
Abstract
Background:
Evidence is needed on the risks and benefits of combination therapy with levothyroxine (LT4)+liothyronine (LT3) for the treatment of hypothyroidism.
Objective and Methods:
We performed a randomized, double-blind placebo-controlled study to assess the effects of LT4+LT3 therapy versus LT4+placebo in a homogeneous group of athyreotic patients, without cardiovascular risk factors during long-term replacement monotherapy with LT4. The primary objective of the study was to assess the effects of combination LT4+LT3 therapy on heart rate, cardiac rhythm, and sensitive cardiovascular parameters of cardiac morphology and function by means of electrocardiography and Doppler echocardiography. The secondary objective of the study was to evaluate patient compliance, tolerability, and potential adverse events.
Results:
Thirty-eight patients with postsurgical hypothyroidism satisfying the inclusion criteria were selected from a group of 300 patients with low-risk thyroid cancer followed for a routine follow-up; they were randomized to receive LT4+LT3 or LT4+placebo. Twenty-four patients were evaluated after 1 year of treatment. All clinical and laboratory parameters were compared with the results obtained from 50 healthy euthyroid volunteers without comorbidities, matched for gender, age, physical activity, and lifestyle. Participants and clinicians remained blinded to the treatment allocation. After 1 year of combination therapy, a significant improvement in the diastolic function, evidenced by a significant reduction in the E/e′ ratio (p = 0.046) and its positive trend over time, was observed in the LT4+LT3 group versus the LT4+placebo group. In addition, the univariate analyses showed a significant relationship between free triiodothyronine (fT3) levels (in pg/mL) with Δ of variation of the E/e′ ratio in the LT4+LT3 group (standardized β coefficient = 0.603 [confidence interval: 0.001–1.248], p = 0.050) after combination therapy. No adverse events including tachycardia, arrhythmias, atrial fibrillation, or other important events occurred between the first administration and the end of the study.
Conclusions:
In this preliminary report, combination treatment with LT4+LT3 induced favorable changes in cardiovascular parameters of diastolic function without any adverse cardiovascular events. Trial Registration: EUDRACT number: 2017-001261-25.
Introduction
Levothyroxine (LT4
Numerous studies and meta-analyses have failed to demonstrate the superiority of combination therapy with LT4+liothyronine (LT3) versus LT4 monotherapy. 14 –19 This is largely due to some methodological limitations regarding the heterogeneity in the trial's populations in terms of etiology and severity of hypothyroidism, the short period of follow-up, and the evaluation of parameters not sufficiently sensitive (such as quality of life or patient preference) for an objective evaluation of the effects of combination treatment. 16 –19 Despite these inconclusive results, expert opinions, guidelines, and a consensus document have recognized the necessity to consider combination therapy in unsatisfied hypothyroid patients without comorbidities to avoid self-prescription of inadequate doses of thyroid hormones. 15,17 –19 They have limited the indication of LT4+LT3 to an experimental approach for the lack of evidence-based data on the benefit–risk of combination therapy. 17,18
It is for this reason that we have performed a randomized, double-blind placebo-controlled study on combination LT4+LT3 versus LT4+placebo therapy to assess sensitive cardiovascular and metabolic parameters of thyroid hormone action in a homogeneous group of athyreotic patients receiving
Study Design
A randomized, double-blind placebo-controlled study was performed to evaluate the effects of LT4+LT3 versus LT4+placebo on metabolic and cardiovascular parameters in patients with postsurgical hypothyroidism. The primary objective of the study was to assess cardiovascular effects (heart's rate and rhythm and cardiovascular structure and function) in patients receiving combination LT4+LT3 therapy versus LT4+placebo. Metabolic parameters such as lipid profile, fasting glycemia and insulinemia, and changes in body mass index (BMI) were also evaluated. The secondary objective of the study was to assess the patient's compliance and tolerability and adverse events.
Although the aim of this study was not to assess the quality of life, the hyperthyroid symptom scale, a questionnaire including 10 categories of symptoms of hyperthyroidism, was included to select patients requiring prompt cardiological evaluation during the study. 20 The duration of the study was 24 months, of which 12 months for the enrollment and 12 months for the treatment with LT4+LT3 versus LT4+placebo. A control group of 50 euthyroid subjects, not suffering from any thyroid disease, with comparable sex, age, BMI, and lifestyle, was included to compare the echocardiographic results of the randomized hypothyroid patients at baseline and after 12 months of treatment.
The study protocol, which included both patients and controls, was approved by the ethics committee of the University of Naples Federico II and by the Italian Medicines Agency (AIFA). The study was registered at the European Union Clinical Trials Registration (EUDRACT No. 2017-001261-25). All patients provided informed consent to the study.
Patients and Methods
Study population
Three hundred patients were assessed for eligibility from a group of postsurgical hypothyroid patients, who underwent total thyroidectomy and radioiodine ablation (29 patients, representing 76%) for differentiated thyroid cancer (DTC); these low-risk patients were receiving long-term LT4 therapy (11.97 ± 7.13 years) with a thyrotropin (TSH) target based on the available recommendations 21,22 (Fig. 1). The enrollment was conducted in the Outpatient Clinic of Thyroid Pathology and Internal Medicine of the University of Naples Federico II. Inclusion and exclusion criteria for patients and controls are reported in Table 1. We did not select a specific group of symptomatic patients receiving LT4 monotherapy at the time of enrollment. Fifty healthy euthyroid volunteers without comorbidities, matched for gender, age, physical activity, and lifestyle, were also recruited as a control group. This control group was decided at inception.
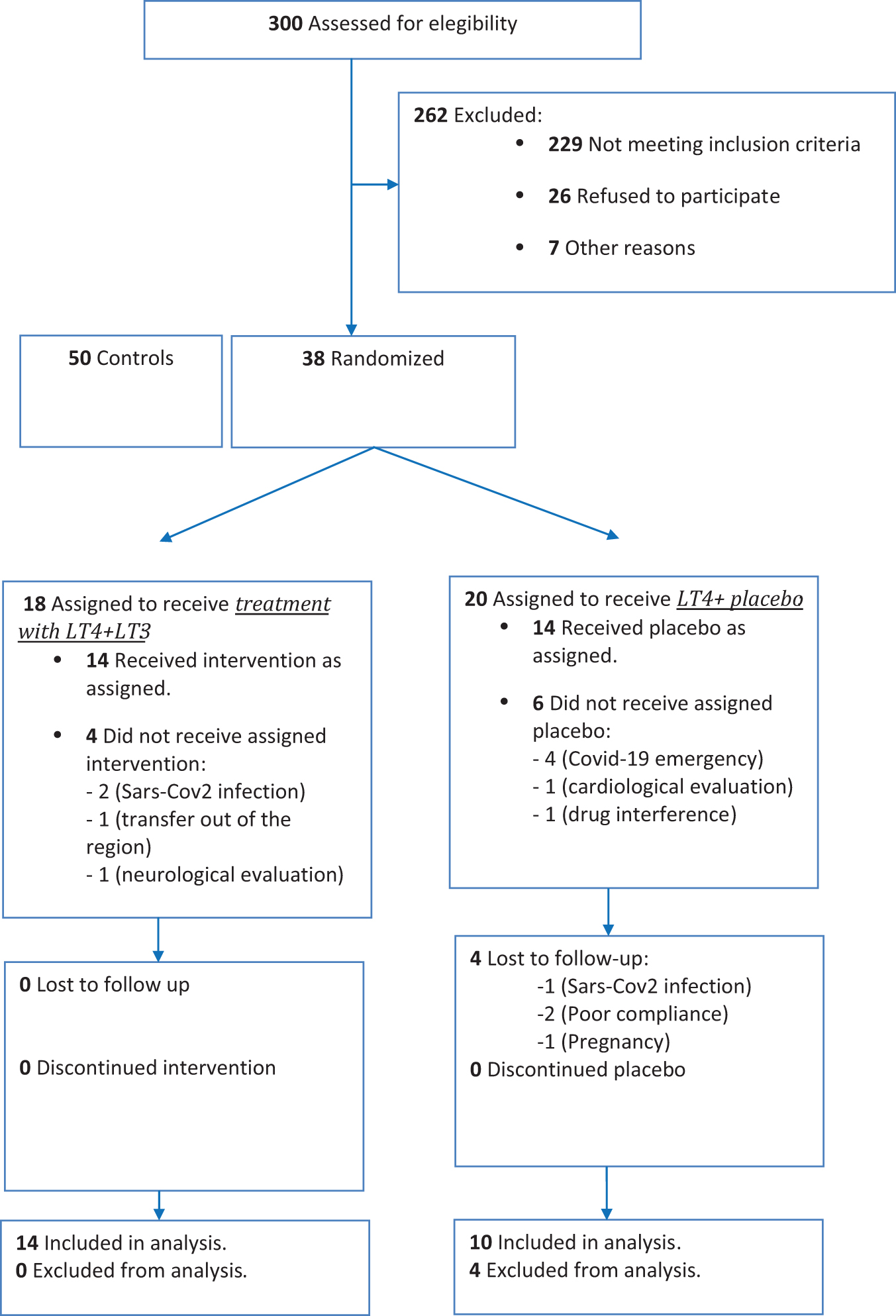
Flowchart describing recruitment of the patients in the study. Three hundred patients were assessed for eligibility from a group of patients with differentiated thyroid cancer followed in our ambulatory for a routine follow-up. Of the 300 patients, 229 did not meet the inclusion criteria, 26 refused to participate to the study, and 7 were excluded for other reasons. Fifty healthy euthyroid volunteers without comorbidities, matched for gender, age, physical activity and lifestyle, were also recruited as a control group. A total of 88 subjects matching our strict selection criteria were randomized. Thirty-eight patients with postsurgical hypothyroidism were randomized to receive LT4+LT3 or LT4+placebo. Eighteen patients were assigned to receive LT4+LT3 treatment; however, among these patients, four did not receive the assigned therapy (two developed SARS-COVID infection, one moved out of the Campania region, and one was excluded after neurological evaluation). Twenty patients were assigned to receive placebo, of which six did not receive the assigned intervention (four for hospitalization for SARS-COVID infection, one after the cardiological evaluation, and one because she started a drug potentially interfering with absorption). Twenty-four patients were finally included in this study and evaluated after 1 year of treatment (14 patients received LT4+LT3 and 10 were randomized to LT4+placebo). Four subjects assigned to receive placebo dropped out from the clinical trial (one for SARS-COVID infection, two due to poor compliance to the protocol, and one for pregnancy intent). LT3, liothyronine; LT4, levothyroxine.
Inclusion and Exclusion Criteria for Patients and Controls at Enrollment
Haugen et al. 22
ATA, American Thyroid Association; BMI, body mass index; LT4, levothyroxine; TSH, thyrotropin.
Methods
At baseline, the following evaluations were performed: (1) anamnestic evaluation; (2) blood pressure and heart rate; (3) anthropometric data (height, weight, BMI, waist and hip circumferences); (4) thyroid function test: TSH, free triiodothyronine (fT3), free thyroxine (fT4), thyroglobulin (Tg), antithyroglobulin (TgAb), antithyroid peroxidase antibodies (TPOAb), and neck ultrasound; (5) parathyroid (PTH), calcium, albumin, and phosphorus; (6) lipid profile (total cholesterol, low-density lipoprotein cholesterol, high-density lipoprotein cholesterol, triglycerides); (7) fasting glycemia and insulinemia; (8) electrocardiography; (9) color Doppler echocardiography; (10) questionnaires to assess symptoms and signs of hyperthyroidism (symptom rating scale). 20
The evaluation of the thyroid function biochemical and metabolic parameters and symptoms of hyperthyroidism was performed at baseline and after 3, 6, and 12 months of combination therapy (Supplementary Table S1). Electrocardiogram (ECG) and color Doppler echocardiography and variations of weight, waist circumference, and hip circumference were assessed at baseline and after 6 and 12 months. All clinical, laboratory, and cardiovascular parameters were compared with the results obtained from 50 healthy euthyroid volunteers.
Blood samples for circulating serum TSH, fT3, fT4, Tg, TgAb, and TPOAb were collected from the antecubital vein after an overnight fast. They were determined by chemiluminescence-based assays (ADVIA Centaur Systems; Siemens Healthineers). ECG and Doppler echocardiography were performed by two cardiologists blinded to the patients' treatment. Eco-Doppler parameters were assessed in agreement with the current recommendations and guidelines. 23 –27
Randomization and treatment
All consecutive patients satisfying the inclusion criteria were randomized to receive a combination therapy with LT4+LT3 or LT4+placebo (Fig. 2). The randomization list was organized by a Randomization Manager (Data Management and Statistics Department of IBSA Institut Biochimique SA) using an SAS Validated software. Copies of the randomization list and the LT3/placebo stocks were sent from the Randomization Manager to the pharmacist in charge of the drugs, who was responsible for the drugs' distribution. LT4 therapy was administered orally in the same formulation already taken by the patient; the daily dose was administered in the morning (1 hour before breakfast).

Flowchart describing randomization and analysis of the patients in the study. Step 1: During the first visit, the starting dose of LT4 was reduced and the LT3 or placebo was added with an initial ratio of 17: 1. Thyroid function tests were repeated 3 and 6 months after the enrollment to assess the euthyroid state. Step 2: After 3 months, the starting dose was modified according to the evaluation of thyroid hormone levels and TSH. The expectation of this adjustment was to obtain fT4 levels in the middle reference range with a serum TSH according to the ATA guidelines.
21
Patients with a serum TSH levels <0.40 or >3 mIU/L and/or fT4 or fT3 higher or lower of their normal reference range were considered, respectively, over- and undertreated. As a consequence, the LT4 dose was adjusted (with changes of about 12.5–25 μg/day during the follow-up at 3 and 6 months) according to serum TSH and fT4 concentration. Similarly, the LT3 and/or placebo doses were adjusted (about 4–6 drops) according to fT3 concentrations to obtain an fT3 level in the middle reference range. Patients taking placebo completed an identical protocol with a similar titration.
IBSA Pharmaceutics provided both the LT3 and placebo; they were produced, packaged, and labeled according to Good Manufacturing Practices. 28 LT3 bottles, placebo bottles, and related droppers were identical to maintain the blinded study design. Liotir (LT3 sodium) was provided in the form of oral drops (1 drop contained 0.71 μg of LT3 sodium). This drug received the marketing authorization in Italy by the AIFA in 2015 (GU Serie Generale No. 123-29/05/2015). The daily LT3/placebo dosage was divided into two doses, one in the morning and the other 12 hours later.
All enrolled patients and investigators involved in the study remained blind to the assigned treatment for all the duration of the study. Only the principal investigator was aware of the TSH and thyroid hormone levels during the follow-up in both the blinded groups to adjust the starting dose during the follow-up as reported in Figure 2.
Evaluation of compliance and tolerability
The evaluation of patient compliance during combination therapy with LT4+LT3 was assessed at each control during the follow-up. All the bottles, once opened, had a 1 month deadline, and the patients reported the bottles' opening date on the labels; they sent back the unused drugs to the investigator.
Pharmacovigilance and adverse effects
Patients were monitored for problems related to tolerability and adverse events during the follow-up. Two series of sealed envelopes containing the correspondence between the randomization code and the treatment group were generated, one for the IBSA Drug Safety Officer, to be opened in case of unexpected, suspected, serious adverse effects, and the other one for the investigator. Only in case of emergency was the investigator authorized to open the emergency envelope, after providing a legitimate reason for the opening.
The investigator was invited to record any adverse events, regardless of the severity and its relationship to treatment, occurred in patients enrolled from the signing of informed consensus and up to 2 weeks of taking the last dose of the drug (approximately five times its half-life) in the Development Safety Update Report (DSUR) for each of the subjects. The case report form (CRF) of each subject was communicated to the Pharmacovigilance (the Clinical Research Technology), a Contract Research Organization involved in the communication of adverse effects to the IBSA Pharmaceutics, the Ethics Committee, and Eudravigilance. All patients received the names and telephone contacts of the principal investigator (B.B.). Patients were protected by insurance for all the duration of the study.
Statistical analysis
IBM SPSS Statistics for Windows v20 (IBM Corp.) was used for statistical analysis. Continuous variables are presented as mean value ± standard deviation. Categorical variables are presented as absolute numbers and percentages. Descriptive statistics were obtained by one factor analysis of variance (Bonferroni post hoc intergroup analysis) and χ 2 distribution with computation of exact p-value by the Monte Carlo method and intergroup post hoc (Bonferroni test) comparison. Linear regression analyses and the partial correlation test using Pearson's correlation method were used to test univariate relations of a given cardiovascular variable. The null hypothesis was rejected at two-tailed p < 0.05.
Results
From the beginning of the study to the Data Lock Point, no patient died. No serious adverse events (SAE) such as arrhythmias, angina, heart failure (HF), stroke, or other serious events occurred, and no identified potential risks were detected in patients receiving LT4+LT3 and LT4+placebo. No patient experienced a rise in Tg or TgAb or structural recurrence of thyroid cancer over the course of the study. All patients had good compliance and tolerability during treatment.
Table 2 shows the anthropometric, clinical, and echocardiographic variables of the overall study population. Thirty-eight athyreotic patients with low-risk thyroid cancer during LT4 monotherapy were compared with 50 euthyroid controls at the baseline evaluation. Anthropometric variables did not show any significant differences. At the time of enrollment, all patients and controls had been biochemically euthyroid for at least 6 months. The mean LT4 dose in the whole group of patients was 1.97 μg/kg/day (range 1.68–2.16 μg/kg/day) to obtain a serum TSH between 0.3 and 2 mIU/L in all patients, according to the recommendations in disease-free athyreotic patients with low-risk DTC. 21,22 The echocardiographic evaluation showed that ventricular ejection fraction was significantly lower and left ventricular (LV) mass index was significantly higher in the athyreotic group of patients during LT4 monotherapy compared with the euthyroid controls. Regarding Doppler LV diastolic parameters, E′ lateral was significantly lower and pulmonary artery systolic pressure and E/e′ ratio were significantly higher in the whole group of athyreotic patients assuming LT4 monotherapy versus controls.
Anthropometric, Clinical, and Echocardiographic Variables in the Hypothyroid Group Compared with the Euthyroid Controls
Early diastolic velocities (e′) of lateral mitral annulus; E/e′ ratio, ratio between the preload-depending transmitral E velocity and the average of septal and lateral velocities of the earliest diastolic motion (e′) of the mitral annulus.
DBP, diastolic blood pressure; LDL, low-density lipoprotein; LV, left ventricular; LVEF, left ventricular ejection fraction; PAPs, pulmonary artery systolic pressure; SBP, systolic blood pressure; TAPSE, tricuspid annular plane systolic excursion.
Supplementary Table S2 shows the basal anthropometric, clinical, laboratory, and echocardiographic data of the 28 patients enrolled in the study, of which 14 patients were included in the LT4+LT3 group and 14 patients in the LT4+placebo group. The results did not significantly differ between the two groups.
Table 3 shows the anthropometric and clinical results at 12 months in the LT4+LT3 group (14 patients) compared with the LT4+placebo group (10 patients). Weight, BMI, waist circumference, and hip circumference did not significantly differ at 12 months in the LT4+LT3 group (14 patients) compared with the LT4+placebo group (10 patients). fT3 was significantly higher in the LT4+LT3 group compared with that in the LT4+placebo group. The hyperthyroid symptom scale was not significantly different.
Anthropometric and Clinical Data in the Levothyroxine+Placebo Group and the Levothyroxine+Liothyronine Group at Baseline and After 12 Months
T0: baseline evaluation; T12: after 12 months.
p: The LT4+LT3 group at 12 months compared with the LT4+placebo group at 12 months.
p: The LT4+placebo group at 12 months compared with baseline.
p: The LT4+LT3 group at 12 months compared with baseline.
fT3, free triiodothyronine; fT4, free thyroxine; HC, hip circumference; LT3, liothyronine; WC, waist circumference.
We observed a statistically significant reduction in body weight, BMI, waist circumference, and hip circumference after 12 months in the 14 patients who received LT4+LT3 treatment versus their baseline evaluation. In addition, in this last group, there was a reduction, although not significant, in total cholesterol and hyperthyroid symptom scale scores after 12 months of LT4+LT3 combination therapy compared with the baseline evaluation.
Regarding the clinical results of the LT4+placebo group, the mean serum TSH was significantly increased after 12 months versus the baseline evaluation. In addition, there was a significant increase in the BMI and a slight increase in other anthropometric parameters (weight, waist circumference, and hip circumference), which was not statistically significant. No other statistically significant differences were observed in other variables at the 12-month evaluation in the LT4+placebo group. The LT4 total weekly dose was significantly increased after 12 months of LT4+placebo (829.86 ± 189.14) compared with the baseline LT4 dose (736.86 ± 187.18) (p = 0.042).
Table 4 shows the echocardiographic variables at 12 months in the LT3+LT4 group compared with the LT4+placebo group and the euthyroid controls.
Echocardiographic Variables at 12 Months in the Levothyroxine+Liothyronine Group Compared with the Levothyroxine+Placebo Group and the Euthyroid Controls
Early diastolic velocities (e′) of lateral mitral annulus; E/e′ ratio, ratio between the preload-depending transmitral E velocity and the average of septal and lateral velocities of the earliest diastolic motion (e′) of the mitral annulus.
p: The LT4+LT3 group at 12 months compared with the LT4+placebo group at 12 months.
p: The LT4+LT3 group at 12 months compared with the euthyroid controls.
p: The LT4+placebo group at 12 months compared with the euthyroid controls.
At the echocardiographic evaluation, with regard to Doppler-derived LV diastolic parameters, there was a significant reduction in the E/e′ ratio in the LT4+LT3 group versus the LT4+placebo group. The univariate linear regression analysis showed a significant relationship between fT3 levels (pg/mL) with Δ of variation of the E/e′ ratio in the LT4+LT3 group (standardized β coefficient = 0.603 [confidence interval: 0.001–1.248], p = 0.050) after combination therapy.
No significant difference was observed in the LT4+LT3 group at 12 months compared with the euthyroid controls. A significant reduction in the left ventricular ejection fraction (LVEF) and a significant increase in the left ventricular mass (LVM) index and E/e′ ratio were instead observed in the LT4+placebo group at 12 months compared with the euthyroid controls.
Table 5 shows the echocardiographic parameters of the LT4+LT3 group at 12 months compared with the baseline evaluation and the group of euthyroid controls. At the echocardiographic evaluation, the LVEF was significantly higher, while the left ventricular mass index and pulmonary artery systolic pressure were significantly lower after 12 months of LT4+LT3 combination treatment compared with the baseline evaluation. Regarding Doppler-derived LV diastolic parameters, there was a significant reduction in the E/e′ ratio. No statistically significant differences were evident compared with the euthyroid controls.
Echocardiographic Variables in the Levothyroxine+Liothyronine Group at Baseline, After 12 Months, and Versus the Euthyroid Controls
T0: baseline evaluation; T12: after 12 months. Early diastolic velocities (e′) of lateral mitral annulus; E/e′ ratio: ratio between the preload-depending transmitral E velocity and the average of septal and lateral velocities of the earliest diastolic motion (e′) of the mitral annulus.
p: The LT4+LT3 group at 12 months compared with the baseline evaluation.
p: The LT4+LT3 group at 12 months compared with the euthyroid controls.
Table 6 shows the echocardiographic parameters of the LT4+placebo group at 12 months compared with the baseline evaluation and the group of euthyroid controls. Echocardiographic evaluation at 12 months did not show any statistically significant differences versus the baseline evaluation. However, the LT4+placebo group showed a significantly lower LVEF and higher left ventricular mass and E/e′ ratio compared with the euthyroid controls.
Echocardiographic Variables in the Levothyroxine+Placebo Group at Baseline, After 12 Months, and Versus the Euthyroid Controls
T0: baseline evaluation; T12: after 12 months. Early diastolic velocities (e′) of lateral mitral annulus; E/e′ ratio, ratio between the preload-depending transmitral E velocity and the average of septal and lateral velocities of the earliest diastolic motion (e′) of the mitral annulus.
p: The LT4+placebo group at 12 months compared with baseline.
p: The LT4+placebo group at 12 months compared with the euthyroid controls.
Figure 3 shows the trend of the E/e′ ratio in the LT4+placebo group (Fig. 3a) and in the LT4+LT3 group (Fig. 3b).
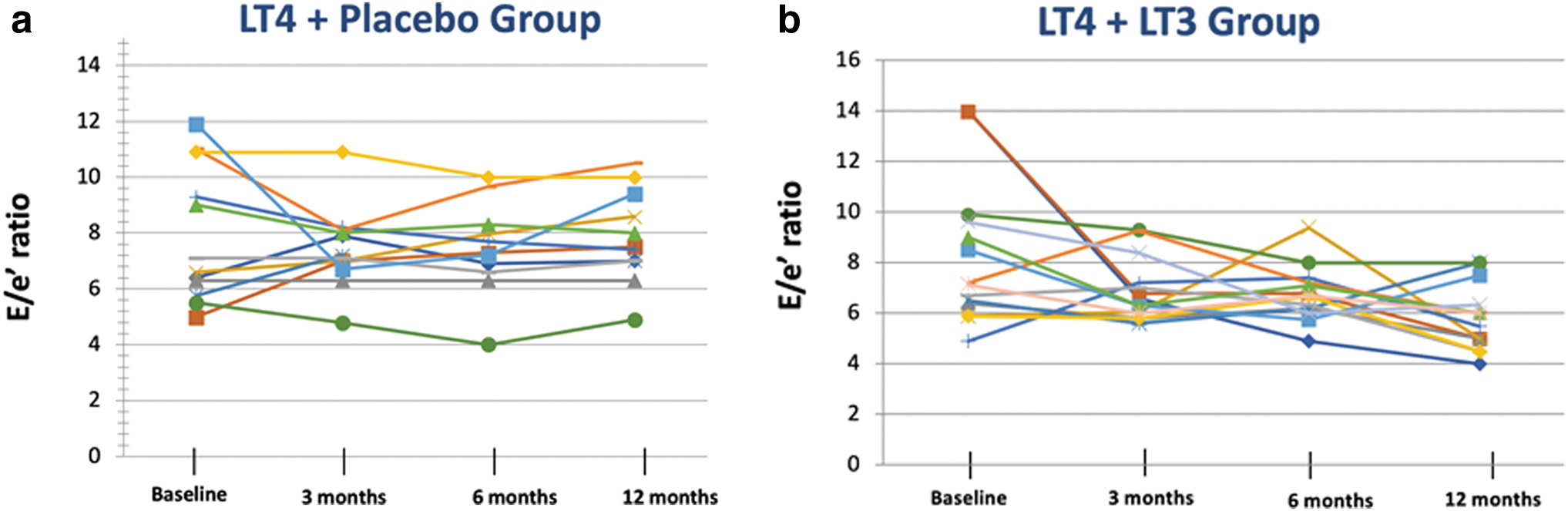
Data over time and trend of the E/e′ ratio in the LT4+placebo group
Discussion
Our study is the first randomized controlled trial (RCT) designed to analyze the long-term effects of combination LT4+LT3 therapy on the cardiometabolic parameters in athyreotic patients without cardiovascular risk factors. It follows the criteria of a well-designed trial on combination therapy established in the statement made by the American Thyroid Association, 15,29 although released for an AIFA project in 2017 and started in 2019.
Thyroid hormone plays an essential role in the growth and development of the cardiovascular system and regulates multiple metabolic processes. T3, the active hormone, exerts its physiological effects on the cardiovascular system leading to an increase in heart rate, myocardial contractility, and cardiac output. 30,31 Regarding the metabolic effects, T3 increases energy expenditure and accelerates the rate of cellular oxidation controlling carbohydrate, lipids, and protein metabolism. 32 –34 Alterations in the lipid profile have been reported in thyroidectomized patients during LT4 monotherapy. 32 –34
In our RCT study, at the baseline echo-Doppler evaluation, we detected a significant reduction in the LVEF and an increase in the LVM index with impaired diastolic function and negative effects on pulmonary arterial hypertension when the whole group of athyreotic patients was compared with the group of well-matched euthyroid controls. These results were observed despite the presence of a stable condition of euthyroidism in our patients in the 6 months preceding their enrollment. Serum TSH suppression with LT4 therapy, after total thyroidectomy and radioiodine ablation, has been used for many years in patients with DTC, and around 20% of LT4-treated hypothyroid patients appeared over-replaced during LT4 therapy.
Excessive LT4 therapy to obtain TSH suppression (exogenous subclinical hyperthyroidism) may induce mild tissue hyperthyroidism and adverse cardiovascular effects leading to an increase in heart rate and left ventricular mass and a consequent diastolic dysfunction with a predisposition to the onset of supraventricular arrhythmias, atrial fibrillation, and increased cardiovascular morbidity, particularly in patients with undetectable serum TSH and in the older population. 35 –37 On the contrary, an increase in LVM with a reduction in LVEF and impaired diastolic dysfunction has been documented in patients with mild subclinical hypothyroidism, 38,39 and an increased risk of HF and coronary heart disease mortality has been associated with serum TSH levels >7 mIU/L. 40 We suppose that some periods of subclinical thyroid dysfunction could be responsible for the negative cardiovascular findings observed in our athyreotic patients receiving long-term LT4 replacement monotherapy when compared with the euthyroid controls. 41
However, we cannot exclude that these negative cardiovascular findings could be related to the reduced fT3/fT4 ratio reported in literature studies in athyreotic patients receiving LT4 monotherapy. 42 It is uncertain whether replacement therapy with LT4 alone is able to completely normalize the cardiovascular function in hypothyroid patients without a residual thyroid function because no data are currently available on the long-term effects of this treatment. In addition, the comparison between the results obtained at the baseline evaluation and after 12 months showed that patients receiving LT4+LT3 had a significant improvement in the LVEF, LVM index, diastolic function, and pulmonary artery systolic pressure after combination therapy.
This subgroup of patients also had a significant reduction in body weight, BMI, waist circumference, and hip circumference. These preliminary results confirm previous findings in a small number of patients showing that the short-term substitution of LT3 for LT4 at equivalent doses was able to reduce body weight and improve the lipid metabolism. 32 Future large prospective studies are necessary to clarify the cardiovascular outcome of athyreotic patients treated with long-term replacement doses of LT4 monotherapy and to assess the potential limits of LT4 monotherapy in normalizing the cardiometabolic risk in athyreotic patients.
Regarding the comparison between the LT4+LT3 and LT4+placebo groups, the evaluation of Doppler-derived LV diastolic parameters showed a significant reduction in the E/e′ ratio in the LT4+LT3 group versus the LT4+placebo group after 12 months. Our study included a small number of patients and was underpowered to compare the cardiovascular and metabolic changes between patients receiving LT4+LT3 combination therapy versus LT4+placebo. However, interestingly, we observed a positive trend of the E/e′ ratio over time in hypothyroid patients receiving combination therapy; all patients in this group showed an improvement in the E/e′ ratio over time after combination therapy with LT4+LT3.
On the contrary, the placebo group had an almost constant trend of the E/e′ ratio over time. Moreover, the results of the univariate analyses of fT3 levels (in pg/mL) with Δ of variation of the E/e′ ratio in the LT4+LT3 group further supported that the beneficial effects of LT4+LT3 therapy on diastolic function could be attributed to LT3 therapy. By combining the early filling velocity on transmitral Doppler (E) with the early relaxation velocity on tissue Doppler (E′), the E/e′ ratio is a reliable expression of left ventricular filling pressure in patients with both diastolic and systolic HF and is considered to be an important prognostic predictor of cardiac events. 43 –45 The improvement of the E/e′ ratio in our patients receiving LT4+LT3 combination could be a positive predictor of an improved cardiovascular prognosis during combination therapy in athyreotic patients.
No important cardiovascular risks were associated with combination treatment with LT4+LT3 compared with LT4 monotherapy in our RCT in adult athyreotic patients without cardiovascular disease or comorbidities. None of the patients in either the LT4+LT3 group or the LT4+placebo group developed SAE or complained of symptoms of thyroid hormone excess. The major concern about the potential adverse effects of LT3 is the peaks of serum T3 concentrations after its administration, which may result in acute potential adverse effects on the cardiovascular system, particularly after a single daily regimen. 46 Our patients receiving combination therapy did not show any significant differences in terms of blood pressure and pulse rate compared with LT4 monotherapy; in addition, we did not observe any atrial arrhythmias. This risk was only reported in literature studies in some overtreated patients during combination therapy, 46,47 particularly after a once-daily administration of LT3 monotherapy for the pronounced T3 peak in the circulation. This peak was not observed in our study, in which the LT3 drops were tailored and administered twice daily.
We cannot compare our results with the previous literature data because no previous RCT has assessed the long-term effects of combination therapy versus LT4+placebo on Doppler indexes of cardiovascular function and metabolic parameters. Two large retrospective studies provided no evidence that long-term combination therapy increases the risk of cardiovascular events, atrial fibrillation, cardiovascular disease, or mortality in patients with hypothyroidism. 48,49 Only one study reported an increased risk of stroke and HF in LT3 users compared with LT4-only users after 52 weeks; however, no data on LT3 dose and compliance, and serum thyroid hormone levels were available in this study. 50
The main strength of our study is the inclusion of a homogeneous group of postsurgical hypothyroid patients without residual thyroid function; these patients represent the best candidates for combination therapy for the reduced T3 levels. 6,42 In addition, as previously mentioned, strict selection criteria were applied for the enrollment of both patients and controls. Furthermore, the long-term follow-up of 1 year allowed us to detect not only acute negative electrophysiological effects of LT3 but also chronic changes in cardiac morphology and function never described in previous literature studies. We used validated measures of cardiovascular morphology and function, which have been already documented to be sensitive to small changes in thyroid function, even in patients with subclinical thyroid disease. In addition, we used a personalized scheme of combination treatment with LT4+LT3 (never published before) to maintain physiological fT4 and fT3 levels, which did not induce any alteration in the serum TSH during the whole study period. This personalized treatment with LT4 and LT3 represents an improvement over what has been performed in past trials.
Our study has, however, a limit, which is the small number of patients enrolled to assess the cardiometabolic effects. This limit can be explained by the strict selection criteria that we used for the study protocol and the poor availability of patients. Unfortunately, the study was performed during the COVID-19 pandemic, which is why we experienced problems with patient enrollment. These limits reflect the real-life complexity of the literature research on the effects of combination treatment in hypothyroid patients, which is demonstrated by the lack of large RCTs on sensitive parameters to this day.
Conclusions
In this preliminary, randomized, double-blind controlled trial that included data from a small number of athyreotic patients, combination treatment with LT4+LT3 induced favorable changes in cardiovascular parameters with no signs of important identified or potential risks. Our results advocate for further RCTs focusing on the cardiovascular (CV) effects of combination therapy before the availability of sustained-release LT3 formulations with potential long-term effects on the heart. We hope that our preliminary data demonstrating the lack of acute and chronic adverse events of combination therapy with LT4 and LT3, when cautiously administered in hypothyroid patients, can encourage future trials on this topic.
Some practical information from our experience may inform the design of future RCTs on this topic: (1) a larger number of hypothyroid patients should be included; a sample size of about 50 patients per group with a total of 100 patients would be significant for a comparison because the possibility of patients dropping-out during the follow-up should be considered; (2) less strict selection criteria could facilitate the enrollment of patients; (3) patients with cardiac arrhythmias should be excluded to avoid adverse CV events; (4) a personalized use of combination treatment could help to obtain maintain normal TSH and thyroid hormones levels; and (5) the E/e′ ratio could be an interesting marker of diastolic function to be assessed in future more extensive trials.
Footnotes
Acknowledgments
This study is in memoriam of Prof. Maurizio Galderisi for his scientific contribution to this project. He was a pioneer in many new ultrasonic cardiological techniques and was the Vice President of the European Association of Cardiovascular Imaging. He worked on the American and European guidelines to promote a program of cardiological surveillance of hematologic-oncologic patients. Maurizio was a great scientist and colleague; he dedicated his life to our scientific community and had a great sense of ethics. His laugh, smile and generosity will always be with us. He died of COVID in March 2020.
Authors' Contributions
B.B. designed the study, performed data collection, statistical analysis, writing and revision of the article. M.P. performed the cardiovascular assessment and contributed to data collection and statistical analysis. G.P. contributed to data collection and extracted data from the electronic medical record system. P.F. performed the laboratory evaluation of thyroid and metabolic parameters. R.E. performed the cardiovascular assessment and contributed to the statistical analysis and writing of the article. All the authors saw the patients at the outpatient clinic of the University of Naples Federico II and verified the extracted data for the study.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This work was supported in part by the AIFA and IBSA Institut Biochimique SA. The IBSA did not contribute in any way to the design of the study, data collection, analysis, and interpretation of the data, nor to the preparation, review, and approval of the article.
Supplementary Material
Supplementary Table S1
Supplementary Table S2