to characterize the thyroid morphology and function of adult CH patients diagnosed in the framework of NBS for CH.
Methods:
A total of 103 adult CH patients born after 1979 were enrolled at Ito Hospital, Tokyo, Japan, and were classified into Goiter, Normal gland, and Dysgenesis groups based on ultrasonographic findings. For 60 patients, genetic analysis was performed. Thyroid function test results and the proportion of patients with thyroid nodules were compared among the three groups and between 56 female CH patients and 168 non-CH women matched for thyrotropin levels.
Results:
A significantly low serum free triiodothyronine/free thyroxine ratio (0.22) was observed in the Dysgenesis group. Thyroid nodules were detected in 14.3% (8/56) of female CH patients, more frequently than in non-CH women. Thyroid nodules were detected most frequently in the Goiter group (71%, 10/14). Genetic defects were identified in 89% (8/9) of patients belonging to the Goiter group, including thyroglobulin defect (33%, 3/9), thyroid peroxidase defect (33%, 3/9), and dual oxidase 2 defect (22%, 2/9).
Conclusions:
Our results suggest that adults with thyroid dysgenesis on levothyroxine replacement therapy have relative triiodothyronine deficiency. Most adults with goitrous CH have genetic dyshormonogenesis. They are at high risk of developing thyroid nodules. Our findings support the current guideline recommendation that CH patients with dyshormonogenesis should undergo periodic thyroid ultrasonography.
Introduction
Congenital hypothyroidism (CH) occurs in 1 in 2000–3000 births worldwide. 1,2 The severity of CH ranges widely, including transient disease, permanent disease with preserved thyroid hormone levels, and permanent disease with thyroid hormone deficiency (overt CH). In Japan, permanent overt CH, defined as elevated thyrotropin (TSH) levels accompanied by low free thyroxine (fT4) levels at age 2 years or older, is estimated to occur in ∼1 in 7000 births. 3 Thus, it is estimated that 2–4% of adult patients with a diagnosis of overt hypothyroidism may have CH.
In Japan, newborn screening (NBS) for CH was initiated in 1979. With the implementation of early diagnosis and treatment, the number of CH cases with growth restriction and intellectual disability decreased dramatically. Now that CH patients are active in society without apparent disabilities, long-term conditions such as quality of life and late complications have become the focus of much attention. There were several reports of population-based cohort studies of adult CH cases born after the NBS era. 4 –6 These questionnaire-based studies showed that most adult CH patients are well integrated into society with respect to education and employment. However, there is little information about the medical and biological status of the thyroid glands of adult CH patients.
Based on thyroid morphology, CH cases can be classified into three major categories: thyroid dysgenesis, thyroid dyshormonogenesis, and CH with an anatomically normal gland. Thyroid dysgenesis, the term used to describe abnormalities in thyroid organogenesis, includes aplasia, hypoplasia, ectopia, and hemiaplasia of the thyroid. Thyroid dysgenesis is the relatively common form of permanent overt CH. 7,8 The majority of thyroid dysgenesis cases is sporadic, indicating that Mendelian disorders are not the principal pathogenesis. Nonetheless, genetic defects involving TSH receptor 9 and thyroid-specific transcription factors such as PAX810 and NKX2-111 have been described as exceptional cases. Thyroid dyshormonogenesis is the term used to describe inborn errors of thyroid hormone biosynthesis. The main causes of thyroid dyshormonogenesis are Mendelian disorders, and the involved genes include TG, TPO, DUOX2, DUOXA2, SLC5A5, SLC26A4, SLC26A7, and IYD. 12,13
Most patients with thyroid dyshormonogenesis have a goiter due to the proliferation of thyroid follicular cells stimulated by elevated TSH. Although rare, cases of nongoitrous CH and thyroid hypoplasia with genetic defects compatible with thyroid dyshormonogenesis have been reported. 14 Another hallmark of thyroid dyshormonogenesis is high serum levels of thyroglobulin (Tg), which is related to increased thyroid gland volume. Exceptionally, serum Tg levels are low in patients with Tg defects. 14 There have been reports of differentiated thyroid carcinomas in patients with TG variants, 15 TPO variants, 16 and SLC26A4 variants. 17 In the 2020–2021 consensus guidelines for CH by an ENDO-European Reference Network Initiative, periodic thyroid ultrasound screening in patients with thyroid dyshormonogenesis was recommended. 1
This report describes a cohort of adult CH patients followed at Ito Hospital, one of the largest thyroid clinics in Japan. Function and morphology of the thyroid gland were evaluated in a systematic manner, and comprehensive genetic analysis was performed in about 60% of the study participants. The aim was to classify adult CH patients (who were diagnosed via NBS and treated appropriately) according to thyroid morphology (goiter, normal, and dysgenesis), characterize thyroid gland anatomy and physiology, and identify a subgroup in which thyroid ultrasonography would be particularly useful in follow-up.
Materials and Methods
Patients
In Tokyo, NBS for CH through an enzyme immunoassay-based TSH measurement was introduced in 1979, and the measurement method was changed to an enzyme-linked immunosorbent assay in 1987. Filter paper blood spot samples are collected on days 5–7 postpartum. Neonates with a blood-spot TSH level >25 mU/L are immediately referred to a regional medical facility, whereas neonates with a TSH level of 9–25 mU/L are retested for TSH. If the blood-spot TSH level is >12 mU/L in a retested sample, the neonate is referred to a regional medical facility. In a national survey of NBS for CH conducted between 1994 and 1999, the average age of the first visit to a regional medical facility was 17.3 days. 18
Before 2014, the Japanese clinical guideline for CH 19 and textbooks recommended an initial levothyroxine (LT4) dose of 10 μg/(kg·d). Although medical records were not available for each participant in this study, it is assumed that LT4 replacement therapy was initiated at 10 μg/(kg·d) in the majority of patients.
In the present retrospective, cross-sectional, and observational study, adult CH patients who were born after 1979 (the year NBS started in Japan) and visited Ito Hospital (Tokyo, Japan) once or more at age of 20 years or older from January 2001 to April 2019 were enrolled.
The study protocol was approved by the Ethics Committees of Ito Hospital (Approval Number 281) and the National Center for Child Health and Development (Approval Number 553). Written, informed consent for genetic analysis was obtained from each participant.
The study participants were classified into three groups based on the ultrasonographic findings: (1) Goiter group, with a large thyroid gland in the normal location; (2) Normal gland group, with a normal-sized gland in the normal location; and the (3) Dysgenesis group, with no detectable thyroid tissue (aplasia), thyroid tissue in an abnormal location (ectopia), small thyroid gland in the normal location (hypoplasia), and hemiaplasia. Goiter and thyroid hypoplasia were defined based on measurements of the right lobe of the thyroid 20 : goiter, thyroid width >20 mm and/or thyroid thickness (anterior-posterior diameter) >16 mm; and hypoplasia, thyroid width <10 mm.
Thyroid nodules in this study were defined as ones with a diameter >10 mm. 21 If ultrasonography was performed multiple times, the most recent images were evaluated.
Biochemical assays
Serum levels of TSH, free triiodothyronine (fT3), fT4, and Tg were measured by electrochemiluminescence immunoassays (Elecsys TSH, Elecsys fT3 III, Elecsys fT4 III, Elecsys Tg II, respectively; Roche Diagnostics GmbH, Basel, Switzerland). The reference intervals were TSH 0.2–4.5 mU/L; fT3 3.4–6.6 pmol/L; fT4 10.3–20.6 pmol/L; and Tg ≤33.7 ng/mL.
Because the majority of study participants underwent thyroid function tests multiple times, the medians of all measurements were calculated for each participant, and the values are shown. In Figure 2B, median Tg levels and corresponding TSH levels measured at the same time were used to draw the scatter plot.
For two patients who underwent total thyroidectomy, data obtained before the surgery were analyzed. For one patient who underwent a right hemithyroidectomy, all data were included.
Comparison of thyroid function and morphology between CH and non-CH adults
Thyroid function test results and thyroid ultrasonography findings were compared between adult CH patients and non-CH individuals (Supplementary Data S1).
Comparative analysis was not performed for men because it was not possible to collect a sufficient amount of relevant data for non-CH men at Ito Hospital.
Genetic screening
Genomic DNA samples were extracted from peripheral leukocytes. A customized gene panel, including 12 CH-associated genes (DUOX2, DUOXA2, FOXE1, IYD, NKX2-1, PAX8, SLC5A5, SLC26A4, SLC26A7, TG, TPO, and TSHR), was purchased from QIAGEN (Hilden, Germany; QIAseq Targeted DNA Custom Panels). Genomic DNA samples (20 ng) were treated to construct the next-generation sequencing library according to the manufacturer's protocol, and the library was sequenced with MiSeq (Illumina Inc., San Diego, CA).
Variants that fulfilled any of the following were classified as pathogenic: (1) truncating variants (i.e., nonsense, frameshift, or splice site variants); (2) previously known pathogenic functional variants; (3) rare missense variants [allele frequency <0.005 in 14KJPN; (
Statistical analysis
Means with standard deviation and medians with interquartile range were used to characterize normally and non-normally distributed data, respectively. The normality of each distribution was examined with the Shapiro–Wilk test. The statistical significance of differences was calculated using Welch's t-test, the Mann–Whitney U test, analysis of variance, the Kruskal–Wallis test, the Steel Dwass test, or Tukey's honestly significant difference test. Fisher's exact test was used to determine if there were nonrandom associations between two categorical variables. The Bonferroni correction was applied for multiple comparisons calculated using Fisher's exact test. The analyses were performed with JMP version 14.0 software (SAS Institute, Cary, NC). The results of the statistical analyses were considered significant at p-values <0.05.
Results
Patients' characteristics
We identified 111 patients who met the inclusion criteria, however, four patients who did not receive thyroid ultrasonography were excluded. As the aim was to analyze the clinical characteristics of adult CH on appropriate treatment, four patients who had never achieved appropriate control of hypothyroidism (i.e., TSH <10 mU/L) were excluded. Therefore, 103 adult CH patients were included in this study (Supplementary Fig. S1).
The characteristics of the 103 study participants are summarized in Table 1. The cohort included more females (N = 72) than males (N = 31). The median age of the patients at the last clinic visit was 31 years (interquartile range, 26–36 years). Nine patients (9%) had a family history of CH. One hundred patients received LT4 replacement therapy (Thyradin-S®; ASKA Pharmaceutical Co., Ltd, Tokyo, Japan) at a median dose of 2.0 (interquartile range, 1.7–2.3) μg/(kg·d). Of the three patients not receiving LT4 replacement therapy, two stopped treatment at the ages of 16 and 17 years and did not receive treatment at age 20 years or older; one stopped replacement therapy at age 22 years and has been followed without treatment thereafter. Serum levels of thyroid autoantibodies, creatinine kinase, and total cholesterol were within normal intervals in most participants (Table 1).
Characteristics of the 103 Study Participants and the Three Morphology-Based Groups
Plus–minus values are means ± SD.
ANOVA, analysis of variance; BMI, body mass index; CH, congenital hypothyroidism; fT3, free triiodothyronine; fT4, free thyroxine; IQR, interquartile range; KW test, Kruskal–Wallis test; LT4, levothyroxine; SD, standard deviation; SDS, standard deviation score; Tg, thyroglobulin; TgAb, antithyroglobulin antibody; TPOAb, antithyroid peroxidase antibody; TRAb, TSH receptor antibody; TSH, thyrotropin.
Thyroid function and morphology of adult CH
All study participants underwent thyroid ultrasonography, mostly while on LT4 supplementation, and were classified into three groups: Goiter group, 14 (14%) patients; Normal gland group, 24 (23%) patients; and Dysgenesis group, 65 (63%) patients. Although serum TSH levels did not differ among the three groups, the fT3/fT4 ratio was significantly lower in the Dysgenesis group (Fig. 1; Table 1). The LT4 supplementation dose was lower in the Normal gland group [1.6 (0.9–2.0) μg/(kg·d)] than in the Dysgenesis group [2.1 (1.8–2.4) μg/(kg·d)].
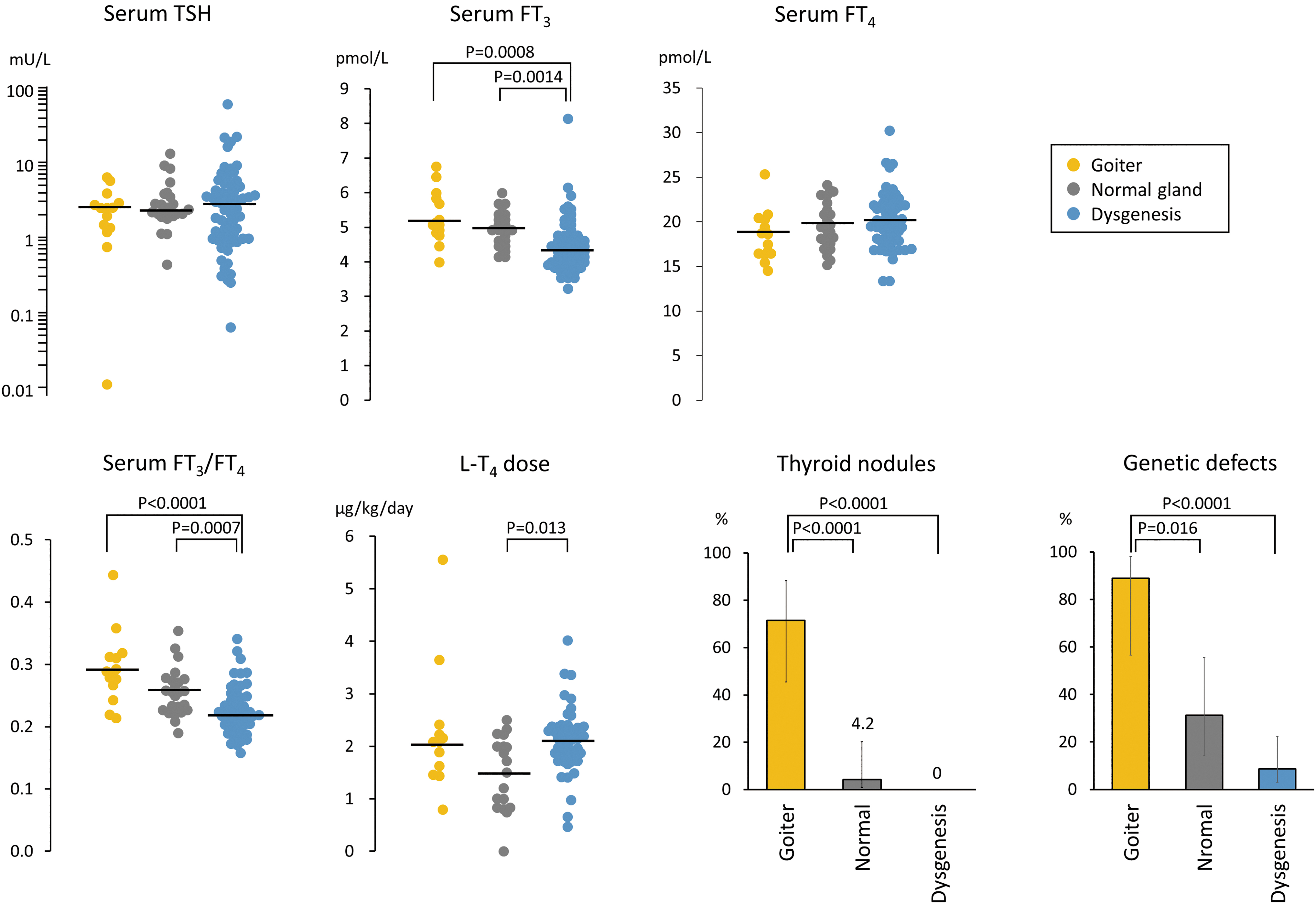
Comparison of thyroid function test results, LT4 dose, thyroid nodules, and genetic defects among the three thyroid morphology groups. Horizontal lines indicate median values. P values are shown only when significant differences were observed. Bars indicate 95% confidence intervals. The Goiter group is characterized by a high proportion of patients with thyroid nodules and genetic defects. fT3, free triiodothyronine; fT4, free thyroxine; LT4, levothyroxine; TSH, thyrotropin.
Serum Tg levels were measured mostly while patients were on LT4 supplementation. Since Tg levels increase depending on TSH levels, a scatter plot of serum TSH and Tg levels was drawn for better evaluation (Fig. 2). Patients belonging to the Dysgenesis and Normal gland groups had mostly normal serum Tg levels if simultaneously measured TSH levels were within the normal range. Patients belonging to the Goiter group showed a bimodal distribution ranging from very low to very high.
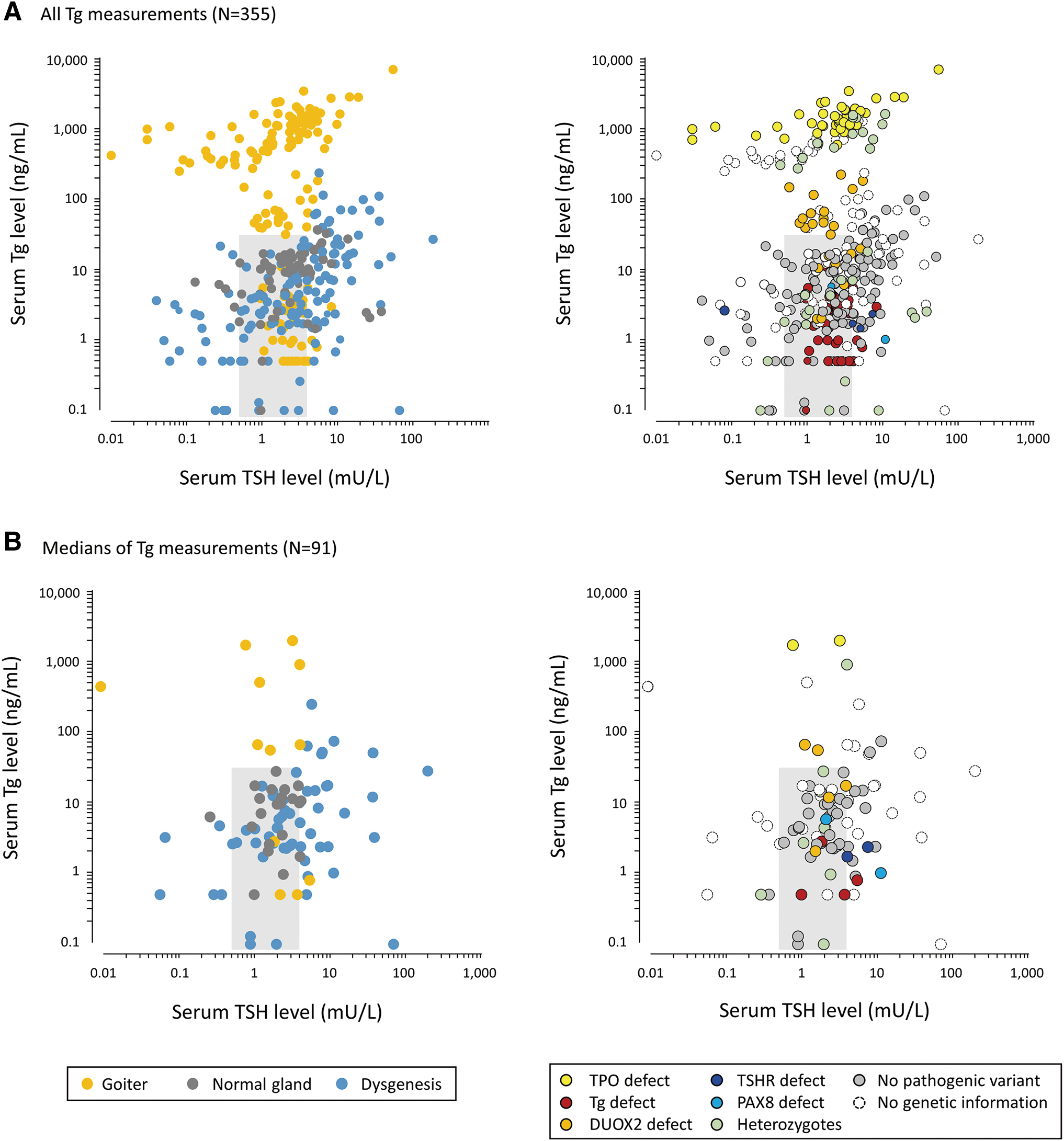
Scatter plots showing the relationship between serum TSH levels and serum Tg levels. The shaded areas indicate the reference intervals for serum TSH and Tg levels.
Thyroid nodules with diameter >10 mm were observed in 11 patients, corresponding to 71% (10/14), 4% (1/24), and 0% (0/65) of the Goiter, Normal gland, and Dysgenesis groups, respectively (Fig. 1). Serum TSH levels and LT4 replacement doses were not significantly different between patients with and without thyroid nodules (Supplementary Table S1). Genetic testing was performed in 8 of the 11 patients with thyroid nodules, and it showed that 7 (88%) had genetic defects. All 11 patients had 2 or more (i.e., multiple) nodules. Three patients underwent thyroidectomy, none of which showed malignant pathology. Six of the remaining eight patients underwent fine needle aspiration cytology which showed no evidence of malignancy.
Comparison of thyroid function and morphology between CH and non-CH adults
To characterize the thyroid function test results of adult CH patients receiving LT4 therapy, a comparison was performed between female patients and non-CH women matched for serum TSH levels (Fig. 3; Supplementary Table S2). CH patients had higher fT4 levels (CH vs. non-CH; 19.6 ± 3.4 vs. 15.8 ± 2.1 pmol/L, p < 0.0001) and lower fT3 levels [4.3 (3.8–4.8) vs. 4.6 (4.3–4.9) pmoL/L, p = 0.0038] than non-CH individuals. Thus, the fT3/fT4 ratio was significantly lower in CH patients [0.22 (0.19–0.25) vs. 0.29 (0.27–0.32), p < 0.0001]. There were no significant differences in the anti-Tg antibody, antithyroid peroxidase (TPO) antibody, and anti-TSH receptor antibody titers (Supplementary Table S2). Thyroid nodules were more frequently detected in the female CH patients than in the non-CH women (14.3% vs. 6.0%, p = 0.034) (Fig. 3).

Comparison of thyroid function test results and thyroid nodules between female adult CH patients and non-CH women matched to the female adult CH patients by age and serum TSH levels. Horizontal lines indicate median values. p-Values are shown only when significant differences were observed. Bars indicate 95% confidence intervals. Female CH patients have a low fT3/fT4 ratio and have thyroid nodules more frequently than non-CH women. CH, congenital hypothyroidism.
Genetics of adult CH
Comprehensive genetic screening was performed in 60 of the 103 participants to define the molecular-level subtype of CH. Fourteen patients had seemingly biallelic inactivating variants in DUOX2 (N = 5), TG (N = 4), TPO (N = 3), or TSHR (N = 2) (Table 2) (Supplementary Data S2). Two patients had a heterozygous variant in PAX8, a responsible gene for an autosomal dominant form of CH. These 16 patients were considered to have genetic defects. Some of their ultrasonographic images are shown in Supplementary Figure S2. Eight patients who had a heterozygous variant in DUOX2, DUOXA2, TG, TPO, TSHR, or SLC26A4 were considered heterozygous variant carriers rather than patients with genetic defects (Supplementary Table S3). The proportions of patients with genetic defects were 89%, 36%, and 9% in the Goiter, Normal gland, and Dysgenesis group, respectively (Fig. 1).
Summary of Patients with Genetic Defects
Age at ultrasonography.
Size of left lobe.
The dose of LT4 was 50 μg/day.
F, female; M, male; NA, not available.
Serum Tg levels of patients with the dual oxidase (DUOX) 2 defect, Tg defect, or TPO defect are shown in Figure 2. Tg levels were marked elevated in TPO-deficient patients, whereas those of Tg-deficient patients were low. Serum Tg levels of DUOX2-deficient patients were variable: they were high in those with goiter, but normal in those with normal-sized gland (Fig. 2).
All three patients with the TPO defect and three of four patients with the Tg defect had thyroid nodules. Of the five patients with the DUOX2 defect, only one had thyroid nodules. All patients with the TSHR defect and PAX8 defect had no thyroid nodules.
Pathological findings of adult CH due to thyroid dyshormonogenesis
Patients 1, 7, and 11 underwent thyroidectomy at age 17, 42, and 27 years, respectively, because their large thyroid glands were a cosmetic concern. The histopathological images are shown in Supplementary Figure S3. The findings of the adenomas of the three patients were compatible with nodular hyperplasia with no evidence of malignancy in tissue slices. When tissues surrounding the adenomas were examined, Patient 1 (DUOX2 p.[Gly488Arg](;)[Lys530*]) had normal thyroid histology with normal-sized follicles and thyroid follicular cells (TFCs) with a low cuboidal appearance. Patient 7 (TG p.[Cys1264Arg](;)[Trp1437*]) showed small follicles, and their colloids were either missing or light in color; TFCs were enlarged. In Patient 11 (TPO p.[Asp633Asn](;) [Cys808Alafs*24]), follicles were filled with colloids, but their size was small; TFCs were enlarged.
Discussion
This cross-sectional study illustrates the thyroid outcomes of adult CH patients followed up in a large thyroid-specialized clinic in Japan. We observed that 10.7% of the participants had thyroid nodules with diameter >10 mm. The prevalence was significantly higher than in non-CH individuals, and it was especially high (71%) in patients with goiter. Six of the seven patients with the TPO or Tg defect had thyroid nodules despite having been treated since infancy, suggesting the TSH-independent effect of mutated proteins in thyroid nodule formation. Whether patients with nodules had higher serum TSH levels or lower LT4 doses was also examined, because TSH stimulates the proliferation of thyroid follicular cells, but no significant differences were observed. At present, the small number of adult CH cases with thyroid nodules makes it difficult to identify factors other than genetic defects involved in nodule development and subsequent growth.
Pathogenic DUOX2 variants were first reported to cause permanent CH in biallelic variant carriers and transient CH in heterozygotes. 23 However, later studies have shown that biallelic DUOX2 variants may result in transient CH. 24 The frequency of the monoallelic DUOX2 variant in Japan was estimated to be 1 in 70, 25 indicating that the vast majority of heterozygotes do not have CH. In this study, five patients were found to have seemingly biallelic pathogenic DUOX2 variants. One of the five patients was not treated (i.e., transient CH), and the remaining four were treated with relatively low doses of LT4. Their thyroid morphology was variable: two had goiter and three did not. One patient with goiter underwent thyroidectomy, providing us the first opportunity to observe DUOX2-deficient thyroid tissues.
As shown in Supplementary Figure S3, the histology was normal. In the DUOX2 defect, thyroid hormone-producing capacity can be normalized after infancy, probably due to compensation by DUOX1 and reduction of thyroid hormone demand per body weight in the period. 26 The present study showed that, not only thyroid hormone-producing capacity, but also thyroid histology may be normal after infancy.
The residual hormone-producing capacity of the thyroid gland is diverse in pediatric CH, 27 but it has been little studied in adult CH. In the present study, the LT4 supplementation dose was higher in the Dysgenesis group than in the Normal gland group, which was in line with a previous study of pediatric CH. 27 It was also found that the fT3/fT4 ratio was lower in patients with thyroid dysgenesis than in the Normal gland group. Of the T3 synthesized in the body, 20% is derived from the thyroid, and the remaining 80% is derived from the effector organs where T4 is converted to T3. 28
In patients with abrogated thyroid hormone-producing capacity, such as thyroid dysgenesis and total thyroidectomy, 29,30 relative T3 deficiency would be induced by LT4 monotherapy. Ito et al. investigated the relationship between postoperative TSH levels and hypothyroidism/thyrotoxicosis symptoms in thyroidectomized patients, and they found that patients with mildly suppressed TSH levels (0.03–0.3 mU/L) were closest to symptomatic euthyroidism, defined by subjective physical activity and tolerance to heat and cold. 31
The present study has several limitations. First, this study included only three patients with transient CH. It was thus not possible to gain insight into the long-term prognosis and complications of transient CH. Second, the most clinical evaluations were performed without stopping LT4 therapy, and thus the hormone-producing capacity of each patient could not be accurately assessed. A subset of patients with thyroid dyshormonogenesis might have had a normal-sized thyroid on LT4 therapy and have been classified into Normal gland group. Third, although this was one of the largest studies of adult patients with CH, the possibility of unmeasured confounding cannot be ruled out. Multivariable analysis was not performed due to the limited sample size and information on covariates. Finally, this was a single-institution study conducted in Tokyo, and the results may not be generalizable to other populations.
In summary, 103 adult patients with CH at a single thyroid-specialized clinic were examined, and their anatomical, physiological, and genetic characteristics were described. An unexpectedly high prevalence of thyroid nodules (71%) was found in adult CH patients with goiter. In the present cohort, most TPO-deficient or Tg-deficient patients had goiter despite LT4 replacement therapy since infancy. Although one cannot predict whether these lesions will progress to malignancy in the future, the present observations support the current guideline (1) that recommends periodic ultrasound investigation in patients with suspected thyroid dyshormonogenesis to monitor thyroid volume and nodules.
Footnotes
Acknowledgments
The authors thank Ms. Ikuko Kageyama and Ms. Saori Miyasako (Department of Molecular Endocrinology, National Research Institute for Child Health and Development) for technical assistance and Dr. Kosuke Inoue (Department of Social Epidemiology, Graduate School of Medicine and School of Public Health, Kyoto University) for his advice on statistical methods. We thank Luba W, MD, from Forte Inc. for editing a draft of this article.
Authors' Contributions
C.S., S.N., N.W., and J.Y.N. designed the study. S.N., K.T.-N., and A.H. performed genetic analyses. C.S., A.H., N.S., H.O., M.F., M.M., A.Y., N.W., K.S., J.Y.N., M.T., and K.I. clinically characterized patients and collected samples. R.K. conducted pathological analyses. C.S. and S.N. analyzed and interpreted the data. C.S. and S.N. wrote the article, which was read by all authors and approved for submission.
Author Disclosure Statement
No competing financial interests declared.
Funding Information
This study was supported by JSPS KAKENHI (22K16420) to Kanako Tanase-Nakao.
Supplementary Material
Supplementary Data S1
Supplementary Data S2
Supplementary Figure S1
Supplementary Figure S2
Supplementary Figure S3
Supplementary Table S1
Supplementary Table S2
Supplementary Table S3