
Abstract

T
While many of the targeted and immunotherapy agents have been available through trials or off-label use since 2015, government approval has only been as recent as 2018 in the United States. 4 Multiple barriers prevent the introduction of these treatments on the global scale. The novel agents are costly and their use requires significant expertise across multiple medical disciplines. Consequently, the current management of ATC places great demands on the health care system. Despite these difficulties, several centers have reported impressive results using these new treatments. One high-volume cancer centre in the United States has reported a recent cohort of all-comer patients with a 1-year survival of 59%, 4 and as high as 94% in a subgroup of patients with BRAF-mutated ATC.
These results represent a paradigm shift in ATC treatment. However, there is no data on how these advances have been implemented in a publicly funded health system where access to novel targeted therapy is limited. In Canada publicly funded health system, access to targeted therapy is primarily through compassionate access programs administered by pharmaceutical companies. To further investigate this question, our group completed a national study to evaluate outcomes of ATC in Canada in the era of molecular testing and targeted therapies, focusing on disease-specific patient outcomes, while also evaluating the more general issue of the introduction of novel, resource-intense treatments into a publicly funded, single-payer health system where BRAF/MEK inhibitors are not funded by payers.
A retrospective review of patients with a histologically confirmed ATC from January 2016 until October 2021 was performed. Patients were enrolled from 14 tertiary care centers across Canada. Patients were identified through pathology reports, preexisting databases of ATC, institutional databases, and cancer registries. Institutional research ethics board approval was granted at every site (Local REB #11553, see Supplementary Data for site specific REB #). The primary outcome measure was overall survival (OS). Secondary outcomes included the proportion of patients that received molecular testing and use of targeted therapy, as well as regional and temporal variation in treatment across Canada, and over the study period.
Data were extracted from patient charts using a common, predetermined collection sheet. Lead investigators of the study regularly met with coinvestigators to ensure uniformity in data collection. Data collected included patient demographics and comorbidity including Charlson Comorbidity Index. Disease stage and mutation status were collected, as well as treatment modality (surgery, radiation therapy, conventional cytotoxic chemotherapy, targeted therapy, and/or immunotherapy). OS was measured from date of histologic diagnosis, with patients censored at date of last follow-up.
All statistical analyses were performed using Stata 13.0 (StataCorp LP, College Station, TX). Categorical variables were analyzed using a two-tailed Pearson Chi-square test, with a Fisher's exact test utilized in lieu when variable values were ≤5, while continuous variables were analyzed using a one-way ANOVA. OS was estimated using a Kaplan–Meier method with the log-rank test used to assess between-group differences. A Cox proportional-hazards model with Efron's method of tie handling was used to assess relative risk (hazard) of death, with Schoenfeld residuals used to base our proportional-hazards assumption tests. Hazard ratios were adjusted for age, sex, and disease stage when appropriate.
A total of 152 patients with ATC were included from the 14 participating sites across Canada. Generally, the number of patients in each province was closely aligned with relative population of that province, with British Columbia being an exception.
The proportional use of BRAFV600E testing increased over the study period (Table 1). This rose from 13% in 2016 to 91% by 2021 (p < 0.001). Testing was performed using both next-generation sequencing methods and immunohistochemistry. When tested, BRAFV600E was positive in 41% of patients. Although the adoption of BRAF testing in Canada increased significantly over the period of interest, the use of BRAF-directed targeted therapy was not uniform across the country, being exclusively used in Quebec and Ontario (p = 0.011). All 152 patients were included in the survival analyses. Median OS was 6.8 months, while 1- and 2-year OS were 34% [95% confidence interval (CI) 26–42%] and 19% [CI 12–26%], respectively (Fig. 1). Patients with BRAFV600E-mutated ATC had a 2-year OS of 23% versus 13% in BRAF wildtype ATC patients; hazard ratio (HR) = 0.57 [CI 0.33–0.96] (Fig. 1).
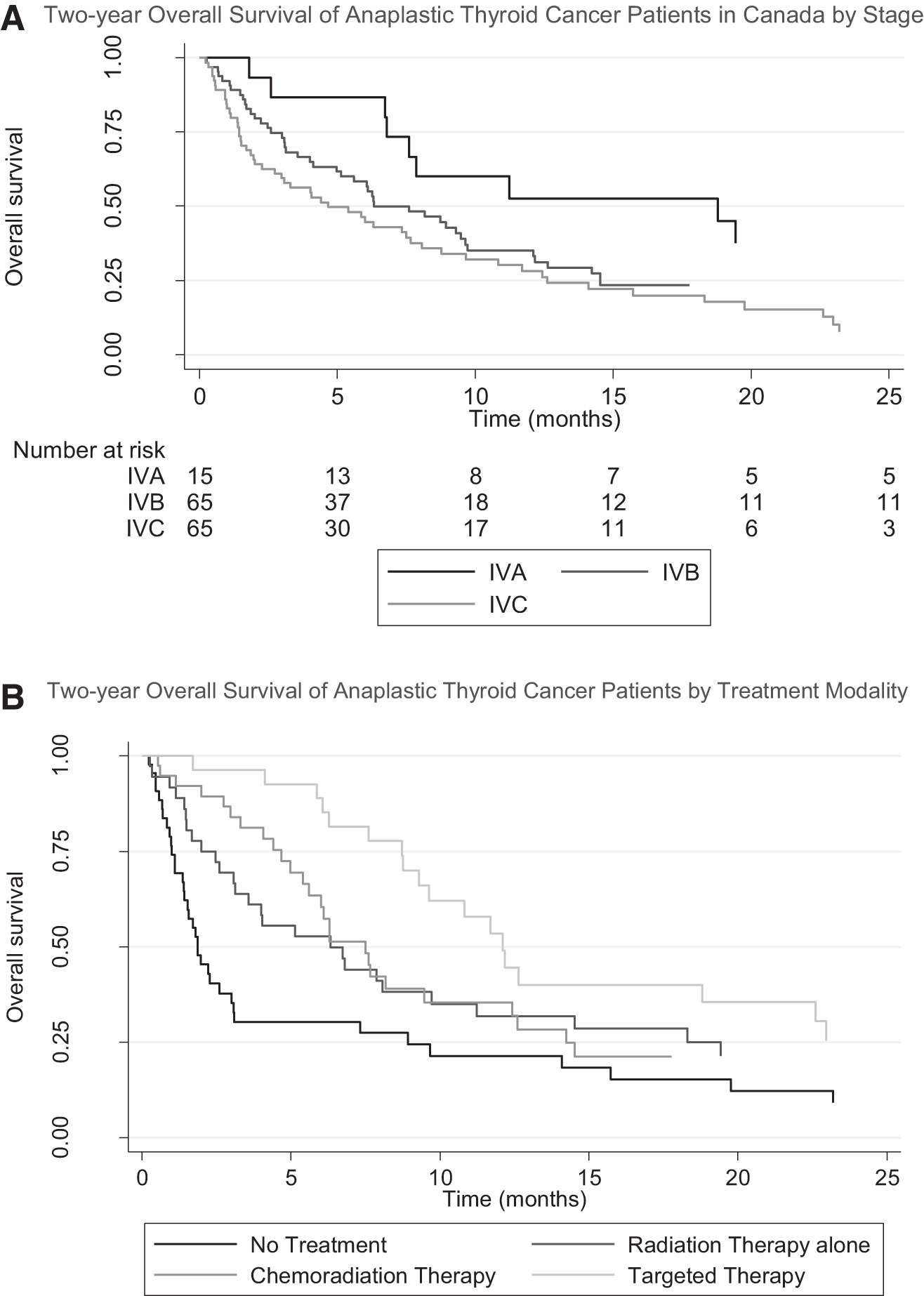
OS by
Cohort Demographics
American Joint Committee on Cancer Staging Manual 8th Edition.
AJCC, American Joint Committee Cancer.
Most patients received radiotherapy either alone or with cytotoxic chemotherapy. Eighty patients, over half of the patients in the cohort, received surgery. However, the nature of surgeries was extremely heterogenous. Procedures varied from partial thyroidectomies to extensive resections including tracheal and laryngeal resections. Only 10 of these patients had confirmed R0 or R1 resections.
In total, 27 patients received targeted therapy. The combination of dabrefinib and trametinib was the most used targeted therapy with 21 patients receiving it. Six patients received Lenvatinib as the sole form of targeted therapy. No patients received targeted therapy before surgical resection. Patients who received BRAF-targeted therapy had an improved 2-year OS (HR = 0.52; CI 0.31–0.87; p = 0.014) with a median OS of 12.1 months, which is more than twofold higher than in patients not receiving targeted therapy (5.4 months). No other treatment modality was associated with improved OS.
This study is the largest review of the treatment of ATC in Canada. It is one the largest reviews of ATC in a publicly funded health care system and the first to examine the adoption of targeted therapy in a publicly funded system.
The 1-year OS in this study of 34% was comparable to other studies from periods predating targeted therapy. 4,5 However, the estimated 1- and 2-year OS was significantly lower than the estimates reported in the only large review from the era of targeted therapy. The group out of MD Anderson Cancer Center reviewed 152 patients from a single-institution treated between 2017 and 2019 and reported 1 and 2-year OS estimates of 59% (CI, 49–67%) and 42% (CI, 30–53%), respectively. However, it is difficult to compare this study to our own. Our study endeavors to report on the survival of ATC across the entire country, whereas the data from MD Anderson represent the findings of a single, highly specialized institution. Regarding patients having received targeted therapy, the median OS of patients in the current study was 12.1 versus 15.7 months in the MD Anderson study. 4 This similarity suggests that the adoption of targeted therapy in Canada has achieved an improvement in OS close to that seen in a centre pioneering the use of the novel treatments.
Regional differences were seen in the adoption of BRAF testing and use of targeted therapy. This is not surprising given differing practice patterns and the fact that health care systems in Canada are provincially administered. In cases of rare and complicated diseases such as ATC, a national strategy should be considered to reduce national variability and achieve the best results across the country. We also hope that this multicentre study improves the understanding, availability, and use of BRAF inhibitors in Canada. With BRAF-directed targeted therapies now considered first-line treatment for BRAF-mutated ATC, having access to such therapies in a timely fashion can have a significant effect on survival outcomes and quality of life for close to 40% of the Canadian ATC population.
Conclusion
Patients with ATC in Canada have survival estimates comparable to many published reports. In addition, when used, targeted therapy for ATC have been successful in Canada, although their adoption has not been uniform. As the use of targeted therapy becomes consistent across the country, we can expect even greater improvements in the survival of patients with ATC.
Footnotes
Authors' Contributions
M.K.G. (conceptualization, methodology, writing-first draft, supervision, project administration), A.-M.M. (conceptualization, methodology, investigation, data curation), N.S. (investigation, data curation), A.C.N. (conceptualization, investigation, data curation, writing-review), F.L. (investigation, data curation, writing-review), A.E. (conceptualization, investigation, data curation, writing-review), H.L. (investigation, data curation), N.W. (investigation, data curation), J.D.P. (conceptualization, investigation, data curation, writing-review), B.G. (investigation, data curation), E.J. (investigation, data curation), S.H.M.v.U. (writing-review), M.B. (investigation, data curation), F.L. (investigation, data curation), N.S. (investigation, data curation), T.S. (investigation, data curation), A.M.M. (investigation, data curation), G.B.M. (investigation, data curation), P.H.F. (investigation, data curation), L.F. (investigation, data curation), S.G. (investigation, data curation, writing-review), S.P.C. (investigation, data curation), E.P. (investigation, data curation), T.A. (investigation, data curation), A.C. (investigation, data curation), J.C.D. (investigation, data curation), M.R. (investigation, data curation), M.C. (investigation, data curation), K.R. (investigation, data curation), A.M. (conceptualization, methodology, writing-first draft, supervision, project administration).
Author Disclosure Statement
M.K.G.: no conflicts to disclose; A.-M.M.: no conflicts to disclose; N.S.: no conflicts to disclose; A.C.N.: no relevant disclosures, but research funding from Novartis, Droplet Biosciences, and Lapcorp, Consultant for NEED Oncology, Patent UWO3 Score; F.L.: no conflicts to disclose; A.E.: none relevant but research funding Merck, consultant Bristol Myers Squibb; H.L.: no conflicts to disclose; N.W.: no conflicts to disclose; J.D.P.: no conflicts to disclose; B.G.: no conflicts to disclose; E.J.: no conflicts to disclose; S.H.M.v.U.: no conflicts to disclose; M.B.: no conflicts to disclose; F.L.: no conflicts to disclose; N.S.: no conflicts to disclose; A.M.M.: no conflicts to disclose; G.B.M.: no conflicts to disclose; P.H.F.: no conflicts to disclose; L.F.: no conflicts to disclose; S.G.: no conflicts to disclose; S.P.C.: no conflicts to disclose; E.P.: no conflicts to disclose; T.A.: no conflicts to disclose; A.C.: no conflicts to disclose; J.C.D.; no conflicts to disclose; M.R.: no relevant conflicts but has worked as consultant for Sanofi Genzyme, Bayer, Eisai; M.C.: no conflicts to disclose; K.R.: no conflicts to disclose; A.M.: no conflicts to disclose.
Funding Information
No funding was received for this article.
Supplementary Material
Supplementary Data