
Abstract
Background:
The dabrafenib plus trametinib combination (DT) has revolutionized the treatment of BRAFV600E -mutated anaplastic thyroid carcinoma (BRAFm-ATC). However, patients eventually develop resistance and progress. Single-agent anti-PD-1 inhibitor spartalizumab has shown a median overall survival (mOS) of 5.9 months. Combination of immunotherapy with BRAF/MEK inhibitors (BRAF/MEKi) seems to improve outcomes compared with BRAF/MEKi alone, although no direct comparison is available. BRAF-targeted therapy before surgery (neoadjuvant approach) has also shown improvement in survival. We studied the efficacy and safety of DT plus pembrolizumab (DTP) compared with current standard-of-care DT alone as an initial treatment, as well as in the neoadjuvant setting.
Methods:
Retrospective single-center study of patients with BRAFm-ATC treated with first-line BRAF-directed therapy between January 2014 and March 2023. Three groups were evaluated: DT, DTP (pembrolizumab added upfront or at progression), and neoadjuvant (DT before surgery, and pembrolizumab added before or after surgery). The primary endpoint was mOS between DT and DTP. Secondary endpoints included median progression-free survival (mPFS) and response rate with DT versus DTP as initial treatments, and the exploratory endpoint was mOS in the neoadjuvant group.
Results:
Seventy-one patients were included in the primary analysis: n = 23 in DT and n = 48 in DTP. Baseline demographics were similar between groups, including the presence of metastatic disease at start of treatment (p = 0.427) and prior treatments with surgery (p = 0.864) and radiation (p = 0.678). mOS was significantly longer with DTP (17.0 months [confidence interval CI, 11.9–22.1]) compared with DT alone (9.0 months [CI, 4.5–13.5]), p = 0.037. mPFS was also significantly improved with DTP as the initial treatment (11.0 months [CI, 7.0–15.0]) compared with DT alone (4.0 months [CI, 0.7–7.3]), p = 0.049. Twenty-three patients were in the exploratory neoadjuvant group, where mOS was the longest (63.0 months [CI, 15.5–110.5]). No grade 5 adverse events (AEs) occurred in all three cohorts, and 32.4% had immune-related AEs, most frequently hepatitis and colitis.
Conclusions:
Our results show that in BRAFm-ATC, addition of pembrolizumab to dabrafenib/trametinib may significantly prolong survival. Surgical resection of the primary tumor after initial BRAF-targeted therapy in selected patients may provide further survival benefit. However, conclusions are limited by the retrospective nature of the study. Additional prospective data are needed to confirm this observation.
Introduction
Anaplastic thyroid carcinoma (ATC) is one of the most lethal human malignancies. 1 Until recently, a diagnosis of ATC was universally fatal, with a historical median overall survival (mOS) of ∼5–6 months. 2 –5 Broader access to next-generation sequencing (NGS) over the past decade has allowed better understanding of the molecular drivers of ATC. Notably, about 40% harbor a BRAFV600E mutation, for which targeted therapies are available. 6 In 2018, the Food and Drug Administration (FDA) approved the combination of BRAF inhibitor (BRAFi) dabrafenib plus MEK inhibitor (MEKi) trametinib (DT) for the treatment of locally advanced or metastatic BRAFV600E -mutated ATC (BRAFm-ATC) following results of the phase II Rare Oncology Agnostic Research (ROAR) trial, which showed an mOS of 14.5 months. 7 However, real-world data suggest that these drugs may impart a much shorter overall survival (OS). 8 In addition, most patients eventually progress on DT, likely due to the development of new mutations secondary to selective pressure. 9 –11
ATCs are immunogenic tumors, often expressing PD-L1 at high levels. 12 Yet, efficacy of single-agent immune checkpoint inhibitors (ICIs) in ATC is modest. In a phase II prospective trial of the anti-PD-1 spartalizumab in ATC, the overall response rate (ORR) was 19%, and the mOS was 5.9 months. 13 However, among patients who had a clinical benefit, responses were durable. As single-agent ICIs take time to start showing effect and ATC is a rapidly growing tumor, there is an interest in combining their durable clinical benefit with the rapid-onset and high response rates achieved with BRAF/MEK inhibitors (BRAF/MEKi). We previously showed that a combination of immunotherapy with kinase inhibitors (KIs) improved OS in ATC compared with KI alone, 14 and that adding pembrolizumab as a salvage to KI at the time of progression can also prolong survival. 15 However, no study comparing directly BRAF/MEKi alone with BRAF/MEKi plus ICI in BRAFm-ATC is currently available.
Since 2017, standard treatment for BRAFm-ATC at our institution has included an anti-PD-1 ICI in addition to DT. Thus, we aimed to compare the efficacy and safety of combination of DT plus pembrolizumab (DTP) to the current standard-of-care DT alone, in locally advanced or metastatic BRAFm-ATC. This is an expanded cohort with additional patients and longer follow-up compared with our previous publications. 6,14,16
Materials and Methods
Study population
This single-center retrospective cohort study was approved by the MD Anderson Cancer Center (MDACC) Institutional Review Board. All patients presenting with a BRAFm-ATC between January 1, 2014, and March 1, 2023, treated with DT for at least 2 weeks, with or without an anti-PD-1 ICI, were eligible for inclusion. BRAFV600E mutation was identified by immunohistochemistry (IHC), and/or NGS testing of tumor tissue or cell-free DNA (liquid biopsy). Patients initially treated with DT but later switched to another BRAF/MEKi combination due to intolerable adverse effects (AEs) to DT were accepted. Patients treated on the ROAR phase II trial were also included, either in the DT group or in the DTP group if they received an anti-PD-1 at progression. Anti-PD-1 ICIs utilized in the study included pembrolizumab and nivolumab.
Patients treated within a clinical trial that has not yet been published, those previously treated with another KI, patients with anaplastic transformation of a differentiated thyroid carcinoma while on a KI, and patients who received radioiodine while on DT (redifferentiation strategy) for treatment of suspected well-differentiated distant metastases were excluded. Patients unable to swallow could receive the oral KI through their gastric tube or by dissolving the pills following standardized directives.
Study groups
Patients were divided into three groups for analyses: (1) DT group, defined as patients treated with DT alone; (2) DTP group, defined as patients treated with upfront DTP or upfront DT+addition of an anti-PD-1 ICI at progression; and a third exploratory (3) neoadjuvant group, defined as patients treated with neoadjuvant DT followed by definitive surgery for primary disease and pembrolizumab added either before or after surgery. A single infusion of anti-PD-1 was sufficient to consider the patient as having received pembrolizumab or equivalent. Patients in the DT and DTP groups could have had surgery before initiation of systemic therapy but did not undergo any additional surgical resection of neck disease while on or after systemic therapy, distinguishing them from the neoadjuvant group.
Outcomes and study assessments
The study's primary endpoint was OS in the DT and DTP groups. Secondary outcomes included best overall response (BOR) and progression-free survival (PFS) in patients treated with DTP compared with DT as the initial systemic therapy. As an exploratory endpoint, we assessed OS in the neoadjuvant group.
PFS was defined as the time between the first dose of BRAFi and documented disease progression or death. OS was defined as the time between the first dose of BRAFi and death from any cause. Patients who were still alive at data cutoff were censored at last evidence of continued response or last follow-up for OS and PFS analyses, respectively. Grade 5 AEs to BRAF/MEKi as well as all immune-related AEs (ir-AEs) were assessed.
Demographics, pathology, mutational analysis, AEs, and survival data were extracted from patients' electronic medical records. A single radiologist reviewed all images of patients treated with DT or DTP as the initial systemic therapy regimen. Response was assessed by percentage change in target lesion size between initial and serial post-treatment computed tomography (CT) scans and/or 18 F-fluorodeoxyglucose positron emission tomography combined with CTs, using Response Evaluation Criteria in Solid Tumors (RECIST) version 1.1. 17 We reported ORRs, defined as complete response (CR) plus partial response (PR) as the BOR.
Statistical analyses
Demographic and treatment characteristics were presented as medians with ranges for continuous variables, and as numbers with percentages for categorical data. The Kaplan–Meier method was used to analyze PFS and OS endpoints. Kaplan–Meier survival curves for OS and PFS were plotted and compared using the log-rank test. We also modeled OS via a Cox proportional hazards regression. A two-sided p < 0.05 indicated statistical significance. IBM SPSS Statistics for Macintosh, Version 28.0, and Stata/MP v17.0 (College Station, TX) were used for statistical analyses.
Results
Baseline characteristics
Between January 1, 2014, and March 1, 2023, 158 patients with BRAFm-ATC presented to MDACC (Fig. 1). Of these, 94 fulfilled the study's inclusion criteria, and were divided into the following 3 groups: 23 patients were included in the DT group, 48 in the DTP group, and 23 in the neoadjuvant group. Baseline demographics and disease characteristics of patients are presented in Table 1. Characteristics were similar across groups, including median age, gender, and stage distribution. Most patients had distant metastases at initiation of systemic therapy. In ICI-treated patients, all evaluable specimens but one had a PD-L1 score ≥1%. Patients unable to swallow DT represented 30% (7/23) of the DT group and 25% (12/48) of the DTP group.

Flow diagram for study groups. ATC, anaplastic thyroid carcinoma; BRAF/MEKi, BRAF and MEK inhibitors; DT, dabrafenib/trametinib; P, pembrolizumab; RAI, radioactive iodine.
Baseline Characteristics
ATC, anaplastic thyroid carcinoma; DT, dabrafenib/trametinib; DTP, dabrafenib/trametinib+pembrolizumab; EBRT, external beam radiation therapy; IQR, interquartile range.
Neutrophil-to-lymphocyte ratio (NLR) at the time of diagnosis, which was recently shown to be an independent predictor for survival in ATC, 18 was available for 72 patients (16 in DT, 36 in DTP, and 20 in neoadjuvant groups). Median baseline NLR was similar between the three groups: 5.6 (range, 1.78–25.6) in DT, 4.4 in DTP (1.36–22.14), and 4.5 in DTP (2.3–24.4). All patients treated with anti-PD-1 ICI received pembrolizumab, except for one who received nivolumab. Other than BRAFV600E , most common additional mutations at baseline included TP53, TERT promoter, PIK3CA, NF1/NF2, and CDKN2A mutations (Fig. 2).

Oncoprint of somatic mutations in 86 patients with available mutational data. DTP, dabrafenib/trametinib+pembrolizumab.
As of May 31, 2023, median duration of follow-up was 102 months (range, 0.6–102) for the DT group, 28 months (range, 3–63) for the DTP group, and 42 months (range, 5–75) for the neoadjuvant group (Table 2). Two out of the 23 patients in the DT group (9%), 21/48 patients in the DTP group (44%), and 15/23 patients in the neoadjuvant group (65%) were still alive at data cutoff. Information about circumstances of death was available for 42 out of the 55 patients who died: 13/42 (31%) died of local disease progression, while 23/42 (55%) died of distant disease progression and 6/42 (14%) of an unrelated cause.
Duration of Follow-Up, Treatment, and Patient Disposition
BRAF/MEKi, BRAF+MEK inhibitors; FU, follow-up.
Local progression or its complications were responsible for 38% of ATC-related deaths in patients treated without the neoadjuvant approach (5/10 of patients with stage IVB disease and 7/22 of those with stage IVC disease), as opposed to 25% (1/4) in the neoadjuvant group (p = 0.877).
Overall survival in DT versus DTP groups
Survival was significantly improved with DTP compared with DT alone: mOS was 9.0 months [confidence interval, CI, 4.5–13.5] in the DT group versus 17.0 months [CI, 11.9–22.1] in the DTP group (p = 0.037) (Fig. 3a). The 12- and 24-month Kaplan–Meier estimates of survival were 36.7% and 31.5% with DT alone, as opposed to 60.2% and 36.5% with DTP. When comparing OS by covariates, none of the analyzed characteristics, including prior neck surgery or radiotherapy for ATC, was found to be a significant predictive factor associated with OS (Supplementary Table S1). There was also no difference in OS whether DT was taken in pill form or dissolved (p = 0.303).
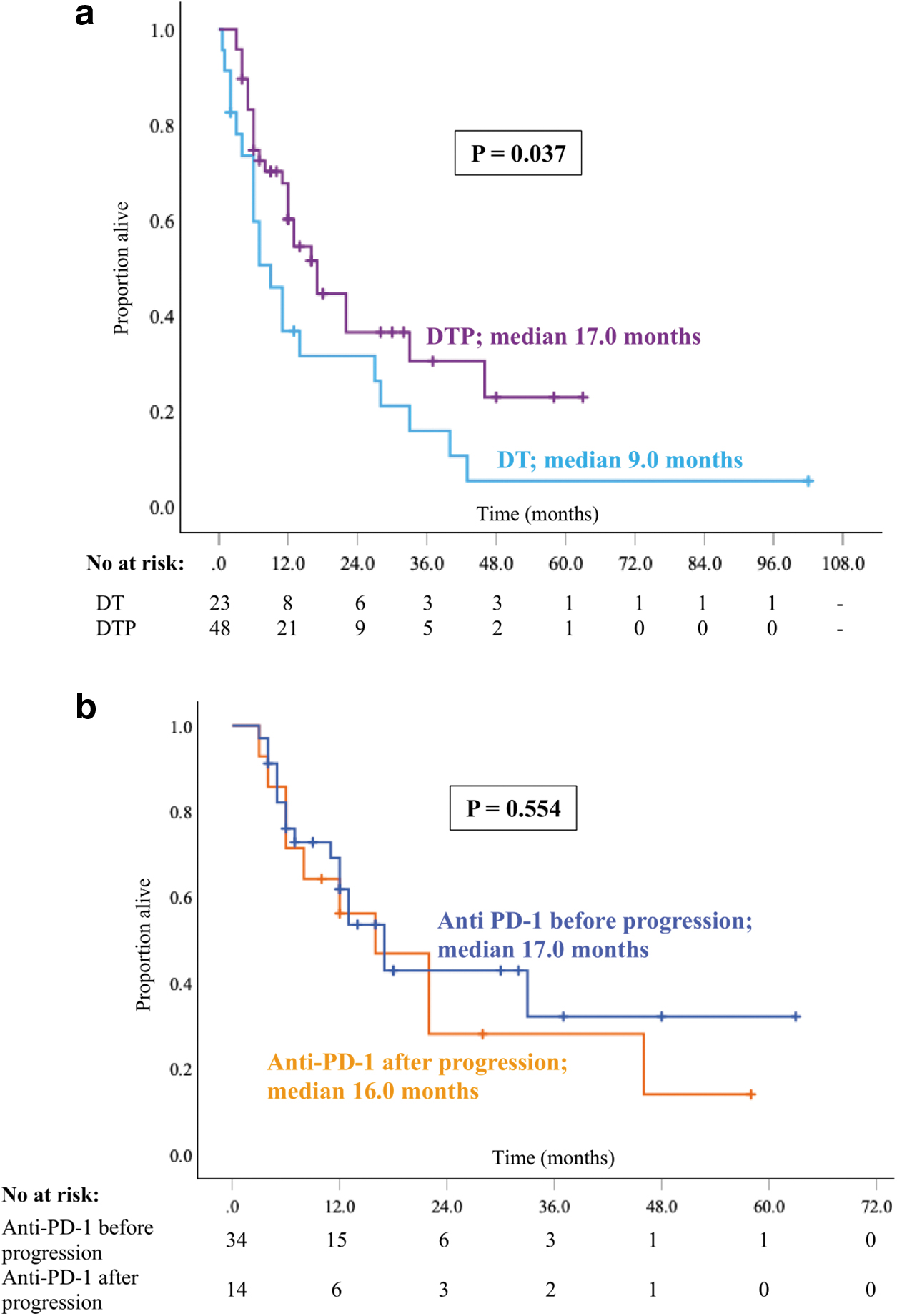
Kaplan–Meier plots for overall survival between DT and DTP groups (
In a subanalysis of the DTP group, there was no statistical difference between mOS from start of systemic therapy in the 14 patients in whom the anti-PD-1 ICI was added at progression on DT (16.0 months; [CI, 6.4–25.6]) and the 34 patients who were treated with upfront DTP (17.0 months; [CI, 0.24–33.8]); p = 0.523 (Fig. 3b).
Response and PFS with upfront DT versus DTP
Response to therapy as per RECIST v1.1 was assessed in all evaluable patients treated with upfront DT or DTP. Thirty patients treated with DT and 31 with DTP as initial systemic therapy regimens were evaluable for response. Patients initially treated with DT who had anti-PD-1 ICI added at progression and were evaluable for response were analyzed as part of the “upfront DT” group. ORR was similar between the two groups: 64.5% in patients treated with DT alone and 73.3% in patients treated with upfront DTP (p = 0.205) (Table 3 and Fig. 4). Median maximal change in target lesion size was also similar between DT and DTP as initial treatments: −48% (range, −100 to +64) and −55% (range, −100 to −22), respectively; p = 0.159.
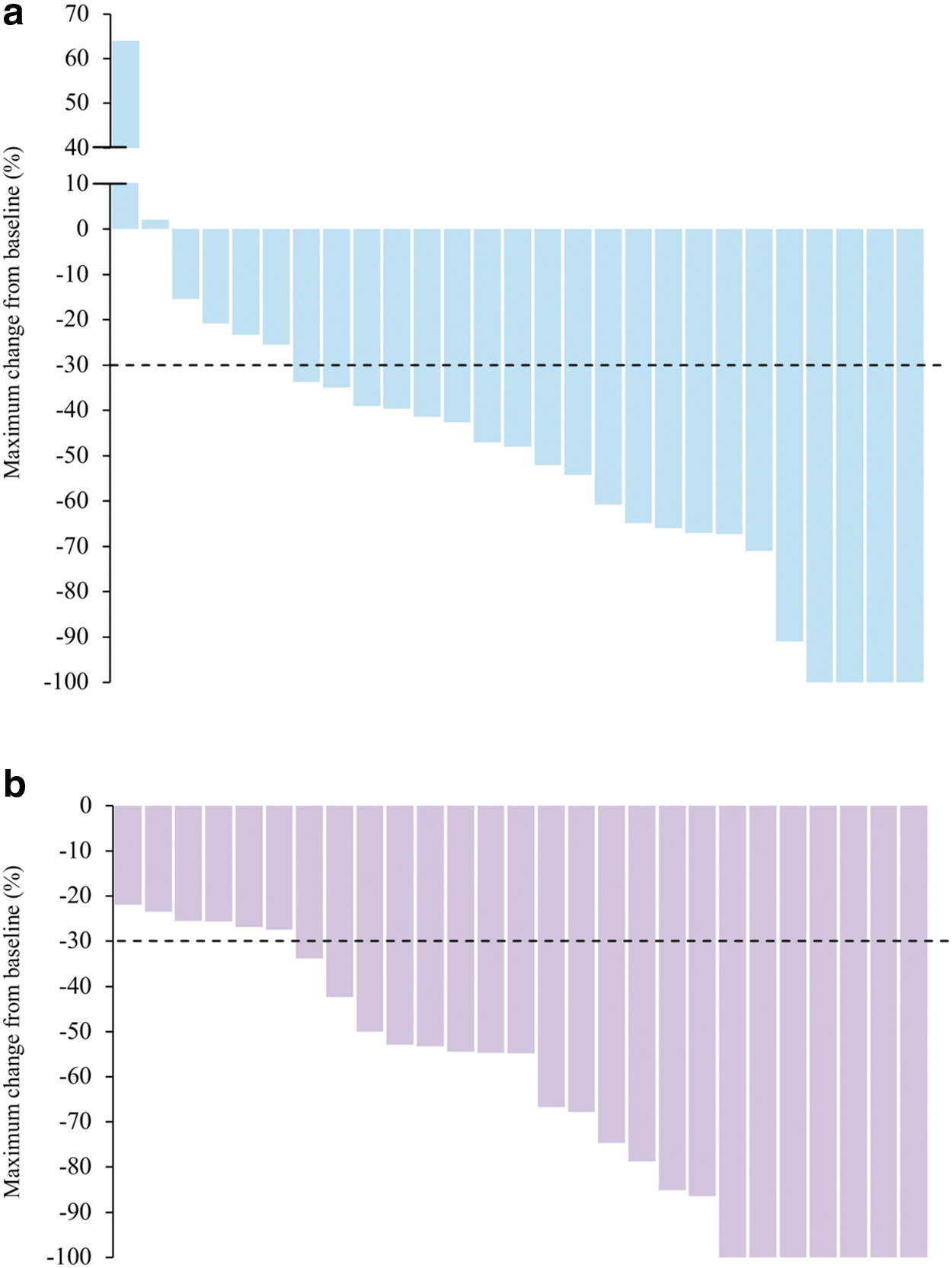
Best percentage change from baseline in sum of diameters of target lesions with DT
Initial Treatment Efficacy Outcomes
CI, confidence interval; CR, complete response; NE, nonevaluable; PD, progressive disease; PFS, progression-free survival; PR, partial response; SD, stable disease.
Median PFS (mPFS), on the contrary, was significantly longer with upfront DTP (11.0 months; [CI, 7.0–15.0]) compared with DT alone (4.0 months; [CI, 0.7–7.3]), p = 0.049 (Fig. 5).
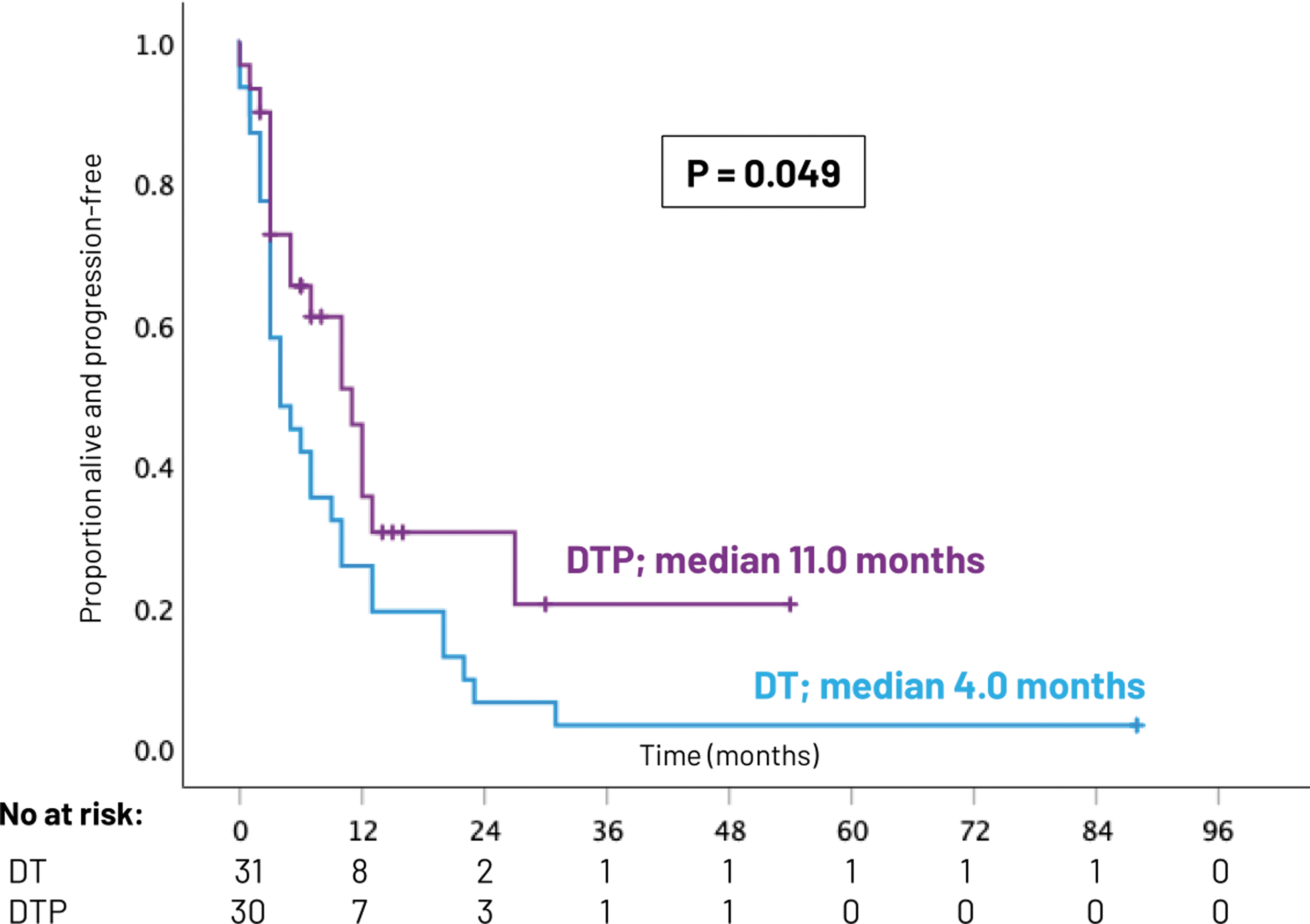
Kaplan–Meier plots for progression-free survival between DT and DTP as initial treatments.
Neoadjuvant approach
In the neoadjuvant group, median duration between initiation of systemic therapy and surgery was 3.0 months (range, 1.0–16.0). Patients treated with this approach had the longest survival, with an mOS of 63.0 months [CI, 15.5–110.5] and 12- and 24-month survival estimates of 80.7% and 74.5%, respectively (Fig. 6). There was no significant difference in OS between stage IVB and IVC patients treated with the neoadjuvant approach (mOS not reached [NR] for IVB, 63.0 months for IVC [p = 0.711]). mOS was longest with the neoadjuvant approach in patients with (M1) or without (M0) distant metastases at initiation of systemic therapy: 11.0 versus 16.0 versus 63.0 months in M1 and 6.0 versus 22.0 months versus NR in M0, for DT, DTP, and neoadjuvant, respectively.
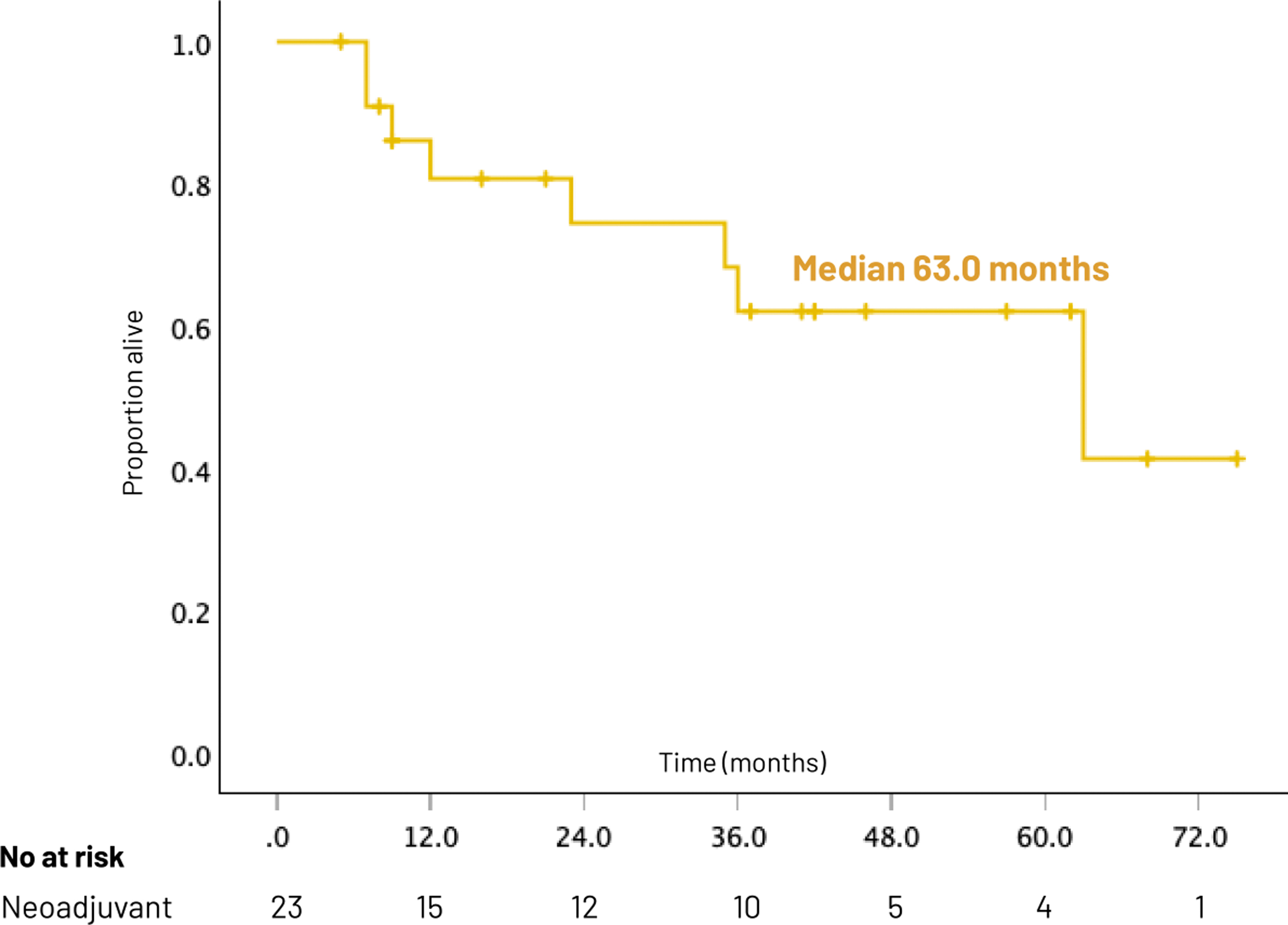
Kaplan–Meier plot for overall survival with the neoadjuvant approach.
Eleven out of the 22 patients (50%) with available pathological results had an ATC pathological complete response (pCR) following neoadjuvant therapy, defined as absence of residual ATC in the primary tumor on surgical specimen. OS was longer in patients who achieved an ATC pCR (mOS NR) compared with those who had not (mOS 23.0 months, [CI, 0.0–52.6]; p = 0.018) (Supplementary Fig. S1).
Of note, six patients were treated with neoadjuvant-intent DT (n = 3) or DTP (n = 3) but did not ultimately undergo surgery. Of these, five patients had an inadequate response with either disease progression or a short duration of response, which precluded surgery, and one patient (in DTP group) declined surgery. These patients were included in the DT and DTP groups, respectively, for analysis.
Neutrophil-to-lymphocyte ratio
In a recent publication, an NLR ≥5.05 was found to be associated with worse prognosis in ATC. 18 Similar findings were observed in our study, where NLR ≥5.05 was also an independent predictor for survival in the overall study population (Hazard ratio = 2.21; p = 0.014) in a multivariate Cox analysis including treatment strategy. As NLR is suggested to be a marker of systemic inflammation and may reflect increased neutrophil recruitment, we then looked at differences in OS between NLR <5.05 and ≥5.05 in patients treated with immunotherapy.
In the DTP cohort, OS was significantly longer in patients with an NLR <5.05 (n = 24, mOS 33.0 months) compared with those with an NLR ≥5.05 (n = 12, mOS 6.0 months); p = 0.002. This was, however, not the case in the neoadjuvant group, where OS was similar in both NLR ≥5.05 and NLR <5.05 subgroups (p = 0.898).
Treatment safety
Due to the retrospective nature of the study, there was no rigorous monitoring of AEs related to KI. Nevertheless, the triplet with DTP was overall safe. No grade 5 events were reported. ir-AEs occurred in 32% of patients who received at least one dose of ICI, the most frequent being hepatitis (9%), colitis (6%), and nephritis (4%) (Table 4).
Immune-Related Adverse Events in Patients Treated with an Anti-PD-1 Immune Checkpoint Inhibitor
DRESS, drug reaction with eosinophilia and systemic symptoms; Ir-AE, immune-related adverse event; STEMI, ST elevation myocardial infarction.
Discussion
This is the first clinical study comparing BRAF/MEKi alone to the BRAF/MEKi plus ICI triplet. Our results suggest that the addition of anti-PD-1 immunotherapy to BRAF/MEKi improves OS, as patients treated with DTP had an mOS of 17.0 months compared with 9.0 months with DT alone.
Our results are in accordance with both preclinical models 19 and clinical data. 14,20 In an immunocompetent murine model of BRAFm-ATC, combination of the BRAFi PLX4720 with an anti-PD-L1 achieved significantly more tumor shrinkage compared with either agent alone. After 2 weeks of treatment, tumor volume was three times smaller with the combination compared with BRAFi monotherapy. 19 Moreover, in a phase II trial looking at the combination of vemurafenib/cobimetinib plus atezolizumab in BRAFm-ATC, mOS had not been reached after a median follow-up of 33 months. 20 In this study, ORR was 72% and the 2-year OS estimate was 67%, which is significantly better than the 2-year survival of 32% with DT alone in the ROAR trial (p = 0.038). 3
Despite a remarkable initial response to BRAF/MEKi, most patients will eventually develop resistance mutations leading to treatment failure and disease progression. 10 In fact, inherent genomic instability of ATC cells allows them to rapidly acquire additional alterations to adapt to a changing environment. Resistance-conferring novel mutations include RAS and NF1/2 activating mutations, as well as c-MET overexpression. 10,21 These cannot be targeted with specific KI, adding to the therapeutic challenge. However, ATCs are favorable targets for ICIs as they are richly infiltrated by macrophages and T cells and express PD-L1 in up to 90% of cases. 12,22 –25 In addition, BRAF/MEKi enhance the response to immunotherapy by increasing T cell infiltration into the tumor microenvironment (TME) and upregulating PD-L1 expression on tumor cells, 19,26 which further supports the combination of these treatments.
Yet, not all patients respond equally to the addition of immunotherapy to BRAF/MEKi. A higher baseline NLR might be an easily accessible biomarker to predict poor responders to immunotherapy in ATC. In fact, data in other solid tumors have already suggested that an elevated NLR is associated with poorer outcomes in patients treated with ICI. 27 –29 However, further investigations are required to validate these observations in ATC.
In our study, mOS with DTP was significantly longer than mOS reported with DT alone in the ROAR trial, suggesting superiority of the triplet. However, survival outcomes in patients treated with DT in our study were shorter compared with the phase II trial 3 : 9.0 versus 14.5 months for mOS, and 4.0 versus 6.7 months for mPFS, respectively. Our results are more similar to other real-world studies of DT in BRAFm-ATC. 8,30 For instance, in a retrospective cohort of 17 patients with BRAFm-ATC treated with DT in the United Kingdom, 8 mOS was 6.9 months [CI, 2.46–NR] and mPFS was 4.7 months [CI, 1.4–7.8]. These differences could be due to the stricter eligibility criteria of clinical trials.
In fact, our study included all patients treated with DT regardless of their performance status and ability to swallow, whereas the phase II trial excluded patients who could not swallow the intact study drug and those with an Eastern Cooperative Oncology Group performance status of >2. Given that 26% of patients in the DT arm in our study received their oral targeted therapies through a gastric tube, one could argue that our patient population had more locally advanced disease, which could account for the shorter PFS and OS.
A subanalysis of the DTP group suggested that the addition of pembrolizumab at progression on DT leads to similar survival benefits compared with upfront DTP. However, this result should be interpreted with caution, given the small number (n = 14) of patients in whom pembrolizumab was added at progression. Tumor biology data in melanoma suggest that resistance to BRAF/MEKi results in an immunosuppressive TME driven by the reactivated MAPK pathway, leading to cross-resistance to immunotherapy. 31 Thus, tumors resistant to BRAF/MEKi might be less responsive to immunotherapy.
Clinical data in melanoma also support this observation, showing that patients who develop resistance to BRAF/MEKi respond worse to the addition of immunotherapy compared with when it is given upfront. 32 If we extrapolate these observations to ATC, addition of the anti-PD-1 earlier in the course of treatment might be preferable. Yet, in BRAFV600E -mutant melanoma, initial treatment with immunotherapy is favored over BRAF/MEKi as it offers more durable responses and greater OS benefits. 32 In addition, large randomized-controlled trials (RCTs) in melanoma led to variable results regarding benefits of triplet therapy compared with immunotherapy alone. 33 –35 Two out of the three conducted RCTs did not show statistically significant difference in PFS with the triplet compared with immunotherapy alone, such that upfront triplet therapy is no longer recommended. Thus, more prospective data are required in ATC to further investigate the benefits of triplet therapy.
Our study was possibly not powered to show a significant difference in survival between upfront DTP and addition of pembrolizumab to DT at progression. Nevertheless, based on our results and clinical experience, we advocate that when pembrolizumab cannot be obtained as part of the initial treatment in BRAFm-ATC, it should be added to DT at the time of progression rather than changing to another class of KI. This statement is further supported by data in BRAFV600E -mutated melanoma where patients in whom the BRAFi is continued beyond disease progression have a longer OS compared with those in whom the BRAFi is stopped. 36
The longest OS in our study was in the exploratory arm of patients treated with the neoadjuvant approach. mOS in this group was 63.0 months, which is especially remarkable given that 65% of patients had stage IVC disease. This is in line with another retrospective study our group recently published, in which OS and PFS were improved with BRAF-directed therapy followed by surgery, compared with BRAF-directed therapy alone, in a stage IVC-predominant cohort. 16 In fact, in this study of 57 BRAFm-ATC patients, those who were treated with the neoadjuvant approach had a 12-month OS of 93.6% and PFS of 84.4%, as opposed to 74.1% and 50%, respectively, in patients who had upfront surgery.
In addition, in the present study, mOS was similar between patients with stage IVB and IVC disease treated with the neoadjuvant approach. Therefore, our data support that in selected patients with stage IVC ATC, DTP, followed by surgery in those who become operable, might provide survival benefit. One hypothesis to explain this observation is that a non-negligible proportion of patients with stage IVC disease will die of locoregional progression rather than from progression of distant disease, despite systemic therapy. For instance, in our study, among the 18 stage IVC patients in the DTP group for whom the cause of death was known, 6 (33%) died from progression of local disease and/or its complications. This suggests that some patients with stage IVC ATC may benefit from resection of the primary tumor, especially in the presence of low-burden distant metastatic disease.
A prospective trial is currently ongoing to confirm the efficacy of the neoadjuvant approach and its impact on survival in patients with BRAFm-ATC (NCT04675710).
Moreover, as we have previously reported, this study confirms that an ATC pCR following neoadjuvant BRAF-directed therapy correlates significantly with OS. 16 Future research avenues should also explore if a pCR might affect subsequent treatment decisions, as it is increasingly the case in breast cancer. 37
One limitation of the neoadjuvant cohort is that only patients who achieved enough tumor shrinkage to undergo surgical resection were included. Nevertheless, most patients (79%) treated with neoadjuvant-intent BRAF-directed therapy seem to successfully undergo surgery, although the retrospective nature of this study limits the ability to accurately identify patients who were treated with intent for surgical resection but could not undergo surgery. The ongoing prospective trial (NCT04675710) will help us better understand how many patients fail the neoadjuvant approach and what are the potential predictive factors for the success of this strategy.
As previously mentioned, this study is an expanded cohort with additional patients and longer follow-up compared with our previous publications. 14,16 The present study includes patients diagnosed with BRAFm-ATC up to March 2023, while our previous publications' accrual stopped in October 201914 and December 2021. 16 In addition, previous publications included all BRAF/MEKi and all ICI immunotherapies, while we restricted our study groups to patients treated with DT and anti-PD-1 ICI. With regard to the neoadjuvant cohort, ours differs from Zhao et al. as we excluded patients who did not receive immunotherapy, those treated with anti-PD-L1 ICI, and those treated with BRAF/MEKi other than DT. Therefore, our groups are more comparable in terms of systemic therapy. In addition, the longer duration of follow-up in our study allowed us to reach a median for OS in the neoadjuvant group, while this was NR in the study by Zhao et al.
In patients with stage IVB disease, current guidelines favor upfront surgery followed by chemoradiation, or definitive-intent chemoradiation when the tumor is not resectable. 5 Yet, the phase II multicenter NRG/RTOG 0912 trial recently showed an mOS of only 8.6 months in patients with M0 disease treated with chemoradiation±surgery. 38 Although this is similar to the mOS in the DT group, survival was markedly longer in M0 patients treated with DTP (22 months) or the neoadjuvant approach (median NR) in our study, favoring these treatment strategies in stage IVB BRAFm-ATC.
One concern that arises when combining immunotherapy with KI is increased toxicity. Given the retrospective nature of this study, there was no systematic documentation of AEs and their grade. Based on record review, there were no deaths related to treatment toxicity, and documented ir-AEs were not more frequent than in previously published single-agent immunotherapy studies in thyroid cancer. 13,39 Yet, about one-third of patients experienced at least one ir-AE, including hepatitis, colitis, nephritis, encephalopathy, and pneumonitis. Hepatitis occurred in 9% of patients, which is non-negligible. Therefore, one should closely monitor potential toxicities, especially liver injury, when combining KI and ICIs.
The main limitation of this study is its retrospective design, which leads to inevitable selection bias. Another limitation is the small number of patients in whom pembrolizumab was added at progression, limiting the conclusions in this subgroup. PD-L1 score was not available for all patients, preventing conclusions regarding correlation between PD-L1 expression and response to ICI. Finally, since this was a chart review-based study, some ir-AEs may be underreported, and we could not obtain data regarding AEs to BRAF/MEKi or grading of AEs.
In conclusion, addition of an anti-PD-1 ICI to BRAF/MEKi in BRAFm-ATC appears to significantly improve OS and PFS. Use of pembrolizumab as a salvage therapy at progression on BRAF/MEKi may also provide survival benefits, although further data are needed to support this observation. In selected cases, DTP used in a neoadjuvant setting, followed by surgery, has shown further improvement in survival outcomes in patients who became operable. Of note, current ATA guidelines 5 only recommend immunotherapy in stage IVC ATC, as a first-line single-agent therapy in tumors with no targetable alteration and high PD-L1 expression, or as a later line therapy within a clinical trial.
However, given the significant survival benefits with the combination of BRAF/MEKi plus immunotherapy shown in this study as well as the prospective phase II trial of vemurafenib/cobimetinib plus atezolizumab, 20 coupled with acceptable toxicity profiles, we advocate that this triplet should be considered in patients with locally advanced and/or inoperable stage IVB disease and those with stage IVC BRAFm-ATC, followed by surgery for resectable primary tumors, ideally within a clinical trial. Moreover, in patients who progress on BRAF/MEKi, we recommend the addition of pembrolizumab rather than switching therapy.
Footnotes
Authors' Contributions
S.H.: study conceptualization, data collection, analysis, writing original draft, and review and editing. M.E.C. and P.C.I.: study conceptualization and article review and editing. M.K.G.-M.: review of imaging for RECIST measurements. A.M., R.D., M.E.Z., J.R.W., and N.L.B.: article review and editing.
Author Disclosure Statement
R.D. has received research grant funding from Eisai, Merck, Exelixis, and AstraZeneca and has participated in advisory boards for Exelixis and Bayer. N.L.B. has received research grant funding from GSK, has received consulting fees from Eisai, and has participated in advisory boards for Exelixis. M.E.Z. has received research grant funding from Merck and Eli Lily. M.E.C. has received research grant funding from Genentech and Merck and consulting fees from Exelixis and Bayer. All other authors have no conflicts of interest to declare.
Funding Information
No funding was received for this work.
Supplementary Material
Supplementary Figure S1
Supplementary Table S1