
Abstract
Objective:
Treatment options in Graves' disease (GD) are limited and do not target the underlying autoimmunity, and relapse rates following a course of antithyroid drug (ATD) reach 50%. Previous research has shown promising results for a role of vitamin D in GD. We aimed to investigate whether vitamin D reduces failure to enter and sustain remission in patients with GD treated with ATD.
Design:
A multicenter, double-blinded, randomized placebo-controlled trial comparing vitamin D 70 mcg once daily (2800 IU) or placebo. The intervention was given first as add-on to ATD treatment, maximally 24 months, and then for 12 months after ATD cessation. Inclusion period was from 2015 to 2017 and study completion by December 2020. Patients included were adults with a first-time diagnosis of GD treated with ATD. Exclusion criteria included pregnancy and glucocorticoid treatment. The primary endpoint was failure to enter and sustain remission defined as relapse of hyperthyroidism within 12 months after ATD cessation, inability to stop ATD within 24 months, or radioiodine treatment or thyroidectomy. Two hundred seventy-eight patients were included in the study, and 4 patients withdrew consent. No adverse effects were found.
Results:
Participants were aged 44 ± 14 years at enrollment and 79% were female. The risk of failure to enter and sustain remission was 42% [95% confidence interval (CI) 33–50%] in the vitamin D group and 32% [CI 24–40%] in the placebo group corresponding to a relative risk of 1.30 [CI 0.95–1.78].
Conclusions:
Vitamin D supplementation did not improve the treatment of GD in patients with normal or insufficient vitamin D status. Thus, supplementation with high-dose vitamin D cannot be recommended for GD.
Study registration:
Introduction
Graves' disease (GD)
Vitamin D has been proposed as a potential modulator of autoimmune diseases, including autoimmune thyroid diseases. 6 –10 In the Vitamin D and Omega-3 trial, supplementation with vitamin D was shown to reduce the incidence of autoimmune disease, although the number needed to treat was high. 11 Three intervention studies have investigated the effects of vitamin D in GD and found faster restoration of euthyroidism. 12 –14 However, the studies were small and of short duration, and the implications of vitamin D for the prognosis of GD are unknown.
We performed a randomized controlled trial testing the hypothesis that supplementation with high-dose vitamin D in patients with newly diagnosed first-time GD would reduce the risk of failure to enter and sustain remission with ATD. We chose a pragmatic trial design with the intent of a high level of generalizability.
Methods
This was a placebo-controlled, double-blinded multicenter trial among patients with a first-time diagnosis of GD randomized (ratio of 1:1) to daily oral supplementation with vitamin D3 or identical placebo.
Participants
Recruitment was performed by monthly screening of patients referred to 1 of the 7 endocrine outpatient clinics in the Central Denmark Region with a diagnosis code of E05* (thyrotoxicosis of any cause) according to the International Classification of Diseases version 10. Potential participants were identified by review of medical charts and approached at their visit to the clinic or by letter. We included men and women able to speak and read Danish, aged 18–80 years, and with a first-time diagnosis of GD. A diagnosis of GD was considered in those who at diagnosis had suppressed levels of thyrotropin (TSH), levels of triiodothyronine (T3) and/or thyroxine (T4) above reference range, and a positive TRAb test necessitating treatment with ATD.
We excluded patients treated with ATD for more than three months, patients with Graves' orbitopathy necessitating treatment with glucocorticoids, patients with planned radioiodine treatment or thyroid surgery, and those with a history of hyperthyroidism including previous treatment with ATD. Patients were also excluded if they received vitamin D supplementation >10 μg/day, which they were unwilling or unable to stop or reduce. Additional exclusion criteria were pregnancy, chronic granulomatous disease, persistent hypercalcemia (ionized calcium >1.40 mmol/L), impaired kidney function (estimated glomerular filtration rate <45 mL/min), active malignant disease, treatment with immunomodulatory drugs, alcohol or drug abuse, allergy toward components of study medication, or major comorbidity as determined by the treating physician.
Treatment
Participants were randomly assigned to supplementation with cholecalciferol 70 μg (2800 IU) per day or matching placebo prescribed as one daily tablet at mealtime. The Pharmacy Department Central Denmark Region utilized a computer program (
As standard ATD, participants were treated with either methimazole or propylthiouracil according to the national guideline (
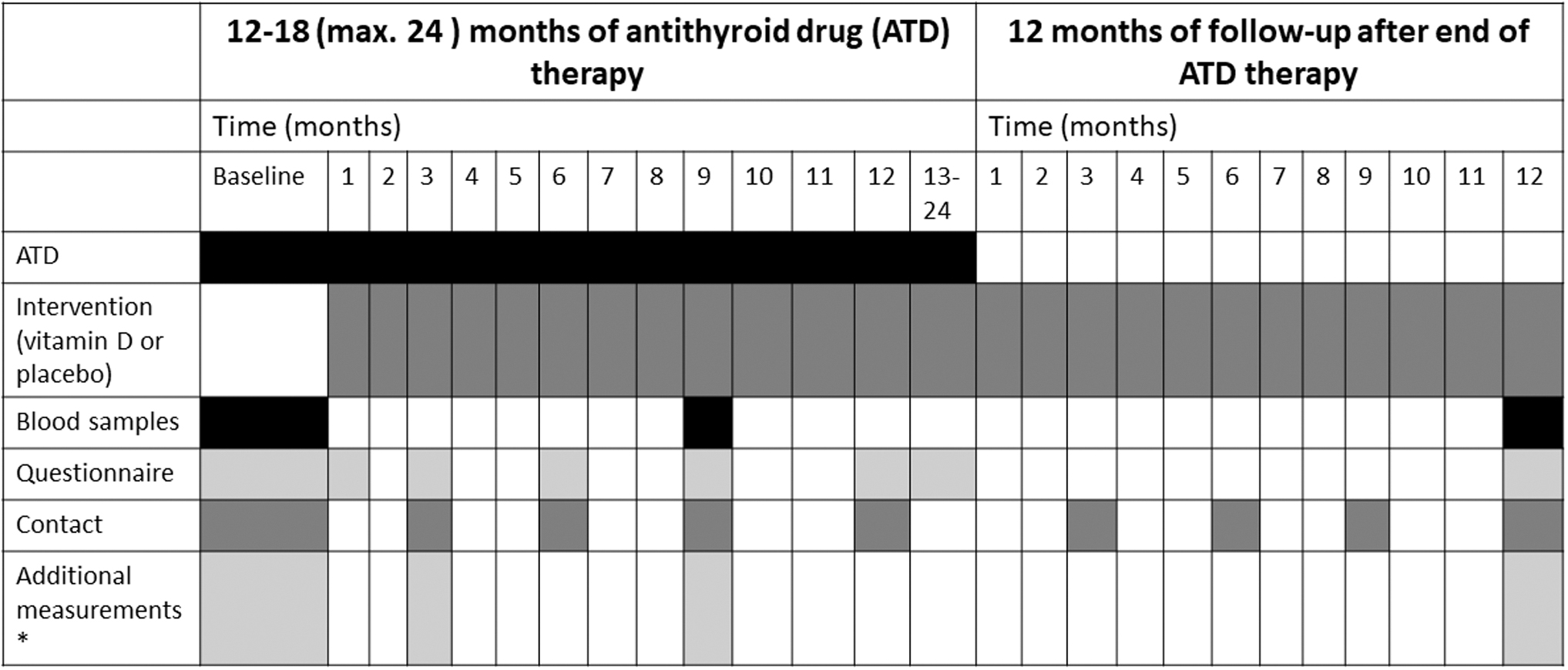
Timeline of the study. *In a subgroup of participants (n = 86), we tested muscle strength, postural balance, blood pressure, arterial stiffness, bone mass density, body composition, and we estimated bone microarchitecture and bone strength.
Outcomes
Primary outcome was the proportion of participants with failure to enter and sustain remission. This was a composite endpoint of (1) relapse, defined as (a) recurrence of hyperthyroidism (TSH <0.1 IU/L) or (b) repeated ATD treatment within 12 ± 1 months after ATD discontinuation or (2) referral for radioactive iodine or thyroid surgery at any time during the study or (3) inability to stop ATD treatment within 24 months after ATD initiation.
Secondary outcome was the risk of relapse (as defined above) and the influence of age, sex, vitamin D status, and smoking status, and the effect on quality of life (QoL).
Measurements
Blood samples were collected at baseline, after nine months, and at the EOS. Questionnaires including assessment of QoL (using ThyPRO-39 15 ), adherence, side effects, and use of vitamin D supplements outside the protocol were sent by email on nine occasions throughout the study. Additionally, participants were regularly contacted by emails (10 times) to improve adherence to protocol. Outcomes were prospectively assessed by review of medical charts and recorded in an electronic database. 16 In a subgroup of patients (n = 86), we previously reported the effect of intervention on arterial stiffness, muscle strength, and QoL. 17,18 Unblinding of the entire cohort was done when all outcome data were on file.
Biochemistry
Blood samples were collected in the morning in the fasting state. Total plasma levels of 25(OH)D [25(OH)D2 + 25(OH)D3] were analyzed by isotope dilution liquid chromatography tandem mass spectrometry with intra-assay coefficients of variation of 5.4% (at 33 nmol/L) and 10% (at 113 nmol/L). Analyses of 25(OH)D were performed in batches. The levels of TRAb, TSH, free triiodothyronine (fT3), and free thyroxine (fT4) were measured as part of clinical follow-up at the local hospital laboratories available to each outpatient clinic. The TSH reference range was 0.3–4.5 mIU/L at all laboratories.
Statistics
We hypothesized that vitamin D supplementation could reduce the risk of failure to enter and sustain remission to two thirds of the usual level (i.e., from 50% to 33%). This would require a sample size of N = 130 patients in each group, with power of 0.80 and two-sided significance p < 0.05. We counted the number of dropouts upon the inclusion of the planned sample size of 260 participants (N = 18, vitamin D group N = 10) and enrolled substitutes with identical randomization. This change in protocol was decided after study commencement but before study analysis with the intent to assure study power.
Baseline characteristics are presented as frequency (percentage) for categorical variables and mean with standard deviation (SD) or median with interquartile range (IQR) for continuous variables. To assess differences between groups, categorical variables were analyzed with a chi-square test, while continuous variables were evaluated with a two-sample t-test or the Wilcoxon rank-sum test as applicable. The primary outcome was assessed by calculating the risk ratio (RR) with a 95% confidence interval [CI].
We used an intention-to-treat (ITT) approach including all subjects who had been randomized and had received at least one dose of study medication. In 44 subjects (n = 23 vitamin D, n = 21 placebo), outcomes could not be determined due to, for example, study withdrawal or exclusion (Fig. 2). They were included in the ITT assuming either a best-case scenario (all experienced a treatment success, i.e., were in remission of hyperthyroidism) or a worst-case scenario (all had failure to enter and sustain remission, as defined above). The best-case scenario is reported if not otherwise stated.

Flowchart depicting identification, treatment allocation, and follow-up of participants. In the intention-to-treat analysis, all randomized subjects were included in the analysis. Please see the Methods section for details. Upon the inclusion of the planned study population of 260 participant, we counted the number of dropout (N = 18, 10 in the vitamin D group) and enrolled substitutes with identical randomization.
In per-protocol analyses, we included all participants in whom outcomes could be assessed.
In a subanalysis, we used Cox regression to assess the risk of relapse at any given time after ATD discontinuation until 12 ± 1 months in per-protocol analyses. The proportional hazard ratio assumption was tested using log-log plots.
We conducted logistic regression analyses to investigate potential interactions between the intervention and various factors. In prespecified analysis, we tested for interaction with baseline 25(OH)D status (categorized as insufficient [<50 nmol/L, <20 ng/mL] or replete) and prior supplementation with vitamin D (yes or no). Additionally, we explored any interaction with factors associated with relapse risk, including age (older than or younger than 40 years), time since diagnosis (above or below 35 days), smoking status (current or not), and sex. If significant interaction was detected, groups were analyzed separately for the effect of intervention, which is presented as odds ratio (OR) with CI. Using mixed modeling, we analyzed the effect of vitamin D on the change in TRAb, fT4, and fT3 at 3 and 9 months in a subgroup of participants.
QoL scores were transformed to the 0–100 ThyPRO range, where a higher score indicates more symptoms. We analyzed the effect of vitamin D on QoL using linear mixed modeling with time and randomization group and their interaction as fixed factors and participants as random effects. The model validation was inspection of QQ plots of the residuals.
A p-value of <0.05 was considered significant. Data were analyzed using STATA version 15 (STATA Corp. LP, College Station, TX). Study results are reported in accordance with the CONSORT statement on reporting parallel group randomized trials. 19
Ethics
All participants gave written informed consent. The trial was performed in accordance with the Declaration of Helsinki 2013. The trial was approved by the Central Denmark Region Committees on Health Research Ethics (1-10-72-568-12). The trial was prospectively registered at
Results
We screened 3767 patients and found 1100 patients with GD, which was a first-time diagnosis in 816 patients (Supplementary Table S1). From this cohort, 278 patients were enrolled and randomized (Fig. 2) to either vitamin D supplementation (n = 140) or placebo (n = 138). The inclusion period was from March 15, 2015, to December 31, 2017, and data collection was completed by December 2020.
Baseline characteristics were balanced between randomization groups (Table 1). Overall, participants were aged 44 ± 14 years and 79% were female. They had been treated with ATD for a median of 25 days (IQR = 11–47) and had biochemically verified thyrotoxicosis. At inclusion, 35% of participants were vitamin D insufficient [25(OH)D level <50 nmol/L]. The number of dropouts was comparable between groups (Fig. 2).
Baseline Characteristics of Participants
Not necessitating treatment (no glucocorticoids).
Baseline 25(OH)D was missing in one patient in the vitamin D group.
25(OH)D, plasma 25-hydroxyvitamin D; ATD, antithyroid drug; IQR, interquartile range; SD, standard deviation; TRAb, thyrotropin receptor autoantibodies.
Study outcomes are summarized in Table 2. In the ITT analysis (n = 278) applying the best-case scenario, risk of failure to enter and sustain remission was 42% [CI 33–50%] in the vitamin D group and 32% [CI 24–40%] in the placebo group. This corresponded to an increased relative risk of 1.30 [CI 0.95–1.78] with vitamin D (p = 0.10). Using the worst-case scenario, we found similar results with a risk of failure to enter and sustain remission of 58% [CI 49–66%] in the vitamin D and 47% [CI 39–56%] in the placebo group (p = 0.07). The improvement of QoL during the study was not affected by vitamin D supplementation (Fig. 3).
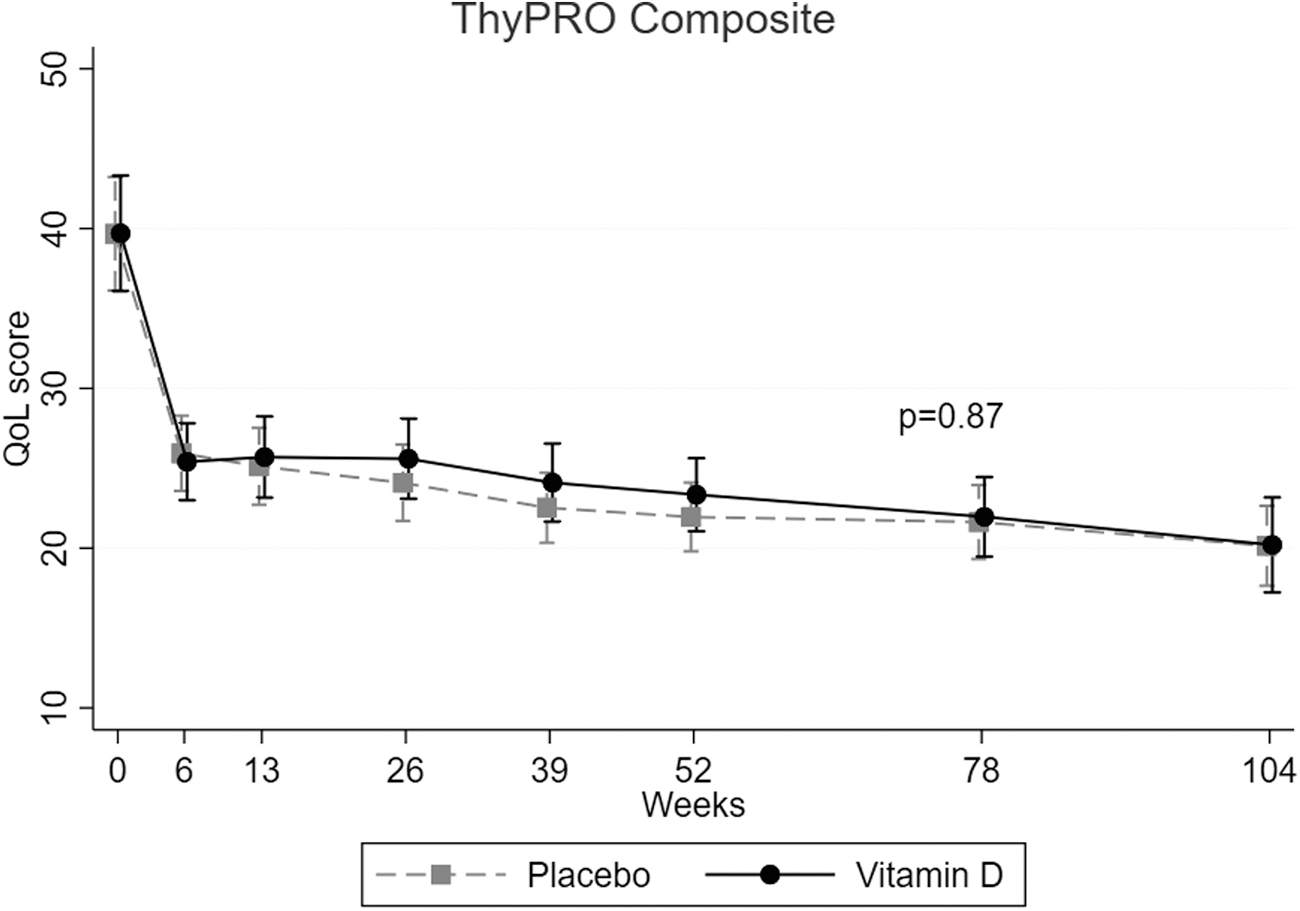
The effect of vitamin D on QoL in patients with Graves' disease during treatment with antithyroid drugs and subsequent remission. Data were collected using the ThyPRO-39 (scores transformed to a 0–100 scale), with a higher score indicating worse QoL or more symptoms. The ThyPRO-39 Composite Scale summarizes mental and social domains and Overall QoL. Data were analyzed using linear mixed modeling with time and randomization group and their interaction as fixed factors and participants as random effects. QoL, quality of life.
Primary and Secondary Outcomes of the DAGMAR Study
Effect of vitamin D (2800 IU/day) vs. placebo on the course of disease in Graves' disease treated with antithyroid drugs. The primary endpoint was a composite of the three secondary outcomes.
CI, 95% confidence interval; DAGMAR, vitamin D and graves' disease: morbidity and relapse reduction.
In per-protocol analyses (n = 234), the risk of failure to enter and sustain remission was 50% [CI 40–59%] in the vitamin D group and 38% [CI 29–47%] in the placebo group (RR = 1.32 [CI 0.98–1.77], p = 0.06).
In per-protocol analyses restricted to patients tapered off ATD (n = 183), the risk of relapse was 33% [CI 24–44%] in the vitamin D group and 23% [CI 15–32%] in the placebo group (RR = 1.48 [CI 0.92–2.38], p = 0.10).
As shown in Figure 4, the estimated hazard ratio for risk of relapse with vitamin D supplementation in the per-protocol analysis was 1.56 [CI 0.89–2.72] (p = 0.12). The time to relapse and the duration of ATD among participants with a relapse were comparable between randomization groups (data not shown).
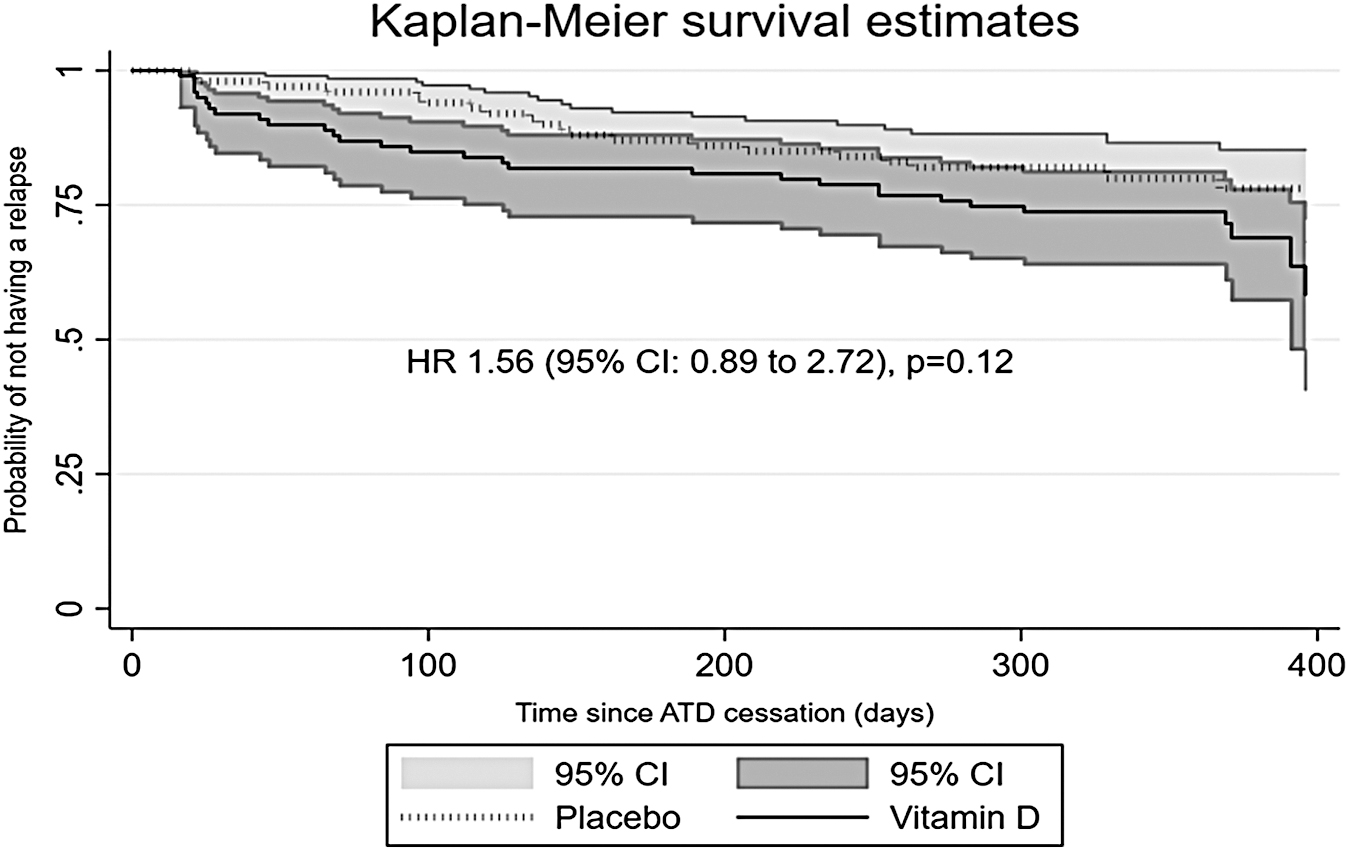
Kaplan–Meier plot of the probability of not having a relapse among participants tapered off ATD. Per-protocol analysis. ATD, antithyroid drug.
The supplemented group included a higher rate of current smokers (borderline significant). In regression analysis, correcting for current smoking did not change the estimated OR for failure to enter and sustain remission with vitamin D supplementation (data not shown). Thus, the uneven proportion of smokers between randomization groups did not influence our results.
The 25(OH)D level at nine months was measured in a subgroup (N = 101, equally randomized). The mean (SD) 25(OH)D level was 107 (21) nmol/L in the vitamin D group and 55 (30) nmol/L in the placebo group, and nine participants reached a level above 125 nmol/L (50 ng/mL). The nine-month 25(OH)D level was significantly associated with failure to enter and sustain remission and with relapse, presumably a mirror of randomization effect (data not shown). These associations as well as the estimated RR with supplementation were unaffected by omitting participants with 25(OH)D >125 nmol/L (data not shown).
In 43% (n = 44), failure to enter and sustain remission was established as the inability to stop ATD within 24 months of treatment. From review of medical charts, the reasons for continued ATD prescription beyond 24 months were ATD requirements and positive TRAb (n = 32) or signs of Graves' orbitopathy (n = 2) with no significant differences between groups. In 10 cases, 5 randomized for vitamin D, reasons were less clear. The duration of ATD treatment (below or above 12 or 18 months) was not associated with the risk of relapse (data not shown).
In a regression analysis of failure to enter and sustain remission (ITT), there was no interaction between the intervention and sex, level of TRAb, use of vitamin D supplementation before study inclusion, or baseline vitamin D status (insufficient vs. replete). We also explored the effect of supplementation among patients with a baseline 25(OH)D level below 35 nmol/L (16%) and found no effect (p = 0.91). However, the effect of intervention depended on smoking status.
Smoking and vitamin D
We found significant interaction between intervention and current smoking (p = 0.02). In nonsmokers (n = 217), vitamin D conferred an increased risk of failure to enter and sustain remission (OR = 1.95 [CI 1.10–3.45], p = 0.02), whereas among smokers (N = 61), the estimated effect of vitamin D had the opposite direction with an OR = 0.43 [CI 0.15–1.26] (p = 0.12). Similarly, we found unfavorable effects of vitamin D on risk of relapse among nonsmokers (OR = 2.13 [CI 1.06–4.26], p = 0.03) but no effect among smokers (OR = 0.56 [CI 0.10–3.10], p = 0.51). In the per-protocol analysis, results were similar (p interaction = 0.03) (data not shown). Baseline 25(OH)D level differed with smoking status (nonsmokers vs. smokers: 64 ± 26 nmol/L and 54 ± 30 nmol/L, p = 0.04). When we adjusted the main analysis for baseline 25(OH)D level, the interaction between intervention and current smoking was unchanged (p = 0.016) and effect estimates were similar (data not shown).
Effect of vitamin D on markers of thyroid function
As previously reported, 17 the intervention did not affect the changes in levels of fT3, fT4, and TRAb at 3 and 9 months (N = 86) (Fig. 5).
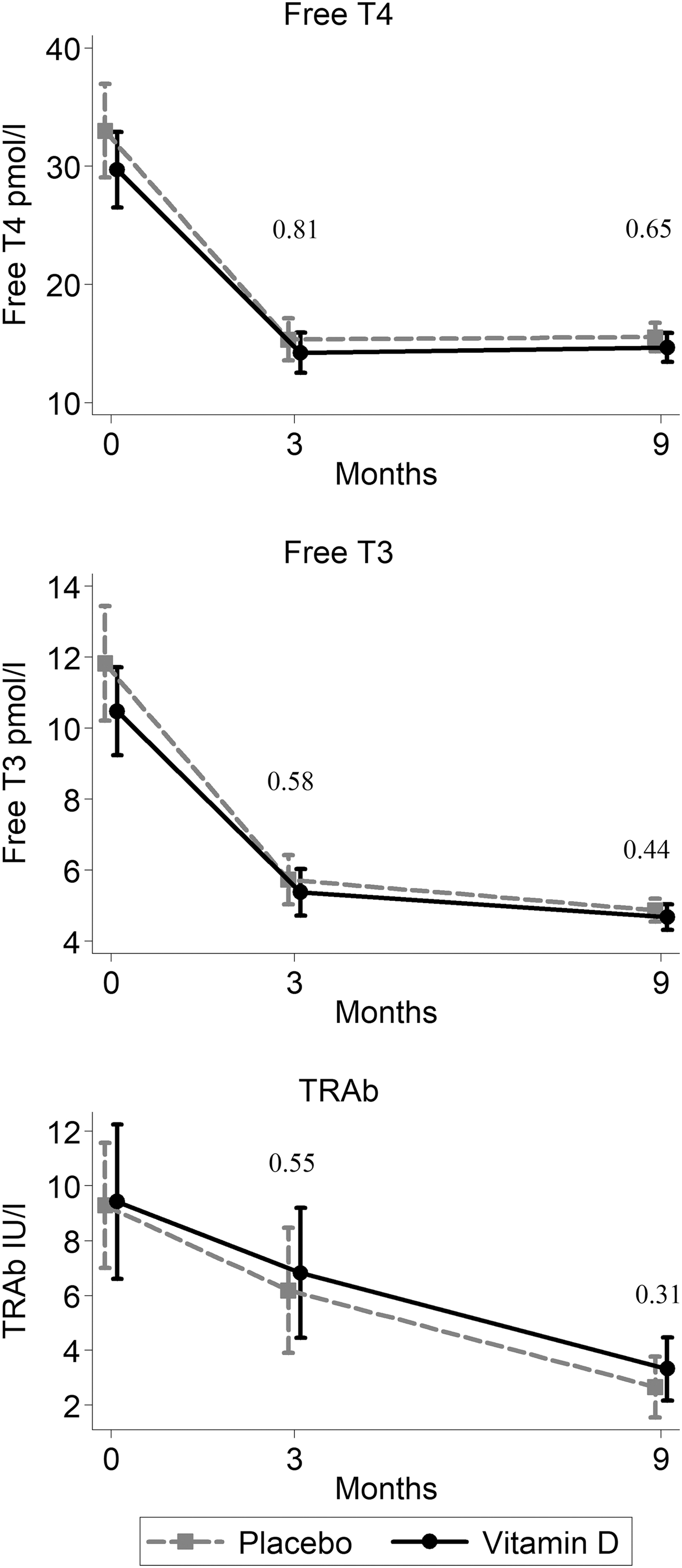
Effect of nine months of supplemental vitamin D vs. placebo on fT3, fT4, and TRAb. N = 86 with available 25(OH)D at both 3 and 9 months. Group mean and standard deviation. p-Values refer to mixed model analysis of difference in change between groups at 3 and 9 months. 25(OH)D, 25-hydroxyvitamin D; fT3, free triiodothyronine; fT4, free thyroxine; TRAb, thyrotropin receptor autoantibody.
Adherence to intervention and side effects
The proportion of responders who reported to comply with study medication 6 or 7 days per week was 96%, 91%, 89%, 80%, and 72% at 1½, 6, 12, 18, and 24 months, respectively. The level of 25(OH)D increased significantly with intervention, and after nine months, the change in level of 25(OH)D with vitamin D and placebo from baseline was 42 ± 34 nmol/L and −11 ± 30 nmol/L, respectively (p < 0.001). In the vitamin D group, all participants reached a 25(OH)D level above 50 nmol/L at nine months. There were no serious side effects, and the intervention was well tolerated.
Discussion
This is the first randomized trial to test the effect of supplemental vitamin D on remission from GD. We clearly showed that vitamin D does not improve the course of the disease. This result was consistent in all analyses and independent on baseline vitamin D status. Contrary to expectations, patients supplemented with vitamin D showed higher proportions of failure to enter and sustain remission and higher proportions of relapse of borderline statistical significance. Among nonsmokers, this unexpected negative effect was statistically significant.
The strengths of this study include the successful inclusion, the high adherence to intervention, the low number of lost-to-follow-up, the use of site randomization, the pragmatic study design, and the placebo-controlled intervention.
Our results apply to a Caucasian population of mainly vitamin D-replete patients treated with the chosen dose and formulation of vitamin D. Whether supplementation is of benefit for the course of GD in cases with severe vitamin D deficiency is not clarified based on our data.
The composite endpoint of failure to enter and sustain remission included prescription of ATD beyond 24 months. This criterion was chosen in accordance with a recommended treatment duration of 12–18 months at the time of study initiation. 20 According to the latest guidelines on management of Graves' hyperthyroidism, published in 2018 after study initiation, it is suggested to continue ATD beyond 18 months if TRAb level is elevated. 21 The decision to continue ATD was opted by the treating physician. A review of medical charts revealed that continued ATD prescription was justified by unresolved disease burden in the vast majority of these patients and with no differences between randomization groups. Secondary outcome analysis on risk of relapse was in agreement with the main finding, thus assuring the conclusion that vitamin D supplementation did not improve the course of disease.
Previous intervention studies, except one, 22 pointed toward beneficial effect of vitamin D on restoration of euthyroidism. Thus, in a three-month, open-labeled intervention study in vitamin D-insufficient GD patients (N = 60), monthly high-dose vitamin D3 injection lead to reduction in fT4 levels, in thyroid volume, and in the degree of orbitopathy. 13 In a 24-week, open-labeled randomized trial (N = 30), treatment with active vitamin D lead to faster restoration of euthyroidism despite comparable ATD dosage. 12 Similar results were obtained in a small single-blinded study (N = 42) of combined vitamin D and selenium supplementation, unfortunately with incomplete recruitment. 14
In our data, which was a larger sample size, vitamin D did not affect the change in thyroid hormones at 3 or 9 months. The combined intervention with selenium in one study might contribute to the different findings. Results of the Selenium supplementation for patients with Graves' hyperthyroidism study, examining the implication of selenium for treatment failure in GD, are awaited. 23 Previous studies found no effect of vitamin D on the level of TRAb, and this was confirmed in our data. This unanimous finding supports the primary outcome of our study.
The interaction of smoking and vitamin D is of interest as smoking is associated with a worse course of GD. 24 The possible mechanism is not clear. In a recent large intervention study, tobacco smoking did not modify the 25(OH)D increase following supplementation. 25 A large cross-sectional study, supported by experimental data, points toward a different metabolic effect of a given 25(OH)D level in smokers with a lower parathyroid hormone level and downregulation of CYP27B1 expression, presumably reducing production of the active vitamin D metabolite. 26,27 Whether smoking affects the response to vitamin D or whether our observation is a chance finding needs further scrutiny.
The recent study by Hahn et al. 11 demonstrated reduction of incident autoimmune disease with vitamin D supplementation, contrary to the lack of effect in this study of established GD. Thus, the immune-regulatory effect of vitamin D in autoimmune disease might depend on the state of disease development, and however, a hypothetical similar underlying pathogenic mechanism, the effect of environmental exposure such as vitamin D might differ between the heterogeneous autoimmune conditions. In the quest of harvesting clinical benefit from the immune-modulating effects of vitamin D, several aspects are unclarified, including the proper timing of treatment and the adequate supplemental dose or formulation and the 25(OH)D level required to achieve the effect.
Our data clearly show that supplementation with high-dose vitamin D does not improve the course of disease in a newly diagnosed Caucasian cohort of patients with GD.
Footnotes
Authors' Contributions
D.G.-L.: Conceptualization (supporting), writing—original draft (lead), formal analysis (lead), writing—review and editing (equal), methodology (supporting). E.E.: Conceptualization (supporting), writing—review and editing (equal), methodology (supporting), formal analysis (supporting). T.W.: Conceptualization (supporting), writing—review and editing (equal), methodology (supporting), formal analysis (supporting). A.L.R.: Methodology (supporting), writing—review and editing (equal). T.Ø.: Methodology (supporting), writing—review and editing (equal). B.J.B.: Methodology (supporting), writing—review and editing (equal). J.J.C.: Methodology (supporting), writing—review and editing (equal). K.W.H.: Conceptualization (supporting), writing—review and editing (equal), methodology (supporting), formal analysis (supporting). L.R.: Conceptualization (lead), writing—original draft (supporting), formal analysis (supporting), writing—review and editing (equal), methodology (lead).
Author Disclosure Statement
No competing financial interests exist.
Funding Information
Trial medication was provided without charge from Orkla ASA. No funding was received for this article.
Supplementary Material
Supplementary Table S1