
Abstract
Background:
Anaplastic thyroid carcinoma (ATC) is a rare and frequently fatal type of thyroid cancer. The degree of heterogeneity in survival rates for ATC is incompletely studied. This study evaluated the factors associated with overall survival (OS) of patients with ATC using multicenter real-world data from a national tertiary care center network in France.
Methods:
In this multicenter, retrospective cohort study, all patients with ATC diagnosed between 2010 and 2020 were identified from the national database of the French ENDOCAN-TUTHYREF network. Factors associated with OS were examined in multivariable analyses using Cox proportional hazards models.
Results:
The study included 360 patients. Of these, 220 (61%) were female and the median age was 72 years (interquartile range: 62–80). The percentages of patients with pure and mixed (synchronously-transformed) ATC (p-ATC and st-ATC) were 62.5% and 26.7%, respectively. The median OS was 6.8 months [confidence interval, CI: 5.5–8.1]: not reached for stage IVa, 11.4 months [8.2–17.8] for IVb, and 4.6 months [3.5–5.7] for IVc. Surgery, radiation therapy to the neck, chemotherapy, and best supportive care were administered to 69 (19.2%), 214 (59.4%), 254 (70.6%), and 66 (18.3%) patients, respectively. In a multivariable analysis, including stage IVb–IVc patients, significantly higher OS was observed in patients with Eastern Cooperative Oncology Group performance-status of 0–1 (hazard ratio [HR], 0.6; [CI, 0.4–0.9], p < 0.02), stage IVb [HR, 0.5; CI, 0.4–0.8, p < 0.001], and multimodal treatment (surgery and chemoradiotherapy) [HR, 0.07; CI, 0.04–0.1, p < 0.001]. Variables associated with significantly worse OS included: p-ATC (vs. st-ATC) [HR, 1.83; CI, 1.33–2.51, p = 0.001] and a neutrophil-to-lymphocyte ratio (NLR) >5.05 [HR, 2.05, CI, 1.39–3.05, p < 0.001].
Conclusions:
Factors independently associated with improved OS in ATC included: European Cooperative Oncology Group performance status, disease stage, multimodality treatment, synchronously transformed ATC, and lower NLR. Long-term OS was observed in selected patients with ATC who underwent multimodal treatment.
Introduction
Anaplastic thyroid carcinoma (ATC) is a rare malignancy with an estimated 1-year overall survival (OS) rate of 20–50%. 1 –5 Nation-wide cohorts report lower median OS (2.3–5.7 months) 1 –3,6 –8 compared to that reported by expert centers (9.5–10 and ∼15.7 months, in recent years). 9,10
Various prognostic factors for OS of patients with ATC have been identified in retrospective studies, including: the European Cooperative Oncology Group (ECOG)-performance status (PS), disease stage, pathological subtype (pure-ATC [p-ATC] and mixed-ATC), and neutrophil-to-lymphocyte ratio (NLR). 1,3,4,6,7,9 –19 Furthermore, longer OS rates have been reported in patients undergoing multimodal treatment (surgery and chemoradiotherapy [CRT], targeted therapy, or immunotherapy). 4,10,16,17,20 –25 To date, all of these identified ATC prognostic factors have not been analyzed concurrently using multivariable analyses, incorporating data from patients also treated with modern therapies (targeted therapy or immunotherapy). 4,10,16,17,20 –25 Most ATC prognostic studies have been derived either from national cohorts with large patient sample size, long accrual period, and partial clinical and pathological characterization 1 –3,5 –8,26,27 or single tertiary expert centers with a more comprehensive characterization, but subject to possible selection bias, that may not best reflect real-world data. 10,23,28
We utilized the multicenter database of the French ENDOCAN-TUTHYREF network, including data from 19 expert referral centers in France, as a framework to gather recent real-world data on ATC prognostic factors. We evaluated OS and ATC prognostic factors, including histological subtype, NLR, and treatment modalities, in patients diagnosed with ATC between 2010 and 2020.
Patients and Methods
Data
ENDOCAN-TUTHYREF is a French national network dedicated to the management of refractory thyroid cancers, approved by the French National Cancer Institute (INCa) in 2009. It includes 19 expert centers recognized for their expertise in the management of thyroid cancer.
This retrospective cohort study complied with the French MR004 methodology regarding general data protection regulations for noninterventional retrospective health research (Délibération n° 2018-155 du 3 mai 2018) and was approved by the internal ethics committee and review board (CSET N° 2022-141). 29
Patients and study outcomes
Patients with ATC that were treated at 1 of the 19 participating centers between 2010 and 2020 were enrolled in this study. The pathological diagnosis was confirmed by expert thyroid pathologists from the TUTHYREF-path network. Patients without available clinical or follow-up data were excluded.
For each patient, the following clinical and pathological data were collected at diagnosis: sex, age, PS, symptoms, pathology, stage (eighth edition of the American Joint Committee on Cancer TNM classification system), metastasis site, and molecular analysis. Regarding histology, p-ATC was defined as the presence of ATC cells only; “synchronously-transformed-ATC (st-ATC)” (referred to as “mixed-ATC” in the literature) was defined as the coexistence of ATC cells and a differentiated thyroid cancer (DTC) component in a pathological sample. ATC in patients with a history of DTC treatment was defined as metachronously transformed ATC (mt-ATC).
Treatment modalities included surgery, chemotherapy, radiotherapy, targeted therapy (anti-angiogenic, NTRK, RET, ALK, BRAF, and mTOR inhibitors), and immunotherapy (PD-1 and PD-L1 inhibitors). CRT was defined as a combination of chemotherapy and radiotherapy administered within three months. Multimodal treatment was defined as a combination of surgery and CRT. The NLR was calculated at the time of ATC diagnosis. The molecular profiles were obtained when available and included different techniques depending on the treating sites (immunohistochemistry, Sanger sequencing, and next-generation sequencing [NGS] with various panels).
Statistical analyses
Data were presented as median and interquartile range (IQR) for continuous variables and frequencies and percentages for categorical variables. The association between categorical variables was tested using Pearson's χ 2 or Fisher exact tests, whereas those between continuous and categorical variables were tested using nonparametric Mann–Whitney or Kruskal–Wallis tests. Receiver operating characteristic (ROC) curve analysis was performed to identify NLR biomarker (R-package: “OptimalCutPoints”). OS was defined as the time from the date of ATC diagnosis, either at the primary or metastatic stage mt-ATC, to death from any cause. Patients who did not die were censored at last follow-up. OS was reported using Kaplan–Meier curves that were compared using the log-rank test. Hazard ratios (HRs) and confidence intervals [CIs] were obtained using the Cox proportional hazards model. Statistical analyses were performed using R software (version 4.0.2, 2020), and p-values <0.05 were considered statistically significant.
Results
Overall cohort
Clinical characteristics
This study included 360 patients with a confirmed ATC diagnosis. A total of 47 patients were excluded owing to insufficient data (Fig. 1). There were 220 women (61%). Participant median age was 72 years (IQR: 62–80), and ECOG-PS was 0–1 in 216 patients (60%) (Table 1). Overall, 41.4% of the patients had at least one cervical compressive symptom at diagnosis, with dysphonia, dysphagia, and dyspnea present in 41.4%, 32.8%, and 22.2% of cases, respectively. The median time from the onset of compressive symptoms to pathological diagnosis was 56 days (26–94), and only 28% of the patients were diagnosed within 30 days. Tumor stages at diagnosis were: IVa in 15 (4.2%), IVb in 102 (28.3%), IVc in 231(64.2%), and unknown in 12 (3.3%) patients. Only 54.4% of patients had a molecular profile, which was evaluated using various heterogeneous, noncomprehensive NGS panels (42% between 2010 and 2015 increasing to 82% between 2016 and 2020). The most frequent molecular alterations were TP53 (63.8%), BRAF (27%), and PI3KCA (23.4%) mutations (Supplementary Table S1).
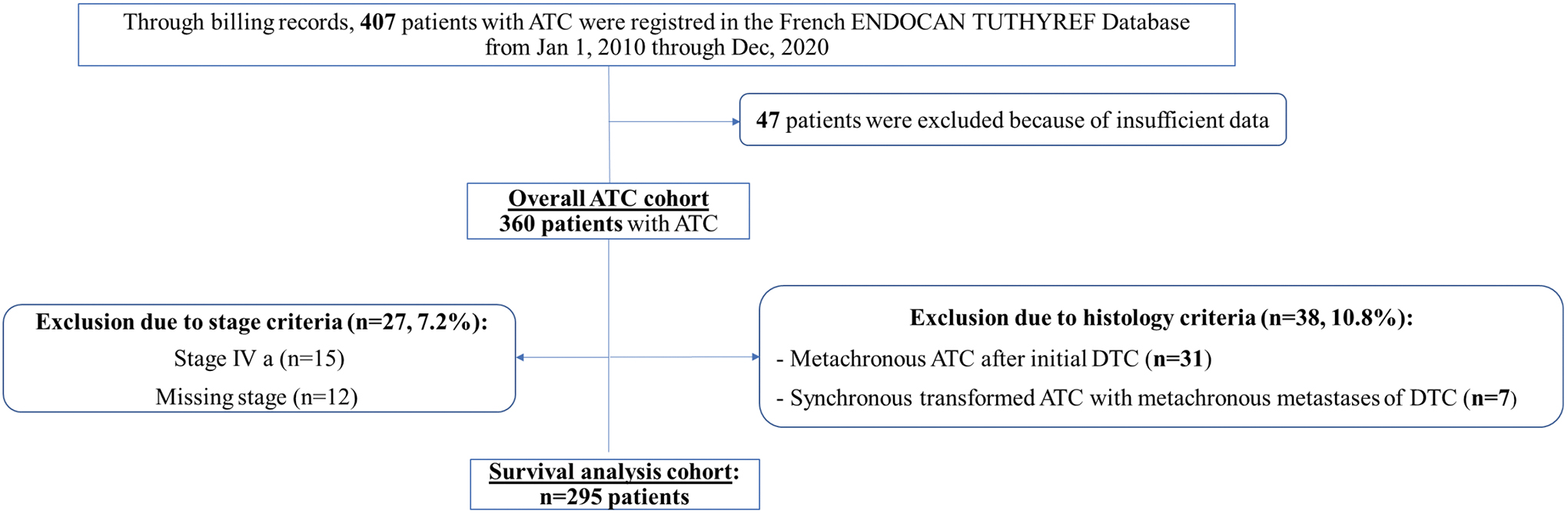
Patient flow diagram of the study. ATC, anaplastic thyroid carcinoma, DTC, differentiated thyroid cancer.
Study Population Characteristics (Clinical, Pathological, Biological, and Treatment Characteristics)
// means not available.
Excluded ATC with metachronous metastatic DTC (n = 14), metachronous ATC after initial DTC (n = 16), and ATC both synchronous and metachronous transformation (n = 9).
Compressive symptoms: dysphonia or/and dysphonia or/and dyspnea.
Only for ATC with Stage IVc.
ATC was considered surgically treated if the type of surgery was thyroidectomy with negative resection (R0) or microscopic resection margins (R1).
Drug therapy included: standard chemotherapy, targeted therapy, and immunotherapy.
ATC, anaplastic thyroid carcinoma; DTC, differentiated thyroid cancer; ECOG, European Cooperative Oncology Group.
Pathology
The most frequent pathological subtype was p-ATC, present in 62.5% of the patients, with st-ATC and mt-ATC present in 26.7% and 4.4% of the patients, respectively (Table 1). DTC-only metastases occurred in 14 patients with st-ATC and were differentiated from the st-ATC group. Stage distribution was different between the pathological subtypes with a higher rate of stage IVc in p-ATC than in st-ATC (150 [69.4%] vs. 55 [55.0%], respectively, p = 0.007).
Biological characteristics
At baseline, the median NLR was 4.4 (2.7–9.1) in 178 patients whose data were available. The NLR was different for each ATC stage: 1.8 (1.6–3.1), 3.1 (2.0–5.7), and 5.1 (3.5–9.8) for stage IVa, IVb, and IVc, respectively (p = 0.001). Median NLR was higher in the mt-ATC subgroup (6.2, 3.0–16.8), followed by the p-ATC (4.8 [3.0–9.7]) and st-ATC (3.7 [1.8–5.7]) subgroups (p = 0.007).
Treatment
Overall, 66 (18.3%) patients received best supportive care (BSC) only. The remaining 294 patients underwent chemotherapy (n = 254, 70.6%), neck radiotherapy (n = 214, 59.4%), thyroidectomy (n = 69, 19.2%), targeted therapy (n = 68, 18.9%), or immunotherapy (n = 18, 5.0%). Thyroidectomy was mostly performed before the administration of systemic treatment and radiotherapy (91%). Targeted therapy and immunotherapy were mainly administered after the first-line treatment (Supplementary Fig. S1 and Supplementary Table S2).
The most common first-line treatment modalities were chemotherapy (71 patients), radiotherapy (31 patients), and CRT (183 patients). The most commonly used first-line chemotherapeutic agents were cisplatin or carboplatin with doxorubicin (65%) or taxanes (30%). Overall, 113 (31.9%) patients received second line treatment, whereas 46 (12.7%) underwent three or more lines of treatment. CRT was administered to 136 (37.8%) patients, and of these, 90 (66.6%) received a RT dose of over 50 Gy. Among patients with molecular alterations, targeted therapy against the molecular alterations was administered in 51 patients (39.5%) (12 started in 2010–2015 and 39 in 2016–2020).
Survival
In the entire cohort, 286 deaths were observed. The following causes of death were identified: disease progression (n = 194), toxicity (n = 5), another disease (n = 5), second cancer (n = 1), and other/unknown causes (n = 82). The median follow-up time and OS were 56.0 months [CI: 29.6–93.3] and 6.8 months [5.5–8.1], respectively (Fig. 2A). OS at 6 months, 1 year, and 2 years was 53.2% (47.9–58.3%), 32.7% (27.8–37.7%), and 20.3% (16.1–24.8%), respectively. The median OS was not achieved (NA), 11.4 months [8.2–17.7], and 4.6 months [3.5–5.7] for stages IVa, IVb, and IVc, respectively (p < 0.001) (Fig. 2B). The median OS was 3.7 (3.0–5.3), 6.0 (1.9–9.1), and 14.7 months (11.4–29.6) in p-ATC, mt-ATC, and st-ATC, respectively (p = 0.001) (Fig. 2C). The OS of the 14 patients with st-ATC with DTC-only metastases was 45 months (14.4–101.9). The median OS of patients treated with BSC only was 0.8 months (0.5–1.3).
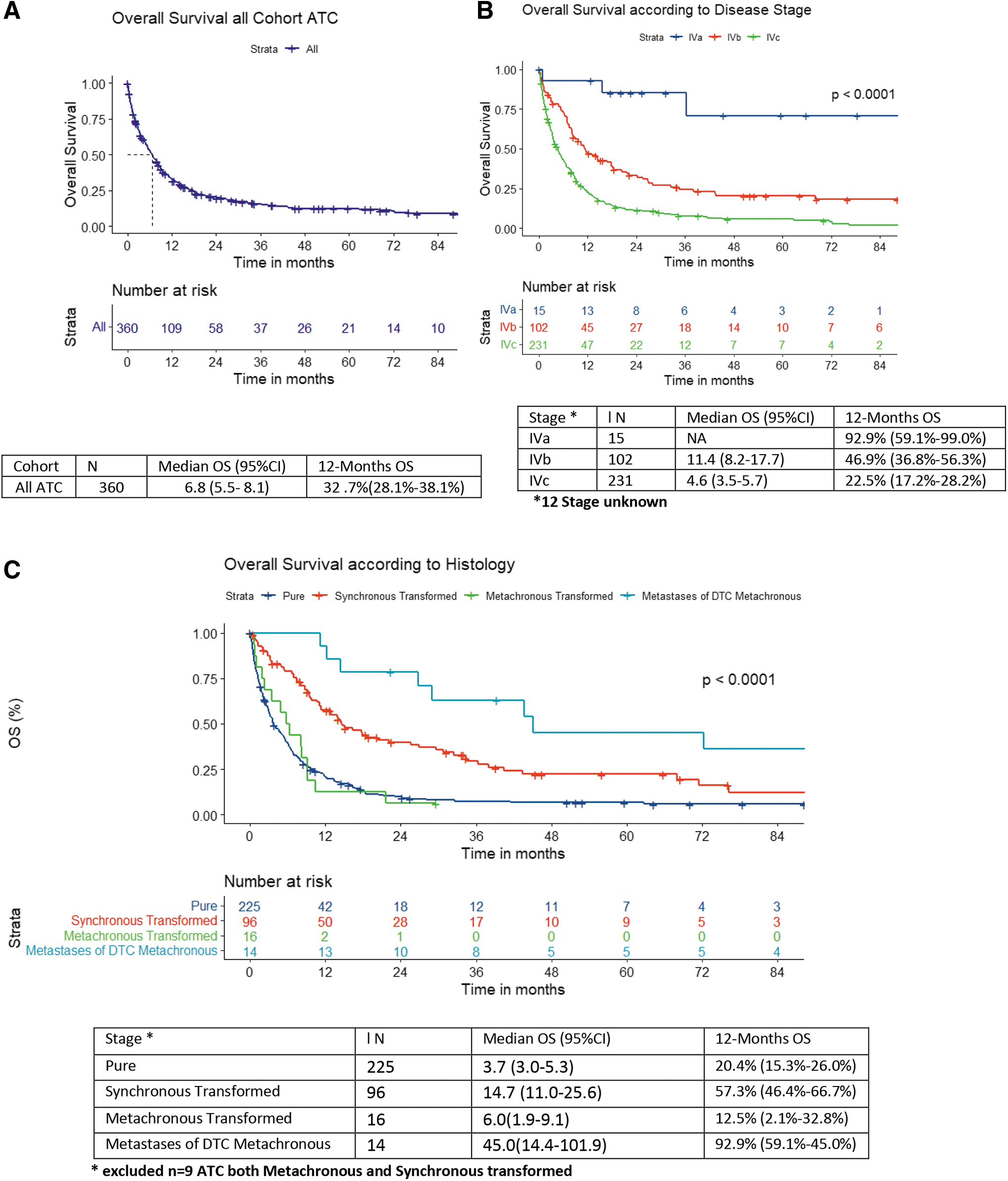
Cohort of n = 360 ATC patients: Overall survival in the entire cohort (
After a median follow-up of 51.9 months (24–77.3), 15 patients (4.2%), with a median age of 59.4 years (48.7–66.5), were disease free. Of these, 5 (33.3%) had stage IVa and 10 (66.7%) had stage IVb disease. Seven (46.7%) patients had p-ATC, and eight (53.3%) had st-ATC. The median NLR at diagnosis was 2.71 (1.94–3.37). All but 1 patient (93.3%) underwent surgery (n = 4, R0-resection), all underwent radiotherapy, and 12 (80%) underwent chemotherapy.
Factors associated with OS of patients with stage IVb or IVc ATC
Of the 295 patients with p-ATC, st-ATC, stage IVb, and IVc, the median OS was 6.0 months (4.6–6.3) (Supplementary Table S2). The AUC of the NLR ROC curve was 0.7 (0.6–0.8), with a cutoff value of 5.05 (Supplementary Fig. S2). A high NLR (>5.05) was associated with shorter survival (median OS, 2.9 months [1.7–4.1] vs. 11.5 months [8.3–14.2]) in the low NLR group (<5.05) (p < 0.001) (Supplementary Fig. S3). Patients treated with CRT (>50 Gy) and multimodal treatment (surgery and CRT) had a median OS of 15.1 months (11.9–20.4) and 25.6 (13.3–42.4), respectively. A total radiotherapy dose of >50 Gy was associated with a significantly better OS (median OS: 14.3 months [10.6–17.8]) compared with that observed with a radiotherapy dose <50 Gy (median OS: 3.6 months [2.8–6.7]) (p < 0.001). The median OS was 6.5 [CI: 5.3–7.7], 14.2 [11.3–18.1], and 20.1 months [11.2–NA] among patients who underwent chemotherapy alone, targeted therapy and/or immunotherapy, respectively, during the disease course (Fig. 3, Supplementary Fig. S4, and Supplementary Table S2).
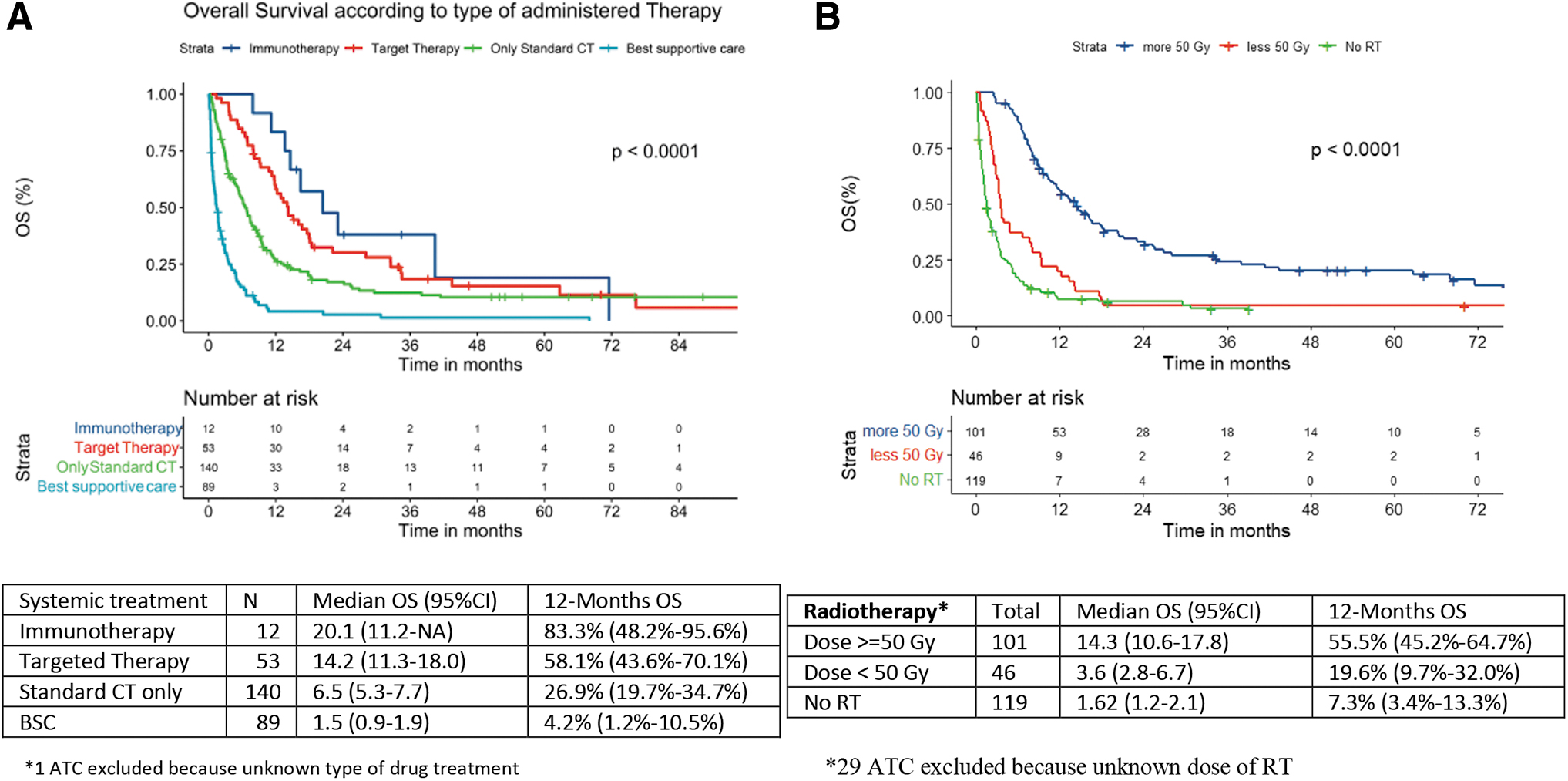
Overall survival in patients with IVb–IVc ATC (n = 295) according to treatment.
Multivariable analysis showed that histology (p-ATC vs. st-ATC), a PS score of 2 versus 0/1 or >3 versus 0/1, disease stage IVc versus stage IVb, and NLR ≥5.05 were associated with a worse OS, whereas multimodal treatment and CRT were associated with improved OS compared to BSC (Table 2).
Univariate and Multivariable Analysis for Overall Survival Outcome
BSC, best supportive care; CI, confidence interval; CRT, chemoradiotherapy; F, female; HR, hazard ratio; M, male; Multimodal treatment, combination of surgery, cytotoxic chemotherapy, and radiotherapy; NLR, neutrophil-to-lymphocyte ratio; Other, Surgery+chemotherapy, surgery+radiotherapy, surgery alone, chemotherapy alone, or radiotherapy alone (regardless of the dose).
Discussion
This multicenter study, including data from 360 patients with ATC, was conducted over a relatively short period (10 years), which was made possible by a large national institutional collaboration among expert centers from the French ENDOCAN-TUTHYREF network. This collaboration provided real-world evidence to capture the heterogeneity of the clinical, pathological, and therapeutic characteristics of ATC, which is usually only available in monocentric series from highly specialized referral centers. 4,10
Consistent with other studies, 3,10,18 stage IVa was associated with a better prognosis in our study. Among patients with stage IVb and IVc, age had no prognostic value; however, the independent prognostic value of ECOG-PS, stage and treatment modalities, namely multimodal treatment, including surgery, radiotherapy, and chemotherapy, and CRT on OS, was observed (Table 2), as reported in previous studies. 1,3,4,6,7,9 –15,26 Overall, patients treated with CRT had a median OS of 9.3 months (7.4–11.7), which increased to 15.07 months (11.9–20.4) with a radiation dose >50 Gy, confirming the importance of neck disease control in patients with stage IVb or IVc disease. However, this also reflects a selection bias as patients who were still alive or in good general condition could complete the radiotherapy sessions. In patients with PS deterioration, a palliative dose (30 Gy) was often chosen.
In addition to confirming some known prognostic factors, we performed a multivariable analysis that included pathological characteristics and NLR. 7,26 We showed that p-ATC was associated with lower OS compared to st-ATC [HR, 1.83; CI, 1.33–2.51, p = 0.001]. The association of st-ATC with a higher OS rate has been reported in retrospective series but has not been previously examined as an independent prognostic factor. 3,4,30 Recently, Greenberg et al. confirmed that mixed-ATC had a better OS than p-ATC in a large cohort, including 763 and 3880 patients with mixed-ATC and p-ATC, respectively, from the National Cancer Database. 16 These pathological subtypes probably reflect some differences in oncogenesis, molecular drivers, transformational processes, and immunological landscape, 3,4,31 but are also associated with different disease stages since stage IVc occurred more frequently in p-ATC than in st-ATC.
We approached the immunological landscape in an imperfect, but clinically applicable manner, by determining NLR, a marker of systemic inflammation and the host immune response. We observed a higher NLR in p-ATC than in st-ATC, suggesting pathophysiological hypotheses to explain the difference in prognosis. Furthermore, we observed an increase in NLR associated with higher stages from IVa to IVc and a lower OS rate with NLR >5.05 [HR, 2.05, CI, 1.39–3.05, p < 0.001]. A high NLR may reflect a higher recruitment of neutrophils (and perhaps other myeloid cells) to the tumor, which fuels a favorable microenvironment for disease progression, thereby potentially explaining the worse OS observed in these patients. 28,32,33 Recently, Xu et al. reported an association between higher NLR and distant metastasis at presentation and poorer prognosis upon univariate analysis, 17 as well as other methods with varying cutoffs. 17,34,35 More studies will be required to validate the prognostic and therapeutic role of NLR in ATC.
In our study, the median OS was 6.8 months (5.5–8.1) for the whole cohort with variability observed among the patient groups, such as patients with localized stage IVa disease (median OS was not reached), or patients who underwent multimodal treatment (median OS: 25.6 [13.3–42.4]), compared to patients with a p-ATC (median OS: 3.7 months [3.0–5.3]) or with a NLR ≥5.05 (median OS: 2.9 months [1.7–4.1]) or treated with BSC (median OS: 0.8 months [0.5–1.3]). Our study provides a multifaceted description of ATC and highlights significant heterogeneity in prognosis, which has partly been overlooked over the years owing to the assumption that ATC is a monomorphic disease entity with very poor prognosis.
Our study highlights the challenges of managing patients with ATC. We revealed a 56-day (26–94) delay from the first compressive symptom to pathological diagnosis, with only 28% of the patients being diagnosed within 1 month from symptom onset. This delay may contribute to the disease prognosis and explain, in part, why 18.3% of the study population received BSC alone. Fast-track management of ATC is associated with better outcomes. 25 Only Wendler et al. reported a BSC rate (4%) although there may have been a selection bias in the ATC series considering the probable number of underreported patients treated with BSC alone in the literature. 2 The nationwide dimension of our study limited this bias. Reducing the time to ATC diagnosis may reduce the number of patients treated with BSC alone, by raising awareness in the medical community about the importance of an urgent workup and establishing appropriate care.
Our study was subject to several limitations. First, it is a retrospective study, and although the TUTHYREF database is a national database, including expert centers network, it lacks the comprehensiveness of population inclusion of a registry. As ATC incidence is estimated to be 0.1 to 0.3 per 100,000 person-years in the different epidemiological series from the United States and Europe, 1,6,8,15,36 we extrapolated that there would be 700 incidental cases in France during the study period (2010–2020); therefore, we estimate that our study covered 58% of the expected ATC incident cases.
Second, we reported a lower rate of stage IVa (4.1% of all patients (n = 15)) than that reported in other studies. 1 –3,7 This could be explained by the median 56 days diagnostic delay in our series or by a selection bias toward more advanced disease managed in the network. Only half of the patients underwent a molecular profile evaluation due to practice heterogeneity among centers in France and the long observation period; therefore, analysis of the prognostic impact of molecular alterations was not feasible. When separating our cohort according to year of diagnosis (2010–2015 vs. 2016–2020), we observed an increase in molecular profiling (42–82% of cases), targeted therapies (12–39), and immunotherapy prescriptions (3–13) but no improvement in OS overtime (median OS 6.3 months vs. 7.7 months, p = 0.957).
However, similar to other reports from tertiary centers, 10 we observed an improved OS in patients treated with either targeted therapy and/or immunotherapy. Moreover, we observed that these innovative treatments were administered as second and further lines of treatment (Supplementary Fig. S1 and Supplementary Table S2). Therefore, improved OS with these novel treatments may be partly biased because the patients who benefited from CRT, surgery, and further treatment lines were those with better prognosis. Our observations are similar to those reported in recently published single-arm phase I and II trials. In the dabrafenib/trametinib phase II study, >80% of the participants underwent prior radiation therapy and surgery, 23 whereas in the phase I trial of spartalizumab, ∼70% of the patients underwent surgery and/or radiation therapy. 20 Unfortunately, tumor PDL-1 expression determined by the Tumor Proportion Score and Combined Positive Score was not evaluated. By collecting multicenter real-life data, we observed that long survival rates were possible in patients with better prognosis (such as low NLR, lower ECOG-PS, stage IVb, and st-ATC), who could benefit from more aggressive treatments. In particular, the median OS was 15.1 months in patients treated with CRT (>50 Gy) and 25.6 months in those treated with multimodal treatment (surgery and CRT).
Because of the prognostic heterogeneity of ATC, randomized trials may be necessary to validate treatment and distinguish between treatment efficacy and prognosis resulting from patient selection. Such trials are feasible, as recently demonstrated by NRG/RTOG 0912. 37 An alternative approach is to use real-world data, as in this study, to build external synthetic control arms for comparative trials, to limit the number of patients exposed to a control treatment with expected poor efficacy. 38
Conclusion
Real-world data from the ENDOCAN-TUTHYREF nationwide network highlighted the multifaceted characteristics of patients with ATC and revealed the association between new prognostic factors such as NLR and pathology with other validated factors such as ECOG-PS, staging, and feasibility of multimodal treatment. This study highlights three challenges in ATC care, which should be addressed over the next decade: (1) improving time to diagnosis, thus reducing the use of exclusive BSC; (2) increasing the number of patients with ATC undergoing multimodal treatment; and (3) improving the characterization of molecular profile with pathological subtypes to achieve personalized medicine.
Footnotes
Acknowledgments
The authors thank N. Synkov, the national Clinical Research Assistant (CRA) of the ENDOCAN-TUTHYREF network who contributed to data collection; the CRAs of other regional centers: T. Cheav, A. Delahaye, M. Hellal, G. Boudou, C. Kergoulay, and A. Kidi; Katty Malekzadeh, the data manager; and all patients who participated in this study.
Authors' Contributions
Investigation (lead), formal analysis (equal), writing original draft (lead), and writing review and editing (lead) by A.J. Formal analysis (equal), writing original draft (supporting), and writing review and editing (equal) by F.G. Conceptualization (equal), database review (equal), writing original draft (supporting), and writing review and editing (equal) by C.d.l.F. Pathological examination (lead) and writing review and editing (equal) by A.A.G., M.D.-P., and E.L. Database completion (equal) and writing review and editing (equal) by J.W., C.N.C., D.D., Y.G., F.I., S.B., S.Z., N.R., M.B.L., L.G., M.K., S.Z., L.L., F.B.C., and C.D.C. Conceptualization (equal), database review and formal analysis (equal), writing original draft (supporting), and writing review and editing (equal) by I.B. Conceptualization (equal), database review and completion (lead), writing original draft (equal), and writing review and editing (equal) by J.H.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
The ENDOCAN-TUTHYREF network, a multidisciplinary nationwide network dedicated to the management of patients with refractory thyroid cancer and funded by the French National Cancer Institute (Institut National du Cancer [INCa]), supported this study with its national database. The authors did not receive any other grant from any funding agency in the public, commercial, or nonprofit sectors.
Supplementary Material
Supplementary Figure S1
Supplementary Figure S2
Supplementary Figure S3
Supplementary Figure S4
Supplementary Table S1
Supplementary Table S2