
Abstract
Background:
Recent successes with immune checkpoint inhibitors (ICIs) and tyrosine kinase inhibitors (TKIs) for the treatment of solid malignancies have paved the way for a new era of combined therapy. A common side effect seen with each of these classes of treatment is thyroid dysfunction, with rates estimated at 30–40% for TKI and 10–20% for ICI. However, little is known about the effect of combined ICI+TKI therapy on thyroid function. Therefore, this study evaluated the incidence, clinical features, and risk factors for developing thyroid abnormalities during ICI+TKI therapy and the relationship to cancer outcomes.
Methods:
We conducted a retrospective cohort study of patients treated with combination ICI+TKI cancer therapy at City of Hope Comprehensive Cancer Center from 2017 to 2023 who had pretreatment normal thyrotropin (TSH) levels. Primary analyses assessed the frequency, timing, and severity of thyroid function test abnormalities during ICI+TKI cancer therapy, and the requirement for thyroid hormone replacement. Secondary analyses evaluated risk factors for the development of thyroid dysfunction, including sex and drug regimen, and the association with cancer progression-free survival or overall survival. Univariable and multivariable models were used.
Results:
There were 106 patients who received ICI+TKI therapy with a median age of 63.5 years and a median follow-up of 12.8 months (interquartile range [IQR] 5.9–20.9). Notably, 63.2% (67/106) developed thyroid function abnormalities during ICI+TKI therapy, including 11 (10.4%) with hyperthyroidism, 42 (39.6%) with subclinical hypothyroidism (SCHypo), and 14 (13.2%) with overt hypothyroidism. The onset of thyroid dysfunction occurred at a median of 7 weeks (IQR 3.1–9.0) after start of ICI+TKI treatment for hyperthyroidism, 8.0 weeks (IQR 3.0–19.0) for SCHypo, and 8.1 weeks (IQR 5.9–9.1) for overt or worsening hypothyroidism. Hyperthyroidism resolved to hypothyroidism or normal TSH without intervention in all subjects, suggesting thyroiditis, and hypothyroidism was readily treated with thyroid hormone replacement.
Conclusions:
Thyroid dysfunction is a frequent adverse event in individuals treated with combination ICI+TKI therapy, with our data suggesting a rapid onset and higher incidence than previously seen with ICI or TKI therapy alone. Therefore, close monitoring of thyroid function during initial therapy and multidisciplinary care with endocrinology are recommended to facilitate early detection and initiation of thyroid hormone replacement in these patients.
Introduction
An estimated 19.3
ICIs activate antitumor immune responses by blocking regulatory proteins on T cells (i.e., cytotoxic T lymphocyte antigen [CTLA]-4, programmed death protein/ligand [PD-1/PD-L1]) and are used for the treatment of patients with melanoma, breast, renal, liver, lung, and head and neck cancers, among others. 5 Because of increased immune activation, many patients develop unwanted autoimmunity in healthy tissues, termed immune-related adverse events (irAEs).
Thyroiditis is a common irAE occurring in ∼10% of individuals during single agent and 20% during combination therapy (e.g., anti-PD-1/anti-PD-L1+CTLA-4). 6 –11 ICI-thyroiditis usually resolves to permanent hypothyroidism requiring thyroid hormone replacement 6,12 and shows near equal incidence in males and females. 13 ICI-thyroiditis is strongly correlated with a beneficial response to ICI treatment, including longer progression-free survival (PFS) and overall survival (OS). 7,8,10,14 –18
TKIs selectively block signaling through growth factor receptors (e.g., vascular endothelial growth factor receptor [VEGFR]) to inhibit cancer cell proliferation and survival. As with ICI, thyroid dysfunction is common, occurring in nearly 40% of TKI-treated patients, with overt hypothyroidism (27%) being the most common, followed by subclinical hypothyroidism (SCHypo; 13%) and rarely hyperthyroidism. 19,20 Risk factors for TKI-associated thyroid dysfunction include female sex and perhaps cumulative TKI exposure. 4,21
While incompletely understood, proposed mechanisms for TKI-associated thyroid dysfunction include direct thyroid follicular cell death, decreased blood flow secondary to VEGFR inhibition, immune-mediated thyroiditis, and impaired iodine uptake by thyroid follicular cells leading to decreased thyroid hormone production. 20,22 TKI-associated thyroid dysfunction, similar to ICI-thyroiditis, has been correlated with longer OS. 19,23
Success with ICI and TKI therapies led to clinical trials evaluating combined ICI+TKI regimens, and subsequently their approval for endometrial cancer in 2019 and renal cell carcinoma in 2021. Preliminary reports suggest that rates of thyroid dysfunction during combined ICI+TKI therapy may be increased; however, studies directly addressing this question have not yet been done. 24,25
The aim of this study was to determine the effect of ICI+TKI therapy on thyroid function in treatment-naive patients with documented normal pretreatment thyrotropin (TSH) levels, as well as risk factors for treatment-associated thyroid abnormalities and the relationship to clinical cancer outcomes. Such data are needed to guide clinical recommendations for the many patients now receiving combined ICI+TKI regimens.
Materials and Methods
Study design and participants
We performed a retrospective analysis of patients treated with combined ICI+TKI therapy at City of Hope Comprehensive Cancer Center (COH) from 2017 to 2023. We included adults with solid malignancies (excluding nonmelanoma skin cancers) who were treated concurrently with FDA-approved ICI and TKI therapies. During the study period, these agents included ICIs (pembrolizumab, nivolumab, and ipilimumab) and TKIs (lenvatinib, axitinib, sunitinib, pazopanib, cabozatinib, tivozanib, and imatinib).
Patients with insufficient thyroid function tests to discern a clear pattern of ICI+TKI effect, prior ICI and/or TKI therapy, a pre-existing diagnosis of thyroid cancer, or prior thyroid removal or ablation were excluded. To ensure accuracy and consistency, all data were collected manually by a board-certified endocrinologist. This study was approved by the COH Institutional Review Board (IRB #23043).
Study definitions
Patients identified as “No Thyroid Abnormalities” had no thyroid function abnormalities after receiving ICI+TKI. Hyperthyroidism was defined as a low TSH and elevated free thyroxine (fT4). Hypothyroidism was defined as elevated TSH and low fT4. SCHypo was defined as elevated TSH with normal fT4 level. Subclinical hyperthyroidism (SCHyper) was defined as low TSH with normal fT4 level.
Worsening hypothyroidism was defined as needing an increase in thyroid hormone therapy (e.g., levothyroxine [LT4]) dose to achieve euthyroid status after initiation of ICI+TKI. Some patients who had SCHypo or hypothyroidism but were never started on LT4 or were deceased before initiation of LT4 were denoted as such. Thyroid function tests that corresponded to potential nonthyroidal illness, medication nonadherence or malabsorption, were excluded from the analysis. In patients who started or had adjustments in their LT4, euthyroid state was defined as achieving a normal TSH level.
Thyroid hormone replacement dose was documented for patients who achieved euthyroid state while on medication. In cases where the patient was taking <7 tablets a week and achieved euthyroid state, an average daily dose was calculated. Weight-based thyroid hormone dosing (mcg/[kg·day]) was calculated by using the daily dose needed to achieve euthyroid state divided by the patient's weight.
Statistical analyses
Descriptive statistics were used to summarize patient baseline characteristics, initial thyroid changes after ICI+TKI, and LT4 replacement dose. Differences in characteristics between patients with and without thyroid abnormalities were compared using the Kruskal–Wallis test for continuous variables and chi-square tests for categorical variables.
Risk factor associations were calculated using odds ratios (ORs) and confidence intervals [CIs] using univariable and multivariable logistic regression models. Our multivariable model adjusted for age at ICI+TKI initiation. Factors such as the type of cancer were not included in our multivariable models due to the limited number of patients in some categories. Instead, we performed sensitivity analyses to examine the impact of female sex on risk of thyroid abnormalities in different cancer combinations.
To assess for associations with PFS or OS, hazard ratios (HR) and corresponding [CIs] were calculated using univariable and multivariable Cox regression models. 26 The factors of interest included sex, type of cancer, age at ICI+TKI initiation, type of ICI+TKI therapy, and presence or absence thyroid function test abnormalities. All statistical tests were two-sided at a significance level of 0.05. Analyses were performed using SAS version 9.4 (SAS Institute, Cary, NC).
Results
Study population and baseline characteristics
There were 133 eligible patients who received concurrent treatment with ICI and TKI (Fig. 1). Twenty-seven patients were excluded because they received ICI before combination ICI+TKI (n = 6), received TKI before combination ICI+TKI (n = 7), received ICI and TKI separately before ICI+TKI (n = 5), or did not receive ICI+TKI or had incomplete data (n = 9). A total of 106 patients remained in the cohort. The median follow-up period for these 106 patients was 12.8 months (interquartile range [IQR] 5.9–20.9).
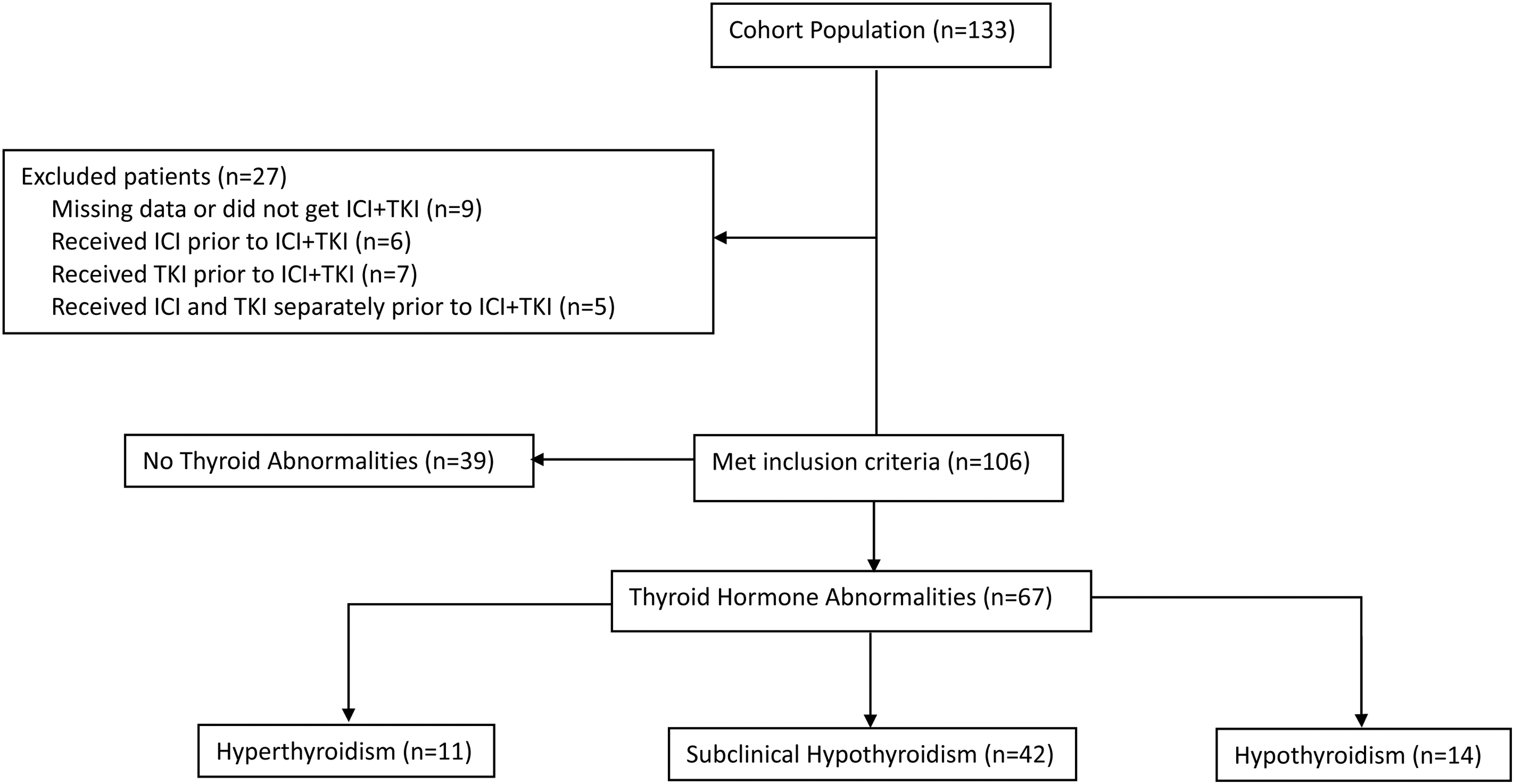
Flowchart of study sample selection.
Patient characteristics are shown in Table 1. The median age at initial ICI+TKI treatment was 63.5 years (IQR 57.0–69.0). Most patients (n = 75, 70.8%) were female and uterine cancer (n = 46, 43.4%) was the most common malignancy. The racial diversity of subjects was 54.7% White, 20.8% Asian, 10.4% unknown, 9.4% Black, and 4.7% other, and most patients (n = 74, 69.8%) were non-Hispanic. Only six (5.7%) patients had prior head and/or neck radiation treatment.
Patient Characteristics for Total Study Population
The bold values are significant p values.
p-Value estimated from chi-square test, except where otherwise noted.
Kruskal–Wallis test.
ECOG, Eastern Cooperative Oncology Group; ICI, immune checkpoint inhibitor; IQR, interquartile range; TgAb, thyroglobulin antibody; TKI, tyrosine kinase inhibitor; TPOAb, thyroid peroxidase antibody.
The most common ICI+TKI therapy was pembrolizumab+lenvatinib (n = 73, 68.9%). Most (n = 59, 55.7%) had Eastern Cooperative Oncology Group 1 at the time ICI+TKI therapy was used, and 47 (44.3%) patients used ICI+TKI as second-line therapy. Ninety-five (89.6%) patients had unknown thyroid peroxidase antibody (TPOAb) or thyroglobulin antibody status. Statistically significant differences between patients who developed thyroid function abnormalities and those who remained euthyroid were found for sex, type of cancer, and ICI+TKI combination (Table 1).
Incidence and pattern of thyroid function abnormalities
Thyroid function abnormalities occur as a side effect of ICI and TKI and, therefore, routine monitoring of thyroid function has been recommended for patients receiving these agents. 4,27 However, guidance for monitoring during combination ICI+TKI is lacking. Strikingly, of 106 euthyroid patients, 63.2% (67/106) developed new thyroid abnormalities after initiation of ICI+TKI. These included 11 (10.4%) with initial hyperthyroidism, 42 (39.6%) having initial SCHypo, and 14 (13.2%) having initial overt hypothyroidism (Fig. 1). The timing and severity of thyroid function abnormalities are shown in Table 2 and are discussed hereunder.
Initial Thyroid Changes After Immune Checkpoint Inhibitor+Tyrosine Kinase Inhibitor
fT4, free thyroxine; TSH, thyrotropin.
Hyperthyroidism group
Eleven patients presented with hyperthyroidism and no patients were categorized as SCHyper. The median time from initial exposure of ICI+TKI to hyperthyroidism was 7 weeks (IQR 3.1–9.0), median TSH was 0.02 mIU/L (IQR 0.01–0.02), and median fT4 was 2.34 ng/dL (IQR 1.90–3.19) (Table 2). In five patients who had Graves' autoantibody testing (e.g., thyroid stimulating immunoglobulin or anti-TSH receptor), results were all negative.
In addition, one patient underwent a radioactive iodine uptake scan that showed thyroiditis. One patient who was on methimazole briefly while awaiting Graves' autoantibody testing had medication subsequently discontinued. All cases of hyperthyroidism resolved to normal thyroid state or hypothyroidism without intervention in 12 weeks. Specifically, five (45.5%) patients evolved from hyperthyroidism to hypothyroidism and required LT4, one (9.1%) patient converted from hyperthyroidism to hypothyroidism and did not start LT4, three (27.3%) patients had hyperthyroidism to SCHypo requiring LT4, and two (18.2%) patients had hyperthyroidism that evolved to euthyroid without LT4 (Supplementary Table S1).
The median time from hyperthyroidism to SCHypo or Hypo was 6.7 weeks (IQR 6.0–12.0) (Supplementary Table S1). A median TSH of 106.95 mIU/L (IQR 67.00–152.00) and median fT4 of 0.46 ng/dL (IQR 0.41–0.49) was seen in those who converted from hyperthyroidism to hypothyroidism only and a maximum TSH of 21.49 mIU/L (IQR 7.08–57.80) was seen for those who converted from hyperthyroidism to SCHypo only (Supplementary Table S1).
Hypothyroidism group
Another subgroup of patients presented with hypothyroidism as their initial thyroid function abnormality. In these 14 patients, 7 (50%) patients had overt hypothyroidism and 7 (50%) patients had worsening hypothyroidism. Of the 12 patients with data on thyroid function tests, the observed median time from initial ICI+TKI therapy to hypothyroidism was 8.1 weeks (IQR 5.9–9.1), with a median TSH of 106.70 mIU/L (IQR 48.95–139.95) and median fT4 of 0.48 ng/dL (IQR 0.42–0.58) (Table 2). The median time from hypothyroidism to euthyroid state was a median of 21.9 weeks (IQR 21.4–37.0) (Supplementary Table S1).
SCHypo group
A third subgroup of patients developed SCHypo during ICI+TKI treatment. Among these 42 patients with new SCHypo after initial ICI+TKI treatment, 24 (57.1%) had SCHypo TSH >10 on LT4, 3 (7.1%) had SCHypo TSH <10 on LT4, 7 (16.7%) had SCHypo TSH >10 not on LT4, 4 (9.5%) had SCHypo TSH <10 not on LT4, and 4 (9.5%) had SCHypo TSH <10 resolved without LT4 (Supplementary Table S1). Using available data from 41 patients, the median time from initial ICI+TKI to SCHypo was 8.0 weeks (IQR 3.0–19.0) with a median TSH of 19.2 mIU/L (IQR 9.70–36.60) (Table 2). The median time from SCHypo to euthyroid state was 20.0 weeks (IQR 11.1–31.1) (Supplementary Table S1).
In summary, new onset hyper- or hypothyroidism occurred in many patients treated with combination ICI+TKI therapy and occurred during the early phases of treatment, with a median time onset of 7–8 weeks.
Differences in thyroid function abnormalities by sex and ICI+TKI regimen
Female sex is a well-established risk factor for spontaneous thyroid disease (e.g., Hashimoto's thyroiditis and Graves' disease), 28,29 and has been linked to TKI- but not consistently with ICI-associated thyroid dysfunction. 4,7 –10 Multivariable analysis, after controlling for age at initiation of ICI+TKI, showed that compared with males, females who received ICI+TKI treatment had a 2.72-fold (adjusted OR = 2.72 [CI 1.12–6.61] p = 0.0267) increased risk of developing thyroid abnormalities (Table 3).
Associations with Risk of Thyroid Abnormalities
The bold values are significant p values.
Model adjusted for age at initiation of ICI and TKI initiation.
[CI], confidence interval; OR, odds ratio.
We were unable to include cancer type in our multivariable models due to the low number of colon cancer and hepatocellular carcinoma patients, although our univariable analysis showed that cancer type was associated with risk of thyroid abnormalities (Table 1). Because there were 50 female patients being treated for uterine cancer or breast cancer, we examined the potential impact of female sex on risk of thyroid abnormalities within different types of cancers.
While all adjusted OR estimates were >1 (OR range: 1.40–4.24) (Supplementary Table S2), these ORs were not statistically significant and likely limited by our small numbers of patients within each type. The association between female sex and thyroid dysfunction needs to be further validated in larger studies across both sexes.
We also evaluated whether thyroid dysfunction risk is associated with a specific regimen. Pembrolizumab+lenvatinib and pembrolizumab+axitinib were the most common ICI+TKI regimens in our patients. Our data did not show any difference in the risk of thyroid abnormalities between patients using these regimens (adjusted OR = 0.50 [CI 0.19–1.31], p = 0.1570) (Table 3). These data suggest that this adverse event is a class effect for combined ICI anti-PD-1/anti-PD-L1 and TKI therapy.
Thyroid hormone replacement and resolution
Table 4 shows the LT4 replacement dose required in the subset of patients who achieved euthyroid state on LT4. The calculated mean ± standard deviation (SD) dose of LT4 was 106.55 ± 40.91 mcg/day with a weight-adjusted mean ± SD dose of 1.52 ± 0.69 mcg/(kg·day) with a median dose of 88 mcg/day (IQR 75–150) and a weight-adjusted median dose of 1.76 mcg/(kg·day) (IQR 0.87–1.89).
Levothyroxine Replacement Dose in Patients with Acquired Hypothyroidism Who Achieved Euthyroid State
Two patients had missing value.
One patient had missing value.
SCHypo, subclinical hypothyroidism.
Similarly in the 21 SCHypo patients that had data to calculate LT4 dosing, the mean ± SD calculated dose in the SCHypo group was 75.62 ± 38.83 mcg/day with a mean ± SD weight-adjusted dose of 1.05 ± 0.56 mcg/(kg·day) and a median daily dose of 75 mcg/day (IQR 50–100) and median weight-adjusted dose of 1.03 (IQR 0.64–1.32) mcg/(kg·day). Only 25/106 (23.6%) patients received endocrinology care.
PFS and OS
Prior studies showed that individuals who developed thyroid dysfunction during ICI or TKI monotherapy had longer PFS and OS. 7,8,10,14 –19 In our study, development of thyroid function abnormalities was not associated with differences in risk of cancer progression or risk of all-cause mortality. Our analysis also included sex, age at ICI+TKI therapy, cancer type, and treatment regimen as predictors of survival. Females had an increased risk of disease progression (adjusted HR = 2.20 [CI 1.03–4.71], p = 0.0428) (Table 5). Cancer type was associated with clinical outcomes, namely significantly increased PFS and OS in renal cell carcinoma and decreased PFS and OS in breast cancer compared with the uterine cancer reference group (Table 5).
Univariable and Multivariable Analysis of Progression-Free Survival and Overall Survival
The bold values are significant p values.
Variables in the table mutually adjusted for each other.
HR, hazard ratio.
Compared with pembrolizumab+lenvatinib use, pembrolizumab+axitinib was associated with decreased risk for both progression (unadjusted HR = 0.32 [CI 0.17–0.61], p = 0.0006) and all-cause mortality (unadjusted HR = 0.36 [CI 0.15–0.87], p = 0.0228) in univariable analyses, but this association was not seen in multivariable analyses (Table 5). In summary, sex and cancer type were associated with disease progression and all-cause mortality during ICI+TKI therapy. However, the development of thyroid function abnormalities was not significantly linked to these outcomes.
Discussion
Combination ICI+TKI therapy is an emerging strategy for the treatment of multiple solid malignancies. In this study, we report the frequency, timing, and severity of thyroid function abnormalities in previously euthyroid, treatment-naive individuals undergoing combination ICI+TKI therapy. Importantly, the incidence of ICI+TKI thyroid dysfunction was 63.2%, which is much higher than that previously reported levels of thyroid adverse events with ICI (∼10–20%) or TKI (∼30–40%) therapies alone. 4,7,8,11
In our patients, the elapsed time from ICI+TKI initiation to the development of thyroid abnormalities was similar to that reported for ICI-thyroiditis (5–7 weeks 2,3,12 ) but shorter than TKI-associated thyroid dysfunction (28–36 weeks 4 ). In addition, the thyroid hormone dose required to achieve euthyroid state for patients with overt hypothyroidism after ICI+TKI treatment was higher than that previously reported for treatment of ICI-associated hypothyroidism (1.76 mcg/[kg·day] vs. 1.45 mcg/[kg·day]). 2,3,12
This difference may reflect increased metabolism of thyroid hormone by TKI, greater thyroid gland tissue destruction, or nonthyroid factors such as decreased gut absorption in patients on ICI+TKI therapy. The median LT4 dose needed to achieve euthyroid state in SCHypo patients was lower than in those with overt hypothyroidism. 2,3,12
Despite the frequency of thyroid dysfunction in our cohort and the known associations with ICI and TKI monotherapies, 23.6% received endocrinology care and some with hormone abnormalities did not receive hormone treatment. The median time from SCHypo or hypothyroidism (overt hypothyroidism and worsening hypothyroidism) to euthyroid state was 20.0–21.9 weeks. With increased awareness of these thyroid function test patterns, the time to euthyroid state may be reduced.
Our study also sought to identify risk factors for the development of thyroid dysfunction. Autoimmune thyroid disease, including Hashimoto's thyroiditis and Graves' disease, occur more often in women (8:1 female to male ratio). 28,29 Female sex was also a significant risk factor for TKI-associated thyroid dysfunction. 4 By contrast, ICI-thyroiditis appears to have more equal incidence in males and females, although the data are mixed. 7 –10,13 Our unadjusted analysis showed 2.7-fold increased risk of developing thyroid dysfunction for females (p = 0.0267), but sex was not a significant factor in a subsequent sensitivity analysis that excluded female prevalent uterine and breast cancer patients.
Whether these data indicate that there is no true sex difference or that our adjusted sample was too small to detect this risk cannot be determined. Thyroid dysfunction during ICI or TKI therapy is now recognized as a “class” effect of these agents, although there may be subtle differences in the rates among specific reagents. 4,6,11 We found a similar risk of developing thyroid dysfunction between ICI+TKI regimens, suggesting that this adverse event may also be a “class” effect for combination therapy with anti-PD-1/anti-PD-L1 antibodies and TKIs.
We assessed the relationship between incident thyroid dysfunction and response to ICI+TKI therapy. There is a consensus that thyroid irAEs are associated with longer OS, decreased mortality, and improved response to cancer therapy. 7,8,10,14 –18 Similarly, patients with overt hypothyroidism or SCHypo while on TKI had improved OS. 19,23 We found no association between the development of treatment-associated thyroid dysfunction and PFS or OS in this cohort, but this finding may be attributed to our small sample size given the emerging nature of this treatment combination.
In addition, female sex was associated with worse clinical outcomes. Potential confounders to this finding include worse outcomes in female predominant cancers (e.g., uterine), either inherent to a specific tumor type or in conjunction with ICI+TKI therapy; increased rates of thyroid dysfunction in females; and the use of ICI+TKI regimens predominantly in subjects with advanced stage malignancies.
Female sex (genetic and/or hormonal) has been previously associated with increased tumor immune surveillance and editing, which may also impact the efficacy of ICI+TKI cancer therapy. 13 Given these multiple inter-related factors, the relationship between sex and clinical outcomes with ICI+TKI therapy warrants further study.
Limitations of our study include the inherent retrospective nature and modest sample size. Inherent in the retrospective design, we acknowledge that some thyroid function changes may not have been not captured in the medical records. However, the recommendation for TSH screening in all patients receiving ICI therapy with each cycle (typically every 3–4 weeks) resulted in most patients having regular assessment of thyroid function.
We acknowledge that an acute thyrotoxicosis phase in patients that subsequently evolved to hypothyroidism may have been missed in some. In addition, free triiodothyronine (fT3) levels were not routinely checked in this patient population, consistent with current guidelines for monitoring thyroid dysfunction during cancer immunotherapy, but, nevertheless, may have limited our identification of patients with SCHyper.
Furthermore, this study was not designed to evaluate OS and PFS and, therefore, the lack of association with survival may be a result of insufficient subjects and future studies with larger sample sizes with longer follow-up are needed. Finally, our data suggest a potential association with female sex and treatment-associated thyroid dysfunction, but our analyses were limited by the unequal sex distribution across cancer types and sample size.
Similarly, few patients had assessment of thyroid autoantibodies, which may be important as a risk predictor for thyroid dysfunction as it is in ICI-thyroiditis, 30 but could not be evaluated in this study. Larger and prospective studies of ICI+TKI treatment that are inclusive of both sexes, multiple cancer types, and assess potential predisposing risk factors such as TPOAb status are needed to answer these remaining questions.
Conclusions
Thyroid dysfunction is a frequent adverse event in individuals treated with combination ICI+TKI therapy, with our data suggesting a rapid onset and higher incidence than previously seen with ICI or TKI therapy alone. Close monitoring of thyroid function during initial therapy is recommended to facilitate early detection and initiation of thyroid hormone replacement in these patients.
Footnotes
Acknowledgments
The authors would like to acknowledge the work provided by the Leadership and Staff of the COH Center for Informatics most notably Research Informatics, and the utilization of the POSEIDON data exploration, visualization, and analysis platform, including the Honest Broker process.
Authors' Contributions
Conceptualization (co-lead), writing—original draft (lead), data curation (lead), data analysis (supporting), and table preparation (supporting) by K.T. Statistical analysis (lead), table preparation (lead), and writing—review and editing (supporting) by H.M. Writing—review and editing (supporting) and writing—original draft (supporting) by T.L. Writing—review and editing (supporting) by Y.X., S.C., T.D., and D.B. Conceptualization (co-lead), writing—review and editing (co-lead), project administration (co-lead), data analysis (supporting), and supervision (lead) by M.L.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This study was supported by grants from the NIH (K08DK129829, Melissa G. Lechner), the Doris Duke Charitable Foundation (Melissa G. Lechner), and the Aramont Charitable Foundation (Melissa G. Lechner).
Supplementary Material
Supplementary Table S1
Supplementary Table S2