
Abstract

T
A 73-year-old woman was diagnosed with T3N1M0 classic PTC in 1999. During the following years, recurrent metastatic neck nodes were surgically removed, and lung and bone metastases developed. The patient was treated six times with 131I [accumulated activity of 34 GBq (919 mCi)]. The last five post-therapy scans were negative.
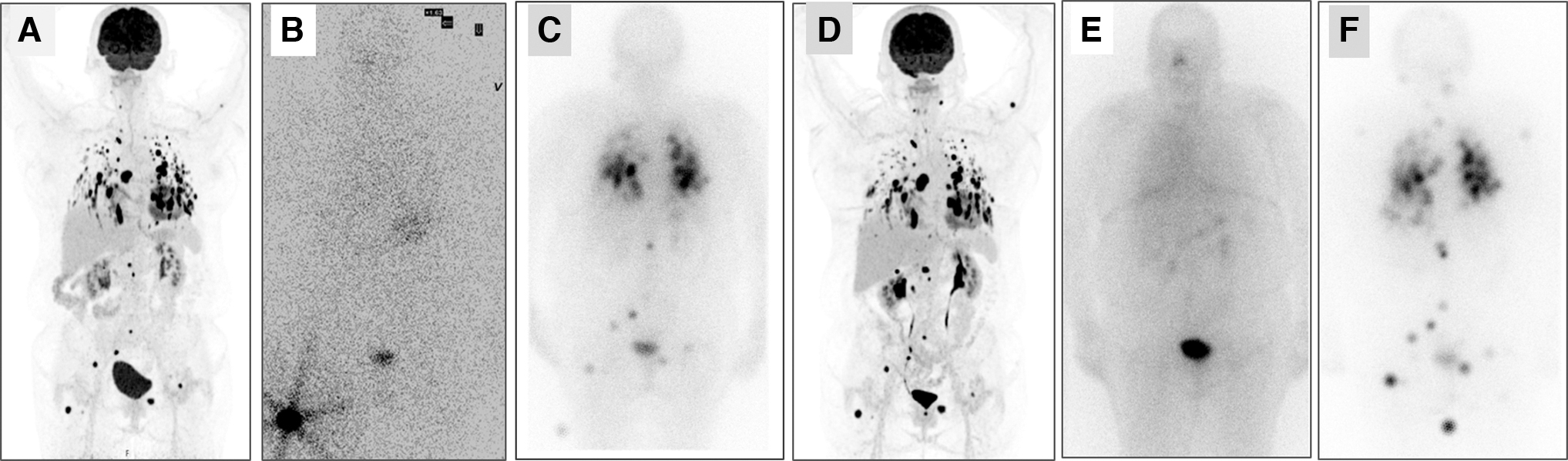
In 2017 the patient was referred to our tertiary care university hospital with progressive metastatic disease. From August 2017 to November 2018, thyroglobulin doubling time (TgDT) was 6 months. The metastases showed very high uptake on 2-[18F]fluoro-2-deoxy-D-glucose (FDG) positron emission tomography/computed tomography (PET/CT) (SUVmax = 34 in target lesions) (Fig. 1).
(
The patient was given the BRAF- inhibitor dabrafenib (Tafinlar®; Novartis) 150 mg × 2 daily for 6 weeks. An recombinant human thyroid stimulating hormone (rhTSH)-stimulated diagnostic scan with 77 MBq (2 mCi) 131I after 4 weeks of dabrafenib showed successful redifferentiation with high radioiodine uptake in the lungs, lymph node, and bone metastases (Fig. 1). Measurements of maximal tolerable activity (MTA), and tumor dosimetry (TuDo) of 3 target lung lesions (TLL) and 1 mediastinal lymph node (TLNL) were performed (Table 1). After 6 weeks on dabrafenib, 11.1 GBq (300 mCi) 131I was administrated, and dabrafenib treatment was stopped 5 days after radioiodine administration.
Measures Before and on Follow-Up for First and Repeat Redifferentiation with Dabrafenib, Each Followed by 131I Therapy
MTA, maximal tolerable activity; TLL, target lung lesions; TLNL, target lymph node lesion; Tg, thyroglobulin.
Four months later, TgDT had increased from 6 to 56 months, a 35% reduction in TLL was measured on computed tomography, and the patient showed substantial clinical improvement (Table 1). An FDG PET/CT showed unchanged very high uptake in the metastatic lesions (SUVmax = 32 in target lesions).
Ten months after the treatment, the disease again progressed, confirmed by diagnostic imaging. Fourteen months after the treatment, a diagnostic rhTSH-stimulated 123I whole-body scan (WBS) and SPECT/CT did not show radioiodine uptake in the metastases (Fig. 1).
An attempt of repeat redifferentiation was initiated 16 months after the first treatment, using the same protocol. An rhTSH-stimulated WBS and SPECT/CT with 77 MBq (2 mCi) 131I after 4 weeks on dabrafenib showed high uptake in the metastases (Fig. 1). Based on the results of MTA and TuDo (Table 1), 13.2 GBq (357 mCi) 131I was administrated. Like the diagnostic scan after four weeks on dabrafenib, the post-therapy scan showed high uptake in the metastases (Fig. 1).
The treatment response parameters five months after repeat treatment are listed in Table 1. In the following months the patient deteriorated gradually. Six months after repeat redifferentiation, treatment with lenvatinib was started. She further deteriorated and died from progressive thyroid cancer 11 months after the repeat redifferentiation, 26 months after first redifferentiation, and 21 years after the primary diagnosis.
Which MAPK pathway inhibitor or combination of inhibitors will be more effective is not known. 1 Some authors have questioned whether the combination of a BRAF inhibitor and MEK inhibitor could be more effective than BRAF inhibitor alone. 1 In a recently published article, Busaidy et al. did not find that the combination of dabrafenib and trametinib was superior in redifferentiation efficacy compared with dabrafenib alone in 53 patients with BRAFV600E mutated RAIR PTC. 3
During the pretreatment with dabrafenib, she improved clinically. We question whether clinical improvement during pretreatment may indicate successful redifferentiation.
There is no agreement about the tumor dose needed for successful 131I treatment of metastases from differentiated thyroid cancer. 131I seems to be less effective for skeleton metastases compared with lymph node or lung metastases. 4,5
We administered 131I based on MTA and TuDo to target lesions (Table 1). The patient had several tiny bone metastases too small for dosimetric measurements. Good partial response was achieved for the lung metastases and stable disease for a solitary TLNL, while the bone metastases progressed slowly. As the numerous lung metastases constituted the predominant part of the total tumor volume, the increase in TgDT and the clinical improvement were primarily a result of the good partial treatment response of the lung lesion.
To our knowledge, this is the first report in which repeat redifferentiation was successfully performed in the same patient with a clinical improvement after each 131I therapy without the simultaneous continuation of long-term MAPK inhibitors.
Footnotes
Acknowledgment
This case report was presented at ATA's Annual Meeting in 2021 (poster 279). A special thanks to Gisle Iversen, MSc for his outstanding help with the images.
Authors' Contributions
T.B. contributed to conceptualization (lead), analyzing data, and writing the original draft and final article. M.J. carried out conceptualization, and was responsible for patient treatment and follow-up. J.D. was involved in conceptualization, analyzing data, and article review and editing. E.L. and O.E. were involved in calculating MTA and performing TuDo.
O.I.H. and M.C. were in charge of target volume measurements. T.B.-G. carried out data analyses, and article review and editing. D.V.N. contributed to conceptualization, supervision, and article review and editing. All authors have controlled the data and reviewed the article.
Written Consent and Institutional Approval
The patient had given a written consent to the use of images and data for possible later publications. According to national rules, an approval of the institutional review board is not required for unapproved use of an approved drug.
Author Disclosure Statement
The authors have nothing to disclose.
Funding Information
No funding was received for this project.