
Abstract
Background:
Understanding of changes in salivary and lacrimal gland functions after radioactive iodine therapy (131I-therapy) remains limited, and, to date, no studies have evaluated dose–response relationships between absorbed dose from 131I-therapy and dysfunctions of these glands. This study investigates salivary/lacrimal dysfunctions in differentiated thyroid cancer (DTC) patients six months after 131I-therapy, identifies 131I-therapy-related risk factors for salivary/lacrimal dysfunctions, and assesses the relationships between 131I-therapy radiation dose and these dysfunctions.
Methods:
A cohort study was conducted involving 136 DTC patients treated by 131I-therapy of whom 44 and 92 patients received 1.1 and 3.7 GBq, respectively. Absorbed dose to the salivary glands was estimated using a dosimetric reconstruction method based on thermoluminescent dosimeter measurements. Salivary and lacrimal functions were assessed at baseline (T0, i.e., immediately before 131I-therapy) and six months later (T6) using validated questionnaires and salivary samplings, with and without stimulation of the salivary glands. Statistical analyses included descriptive analyses and random-effects multivariate logistic and linear regressions.
Results:
There was no difference between T0 and T6 in the level of parotid gland pain, nor was there difference in the number of patients with hyposalivation, but there were significantly more patients with dry mouth sensation and dry eyes after therapy compared with baseline. Age, menopause, depression and anxiety symptoms, history of systemic disease, and not taking painkillers in the past three months were found to be significantly associated with salivary or lacrimal disorders. Significant associations were found between 131I-exposure and salivary disorders adjusted on the previous variables: for example, per 1-Gy increase in mean dose to the salivary glands, odds ratio = 1.43 [CI 1.02 to 2.04] for dry mouth sensation, ß = −0.08 [CI −0.12 to −0.02] mL/min for stimulated saliva flow, and ß = 1.07 [CI 0.42 to 1.71] mmol/L for salivary potassium concentration.
Conclusions:
This study brings new knowledge on the relationship between the absorbed dose to the salivary glands from 131I-therapy and salivary/lacrimal dysfunctions in DTC patients six months after 131I-therapy. Despite the findings of some dysfunctions, the results do not show any obvious clinical disorders after the 131I-therapy. Nevertheless, this study raises awareness of the risk factors for salivary disorders, and calls for longer follow-up.
Clinical Trials Registration:
Number NCT04876287 on the public website (
Introduction
Approximately 10,600
Thyroidectomy followed by vectorized internal radioactive iodine therapy (131I-therapy) is the usual treatment for differentiated thyroid cancer (DTC). 3 However, because salivary glands are able to absorb and accumulate iodine, patients might suffer from salivary glands inflammation, and symptomatic or chronic salivary disorders after 131I-therapy. 4 Salivary disorders include any alteration in the quantity or quality of saliva production, that is, reduced salivary flow (hyposalivation) and/or altered saliva biochemistry, and the feeling of dry mouth (xerostomia). 5
A distinction is made between unstimulated and stimulated salivary flows, the former corresponding to rest, conversation, or sleep, the latter corresponding to feeding and swallowing. Salivary composition changes may indicate sialadenitis or acinar dysfunction. Subsequent effects can include mouth infections, altered perception of flavors, and impaired ability to swallow and digest food, leading to reduced quality of life. Disorders of the lacrimal glands have also been described after 131I-therapy. 6 However, there is still uncertainty regarding the incidence of such outcomes. 7 While several studies have focused on short-term symptoms (1–3 months after 131I-therapy), few studies have assessed mid-term (6 months later) or long-term (1 year or more) symptoms.
Furthermore, the knowledge of the risk factors for salivary/lacrimal disorders associated with thyroid cancer treated by 131I-therapy is limited by the paucity of studies on the subject, highlighting the need for further studies. 8 A better understanding of these factors may allow the identification of patients likely to develop salivary disorders after 131I-therapy, and thus enable treatment and follow-up to be adapted accordingly.
Finally, the radiation dose–response relationship between 131I-dose and the occurrence of salivary and lacrimal disorders has been poorly studied, with the administered activity (AA) used as a proxy for the dose absorbed by the salivary glands. 8,9 However, due to several factors such as iodine biokinetics or the ability of the salivary glands to absorb iodine, the AA may not be adequate to accurately characterize the exposure. The use of an appropriate dosimetric method could allow a better estimation of the absorbed dose to the salivary glands, and then a more precise evaluation of the dose–response relationship.
To address these issues, the Salivary dysfuncTions After Radioiodine Treatment (START) study was set up in 2020. Based on the data from the START study, this article aims to (1) describe the incidence of salivary and lacrimal dysfunctions in DTC patients six months after 131I-therapy, (2) identify post-therapy risk factors, and (3) assess the dose–effect relationship between 131I-exposure and salivary and lacrimal dysfunctions.
Materials and Methods
Study population
The START cohort study has been described in detail elsewhere.
10
In brief, START is a prospective study, which included 139 DTC patients in 2020, aged 18 years and over, who have undergone thyroidectomy, and awaiting a complementary 131I-therapy at Pitié-Salpêtrière Hospital (Paris, France). Inclusion was nonrandomized, according to a systematic and consecutive selection of patients. Patients were split into 2 groups according to the administered 131I-activity: 1.1 GBq (N = 45) and 3.7 GBq (N = 94). Thyrotropin (TSH) elevation protocol was
Patients who had previously received 131I-therapy or who were likely to receive several 131I-therapies in the 18 months after enrollment were excluded. The number of patients required for the study was calculated for a statistical power of 80% with a first order risk of 5% and a theoretical odds ratio (OR) of salivary complications of 3.
Approvals from the local ethical committee have been received (Comité de Protection de Personnes Sud Mediterranée III, ID: 20.01.24.56149, and Agence Nationale de Sécurité des Médicaments, ID: 2020-A00208-31). The protocol was registered and posted on the
Radiation dose assessment
Three LiF thermoluminescent dosimeters (TLDs) from APVL (Saint-Cyr-sur-Loire, France) were placed under both earlobes and at the sternal notch before 131I-therapy, and removed after 5 days, immediately before the post-therapy scan. A computational method was developed to convert the TLD readings, that is, skin dose into salivary glands cumulated activity. 10 The methodology based on TLD measurements has been described elsewhere for several organs, but not for salivary glands. 11 –15 For that purpose, skin dose per unit nuclear disintegration at the TLD location was calculated using the International Commission on Radiological Protection female computational phantom and the Monte Carlo N-Particle Transport code. 16,17
The computations were checked thanks to dedicated experiments, one consisting in irradiating TLDs placed at several locations on a RANDO head phantom with an 131I-capsule inserted at the salivary gland location. 18 The TLD at the sternal notch was used to subtract the contribution of the thyroid remnant to earlobe TLD (measured from ultrasound), but it was found to be negligible. The calculated cumulated activity was then converted into absorbed doses to the right and left salivary glands (D r and D l , respectively) using S-factor. 19
Then, a mean dose to the salivary glands (MD) was calculated from D r and D l to be included in analyses. In addition, the mean dose to the salivary glands per unit of administered activity (MD/A) was calculated. Administered activity (AA) of 131I (1.1 or 3.7 GBq) was also considered in analyses.
Questionnaire-based outcome assessment
Mid-term symptoms were assessed using validated questionnaires on salivary complaints (Moreddu et al. questionnaire), lacrimal dryness (Ocular Surface Disease Index [OSDI©] Questionnaire), anxiety and depression (Hospital Anxiety and Depression [HAD] scale), nutrition (visual analog scale assessment), and quality of life (Medical Outcome Study Short Form-36). 20 –23 Information on potential systemic diseases was provided by the patients' medical records and confirmed or supplemented directly by questions to the patients. All the questionnaires were filled at baseline, that is, immediately before 131I-administration (T0) and six months later (T6) for all patients, during a face-to-face meeting with a trained interviewer, as part of the treatment follow-up at the hospital.
Salivary collection and characterization
Whole saliva was collected for each patient during 5 minutes at T0 and T6, before and after salivation stimulation, using the Navazesh's standardized method, allowing the calculation of salivary flows before and after stimulation. 24 In brief, patients were asked not to eat, drink, chew gum, brush their teeth, or smoke for at least 60 minutes before saliva collection. Saliva was sampled under quiet and restful conditions for five minutes by spitting out into a tube, in an upright position, following three steps: (1) collection of unstimulated whole saliva, (2) stimulation of the salivary glands by chewing a gum, (3) collection of stimulated whole saliva.
Saliva samples were collected at the same time of the day between 9am and 1pm for both T0 and T6. The concentrations of sodium, potassium, chlorine, calcium, and amylase in the saliva were also assessed at T0 and T6. Salivary and lacrimal dysfunctions were characterized as both binary and continuous outcomes as summarized in Table 1.
Summary of the Different Outcomes Considered in the Salivary dysfunctions After Radioiodine Treatment Study and Their Definitions
An OSDI score >12 corresponding to non-normal dryness of the eye. 27
OSDI, Ocular Surface Disease Index.
Study covariates
Several variables, listed in Table 2, were collected during the enrollment visit to be tested as potential risk factors for salivary and lacrimal dysfunctions. Qualitative and quantitative variables were introduced into the models without being modified.
List of the Potential Confounders
ATC, Anatomical Therapeutic Chemical; HAD, Hospital Anxiety and Depression; MOS SF-36, Medical Outcome Study Short Form-36; TNM, tumor-node-metastasis.
Statistical analyses
Patient characteristics at T0 and T6 and exposure descriptions (means and standard deviations, or frequencies and percentages) were examined in relation to the administered activity (1.1 and 3.7 GBq groups). Differences between both groups were assessed using Pearson's chi-squared test for categorical data, and t-test for continuous data. Differences for time-varying variables of interest between T0 and T6 were assessed using the McNemar test and t-test for paired comparisons.
Random-effects logistic and linear regressions were used to test established or potential risk factors that may be associated with salivary or lacrimal dysfunctions. Random-effects multivariate logistic and linear regressions, providing OR and beta coefficients (β), respectively, with their 95% confidence intervals (CIs), adjusted on the significantly associated risk factors allowed to assess associations between 131I-exposure and salivary and/or lacrimal dysfunctions. Sensitivity analyses were conducted using fixed-effect models in which subject effects controlled for explicitly, thereby providing control for any characteristic of a study subject that is time invariant over the period of study T0 to T6.
Analyses were performed using the GLIMMIX procedure of SAS V.9.4 statistical software for Windows (SAS Institute, Cary, NC). An alpha level of 0.05 was considered as significant.
Results
Among the 139 patients in the study, 3 left the cohort (1 exclusion for refusal of 131I-therapy, 1 death before follow-up at T6, 1 patient lost to follow-up). Thus, analyses included 136 patients, with 44 and 92 patients treated with 1.1 and 3.7 GBq, respectively (Fig. 1). The mean age at inclusion was 47.1 (±14.1) years, 71% were women, 85% had papillary cancer, and 47% had thyroid remnants after 131I-therapy (Table 3). There was no statistically significant difference between the two 131I-activity groups in terms of sex and age.
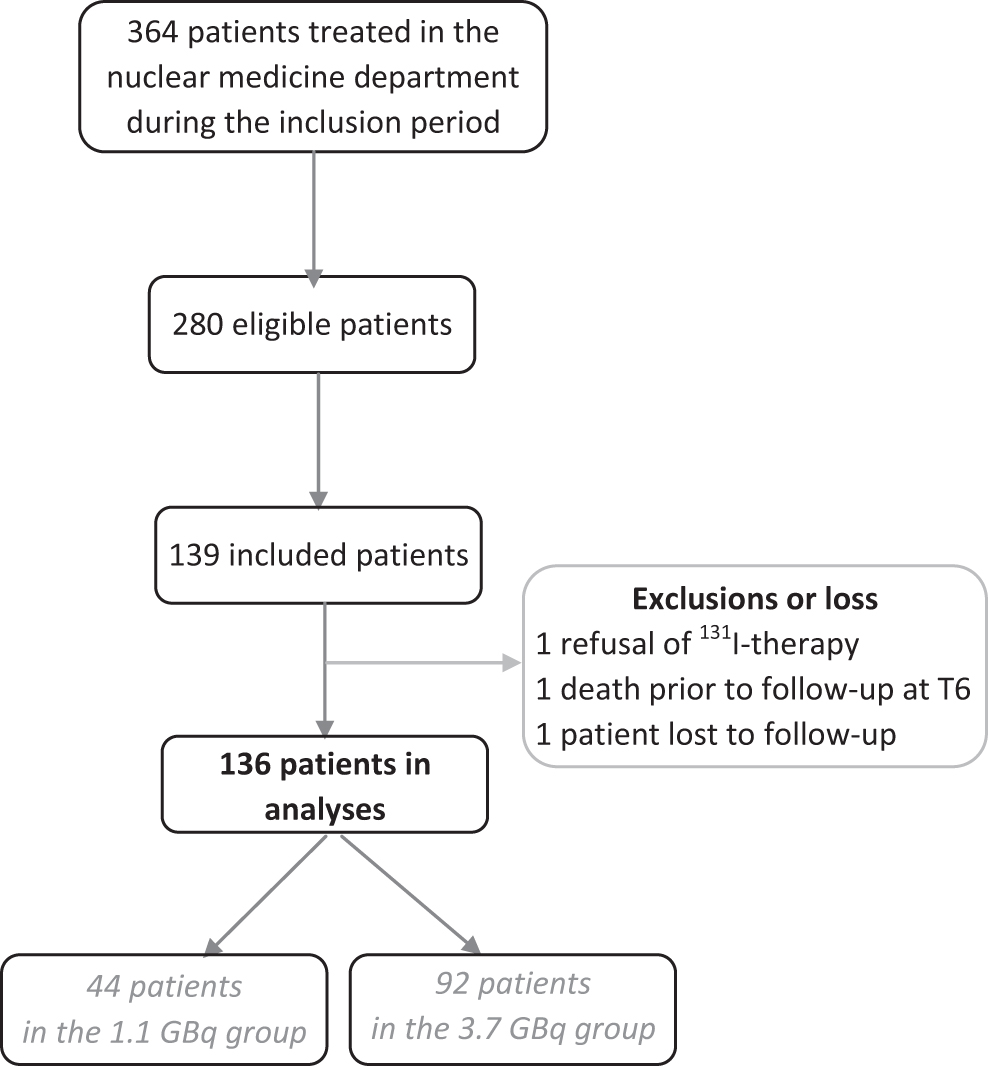
Flow chart of patients participating in the study.
Baseline Characteristics of Differentiated Thyroid Cancer Patients, Exposure, and Factors of Interest
Statistically significant values are in bold.
p-Value of t-test for continuous variables, or chi-squared test for categorical variables between the two activity groups.
n (%).
Mean (±SD).
Dr and Dl , absorbed doses to the right and left salivary glands, respectively; MD, mean of absorbed dose to the right and left salivary glands; MD/A, mean of absorbed dose to the salivary glands per unit of administered activity; SD, standard deviation; T0, evaluation before radioiodine treatment; T6, six months visit after radioiodine treatment.
The mean salivary gland doses were similar for the left and right glands within each 131I-activity group, respectively, while the mean dose to the salivary glands per unit of administered activity was similar for both 131I-activity groups (0.6 [±0.3] mGy/MBq) (Table 3).
Clinically, there was no difference between T0 and T6 in the number of patients with parotid gland pain or with hyposalivation defined from a dichotomization of salivary flows (Table 4). However, there were significantly more patients with dry mouth sensation and dry eyes after therapy compared with baseline, with 30 (22%) and 23 (17%) who complained of these symptoms at T6 and not at T0, respectively (Table 4). There was no correlation between salivary flows or hyposalivation and dry mouth sensation (p = 0.70) (Supplementary Table S1).
Comparison Tests for Time-Dependent Variables between Before (T0) and Six Months (T6) After 131I-Therapy
Statistically significant values are in bold.
n (%).
Mean (±SD).
t-Test for paired comparison.
McNemar test for paired comparison.
New cases were coded as “yes” when the outcome was recorded as “yes” at T6 and “no” at T0.
MCS, mental component summary; PCS, physical component summary; VAS, visual analog scale for nutrition.
Notably, the use of painkillers and the level of anxiety and depression decreased at T6 compared with T0. For paraclinical evaluations, salivary flows decreased at T6, but significantly only for the stimulated flow. Finally, amylase and mineral ion concentrations were significantly higher at T6 than at baseline (Table 4).
Age, menopause, depression and anxiety symptoms, and history of systemic diseases were risk factors for gland disorders, and painkiller intake in the past three months was associated with a decrease in salivary disorders (Supplementary Tables S2 and S3). There was no correlation between salivary and lacrimal outcomes (Supplementary Table S1).
Multivariate regression analyses quantified relationships between 131I-exposure and salivary or lacrimal dysfunctions, adjusted for age at the time of interview, baseline anxiety and depression score (HAD scale), history of systemic diseases, menopause status, and painkiller use in the past three months (Tables 5 and 6). For clinical outcomes, no significant association was found between 131I-exposure and stimulated or unstimulated hyposalivation. However, dry mouth sensation was positively associated with mean salivary gland dose (OR = 1.43 [CI 1.02 to 2.04] for a 1-Gy increase), and with the administered 131I-activity (p = 0.04).
Adjusted Odds Ratio for the Relationship between 131I-Exposure and Salivary and Lacrimal Disorders (Binary Variables) at T6
Statistically significant values are in bold.
Exposure indicators were introduced separately in the models, adjusted for age at the time of interview, anxiety and depression score (HAD scale), history of systemic diseases, menopause status, and painkillers intake in the past three months.
AA, administered activity of 131I; CI, confidence interval; n/a, not applicable; OR, odds ratio.
Adjusted Linear Regression Coefficient for the Relationship between 131I-Exposure and Salivary and Lacrimal Disorders (Quantitative Variables) at T6
Statistically significant values are in bold.
Exposure indicators were introduced separately in the models, adjusted for age at the time of interview, anxiety and depression score (HAD scale), history of systemic diseases, menopause status, painkillers intake in the past three months.
A significant positive association was observed between administered 131I-activity and dry eyes (OR = 3.58 [1.19–10.81] in patients treated with 1.1 GBq vs. before treatment), but not for those treated with 3.7 GBq. The latter trend was confirmed when the OSDI score, used to assess lacrimal dryness, was analyzed using linear analyses.
For paraclinical outcomes, the association between mean dose to the salivary glands and stimulated saliva flow was significant after adjustment for confounders, with an average decrease of −0.08 [−0.12 to −0.02] mL/min per 1-Gy increase in mean salivary gland dose. The change in saliva biochemical concentrations remained significant only for potassium, with an average increase of 1.07 [0.42 to 1.71] mmol/L per 1-Gy increase in mean salivary gland dose.
Discussion
The START study is the first study to evaluate salivary disorders, using both objective and subjective indicators, in relation to the absorbed dose to the salivary glands in DTC patients treated by 131I-therapy. The results suggest no clinically significant impact of 131I-therapy on the salivary glands, but do suggest changes in stimulated saliva flow, salivary potassium concentration, and dry mouth sensation in relation to the dose absorbed by the salivary glands. In addition, increased dry eyes as assessed by the OSDI tool was reported in patients treated in the low administered 131I-activity group.
In this study, salivary disorders were assessed in a variety of ways, leading to different incidence values (Table 4). In the review by Clement et al. about DTC patients treated with 131I, objective and subjective salivary disorder symptoms ranged between 37% to 72% and 16% to 54%, respectively. 29 Whereas most studies using a subjective criterion reported significant associations with 131I-exposure, conflicting results were found when objective salivary indicators were used. 29 In a prospective study of 25 patients, Vieira et al. 30 found a nonsignificant increase in salivary flows (with and without stimulation) 3 months after 131I-therapy, whereas, in a prospective study of 56 patients, Hesselink et al. 9 found a significant decrease in stimulated and unstimulated saliva flows.
In addition, significantly lower flows were found in 131I-treated patients compared with noncancer patients, 31 and a significant association was found between 131I-administration (yes/no) and stimulated saliva flow in DTC patients. 8 In our study, we reported a positive and significant association between 131I-exposure and dry mouth sensation six months post-therapy, and a significant decrease in stimulated flow at T6 in relation to 131I-dose, but not for unstimulated flow. Our study, therefore, confirms some discrepancies between the results from subjective and objective outcomes, and highlights the lack of reference tools for the assessment of salivary disorders.
In other studies, lacrimal dysfunction, ocular dryness, or abnormalities revealed by the Schirmer test were found significantly more frequent in 131I-exposed patients than in unexposed patients, but no study showed an association between 131I-activity levels and lacrimal gland disorders, assessed both objectively and subjectively, while incidences ranged from 4% to 25.3%. 6,29,32 –34 In our study, we observed an increased OR and score for dry eyes after 131I-therapy, with 17% of the patients reporting dry eyes at T6 while they did not before. Surprisingly, associations were higher and significant only for the 1.1 GBq 131I-activity group compared with the 3.7 GBq group.
We may suppose that other risk factors not taken into account in analyses may obscure this relationship. Dose–response analysis was not possible as the absorbed dose to the lacrimal gland was not assessed in this study. We can hypothesize that the dose to the lacrimal gland does not correlate entirely with the activity delivered. Nevertheless, our study of lacrimal disorders is based on a subjective assessment using a validated questionnaire. An objective measurement of dry eyes would be useful to confirm these results.
Moreover, although this study shows some significant associations for both lacrimal and salivary disorders with 131I-administration, these disorders were not correlated, suggesting that the sensitivity to iodine and the underlying biological mechanisms are different for these organs. It would appear that no pathophysiological relationship between the lacrimal and salivary glands is expected. Each type of gland may be affected by 131I, but the mechanisms could be different and could perhaps explain the rather large differences between lacrimal and salivary dysfunction in dose–response relationships.
Therefore, the creation of a composite criterion is innovative and interesting, as it allows to consider both objective and subjective indicators, including lacrimal and salivary disorders. The association between 131I-activity and the composite criterion was positive but nonsignificant, therefore, did not provide evidence of a clinical impact of 131I on the salivary and lacrimal glands.
Regarding sialochemistry, significant relationships after adjustment for confounders were found only between 131I-exposure and potassium concentration, among a large set of mineral ions and enzymes tested. Noteworthy, the composition of saliva is actively modulated during transport through the ductal system, for example, sodium and chloride are absorbed and potassium is excreted in the saliva. As 131I is mainly concentrated in the ductal system after 131I-therapy, the emitted β-radiation may generate luminal debris, which may lead to narrowing of the ducts, and would explain the change in saliva composition. 9 To our knowledge, only three studies have assessed salivary composition in DTC patients after 131I-therapy, showing discrepant results, possibly linked to different collection time. 9,35,36
Very few studies have assessed the dose–response relationship between 131I-exposure and salivary disorders, and only 1 study has evaluated this relationship in a well-controlled statistical model: in 179 patients, Almeida et al. found a statistically significant linear relationship between administered 131I-activity (30–450 mCi) and stimulated flow adjusted for age, sex, and xerostomic drug use, but not with unstimulated flow. 8,33,37 The authors showed that increased age and the use of xerostomic drugs were significantly associated with decreased saliva flows, in particular stimulated flow. 8
Moreover, hypothyroidism and stress can modify the composition and decrease the flow of saliva, although the exact mechanism is unknown, what may have disrupted the change in salivary flows between T0 and T6, which have been assessed in analyses. 38,39 In such a study, it is essential to consider risk factors to avoid confusion bias.
One of the strengths of our study is its design, where the cases are their own controls, allowing to automatically control for individual risk factors that are not time dependent. 40,41 In relation to this design, both fixed-effect and random-effects regression models have been used to assess potential associations between 131I-therapy and dysfunctions. Under random-effects models, we do not condition out the unique study identifier (i.e., subject effect); instead, a random-effect model where this variable is treated as a random intercept is fitted. An alternative approach is to use conditional logistic regression to obtain fixed-effect estimates; this approach also was used, thus conditioning the effect of the subject being “conditioned out” of the model, leading to similar conclusions (results not shown).
In our random-effects regression models, we were able to test a large number of potential cofactors, and to fit our multivariate models to the significant cofactors. This enabled identifying menopause, history of systemic diseases, not taking painkillers, age, and the level of anxiety–depression as risk factors for salivary disorders after 131I-therapy. This adjusted analysis provides more information about the relationship between the treatment and the studied outcomes than before-and-after studies, which account for most of the studies on the subject.
Other strengths of our study lie in the assessment of adjusted dose–response relationships considering not only the administered activity, but also the dose to the salivary glands, which has never been done before. This study is innovative as it is the first to use calibrated TLDs to assess the absorbed doses to the salivary glands, whereas other studies generally use the administered activity as proxy. 8,9 Indeed, iodine uptake by the salivary glands can be modified by the uptake of the thyroid remnants, the “iodine status” of the patient before the therapy, and by other biokinetic parameters. Accurate estimation of absorbed doses to organs is a time- and resource-consuming process based on repeated single photon emission computed tomography imaging.
In this study, the dose to salivary glands was found to be 0.6 (±0.3) mGy/MBq, which is in agreement with previous studies based on imaging where doses ranged between 0.4 and 0.8 mGy/MBq. 42 –45 The availability of organ dosimetry has thus provided accuracy in the estimation of dose–response relationships. Nevertheless, the results of logistic and linear regression analyses for the absorbed dose to the salivary glands are consistent with those obtained for the administered activity.
Limitations concern potential biases related to the study design, which were minimized by a rigorous protocol, involving hospital visits that were as similar as possible at baseline and at T6 (face-to-face interview, using identical questionnaire). Patients who received more than one 131I-therapy were excluded from the study even if an evaluation of repeated 131I-therapies would be interesting. Nevertheless, due to the small number of patients with unstimulated or stimulated hyposalivations as described using the validated thresholds for moderate hyposalivation, the results may lack statistical power. In fact, one interpretation of our results might be that 131I-exposure can disrupt stimulated salivary flow, but to too small an extent, that is, not enough to cause moderate hyposalivation as described by Ericsson and Hardwick. 25
Other reasons could be that our indicators may not be sensitive enough to account for hyposalivation, or that there really is no correlation between objective and subjective measurements potentially due to a difference in sensitivity patients with objectively measured functional disorders. In addition, this article focused only on mid-term symptoms at six months after 131I-therapy, as acute symptoms in the short terms have been studied elsewhere. 46 However, long-term symptoms are lacking in this article, and will be analyzed at the 18-month follow-up. Finally, the potential effects of the few symptoms revealed after 131I-therapy, discussed in this article, on the occurrence of other clinical effects (e.g., quality of life or caries) deserve further study.
Conclusions
This study confirms the possible occurrence of salivary and lacrimal disorders in patients treated with 131I for thyroid cancer. Despite the findings of some dysfunctions, the results do not show any obvious clinical disorders after the 131I-therapy. This study confirms the risk factors of these disorders and brings new knowledge on the dose–response relationships, involving the absorbed dose to the salivary glands based on an accurate dosimetric reconstruction. This study now calls for a longer follow-up, for studying the quality of life of patients after 131I-therapy, and for investigating the epigenetic changes that may contribute to an increased sensitivity to ionizing radiation. 47
Footnotes
Acknowledgments
The authors express their gratitude to all the patients included in this study, and all the medical staff for their valuable assistance. Also, we thank Dr. Sophie Ancelet for her careful help in the statistical analyses part.
Authors' Contributions
Cl.B. and M.O.B. did the acquisition of the financial support. Cl.B. and M.O.B. with C.L.L., D.B., and G.A. conceived and designed the START study. C.B., A.B., and M.O.B. conducted the study. A.T.L., T.C., D.B., Cé.B., and C.H. managed the dosimetry part, that is, the reading of the dosimeters, the implementation and validation of the method for the calculation of the dose to the salivary glands, and the estimation and interpretation of the doses.
Ca.B., F.M., M.S., L.L., and C.L.L. were the clinicians and radiophysicists in charge of treating patients at the Pitié Salpêtrière Hospital. D.B.R. developed the most appropriate statistical method for the study. C.B. performed the statistical analyses and drafted the article. All coauthors revised the report and approved the final version. Cl.B. and M.O.B. are responsible for the overall content as the guarantors of this article.
Author Disclosure Statement
The authors of this article declare no relationships with any companies, whose products or services may be related to the subject matter of the article. They declare no conflicts of interest.
Funding Information
The START study was supported by an internal IRSN funding set up to enhance exploratory research projects.
Supplementary Material
Supplementary Table S1
Supplementary Table S2
Supplementary Table S3