
Abstract
Background:
Thyroid carcinoma >4 cm in size is staged as T3a. The current American Thyroid Association guidelines recommend subtotal/total thyroidectomy and consideration for postoperative radioactive iodine (RAI) treatment for these tumors. In this retrospective cohort study, we aimed to explore the clinical course of large encapsulated thyroid carcinoma without other risk factors.
Methods:
Eighty-eight patients with large (>4 cm) encapsulated well-differentiated thyroid carcinoma resected between 1995 and 2021 were included in this retrospective cohort study. Exclusion criteria were tall cell variant, any extent of vascular invasion, extrathyroidal extension (microscopic or gross), high-grade histology, noninvasive follicular thyroid neoplasm with papillary-like nuclear features (NIFTP), infiltrative tumors, positive resection margin, and cases with follow-up <1 year. The primary outcomes are risk of nodal metastasis at the initial resection, disease-free survival (DFS), and disease-specific survival (DSS).
Results:
The tumor histotype was follicular carcinoma (n = 18, 21%), oncocytic (Hurthle cell) carcinoma (n = 8, 9%), and papillary thyroid carcinoma (PTC; n = 62, 70%). Among PTC, 38 were encapsulated follicular variant, 20 classic type, and 4 solid variant. Four cases had extensive capsular invasion (CI), 61 (69%) had focal CI, whereas 23 did not have CI. Thirty-two cases (36%) were treated with lobectomy/hemithyroidectomy alone, and 55 patients (62%) did not receive RAI. Five patients had nodal metastasis at the time of primary resection, all of whom had classic-type PTC. The median follow-up period was 4.8 years (interquartile range: 3.2–9.7 years). No recurrence, being local, regional, or distant, was observed in the entire cohort, including those patients treated with lobectomy alone without RAI. The 10-year DFS and DSS were 100%, respectively.
Conclusion:
Large intrathyroidal encapsulated well-differentiated thyroid carcinoma without vascular invasion follow an extremely indolent clinical course with negligible risk of recurrence. Lobectomy alone without RAI may be the appropriate treatment strategy for this selected group of patients.
Introduction
In the modern era, risk assessment and stratification are crucial components in the management of differentiated follicular cell-derived thyroid carcinoma. One pathology parameter included in the initial postoperative risk stratification is tumor size. Large tumors defined as tumor with a greatest dimension >4 cm are considered as pT3a and prognostic stage group II in patients ≥55 years using the American Joint Committee on Cancer/Union for International Cancer Control (AJCC/UICC) 8th edition staging manual. 1
The National Comprehensive Cancer Network (NCCN) clinical practicing guideline mandates the following for a well-differentiated thyroid follicular cell-derived carcinoma, including papillary thyroid carcinoma (PTC), follicular thyroid carcinoma (FTC), and oncocytic (Hurthle cell) thyroid carcinoma (OTC), >4 cm in diameter: (1) total thyroidectomy with a preoperative diagnosis of PTC and a pre- or intraoperative finding of >4 cm tumor; (2) completion thyroidectomy with a pathologic diagnosis of well-differentiated thyroid carcinoma >4 cm in lobectomy specimen; and (3) postoperative radioactive iodine (RAI) therapy. 2
Similarly, the American Thyroid Association (ATA) management guidelines recommends near-total or total thyroidectomy for patient with a carcinoma >4 cm (strong recommendation). 3 In addition, ATA recommends consideration for postoperative RAI in these patients, especially when the tumor exhibits other adverse features. Hence, many surgeons and endocrinologists remain uneasy about managing large thyroid carcinoma >4 cm in size conservatively with lobectomy alone and without postoperative RAI scanning and/or ablation.
We have shown previously that encapsulated well-differentiated thyroid carcinoma without extensive vascular invasion or distant metastasis at presentation, regardless of the tumor size, follows an indolent clinical course with zero or near-zero risk of structural recurrence. 4,5 However, such observation was conducted before the introduction of noninvasive follicular thyroid neoplasm with papillary-like nuclear features (NIFTP) when NIFTP was regarded as a form of PTC. 6 –8 The clinical course and the necessity for total thyroidectomy plus postoperative RAI of large encapsulated well-differentiated follicular cell-derived thyroid carcinoma remain to be determined in the post-NIFTP era. Aiming to study the natural course of these lesions, we herein investigated the risk of nodal metastasis and structural recurrence in a retrospective cohort of 88 patients harboring large (>4 cm) intrathyroidal well-differentiated thyroid carcinoma devoid of other risk factors (such as vascular invasion, extrathyroidal extension, positive surgical margin, distant metastasis, or high-grade histology).
Materials and Methods
This retrospective cohort study was approved by the Institutional Review Board (IRB 17-103). A search of the pathology database at Memorial Sloan Kettering Cancer Center (MSKCC, New York, NY) was performed to retrieve cases meeting the following inclusion and exclusion criteria. The inclusion criteria were: (1) a reviewed diagnosis of well-differentiated thyroid carcinoma, including PTC, FTC, and OTC; (2) tumor greatest dimension >4 cm (i.e., AJCC 8th edition pT3a); and (3) encapsulated/well-demarcated carcinoma with or without capsular invasion (CI). Additional foci of subcentimeter papillary carcinoma (formerly known as papillary microcarcinoma) were acceptable.
Exclusion criteria were as follows: (1) high-grade follicular cell-derived nonanaplastic thyroid carcinoma with elevated mitotic count and/or tumor necrosis as defined by the World Health Organization (WHO) classification 5th edition; 9 (2) infiltrative tumor with an infiltrative tumor border permeating between background non-neoplastic follicles; (3) no or short follow-up defined as follow-up <1 year; (4) carcinoma with other risk factors such as PTC tall cell variant, any degree of vascular invasion (focal or extension), gross or microscopic extrathyroidal extension, and/or gross or microscopic positive resection margin; (5) distant metastasis at presentation, and (6) tumors fulfilling the diagnostic criteria of NIFTP defined by the WHO classification 5th edition (Fig. 1). 8,9 All slides were reviewed and diagnosed by Head and Neck Pathologists and all reports re-reviewed by at least one Head and Neck pathologist (R.G. or B.X.) to confirm the diagnosis and document relevant pathologic features.
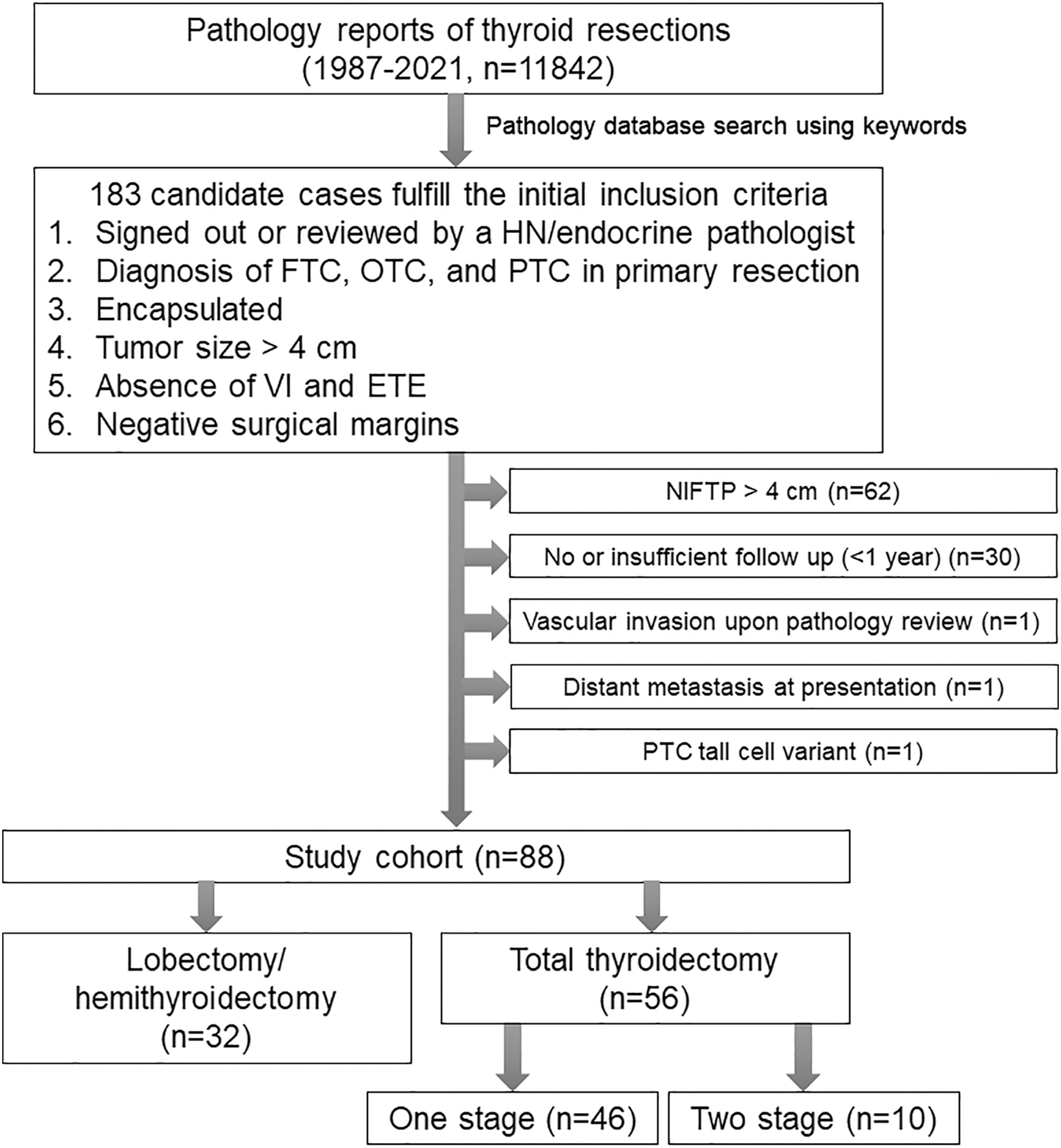
Flow diagram of the cohort selection. ETE, extrathyroidal extension; FTC, follicular thyroid carcinoma; NIFTP, noninvasive follicular thyroid neoplasm with papillary-like nuclear features; OTC, oncocytic thyroid carcinoma; PTC, papillary thyroid carcinoma; VI, vascular invasion.
Five patients harbored encapsulated noninvasive follicular pattern-predominant PTC that did not meet the diagnostic criteria of NIFTP given the presence of the following features: mitotic count 3 per 2 mm2 (10 high-power fields, n = 2), psammoma body (n = 1), very focal tall cell changes (n = 1), and 35% solid growth pattern (n = 1). For simplicity reason, these tumors were classified as encapsulated follicular variant. All included carcinomas are entirely encapsulated with invasion (i.e., invasive encapsulated carcinoma) or without CI (i.e., encapsulated noninvasive carcinoma).
Additional clinicopathologic parameters recorded were sex, age at diagnosis, type of surgery (lobectomy defined as removal of a thyroid lobe, hemithyroidectomy defined as resection of a thyroid lobe and isthmus, or total thyroidectomy), the extent of lymph node sampling during surgery, sampling of the main tumor, number of tumor sections if tumor is representative sampled, diagnosis, the presence or extent of CI, the presence or type of additional subcentimeter carcinoma, postoperative RAI therapy and its dose. Molecular data, when available, were collected from the medical chart.
The primary focus of the study was to determine the frequency of pathological nodal metastasis (pN1 disease) at the time of primary resection, disease-free survival (DFS), and disease-specific survival (DSS).
Results
This retrospective cohort study included 88 patients with a reviewed diagnosis of encapsulated well-differentiated follicular cell-derived carcinoma of >4 cm (i.e., AJCC pT3a) in greatest dimension resected between 1995 and 2021. Given the above-defined inclusion and exclusion criteria, all tumors were intrathyroidal, encapsulated, and devoid of vascular invasion, extrathyroidal extension, or positive resection margin. The clinicopathologic characteristics of the study cohort are provided in Table 1.
Clinicopathologic Characteristics of the Study Cohort Stratified by Types of Surgery
The study cohort includes 88 patients with intrathyroidal encapsulated well-differentiated thyroid carcinoma with negative surgical resection margin. p-Values are obtained using Fisher's exact test for categorical variables and two-tailed Student's t-test for continuous variables.
CI, capsular invasion; CT, classic type; NA, not applicable; RAI, radioactive iodine; TT, total thyroidectomy.
The reviewed diagnoses of the study cohort were PTC (n = 62, 70%), FTC (n = 18, 21%), and OTC (n = 8, 9%). Among patients with PTC, encapsulated follicular variant was the most common subtype (n = 38), followed by classic type (n = 20), and solid variant (defined as ≥50% of solid architecture using WHO classification, 9 n = 4).
The median age of diagnosis was 51 years (range: 18–81 years, interquartile range: 41–61 years). There was a female predominance with a female-to-male ratio of 1.2:1. The median tumor size was 5.0 cm (range: 4.1–12.5 cm, interquartile range: 4.5–5.9 cm). In 69% of cases, either the entire tumor or the entire tumor capsule was submitted for histologic examination to evaluate invasion. In the remaining 31 tumors, the tumor capsule was representatively sampled with a median of 10 sections per tumor examined (range: 3–27, interquartile range: 7–15). CI was identified in 65 cases (74%), being either focal (<4 foci, n = 61, 69%) or extensive (≥4 foci, n = 4, 5%). Twenty-nine patients (33%) had additional foci of subcentimeter PTC (papillary microcarcinoma). Lymph node sampling was performed in 39 cases (44%), including 36 cases with central compartment lymph node excision/dissection, and 3 cases with central and lateral neck dissection.
Molecular testing and/or immunohistochemistry for BRAFV600E and RAS Q61R were performed in a subset of 12 cases. The results are given in Supplementary Table S1. In brief, two of eight PTCs encapsulated follicular variant and one PTC encapsulated solid variant had NRAS Q61R mutations, whereas BRAFV600E mutation was not detected.
During the primary resection, nodal metastasis was confirmed pathologically in five cases (6%, Table 2). The reviewed pathologic diagnoses of these patients were PTC classic type. The frequency of nodal metastasis was 25% (5/20) in PTC classic type, and 0% in PTC encapsulated follicular variant, FTC and OTC. The histotype of the nodal metastasis was PTC in all cases.
Features and Outcome of Five Patients with Nodal Metastasis in the Primary Resection
C, central; C+L, central and lateral; M, male; N, case number; NED, no evidence of disease; PTC, papillary thyroid carcinoma.
All patients with nodal metastasis were subjected to total thyroidectomy. Five of those patients had postoperative RAI with a dose ranging from 50 to 300 mCi. All patients with nodal metastasis had no evidence of disease without recurrence during their follow-up (median follow-up = 12.4 years, range: 1.8–23.1 years).
All patients had clinical follow-up at MSKCC for at least 1 year. The median follow-up period was 4.8 years (range: 1.1–23.1 years, interquartile range: 3.2–9.7 years). Thirty-two (36%) patients received lobectomy/hemithyroidectomy only, whereas the remaining 57 patients had total thyroidectomy. Ten patients were treated with two-stage total thyroidectomy. Compared with patients treated with lobectomy alone, patients treated with total thyroidectomy were associated with additional foci of subcentimeter PTC, postoperative RAI, and longer follow-up (Table 1). Other clinicopathologic parameters did not differ between these two groups.
Fifty-five patients (62%) did not receive postoperative RAI therapy (Fig. 2). Thirty-four patients received postoperative RAI with a dose ranging from 28 to 300 mCi (median: 99 mCi). There was no local, regional, or distant recurrence, or disease-related death in the entire cohort. All but one patient was alive without evidence of disease at the last follow-up. One patient died of other causes (metastatic dedifferentiated liposarcoma) 11.2 years after the resection of thyroid tumor. The 10-year DSS and DFS were 100% in our cohort.
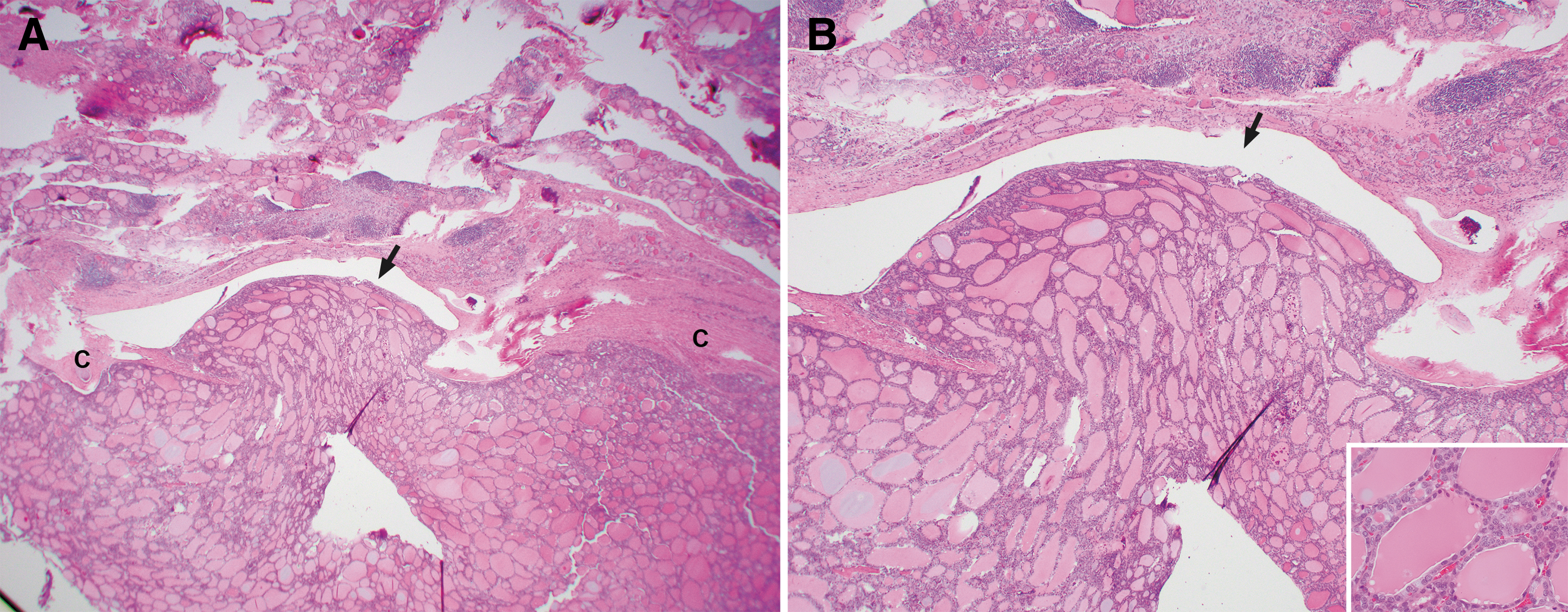
Thyroidectomy specimen from a 54-year-old patient with a minimally invasive follicular carcinoma (4.2 cm in size). The patient was free of disease 11 years and 9 months after diagnosis without radioactive iodine therapy. (
Discussion
Thyroid carcinomas >4 cm in size is traditionally staged as pT3 in AJCC 7th 10 and 8th 1 editions. In addition, a carcinoma >4 cm in size is a major indicator for total thyroidectomy and for consideration of postoperative RAI in multiple major guidelines worldwide, such as the NCCN clinical practicing guideline, 2 the ATA management guideline, 3 the Japanese Society of Thyroid Surgeons/Japan Association of Endocrine Surgeons (JSTS/JAES) guideline, 11 and the British Thyroid Association guideline for the management of thyroid cancer. 12
Most studies on well-differentiated thyroid carcinoma (PTC, FTC, and/or OTC) have found that tumor size >4 cm is an (independent) prognostic factor for overall survival, 13 DSS, 14 –16 recurrence-free survival, 16 –21 and distant metastasis free survival, 14,15,19 supporting the notion that carcinomas >4 cm in size follow a more aggressive clinical course and should be managed accordingly. For example, in a retrospective study of 3965 patients with PTC, Ito et al. reported that the risk of regional and distant recurrence was 8.3% and 3.4% in PTC >4 cm, significantly >4.8% and 1.6% risk in PTC between 2 and 4 cm, and 1.9% and 0.4% risk in PTC ≤2 cm in size. 19 Similarly, FTC and OTCs >4 cm in size were associated with decreased DSS and DFS on multivariate survival analysis. 16 However, not all studies reported tumor size >4 cm as a significant prognostic factor. 22,23 In a retrospective study by Matsuzu et al. including 1088 patients with PTC treated with lobectomy alone and a subgroup of 109 patients with PTC >4 cm, a tumor size >4 cm did not incur a shortened recurrence free survival. 22
The impact of tumor size on prognosis may also in part depend on the histotype and/or microscopic parameters of the thyroid carcinoma. Minimally invasive FTC and OTC, defined by the WHO classification as encapsulated FTC and OTC with CI only but without angioinvasion, 24 appear to be associated with very low, if any, risk of recurrence or mortality. 4,15,25 In a retrospective study of 190 patients with FTC and OTC, Matsuura et al. reported no recurrence or death in 82 patients harboring minimally invasive FTC or OTC, including 22 cases >4 cm in size. 25 Similarly, Cady et al. 26 and van Heerden et al. 15 reported no recurrence or cancer-related death in minimally invasive FTC.
In a group of 61 minimally invasive FTC, O'Neill et al. observed a single case of disease-related death and this patient had widely metastatic disease at presentation. 27 This patient would be considered as ATA high risk given the presence of distant disease at diagnosis. Overall, it appears that minimally invasive FTC and OTC (i.e., carcinomas with CI only) had an excellent prognosis, regardless of the tumor size. Our results further support such observation. In addition, we have expanded the histotype from FTCs and OTCs to encapsulated well-differentiated thyroid carcinoma, which also include PTCs. We herein showed that when stringently selected for to exclude other risk factors (such as vascular invasion, extrathyroidal extension, positive resection margin, high-grade histology and distant metastasis at presentation, large volume of nodal metastasis, e.g., ≥5 positive lymph nodes or nodal metastasis >3 cm), large (>4 cm) encapsulated well-differentiated thyroid carcinoma followed an extreme indolent clinical course with negligible risk of recurrence or disease-specific mortality.
Such observation remained true for the subgroup of 36 patients treated by lobectomy alone and the 61 patients who did not receive postoperative RAI. The results of this study further supports our previous observation that encapsulated well-differentiated thyroid carcinoma, being FTC, OTC, or PTC, without extensive vascular invasion or distant metastasis at presentation followed an indolent clinical course with zero or near-zero risk of locoregional recurrence or distant metastasis, regardless of tumor size. 4,5 Our results, together with other previous studies on minimally invasive PTC, FTC, and OTC, 4,15,25,27 suggest that large intrathyroidal encapsulated well-differentiated thyroid carcinoma can be safely managed with lobectomy alone, rather than the traditional recommendation of total thyroidectomy and postoperative RAI.
From a practical clinical perspective, the primary imaging modality used in the preoperative evaluation of the thyroid gland and cervical lymph nodes is neck ultrasound. Computerized tomography scan of the neck with contrast is performed if there is any suspicion of gross extrathyroidal extension or clinically apparent lymph node metastases. In the absence of preoperative evidence of gross extrathyroidal extension, lymph node metastases, or clinical symptoms of distant metastasis, we do not routinely image outside the neck searching for distant metastasis as the risk of distant metastasis without these clinically features are very low. However, patients are fully informed that the final determination of whether a thyroid lobectomy is the appropriate initial therapy can only be achieved by the integration of preoperative, intraoperative, and postoperative risk stratification. 28,29
Thus, patients opting for thyroid lobectomy understand and accept the possibility that intraoperative and/or postoperative findings could change our recommendation regarding the extent of thyroid surgery that may be required as part of initial therapy. Additional imaging outside the neck is considered in the postoperative period if intraoperative or postoperative findings indicate high-risk features such as gross extrathyroidal extension, histological evidence of extensive vascular invasion, high-grade tumor histology, or if the 6-week postoperative thyroglobulin is inappropriately elevated. So, in clinical practice, the routine search for distant metastasis is reserved for the few cases that have high-risk features identified either intraoperatively or postoperatively to help inform decision making about whether or not a completion thyroidectomy is warranted to facilitate diagnostic/therapeutic use of RAI.
In this study, the frequency of nodal metastasis was 6% (5/88) in the entire cohort, 20% (5/20) in PTC classic type, and 0% in PTC follicular variant, PTC solid variant, FTC and OTC. The extremely low rate (0%) of nodal metastasis in encapsulated follicular-patterned thyroid carcinomas (FTC , OTC, and encapsulated follicular variant of PTC) are consistent with what have been previously reported. 25,30 –32 In addition, we have recently shown that PTC, encapsulated solid variant was enriched with RAS mutations, akin to encapsulated follicular variant. 33 Indeed, among the 12 cases with molecular results, RAS mutations were detected in 2 of 8 PTC encapsulated follicular variant and 1 PTC encapsulated solid variant.
Together, it is now known that encapsulated follicular-patterned and solid thyroid carcinomas are enriched with RAS mutations, have a RAS-like molecular profile, and a very low tendency for lymph node spread, compared with PTC classic type, which typically harbor BRAFV600E mutations, have a BRAF-like molecular signature, and tend to spread to regional lymph node even when encapsulated. 34 –37
One limitation of the current study was that it was a retrospective study containing only a limited number of patients with long-term follow-up. Additional large-scale multicentric/national studies with long-term follow-up, preferably prospective in nature, are needed to validate our findings. Second, not all tumors had their capsule entirely sampled. Complete sampling of the tumor capsule is desired to evaluate the presence and extent of vascular invasion.
In conclusion, large (>4 cm) intrathyroidal encapsulated well-differentiated thyroid carcinoma without other risk factors (such as tall cell variant, vascular invasion, extrathyroidal extension, positive resection margin, distant metastasis at presentation, and large volume of nodal metastasis) is extremely indolent with negligible risk of recurrence or disease-related death, even when treated with thyroid lobectomy alone without postoperative RAI. Tumor size per se should not generally be used to predict risk of recurrence in encapsulated well-differentiated thyroid carcinoma. Consideration may be given in treatment guidelines to recommend lobectomy rather than total thyroidectomy with postoperative RAI in this selected group of patients.
Footnotes
Acknowledgment
A modified version of the abstract was presented at the United States and Canadian Academy of Pathology (USCAP) annual meeting, New Orleans, LA, March 2024.
Authors' Contributions
R.G.: study design, pathology review, article revision. I.G. and R.M.T.: conception, article revision. B.X.: study design, database collection and management, statistics, clinical and pathology review, article drafting.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
Research reported in this publication was supported in part by the Cancer Center Support Grant of the National Institutes of Health/National Cancer Institute under award number P30CA008748 (R.G., R.M.T., and B.X.).
Supplementary Material
Supplementary Table S1