
Abstract
Background:
The most frequent site of recurrence of differentiated thyroid cancer (DTC) is cervical lymph nodes (LNs), which often necessitates repeated surgical interventions and morbidity in a generally indolent disease. Data on active surveillance (AS) of small cervical nodal metastasis are still scarce, particularly in real-world clinical settings. In this study, we evaluated the DTC outcomes of AS of metastatic cervical LNs and explored factors associated with disease progression.
Methods:
We conducted a retrospective cohort study, including DTC patients with biopsy-proven metastatic cervical LNs, who were followed on AS in a tertiary care, university-based institution in Brazil. The inclusion criteria were cervical metastasis ≤2.0 cm and an AS duration of at least 6 months. We excluded lesions with aggressive histology, those in close proximity to or invading local structures. The primary outcome was disease progression (enlargement ≥3 mm in any diameter or a new cervical metastasis).
Results:
Data from 40 patients were analyzed. Most were female (77.5%) and had papillary thyroid cancer (97.5%). The mean age was 47.0 (± standard deviation 15.8) years. The 8th edition of the tumor, node, metastasis stage (TNM8) staging for DTC was as follows: 29 in stage I (74.4%), 8 in stage II (20.5%), and 2 in stage IV (5.0%). The median maximum LN diameter was 0.9 (interquartile range [IQR], 0.8–1.3) cm, and the median AS follow-up duration was 27.5 (IQR, 16.5–47.3) months. Disease progression occurred in 14 (35%) patients: 7 (17.5%) due to enlargement ≥3 mm, and 7 (17.5%) had new cervical metastasis. The cervical progression-free survival was 51.0 (confidence interval, 47.0–55.0) months. No demographic, oncological, or biochemical factors were associated with disease progression. Of the 14 patients with disease progression, 8 were referred for surgery. No permanent surgical complications were reported. Of the six patients who remained on AS despite disease progression, five showed no further progression during subsequent follow-up (range 6–40 months).
Conclusions:
We observed that most small metastatic cervical LNs remained stable and were safely managed with AS. Nevertheless, these observations are limited by the retrospective design, small sample size, and short follow-up. Further prospective and long-term studies are warranted.
Introduction
Thyroid cancer is the leading endocrine cancer, with an incidence projected to grow continuously until at least 2030, although the disease mortality rate remains stable. 1,2 Papillary thyroid carcinoma (PTC) is the most frequent histological type, and previous data have shown low rates of cancer growth of small tumors in patients under active surveillance (AS). 3,4 Recently, real-world studies have indicated that AS is gaining worldwide acceptance and is currently the primary management strategy for low-risk papillary thyroid microcarcinoma in Japan. 5,6
Cervical lymph nodes (LNs) are the most common site for differentiated thyroid cancer (DTC) metastasis, accounting for approximately three out of four recurrences. 7 Approximately 28–38% of patients develop recurrence after therapeutic neck dissection, 8 –10 and these patients often require repeated lymphadenectomy, which is potentially associated with complications such as hypoparathyroidism, chyle leak, cervical hematoma, and voice disturbances, with an incidence ranging from 1.4% to 17.1%. 11
According to the last American Thyroid Association (ATA) guidelines for DTC management in adults, “therapeutic compartmental central and/or lateral neck dissection in a previously operated compartment, sparing uninvolved vital structures, should be performed for patients with biopsy-proven persistent or recurrent disease for central neck nodes ≥8 mm and lateral neck nodes ≥10 mm in the smallest dimension that can be localized on anatomic imaging” (Strong recommendation, Moderate-quality evidence). 12 However, these guidelines also discuss that “through thorough patient and multidisciplinary collaborative discussions, metastatic nodes >8–10 mm can be carefully observed in properly selected patients with serial clinical and radiographic follow-up, with surgery being offered if they progress during follow-up and conservative follow-up being maintained if they are stable over time.” 12 Most LN metastases do not enlarge, and some might resolve spontaneously, rendering AS an attractive alternative approach. 10,13
In this study, we aim to describe a single-center reference experience on AS in DTC patients with persistent or recurrent disease in cervical LNs. In addition, we explore predictors of cervical disease progression and attempt to define characteristics that can help select the optimal patient for AS.
Materials and Methods
Study design and patients
We reviewed a retrospective cohort of adult DTC adult patients who had a total thyroidectomy and were diagnosed with recurrent or persistent cervical nodal metastatic disease by ultrasonography (US)-guided fine-needle aspiration biopsy (FNAB) at the Thyroid Unit, Hospital de Clínicas de Porto Alegre from May 2013 to December 2021 and who then underwent AS. Adult DTC patients with cervical nodal metastasis smaller than 2.0 cm in maximum diameter were considered eligible for AS in our institution. The exclusion criteria were aggressive histology (poorly DTC, widely invasive follicular thyroid carcinoma, oncocytic carcinoma, and papillary thyroid carcinoma high-risk subtypes), proximity to or invasion of local structures (e.g., aerodigestive tract, great vessels), treatment with systemic therapy, or cervical radiotherapy.
Among 145 patients with biopsy-proven DTC cervical nodal metastasis followed at our institution, 19 did not meet the eligibility criteria for AS due to lesions larger than 2 cm, and 1 patient did not complete AS for at least 6 months. Six patients met the exclusion criteria for other reasons, including: five—aggressive tumor histology and one—cervical radiotherapy. Of the remaining 119 patients, 79 underwent immediate surgery due to patient preference after a shared decision-making process (Fig. 1). The clinical data were retrieved from the medical records.

Flowchart—Management after biopsy-proven metastatic LN detection in 145 DTC patients. AS, active surveillance; DTC, differentiated thyroid cancer; LN, lymph node.
All patients provided written consent for data review and analyses. The study was approved by the institution's Ethics Committee (CAAE 47654321.8.0000.5327/GPPG 20210231) and was performed in accordance with the Declaration of Helsinki (2013).
Institutional routine care of DTC and AS of metastatic cervical nodes
The routine care in the follow-up of DTC in our institution includes an initial assessment 3–6 months after the thyroidectomy: physical examination of the neck, measurements of the serum thyroglobulin (Tg), antithyroglobulin antibodies (TgAbs), thyrotropin (TSH) levels, and neck US. In a second evaluation, 6–12 months after the initial treatment, the patient's disease status is classified according to his or her response to initial therapy. Suspicious LNs, characterized in the US by the presence of malignancy characteristics (microcalcifications, cystic aspect, peripheral vascularity, round shape, lobulated margins, hyperechogenicity, or loss of hilum), are evaluated through FNAB for cytology and complementary cell block and for thyroglobulin measurement in the FNAB washout (FNAB-Tg). The management options (surgery or AS) are discussed between the patient and the multidisciplinary team through the shared decision-making process and after malignancy confirmation.
AS of metastatic cervical nodes consists of biannual US for at least 1 year and then annually if the disease remains stable. The patients are maintained on levothyroxine suppressive therapy with a target TSH <0.1 mUI/L (or a TSH target of 0.1–0.5 mUI/L if there is a history of atrial fibrillation). TSH, thyroglobulin on levothyroxine suppressive therapy (Tg-T4), and TgAb are measured at least twice a year. If one or more suspicious LNs were not submitted to FNAB at the beginning of the AS, they were also subject to US monitoring. Any new suspicious LNs are submitted to FNAB for cytological diagnostic confirmation of metastatic disease. The decision to undergo surgery is reassessed at every clinical appointment.
US-FNAB and laboratory evaluation
In this study, grayscale and color Doppler US were performed in all cervical compartments by experienced radiologists with expertise in thyroid diseases (M.F. and C.S.F.) using a high-resolution ALOKA US device (Tokyo, Japan) with a 7.5 MHz linear transducer. The US-FNAB, cytologic, and cell block evaluations were performed as previously described. 14,15 The serum Tg-T4 and FNAB-Tg levels were measured by chemiluminescence (electrochemiluminescence immunoassay [ECLIA]) using a commercially available kit (Modular E-170 Roche). TSH was measured by ECLIA (ADVIA Centaur XP; Siemens, Tarrytown, NY). The TgAb level was measured by chemiluminescent microparticle immunoassay, and different kits were used for the analyzed data.
Outcomes
The primary study outcome was cervical disease progression, defined as LN enlargement ≥3 mm in any diameter (compared to the size at metastasis confirmation) or new cervical metastasis confirmed by FNAB, whichever occurred first. We performed a secondary analysis subgrouping stable disease into two groups: patients with disease reduction (shrinkage ≥3 mm in any diameter and the absence of enlargement in the other diameters) and those without disease reduction. We also evaluated possible predictors for the outcomes, surgical complications in the subjects who underwent cervical dissection, and cervical progression-free survival (PFS, from the month of initial cervical metastasis detection until the progression date or last follow-up).
Statistical analyses
Data were reported as the mean ± standard deviation or the median and interquartile range (IQR) for continuous variables. Absolute numbers and percentages were used for categorical variables. The statistical analysis included Pearson's chi-square test for categorical data. According to the normality of the distribution and variance of the continuous data (assessed with the Shapiro–Wilk test and Levene's test), independent two-sample t-test and analysis of variance (complemented by the Tukey test) or the Mann–Whitney and Kruskal–Wallis (complemented by the post hoc Dunn's test) tests were performed.
Univariate and multivariable analyses were executed to explore predictors for disease progression or reduction, considering a bivariate analysis with p < 0.25 as the entrance criteria, but only those variables with p < 0.05 remained in the final model. Patients with positive TgAb were excluded from the Tg analysis. Cervical PFS was assessed through Kaplan–Meier analysis. p < 0.05 was considered statistically significant, and all tests were two tailed. Statistical analyses were performed with Statistical Package for Social Sciences (SPSS) software, version 25.0 (IBM Corp., Armonk, NY).
Results
Patients
Of the 145 patients with biopsy-proven DTC cervical nodal metastasis followed at our institution, 41 were eligible for AS and 40 completed 6 months of AS and were included in this study (Fig. 1). The majority was female (77.5%; n = 31), and the mean age was 47.0 (±15.8) years. The most prevalent histologic type was PTC (97.5%; n = 39). The ATA recurrence risk (2015) was low in 7 (17.9%), intermediate in 29 (74.4%), and high in 3 patients (7.6%). According to the 8th edition of the tumor, node, metastasis stage (TNM8) staging system for DTC,
16
the patients were distributed as follows: 29 in stage I (74.4%), 8 in stage II (20.5%), and 2 in stage IV (5.0%). One patient had unknown TNM staging and ATA recurrence risk due to missing data
Baseline Characteristics of Biopsy-Proven Metastatic Cervical Lymph Nodes in Differentiated Thyroid Cancer Patients Referred for Active Surveillance or Immediate Surgery
Numerical variables with normal distribution by the Shapiro–Wilk test and equal variance by Levene's test are presented as the mean ± SD and were analyzed with Student's t-test. Non-normal variables are presented as median (interquartile range; range) and were analyzed with the Mann–Whitney test. Categorical variables are presented as proportions (n, %) and were analyzed by Pearson's chi-square test. Patients with positive TgAb were excluded from the Tg-T4 analysis.
Seven patients (one in AS group and six in immediate surgery group) underwent thyroidectomy at other institutions, and complete histology result was unavailable.
AS, active surveillance; ATA, American Thyroid Association; FTC, follicular thyroid carcinoma; LN, lymph node; OC, oncocytic carcinoma; PDTC, poorly differentiated thyroid carcinoma; PTC, papillary thyroid carcinoma; RAI, radioactive iodine; SD, standard deviation; TgAb, antithyroglobulin antibody; Tg-T4, thyroglobulin on levothyroxine suppressive therapy; TNM8, 8th edition of the tumor, node, metastasis stage; UICC, Union for International Cancer Control.
Cervical disease progression
Twenty-six patients (65%) had stable disease. Cervical disease progression occurred in 35% (n = 14): 17.5% (n = 7) had enlargement ≥3 mm, and 17.5% (n = 7) had new cervical metastatic node(s). The median time until progression among the 14 subjects in the progression group was 15.5 (IQR, 7.0–27.5) months.
There were no demographic, oncological, or biochemical factors associated with the primary outcome in the statistical analysis. TNM8 staging and ATA recurrence risk were similar between those patients who presented with disease progression and those with stable disease. The LN diameter was also similar: 1.1 (IQR, 0.8–1.2) cm in the progression group and 0.9 (IQR, 0.8–1.3) cm in the stable disease group (p = 0.528). The interval from thyroidectomy to cervical metastasis detection was 39.5 (IQR, 29.8–80.8) months in the patients with disease progression and 51.0 (IQR, 24.0–60.0) in those with stable disease (p = 0.567). Twelve (85.7%) subjects in the disease progression group and 19 (73.1%) in the stable disease group underwent RAI treatment before metastasis diagnosis (p = 0.361) (Table 2).
Clinical, Radiological, and Laboratory Features of Differentiated Thyroid Cancer Patients Who Presented Cervical Disease Progression Versus Stable Disease During Active Surveillance
Numerical variables with normal distribution by the Shapiro–Wilk test and equal variance by Levene's test are presented as the mean ± SD and were analyzed with Student's t-test. Non-normal variables are presented as the median (interquartile range; and range) and were analyzed with the Mann–Whitney test. Categorical variables are presented as proportions (n, %) and were analyzed by Pearson's chi-square test. Patients with positive TgAb were excluded from the Tg analysis.
One patient underwent thyroidectomy at another institution, and the complete histology result was unavailable.
Tg, thyroglobulin.
To further explore nodal disease behavior, we performed a secondary analysis dividing the stable disease group into two groups: patients with disease reduction (n = 8; 20.0%) and those without disease reduction (n = 18; 45.0%), and compared them with the patients with cervical disease progression (n = 14; 35.0%). There were no differences among the three groups regarding ATA recurrence risk, TNM8 staging, RAI treatment during AS, or maximum LN diameter (all p > 0.05). Interestingly, the reduction group had an initial Tg-T4 level lower than the disease progression group (medians of 0.2 [IQR, 0.2–0.7] ng/mL and 4.4 [IQR, 1.1–14.0] ng/mL, respectively; p = 0.041) (Supplementary Table S1). Three patients in the reduction group (37.5%) progressed to complete remission of the metastasis at the 27th, 42nd, and 58th months of AS.
Eight patients with disease progression and one with stable disease (patient preference) were referred for lymphadenectomy. One patient with disease progression is awaiting surgery at the time of writing of this article. The dynamic risk stratification at the last follow-up of the three patients who underwent surgery was excellent response in three; indeterminate response in two (one due to positive TgAb and another to a Tg-T4 level of 0.5 ng/mL); biochemical incomplete response (a Tg-T4 level of 4.22 ng/mL and negative TgAb) in one; and structural incomplete response in two (one had new cervical recurrence and the other had systemic progression).
Six of the 14 patients who met the primary outcome continued under AS despite disease progression. Among them, four refused to undergo nodal dissection due to the fear of surgery-related complications, one was under investigation for another primary cancer (lung), and one presented with systemic disease progression and initiated tyrosine kinase inhibitor therapy. This last patient was one of the three high recurrence-risk patients in the cohort, as detailed in Supplementary Table S2. Five of these six patients met the enlargement criteria for disease progression and showed no further enlargement in subsequent follow-ups (range, 6–40 months).
The Kaplan–Meier analysis, which was designed considering the time from the beginning of AS until disease progression or the last follow-up for the 40 patients of the cohort, showed a median cervical PFS of 51.0 [confidence interval, CI, 47.0–55.0] months (Fig. 2).
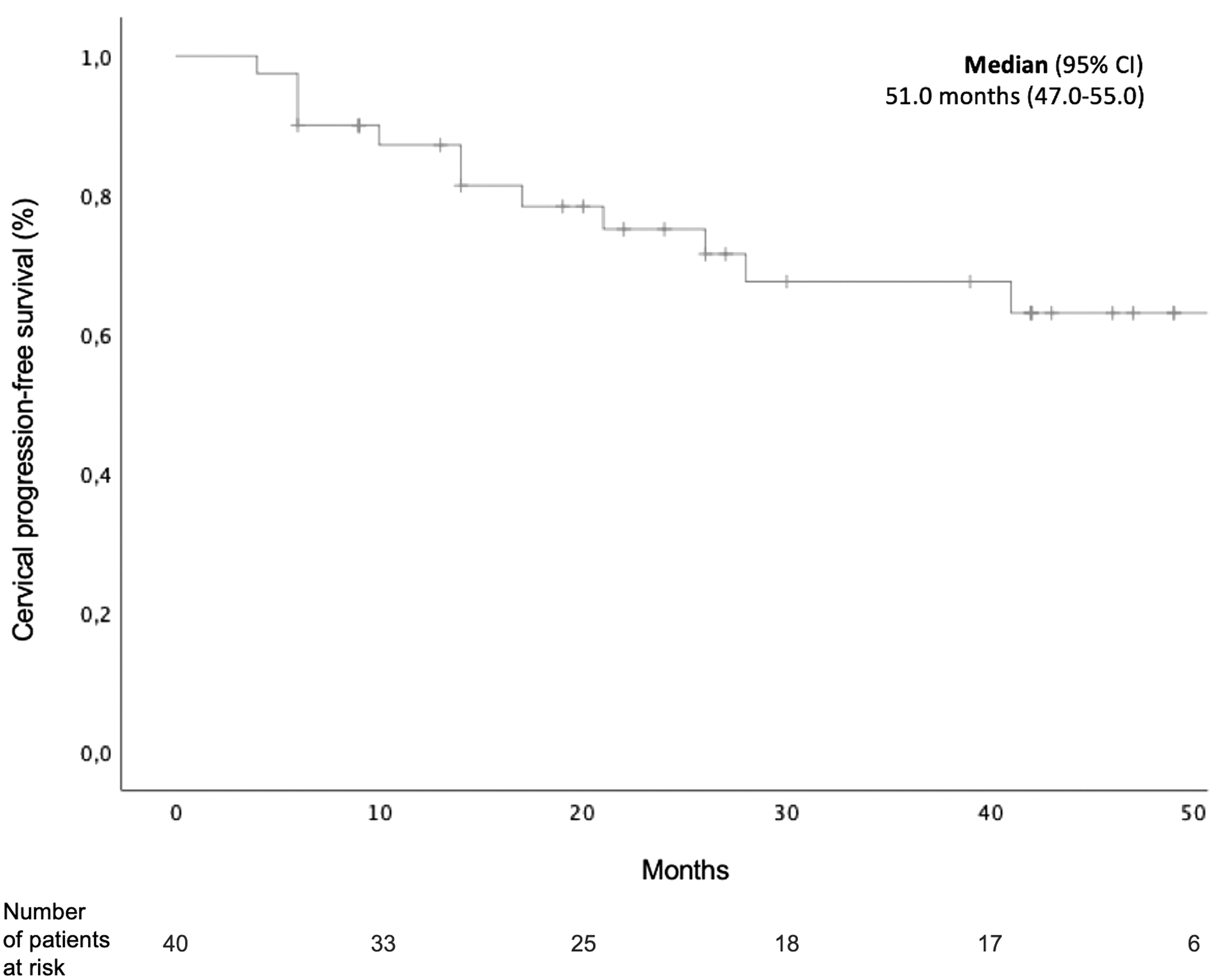
Kaplan–Meier analysis of cervical progression-free survival (months) in 40 patients with cervical metastasis under AS, from metastasis confirmation until disease progression (nodal enlargement ≥3 mm in any diameter, compared to the size at metastasis confirmation, or new biopsy-proven cervical metastasis) or last follow-up.
Surgical outcomes
Only two patients presented with mild transient surgical complications: there was one patient who developed a seroma and another who developed dysphonia, with spontaneous resolution within 6 months (i.e., the permanent complication rate was 0%). The surgical outcomes and case descriptions are reported in Table 3. The median time for surgery after the beginning of AS was 20.0 (range, 17.5–40.0) months.
Surgical Outcomes of Nine Patients Referred for Cervical Dissection After Active Surveillance
FNAB, fine-needle aspiration biopsy; US, ultrasonography.
Discussion
In this study, we showed that most DTC cervical metastatic LNs (65.0%) remained stable under AS. Moreover, there was no increase in surgical morbidity when lymphadenectomy was performed after disease progression. Our results support previous data indicating AS as a valuable and safe strategy for metastatic LN disease in DTC patients.
One of the main concerns regarding AS in cervical metastasis is the possibility of disease progression. In a previous work by Tomoda et al assessing the outcomes of cervical nodal metastasis in 83 PTC patients under AS, 10 an enlargement of ≥3 mm and new cervical metastasis sites were reported in 20.5% and 10.9% of patients, respectively. There was no predictor for enlargement ≥3 mm in the multivariate analysis. Comparably, Robenshtok et al 17 reported a 20.0% incidence of ≥3 mm enlargement in suspicious LNs detected on US after thyroidectomy for PTC in 166 patients with a 3.5-year median follow-up. There was also no independent predictor for LN enlargement. However, not all suspicious LNs were evaluated through FNAB. Jerkovich et al recently reported a 24% rate of ≥3 mm enlargement in 50 PTC patients under AS for metastatic LNs. They found that a rise ≥0.5 ng/mL in the Tg-T4 level during AS was the only predictor for enlargement in the multivariate analysis (odds ratio 16.2 [CI 1.5–120.2]). 18
Our data showed comparable enlargement rates (17.5%). Of note, we also included a criterion of new nodal biopsy-proven metastasis as disease progression to avoid the concept that the initial metastatic LN is the central concern in AS. Indeed, disease progression was due to new metastatic LNs in half of the patients in our cohort. This finding emphasizes the importance of detailed cervical US evaluation beyond the initial metastasis site.
A significant proportion of the patients with cervical metastasis in our cohort had persistent/first-time recurrent disease (n = 21; 52.5%). Of note, some studies have reported high complete response rates after the first reoperation for persistent/recurrent disease. 19 Nevertheless, it should not preclude discussing AS with those patients, particularly when experienced high-volume surgeons are not available. Notably, most patients were classified as low to intermediate recurrence risk (n = 36; 92.3%); although a high recurrence risk is not a formal contraindication for AS, further studies are needed to evaluate AS in this subgroup of patients.
Another interesting finding of our work was that eight patients showed nodal shrinkage. Spontaneous remission is a phenomenon reported in previous studies with rates between 14.0–39.8% in cervical recurrences 10,17 and 9.0–12.1% in primary PTC lesions. 20,21 It has been proposed that the traumatic effect generated by FNAB could lead to immunological processes, resulting in destruction and necrosis, causing shrinkage. 22 Nevertheless, other immunogenic independent factors might play a role, as suggested by suspicious LNs that were not biopsied but ended up resolving. 23
In our secondary analysis, the Tg-T4 level in ng/mL at the metastasis diagnosis was significantly lower in the disease reduction group. These findings are in agreement with a previous study that evaluated predictors for recurrence after a second surgery for locoregional relapse in PTC and that study found that biochemical remission (stimulated Tg <1 ng/mL) was the only independent predictor for recurrence-free survival. 24 Taken together, these results may suggest that patients who present with undetectable Tg-T4 at diagnosis of nodal metastasis may have a better prognosis in considering AS for disease management of persistent or recurrent cervical nodal disease. Notably, suspicious sonographic classification of posttreatment cervical disease has been suggested as a potential tool to detect nodal enlargement in subsequent follow-up. 25
Social beliefs about cancer, unclear surveillance protocols, and lack of supporting data are considered barriers to AS implementation in PTC. 26 In contrast to the long-standing cultural perception that delaying nodal dissection would result in a more aggressive surgery, our surgical complication rate was low, suggesting that postponing surgery may not increase the risk for surgical morbidity. A similar finding was reported in previous studies comparing immediate thyroidectomy versus thyroidectomy after progression under AS for PTC, which showed a lower incidence of surgical complications in the second group. 4,22 Further research is needed to compare surgical complications between immediate surgery versus surgery after disease progression in patients with cervical metastases under AS. Of note, eight patients (20%) in this cohort met the ATA guidelines recommendation criteria for immediate surgery, and only two of them had disease progression.
Our study has some weaknesses, including the small sample size, short follow-up, and retrospective nature, which limit our conclusions. Moreover, our study includes many patients referred to us at different intervals after thyroidectomy, which precludes proper categorizing of persistent versus recurrent cervical disease. The surgical management was probably heterogeneous, and its descriptions were incomplete in many cases. Data on the number of LNs, the ratio between malignant and benign LNs, and the extent of nodal disease resected in the primary surgery are lacking.
Another possible limitation is the arbitrary criteria for defining disease progression. The 3 mm sonographic enlargement was used in other studies assessing cervical metastases on AS 10,17,18,23 and was an independent predictor for shorter survival in a single study. 10 It is also used for AS of primary small, localized PTC. 6 An alternative criterion for nodal enlargement is a 50% increase in volume by measuring three dimensions. This method is used in some studies assessing primary PTC under AS, but it is considered overly sensitive. 6 The Response Evaluation Criteria in Solid Tumours criteria were also applied to determine disease progression in a recent study evaluating PTC cervical metastases under AS. 27 The discrepancy in the criteria used and lack of validation of outcomes limit the interpretation and replicability of studies in this area.
A strength of our study is a multidisciplinary team of experienced pathologists, radiologists, surgeons, and endocrinologists with expertise in thyroid cancer. Although this could be seen as a potential limitation to the external validity, we consider that our data are relevant to instigating further studies, demystifying AS, and updating the current DTC management guidelines.
In conclusion, we observed that most cervical DTC metastatic LNs remained stable and could be safely managed with AS, avoiding unnecessary surgical interventions. These results confirm previous data, which support AS as a treatment option for small recurrent or persistent metastatic LNs in DTC. Nevertheless, these conclusions are limited by to the retrospective nature of this study, which included a small number of patients and a short follow-up period. Further prospective studies with a larger number of patients and extended follow-up are warranted.
Footnotes
Acknowledgments
The authors recognize the collaboration of the surgeons José Ricardo Guimarães and Alceu Migliavaca (Hospital de Clínicas de Porto Alegre). The authors also thank PhD Carla Vaz Ferreira for her promptitude and availability to contribute to this study.
Authors' Contributions
L.B.W.: conceptualization, data curation, formal analysis, writing—original draft. R.S.S.: conceptualization, methodology, writing—review and editing. A.B.Z.: conceptualization, formal analysis, writing—review and editing. M.F.: writing—review and editing. C.S.F.: writing—review and editing. M.S.G.: writing—review and editing. J.M.D.: conceptualization, methodology, writing—review and editing. A.L.M.: conceptualization, methodology, writing—review and editing, supervision.
Author Disclosure Statement
R.S.S. has served as a subinvestigator in multicenter studies for Sanofi-Genzyme, Exelixis, and Lilly within the past 2 years. A.L.M. has served as principal investigator in multicenter studies for Sanofi-Genzyme, Exelixis, and Lilly within the past 2 years. All other authors have nothing to disclose.
Funding Information
This work was funded by the Fundação de Amparo à Pesquisa do estado do Rio Grande do Sul (FAPERGS), Programa de Apoio a Núcleos de Excelência (PRONEX), Conselho Nacional Pesquisa e Desenvolvimento (CNPq), Fundo de Incentivo à Pesquisa e Eventos do Hospital de Clínicas de Porto Alegre (Fipe/HCPA), and Programa Institucional de Bolsas de Iniciação Científica da Universidade Federal do Rio Grande do Sul (Pibic/UFRGS).
Supplementary Material
Supplementary Table S1
Supplementary Table S2