
Abstract

R
Even though RAS mutated tumors are better differentiated than BRAFp.V600E mutated tumors, the expression of proteins involved in the iodine metabolism is decreased. These abnormalities may be reverted by the inhibition of the MAPK pathway. 4 In a pioneer study on the redifferentiation of RAS mutated radioactive iodine refractory (RAIR) TC with selumetinib (a MEK inhibitor), significant 131I tumor uptake reappeared in all 5 patients, resulting in partial tumor responses in 4 (80%) of the patients treated with 131I. 5
In a recent phase II prospective trial in 21 patients with a BRAFp.V600E mutated RAIR differentiated TC (DTC), dabrafenib-trametinib was associated with reinduction of radioiodine uptake in 95% of the patients with a 6-month response rate of 38%, after the administration of a high 131I activity following recombinant human TSH (rhTSH) injections. 6 In the present study focused on metastatic RAIR RAS-mutated DTC, we investigated the efficacy and safety of trametinib treatment before the administration of a high 131I activity (following rhTSH injections).
MERAIODE is a multicenter, prospective phase II trial in patients with RAIR DTC, with two independent cohorts with similar designs: one for BRAFp.V600E and one for RAS mutated patients (NCT 03244956). The results of the BRAFpV600E-mutated cohort study were recently published. 6 Detailed inclusion and exclusion criteria, procedures and objectives, available in the Supplementary Table S1, were similar to the BRAFp.V600E mutated cohort except for treatment consisting of trametinib-131I.
Briefly, RAIR patients were treated with trametinib (2 mg/day) for 42 days. A 131I diagnostic whole body scan (WBS) (185 MBq, 5 mCi) was performed at baseline prior to trametinib (dc1-WBS) and between days 28 and 35 (dc2-WBS). A fixed 131I activity of 5500 MBq (150 mCi) was administered after rhTSH injections at day 35 ± 2 regardless of the results of the dc2-WBS.
Tumor response was assessed according to RECIST version 1.1 at 1, 3, 6, 12, and 18 months after trametinib initiation or until tumor progression. 7 Patients with a partial response assessed by the local investigator at 6 or 12 months could undergo a second course of trametinib-131I (5500 MBq–150 mCi after rhTSH). The primary endpoint was the overall response rate (ORR) at 6 months according to central review.
This investigator-initiated trial was sponsored by Gustave Roussy and conducted within the French Endocan-TuThyRef network. The study was conducted in accordance with the protocol approved by the ethics committee (Comité de Protection des Personnes Ouest IV; N.33/17 1-PPRE) in accordance with the 2013 revised Declaration of Helsinki. All patients provided written, informed consent. Detailed statistical analysis is available in Supplementary Table S1. Tissue genotyping and gene expression analysis were performed in a central laboratory at Gustave Roussy at the end of the study (Supplementary Tables S1 and S2).
From March 2018 to March 2020, among 13 screened patients, 11 were included (Supplementary Fig. S1). Ten patients were evaluable for the efficacy of the first treatment course at 6 months. Most patients were men (64%) with poorly differentiated TC (45%) (based on central review) (Table 1). Based on the investigator RECIST assessment, 3 patients with partial response (PR) at 6 or 12 months were re-treated with a second course of trametinib-131I.
Initial Characteristics of the 11 Included Patients
Including one insular.
Two pazopanib and one lenvatinib.
One patient with bone RT+cementoplasty and one patient with bone RT only.
ECOG, Eastern Cooperative Oncology Group performance status; GBq, GigaBecquerel; mCi, millicurie; std, standard.
Abnormal 131I uptake was present at baseline (dc1-WBS) in 3 out of 10 (30%) patients, on dc2-WBS in 4 out of 9 (44.4%) patients, and on the post-treatment WBS in 6 out of 10 (60%) patients.
On dc1-WBS, the three patients with abnormal 131I uptake had one metastatic site with 131I uptake. Two of them had two metastatic sites on the dc2-WBS, and one remained with one metastatic site on the dc2-WBS (Supplementary Fig. S2). One patient without abnormal dc2-WBS was found to have abnormal uptake on the post-treatment WBS and in three patients, the number of metastatic sites with abnormal uptake was higher on the post-treatment WBS compared with the dc2-WBS.
At 6 months following the first treatment course, there were no Complete Response, 2 (20%, 95% confidence interval [CI] = [3–56]) PR, 7 (70%, CI = [34–93]) stable disease (SD), and 1 progressive disease (PD) (Table 2, Fig. 1, Supplementary Table S3, and Supplementary Figs. S3 and S4). The median size change of the target lesions was +1.8% (mean = −3.8%; range: −53 to +23) (Fig. 1). The ORR at 1 and 3 months were 10% and 20%, respectively. PERCIST evaluation was available in 9 patients at 6 months, and it demonstrated PR in 2 cases (22%), SD in 6 (67%), and PD in 1 (11%). Among the seven patients without serum Tg antibodies, one patient had a biochemical partial response at three and six months.
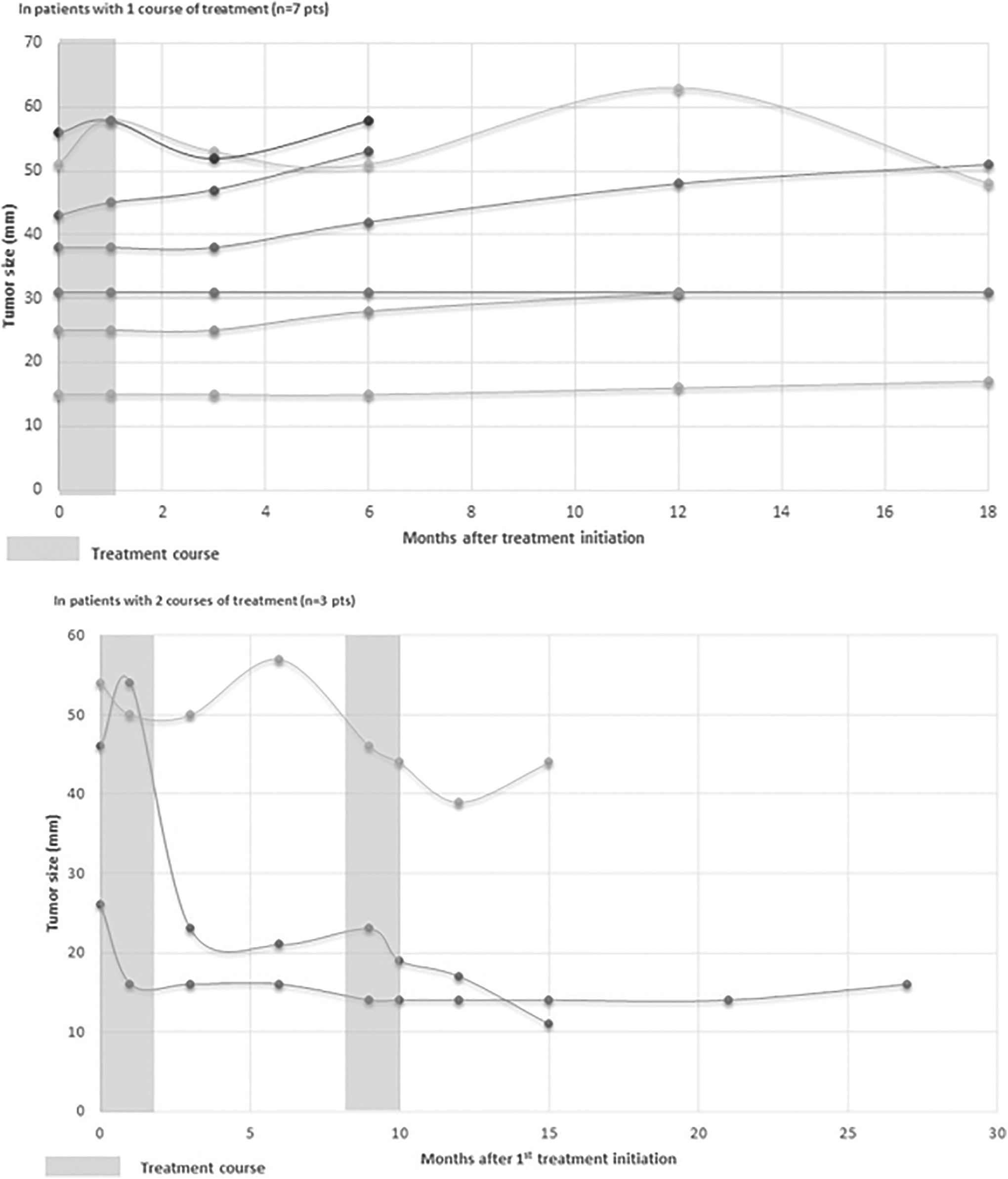
Efficacy of trametinib-131I therapy in the 10 evaluable patients. Evolution of the sum of the size of the target lesions based on independent central review (RECIST v1.1), for the patients treated by one or two courses of treatment.
Radiological Assessment (Central Review) of Efficacy with RECIST Criteria Version 1.1, After First Trametinib-131I Course (A), in the Absence of Second Trametinib-131I Course (B), After Second Course of Trametinib-131I (C)
CI, 95% confidence interval; CT, computed tomography.
The three evaluable patients who had a second treatment course had abnormal 131I uptake on the post-treatment WBS of the second 131I administration. The number of metastatic sites on the second post-treatment WBS was similar to the first post-treatment WBS in two cases and lower in one case (4 vs. 2). Among the 3 patients, 1 had a PR during the 18 months following the second course, whereas the other 2 patients progressed at 3 and 6 months after the second course.
On September 1, 2022, the median follow-up time was 34 months (range: 1.1–49.2). The median Progression Free Survival (PFS) (central evaluation) was 12.0 months. The 12-month-PFS and 24-month-PFS rates (central evaluation) were 60.0%, CI = [25.3–82.7] and 40.0%, CI = [12.3–67.0], respectively. No deaths occurred. None of the patients developed anaplastic transformation during follow-up.
During trametinib treatment, 9 out of 11 (82%) patients experienced at least one AE, related or not to treatment. Most adverse events (AEs) were grade 1 (36%) and grade 2 (27%) (Supplementary Table S4). There were three grade 3 AEs in two patients, and no grade 4.
Treatment was definitively stopped in two cases due to AE: at day 12 for a grade 3 erythematous colitis; at day 28 for a grade 2 decrease of left ventricular ejection fraction. In this last case, 131I was administered.
Following treatment initiation, the global health, the functioning dimensions, and the symptoms were impacted with a deterioration from baseline to the end of treatment (D42), which was reversible afterward (Supplementary Table S5 and Supplementary Fig. S5).
Among the 11 patients included, based on the local RAS mutation assessment, 9 tissue samples were available for Next Generation Sequencing genotyping at the central laboratory. The average coverage depth was 693 × (301 × to 897 × ). Tumor mutational load ranked from 1.7 to 135.7 mutations per megabase. Five samples harbored an NRAS mutation, and two samples harbored an HRAS mutation, whereas no RAS mutation was detected in two samples.
All samples were wild type for TERT promoter. Six samples had one to six additional variants, largely of an unknown significance. Three pathogenic mutations other than RAS were detected, in FANCD2, PTEN, and MSH2 (Supplementary Table S6). The gene expression analysis of 2559 transcripts, from genes associated to cancer, was performed on 8 samples, which did not show significant differential expression associated to tumor response.
This phase 2 trial, which included 11 patients, showed that the administration of trametinib for 6 weeks increased the 131I uptake in two-thirds of RAIR RAS mutated tumors with a 6-month response rate of 20%. These results were not as good as expected, given the previous results of redifferentiation with another MEK inhibitor selumetinib. 5
Trametinib is also less effective in RAIR RAS mutated tumors than the combination of dabrafenib-trametinib in BRAFp.V600E mutated RAIR DTC tumors, for patients otherwise meeting similar inclusion criteria, that is, RAIR, progression within 18 months before inclusion and no lesion over the size of 30 mm. 6
RAS mutated tumors are known to have a better differentiation score than BRAFp.V600E mutated tumors. Indeed, despite being RAIR, 3 of the 10 patients had abnormal 131I uptake on the baseline dc1 WBS compared with 5% in BRAFp.V600E mutated tumors. Further, trametinib was not very efficient in restoring 131I uptake, with only 44% of the cases showing abnormal 131I uptake on the dc2 WBS and 60% on the post-therapy WBS.
Subsequently, the response rate at 6 months was only 20% and the response rate was anecdotal in patients who received a second course of trametinib-131I. The 12- and the 24-month-PFS rates were also low, being 60% and 40%, respectively, in patients who had an RECIST progression within 18 months before inclusion.
We did not observe any decrease in tumor size during trametinib treatment and before the administration of 131I, contrary to the association of anti BRAF and anti-MEK in BRAFp.V600E mutated tumors. 6,8 This observation raises the hypothesis that trametinib alone does not have a major anti-tumor effect. These results also highlight the difficulty in targeting the RAS mutation in oncology, with limited efficacy of anti-MEK treatment and the occurrence of RAS mutation in RAIR DTC as resistance mutation in patients treated with RET or BRAF inhibitors 9,10 inhibitors. Indeed, the KRASG12C mutations for which specific inhibitors such as adagrasib or sotorasib are available are rarely seen in RAIR TC.
The tissue genotyping in this study confirmed a higher frequency of the NRAS mutation. Surprisingly, in two samples, RAS mutations, found locally, were not found on the central analysis performed at the end of the study. Since the protocol did not plan to exclude patients based on this central analysis, these patients were not excluded. One of them though disclosed 131I abnormal uptake on the post-treatment WBS and had a partial response.
Safety of trametinib treatment showed a tolerance concordant to what was expected, with the absence of grade 4 AE event and grade 3 AEs in 18% of the cases.
Given the small sample size of the cohort, this study is mainly descriptive, precluding any definitive conclusion. The high rate of poorly differentiated tumors and the absence of RAS mutation on the central laboratory analysis in two cases might have negatively impacted the present results.
However, this is the first prospective study that used trametinib treatment with 131I treatment administration planned for all patients, and not based on the dc2-WBS findings. It is also the first study to provide long-term follow-up and to explore a second course of trametinib-131I treatment.
Conclusion
The treatment with trametinib in RAS mutated DTC is not highly effective for restoring/increasing 131I uptake, and the administration of high activity (150 mCi, 3700 MBq) of 131I is followed by a low response rate. Other strategies than trametinib alone should be developed for the redifferentiation of RAS mutated RAIR DTC.
Footnotes
Acknowledgments
The authors would like to thank the patients, their families, all research staff, and investigators involved in this study; Catherine Richon and Patrick Saulnier from BMO unit in AMMICa UMS3655/US23 for their technical assistance for Tissue genotyping and GE analysis; and finally Bastien Job from Bionformatic unit in AMMICa UMS3655/US23 for GE bioinformatics analysis.
Authors' Contributions
S.L.: Conceptualization, funding acquisition, investigation, methodology, resources, visualization, and writing—original draft; writing—review and editing. D.B., D.T., C.B., A.S., M.E.G., L.L., and Y.G.: Investigation, resources, and writing–editing. M.A., M.T.-C.-M., and A.A.G.: Resources-editing. L.L.: Resources, writing–original draft; writing–review and editing. N.A.: Methodology. M.S.: Investigation, resources, and writing–review and editing. I.B.: Conceptualization, data curation, formal analysis, methodology, project administration, supervision, validation, and visualization—writing—review and editing.
Author Disclosure Statement
S.L. reports advisory boards from Lilly, EISAI, IPSEN. L.L. reports advisory boards from EISAI, Lilly, Ipsen; AAA, Novartis and Roche. I.B. reports grants from Roche, BMS, Novartis, Gilead, MSD. D.B., D.T., M.A., C.B., M.T.-C.-M., L.L., N.A, M.E.G, A.A.G., M.S., and Y.G. report no competing interests nor personal financial interests.
Funding Information
MERAIODE was financed by the French Ministry of Health, through the National Institute for Cancer (INCa, PHRC2015). Trametinib was provided by Novartis, and rhTSH was provided by Sanofi Genzyme. These companies did not participate in any aspect of the study design, data accrual, data analysis, or manuscript preparation and submission. The authors assume responsibility for the accuracy and completeness of the data and analyses (NCT 03244956).
Supplementary Material
Supplementary Data