
Abstract
Background:
Agranulocytosis is a rare antithyroid drug treatment (ATD) side effect seen in children suffering from Graves’ disease (GD). Neutropenia is a recognized adverse event associated with ATD but has also been reported as pre-treatment neutropenia in GD.
Methods:
We performed a retrospective cohort study to analyze the longitudinal clinical and biochemical data of 161 pediatric patients with GD who received either methimazole (MMI) or carbimazole (CBZ) as ATD. The inclusion criteria were elevated free thyroxine (fT4 >25 pmol/L), suppressed thyrotropin (TSH <0.05 mlU/mL), and elevated thyrotropin receptor antibodies (TSHRAbs >2.5 IU/L). Absolute neutrophil count (ANC) was used to define neutropenia (ANC <1800/µL) and agranulocytosis (ANC <500/µL).
Results:
Nine of the 161 patients had neutropenia at diagnosis (ANC: 1348/µL ± 250) without further deterioration under ATD. In this subgroup, we found higher levels of free triiodothyronine (fT3: 31.45 pmol/L ± 3.99) at diagnosis in comparison with those who developed neutropenia (26.29 pmol/L ± 12.96; p = 0.07) and those without neutropenia before and during therapy (23.12 pmol/L ± 13.7; p = 0.003). Thirty-eight patients (23.6%) became neutropenic (ANC: 1479/µL ± 262) while receiving ATD. Neutropenia occurred after a mean of 551.8 (range: 10–1376) days, mostly without further deterioration. Two of these 38 patients developed agranulocytosis and underwent emergency thyroidectomy. The patients with neutropenia were significantly younger (p = 0.031). Neutropenia occurred significantly more often in patients receiving CBZ (50%; n = 20/40) than in those receiving MMI (16.5%; n = 18/110; p = 0.001). The minimum ANC was significantly lower in the CBZ (1971/µL ± 1008) than in the MMI group (2546 ± 959); p = 0.004.
Conclusions:
Neutropenia occurred significantly more often under CBZ than MMI. As this is potentially due to higher immunogenicity, we suggest that children with GD should be treated with MMI. Frequent measurements of ANC may be needed to detect severe agranulocytosis, although low pre-treatment ANC may not necessarily be a contraindication to ATD treatment. Young age may be potentially associated with an increased risk of reduced ANC. Further investigation is necessary to fully understand risk factors for neutropenia in children with GD.
Introduction
Graves’ disease (GD) is a rare systemic autoimmune disease seen in children and adolescents, with an incidence of 4.6/100,000 per year. 1 Children younger than 5 years are only rarely affected. 1 The girl-to-boy incidence rate ratio is about 4:1. 2 Autoimmune thyrotropin receptor antibodies (TSHRAb) induce excessive thyroid hormone secretion, escaping pituitary control. 3 Antithyroid drugs (ATD) are used to treat GD for symptom control but it also affects the immune process in ways that remain to be elucidated. The recommended duration of ATD treatment is longer in children (3 years) than adults. 2,4 The reason for this is that children are at a higher risk of recurrence after discontinuation, and prolonged therapy makes lasting remission of GD more likely. Whether “dose titration” (DT) or “block and replace” (BaR) is the better treatment regime remains a point of discussion. The European guideline recommends DT as the preferred means of ATD treatment in most cases. 2
Neutropenia is a recognized adverse event associated with ATD. However, it is also described as pre-treatment neutropenia in autoimmune hyperthyroidism in adults and children, similarly affecting 14%–16%. 5 –8 This drug-associated side effect occurs in a dose-dependent manner, usually within the first 3 months of treatment, and may develop suddenly or in a gradual manner. 9 However, case reports describing severe neutropenia after some years of ATD treatments have been published. 10,11 A Japanese study including patients aged 7–81 years, demonstrated that agranulocytosis is more common in patients in their 40s and 50s. 9 There is a paucity of research into pediatric cohorts on this topic, particularly in Caucasians. Different definitions of neutropenia in the published studies on this topic restrict the comparability. While some authors define neutropenia as absolute neutrophil count (ANC) < 2000/µL, 4 others use a cut-off for neutropenia of ANC < 1500/µL. 6 We define normal ANC as > 1800/µL, as do most laboratories involved in the analysis of hematological parameters of our cohort. This definition is based on the 90% confidence interval (CI) of a reference population of healthy individuals. We deliberately chose this cut-off for our analysis to detect all abnormal ANC measurements. Even though propylthiouracil (PTU) is rarely used in pediatrics, most previous retrospective studies examine side effects of PTU compared with methimazole (MMI) and carbimazole (CBZ). 12 This is the first study comparing the effects of MMI and CBZ treatment on the ANC in children. Furthermore, we wanted to detect potential risk factors for neutropenia in pediatric patients with GD.
Materials and Methods
We analyzed longitudinal data from 161 patients diagnosed with GD between 2004 and 2021. We used patients’ medical records from three tertiary care centers (Divisions of Pediatric Endocrinology, University Children’s Hospitals in Bonn, Erlangen, and Duesseldorf, Germany). Patients received ATD therapy with MMI or CBZ in a retrospective longitudinal study.
Firstly, we screened the hospital computer database for diagnosis-related group (DRG) coding of hyperthyreosis and autoimmunthyreoiditis in all patients who had been treated in the department of pediatric endocrinology of the three care centers between 2004 and 2021. We matched these results with a screening of the central laboratory database of the hospitals for all patients younger than 18 years who had measurements of a thyrotropin stimulation hormone(TSH) < 0.01 IU/L during this period. The innclusion criteria were elevated free thyroxine (fT4) (normal range [NR]: 10–25 pmol/L), completely suppressed TSH (NR: 0.5–4.5 mIU/L), and elevated thyrotropin receptor antibodies (TSHRAb > 2.5 IU/L) at diagnosis. Neutropenia was defined by ANC < 1800/µL, and agranulocytosis by ANC < 500/µL. We excluded patients with hyperthyroidism caused by Hashimoto disease. The process of retrospective analysis was evaluated and approved by the local institutional review boards or ethics committees (IRB Bonn University, Ref. no 256/19). Both patients and caregivers signed informed consent forms. V.S., N.C., H.D., M.R., and C.R. collected patients’ data from the patients’ medical records in the three tertiary care centers. As some of these patients continued treatment after the diagnosis and treatment initiation at independent physicians near Bonn and Duesseldorf, M.R. collected their follow-up data in these private practices. Our cohort comprises patients treated in Erlangen (60.3%), Bonn (23.0%), and Duesseldorf (16.7%). The mean follow-up duration was 24.3 months (range: 4–110 months).
In our primary analysis, we compared three groups: patients without neutropenia, patients with neutropenia at diagnosis, and patients with neutropenia under ATD. In a secondary subgroup analysis of patients who had neutropenia during ATD treatment, we compared those receiving CBZ to those receiving MMI. Two cases of severe agranulocytosis were described in detail.
Comparisons of binary variables (e.g., sex) were examined using a binomial test. Comparisons of continuous variables (e.g., maximal dose) were examined using an unpaired Welch’s t-test. The chi-squared is used to compare categorical variables. For example, to assess if the use of a certain drug in the therapy was associated with a clinic. The Pearson correlation coefficient is used to assess the correlation between two continuous variables. For example, to analyze a possible correlation between the age of a patient and the minimal ANC or the ANC and free triiodothyronine (fT3). Statistical analysis was performed using “R”, version 4.2.3, R Core Team (2023), R Foundation for Statistical Computing, Vienna, Austria. URL https://www.R-project.org/. We defined p < 0.05 as statistically significant.
The treatment duration until patients became neutropenic varied substantially between 10 and 1376 days after diagnosis. This makes it difficult to examine whether the cumulative dose is a risk factor for neutropenia by comparing with the neutropenic group (i.e., patients who became neutropenic under treatment) and the non-neutropenic group (patients who never became neutropenic). Therefore, we examined four different intervals, defined as the time point until 25%, 50%, 75%, and 100% of the patients became neutropenic. For each of those time points, we compared the cumulative dose between the neutropenic group and the non-neutropenic group.
Results
We started the data collection by screening the documented visits and blood results of all 171 eligible patients (see Fig. 1). We then collected data from various predefined time-points: the time of diagnosis, three visits in the first year of treatment (V1a: 1 month, V1b: 3–6 months, V1c: 9–12 months), one after 2 years (V2), one after 3 years (V3), and the last documented visit (V4). We always included the visit with the lowest ANC. In the patients who became neutropenic, we always included the visit with the first occurrence of neutropenia. Ten patients were excluded from the ANC analysis, as they were lost to follow-up (6 patients) or pre-treatment ANC levels were missing (4 patients). In total, 161 patients were included and analyzed. For all 161 patients, we collected information about age, sex, ethnical background, treatment regime, type of ATD, dose of ATD, TSH, and fT4 in all analyzed visits. The ANC was missing in V3 and V4 in 78 patients in the cohort because it was not common in the three care centers to check the ANC for more than 3 years after the start of ATD. For the detailed ANC progress of two cases of agranulocytosis, we collected all available data of ANC results up to the final surgical treatment (Fig. 4). fT3 is missing from one visit in 20 patients, and TSHRAb was not available from one visit in 32 patients. In each of these cases, a blood check was initiated by the patient’s primary pediatrician. Some data points are missing owing to circumstances where laboratories did not offer to measure these parameters and/or they were not covered by health insurance.
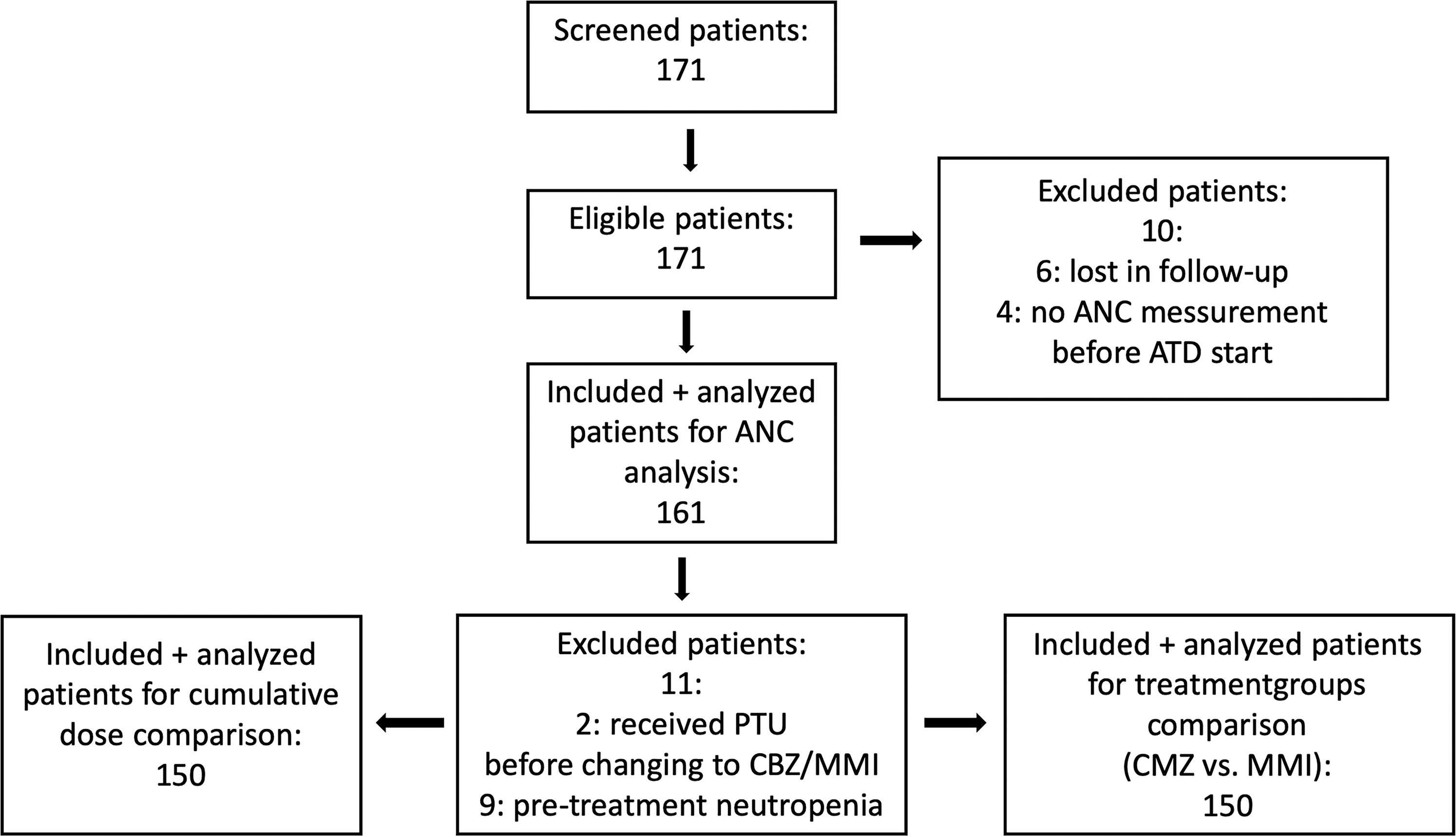
Flow diagram of the participants with number of individuals at each stage of the study.
The mean age of the 161 patients (129 female, 32 male) was 11.8 years (±3.6; range: 1.4–17.8). Eighty-three percent were Caucasian, and 17% belonged to other ethnic groups, mainly Turkish or Syrian. All patients were nonsmokers. Two patients initially received PTU before changing to CBZ or MMI and were excluded from the comparison with the treatment groups (CBZ vs. MMI) and cumulative dose. In contrast to other European countries, both ATDs (CBZ and MMI) are always available in Germany. Our analysis shows significant differences in the type of ATD prescribed between the three care centers (use of MMI: 78%, 54%, and 88%, p = 0.003). Furthermore, we found significant differences in the choice of treatment regime between the three care centers (use of BaR: 71%, 67%, and 30%, p = 0.001). All patients started with DT after diagnosis of GD. In total, 102 patients (63%) changed to BaR after a mean of 4.7 months (range: 0.5–45.0 months).
Nine patients (5.6%) had pre-treatment neutropenia at the time of diagnosis (ANC: 1348/µL ± 250; 2 < 1800/µL, 6 < 1500/µL, 1 < 1000/µL, 0 < 500/µL). All of them received ATD treatment without further deterioration (Fig. 2). In these patients, we found significantly higher fT3 level (31.45 pmol/L ± 3.99) than in those who developed neutropenia under ATD (26.29 pmol/L ± 12.96; p = 0.070) and in those without neutropenia (23.12 pmol/L ± 13.7; p = 0.003) during therapy (Table 1). However, fT3 did not correlate with the ANC in the whole cohort (Pearson correlation coefficient: −0.115; p value: 0.357). These nine patients were excluded from the comparison of CBZ versus MMI group and from the cumulative dose analysis.
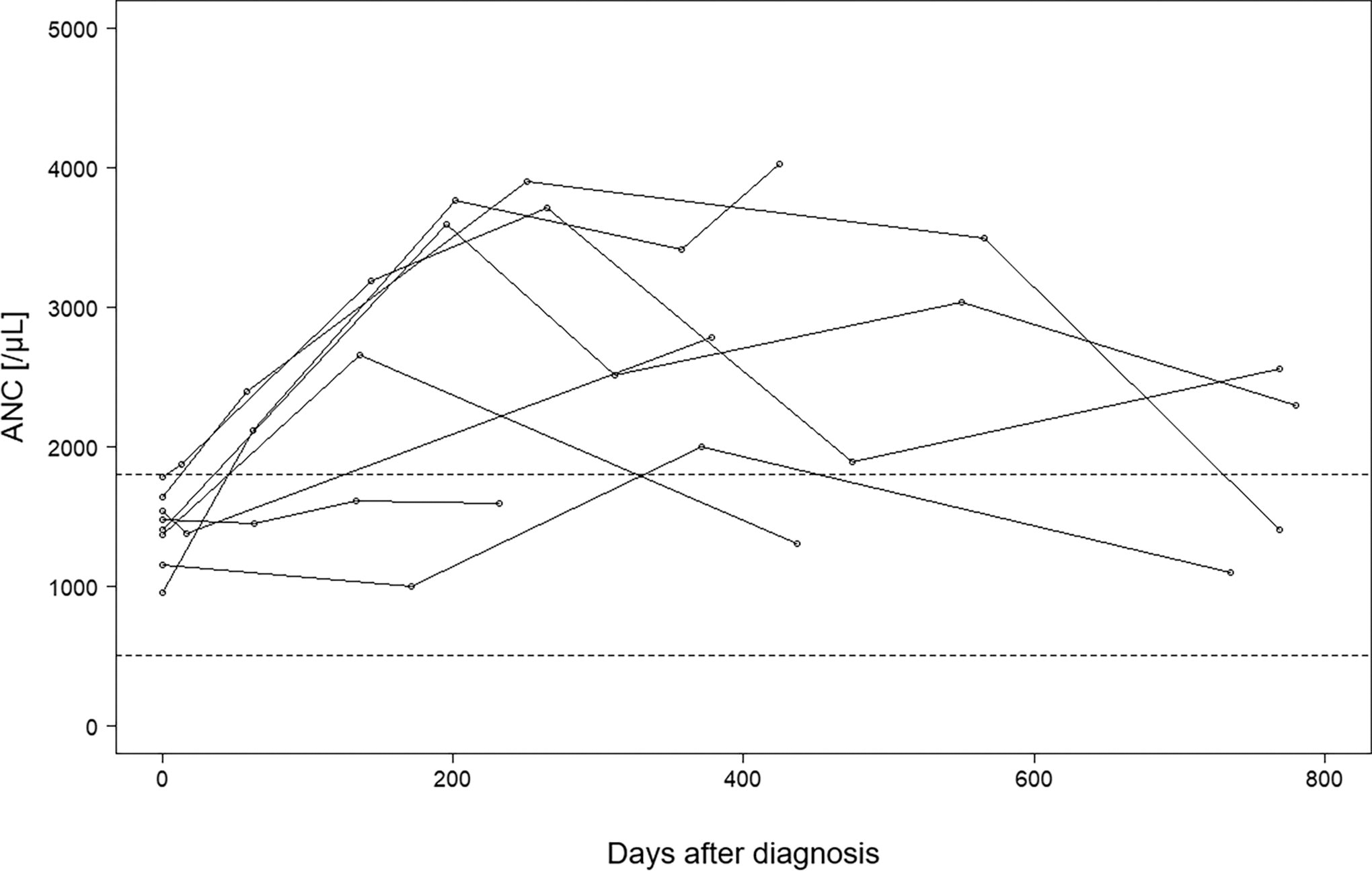
Progression of the absolute neutrophil count (ANC) in the 9 patients with neutropenia before treatment.
Characteristics and Comparison of Patients with Pre-Treatment Neutropenia (A), Neutropenia under ATD (B), without Neutropenia (C)
fT4, fT3, TSHRAb levels at diagnosis.
Significant results (p < 0.05) in boldface.
BaR, block and replace; fT3, fT4, free thyroxine; Max. Dose, maximal dose of ATD (before neutropenia occurred); Min. ANC, minimum absolute neutrophil count; TR, titration regime; TSHRAb, thyrotropin receptor antibodies.
Thirty-eight patients (23.6%) developed neutropenia while receiving ATD (Fig. 3). Neutropenia occurred after a mean of 551.8 days (range: 10–1376) after diagnosis. The majority of these exhibited only mild neutropenia (min. ANC: 1468 ± 295.39; 20 < 1800/µL, 16 < 1500/µL, 0 < 1000/µL, 2 < 500/µL). All patients continued on ATD, and only 1 patient had a dose reduction of ATD. We analyzed the difference between ANC at the onset of neutropenia and at the last ANC measurement for each patient with neutropenia and found no significant difference (p = 0.9).

Progression of the absolute neutrophil count (ANC) in 36 patients suffering neutropenia under ATD treatment without developing agranulocytosis.
Only 2 patients developed agranulocytosis under ATD and needed an emergency thyroidectomy. As both patients had no clinical symptoms of agranulocytosis, low ANC was detected by routine ANC testing. Figure 4 demonstrates their ANC progress. Patient 1, an 11-year-old German girl, developed neutropenia (1000/µL) 3 weeks after the start of ATD with further deterioration to severe agranulocytosis (40/µL) 1 week later. Agranulocytosis was associated with a high maximal dose of CBZ (1.8 mg/kg/d), which had to be increased to this level because of severe thyrotoxicosis (fT3 > 30 pg/mL [46 pmol/L]; fT4 > 8 ng/dL [12.9 pmol/L)], both above the assays range) and TSHRAb 101.20 IU/L.
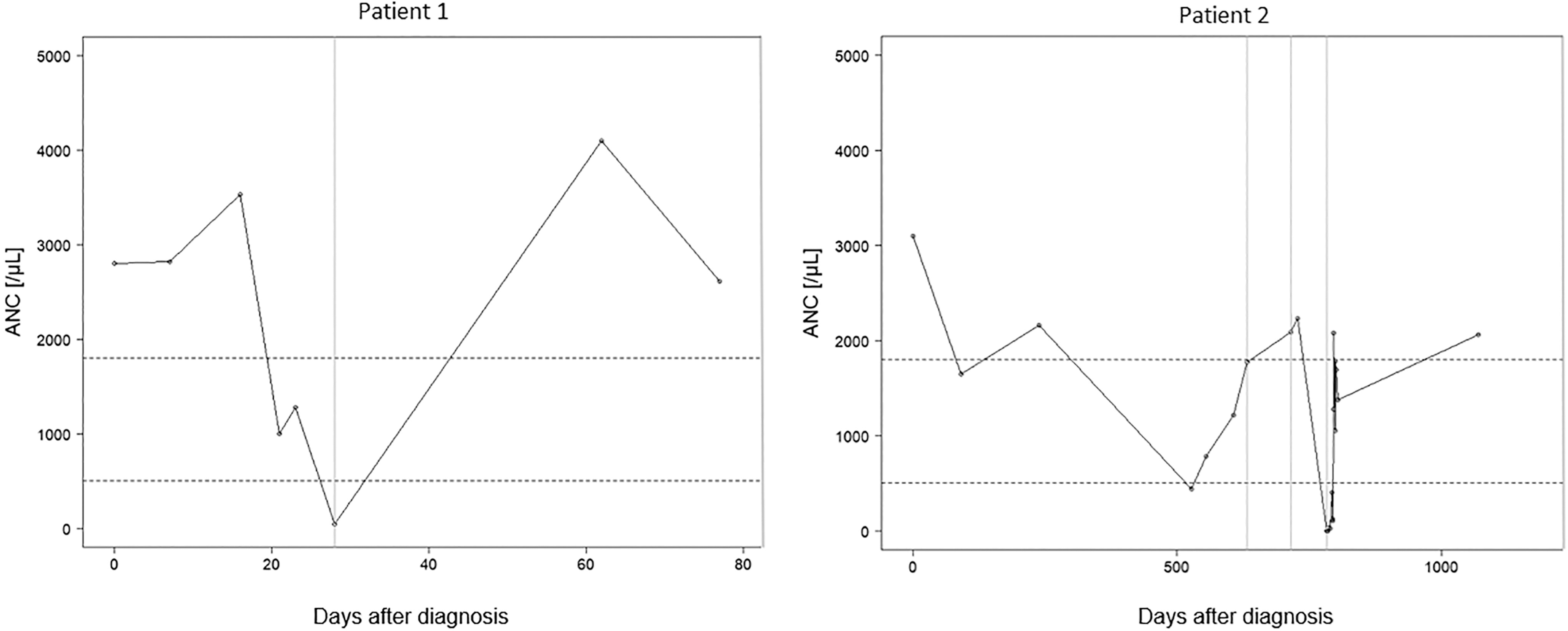
Progression of the absolute neutrophil count (ANC) in patients 1 and 2. Vertical lines: Patient 1: day 28: ATD stopped; patient 2: day 632: ATD stopped, day 715: ATD re-started, day 784: ATD stopped.
Patient 2, a 10-year-old German girl with mild hyperthyroidism (fT3 21,27 pmol/L; fT4 32,1 pmol/L) and low TSHRAb (4,9 IU/l), receiving maximal 0.47 mg/kg/d MMI and BaR treatment with 1.13 µg/kg levothyroxine, initially developed mild neutropenia (1645/µL) 90 days after diagnosis with spontaneous normalization under the same ATD dose. Day 527, mild agranulocytosis (440/µL) was detected. Consequently, the ATD dose was reduced (to 0.18 mg/kg/d). Her ANC subsequently increased up to 1770/µL (Fig. 4, day 632). Three months later, after an attempt to discontinue the medication (euthyroid, TSHRAb negative), she had a hyperthyroid relapse, which recommenced on MMI (0.37 mg/kg), and went on to develop severe agranulocytosis 69 days later (ANC 0/µL). Granulocyte-Colony Stimulating Factor (G-CSF) was administered, and an emergency thyroidectomy was performed.
Patients with neutropenia were significantly younger than the non-neutropenic group (10.7 ± 3.3; range: 3.8–16.0 vs. 12.2 ± 3.7, range; 1.4–17.8 years; p = 0.03). No statistically significant relationship was demonstrated between neutropenia and sex, race, fT3, fT4, or TSHRAb concentration at diagnosis, treatment regime (BaR/DT) or maximal daily dose (Table 1).
Neutropenia occurred significantly more frequently in patients on CBZ (50%; n = 20/40, 95% CI: 0.345–0.655 [0.500 ± 0.155]) than in those rece iving MMI [16.5%; n = 18/110, 95% CI: 0.095–0.233 [0.164 ± 0.069]); (p = 0.0008). Minimum ANC (1971 ± 1008/µL) was significantly lower in the CBZ group than in the MMI (2546 ± 959/µL) group (p = 0.004). There was no difference in sex, age, race, fT3, fT4, or TSHRAb concentration at diagnosis between the two treatment groups (Table 2). Neither the maximum daily dose (0.52 vs. 0.51 mg/kg, p = 0.98) nor the daily (0.62 vs. 0.29 mg/kg, p = 0.19) or cumulative dose (243.3 vs. 182.9 mg/kg, p = 0.58) before neutropenia differed between the CBZ and the MMI group.
Patient Characteristics according to Treatment Group
Patients with pre-treatment neutropenia 2 treatment were excluded.
Comparison with group A to group B (t-test).
Comparison with one subgroup (A, B) to the whole group (A + B) (binominal test).
Significant results (p < 0.05) in boldface.
ANC, Absolute neutrophil count; ATD, antithyroid drug treatment; fT3, fT4, free thyroxine; TSHRAb, thyrotropin receptor antibodies.
At all four defined time points, the cumulative dose in the neutropenic group was numerically higher than in the non-neutropenic group. However, no statistical significance was found, likely owing to a limited number of patients and high variance (Table 3).
Cumulative Dose of Patients with Neutropenia under ATD Versus Patients without Neutropenia
Cumulative dose (mean ± SD) of patients with neutropenia under ATD (B) and patients without neutropenia (C) at four defined time points when 25%, 50%, 75%, or 100% of the patient with neutropenia became neutropenic.
Discussion
Our retrospective study is relatively large given the topic of pediatric GD, allowing us to present important new insights on this topic. Our results confirm that agranulocytosis (ANC < 500/µL) is a rare adverse event associated with ATD in children suffering from GD. Only 2/161 (1.2%) patients developed severe neutropenia, thus making it necessary to change their treatment regime.
Studies on adult patients with GD report high ATD doses as a predictor for neutropenia. 13 In contrast, Watanabe et al. could not identify specific risk factors in a study of 55 adult patients with GD with agranulocytosis. 14 The avoidance of high doses is in accordance with the recently published guidelines for GD treatment in children by Mooji et al. 2 Studies with Caucasian pediatric patients with GD and neutropenia are infrequent, and different definitions of neutropenia complicate comparability. In a Japanese cohort with 18 patients with GD of age <15 years, agranulocytosis occurred dose-dependently. 15 In contrast, in our cohort, maximum dose and daily dose at onset of neutropenia were not associated with an increased risk for neutropenia and were not significantly different between the treatment groups. However, patient 1 received the highest maximal dose of the patient cohort, suggesting that a very high dose of ATD might be associated with agranulocytosis. In contrast, patient 2 demonstrated a completely different risk profile (less severe, lower ATD dose, BaR treatment) but developed severe agranulocytosis under relapse treatment.
An important question we wanted to answer by our analysis was how often ANC should be measured in patients under ATD to detect severe neutropenia. There is no clear recommendation in the European guidelines. 2 Existing data refers mainly to adult patients: Nakamura et al. demonstrated in 754 adult patients with GD and agranulocytosis that 52.6% had normal ANCs even 2 weeks before agranulocytosis occurred. 9 In adults, neutropenia mainly occurs within the first 3 months, 14 but case reports of late onset of severe neutropenia have also been published. 10 In contrast, in our pediatric cohort, neutropenia occurred on average 552 days after ATD start, ranging from 10 to 1376 days. Therefore, no definitive conclusion can be drawn, and it remains debatable as to how often ANC should be measured. In our study, 38 patients developed neutropenia under ATD. In only two of those cases did neutropenia progress into a severe agranulocytosis. For 35 of the other 36 neutropenic patients, the treatment regime remained unchanged, with the dose being reduced in only 1 patient. However, neutropenia made parents more attentive to infection symptoms, and physicians checked ANC again. Even moderate neutropenia increases the risk of complication when the child gets an infection. In Figure 3, we demonstrate that under ATD, the ANC count did not show further significant reduction in these 36 patients (p = 0.9). Both patients who developed severe agranulocytosis had mild neutropenia prior to this. We conclude that the risk for agranulocytosis is still relatively low, as only 1% of our cohort and only 5% of the patients with neutropenia developed agranulocytosis. However, this finding should be taken into account for further recommendations in the next guideline.
The recommendation for a longer duration of ATD therapy over several years is specific to pediatric patients. To the best of our knowledge, this is the first study to analyze whether the cumulative dose is a risk factor for neutropenia. At all points in time, the cumulative doses were higher in the neutropenic than in the non-neutropenic group. Statistical tests did not show significant effects for the subsequent time points. However, the statistical power of the tests is low owing to the small number of patients and high variability. We therefore recommend further investigation into this topic in larger cohorts. Given that long-term ATD treatment is recommended in pediatric patients, 2,4 identifying potential negative effects of the cumulative ATD dose would be very important, given the risk of neutropenia and other side effects.
Our study aimed to examine known risk factors for the occurrence of ANC with respect to their validity in pediatric patients and to detect further correlations between the given parameters and neutropenia. Aggarwal et al. found high fT3 levels to be the only independent predictor for pre-treatment neutropenia in adults with GD. 5 Our data confirm these findings for pediatric patients. Furthermore, as the neutropenic patients were significantly younger than the non-neutropenic patients, we suggest that a young age seems to be associated with neutropenia in GD. Coincidental unidentified viral infections cannot be ruled out and may have an effect on the results, as they are more common in younger children. However, both agranulocytic patients were younger than the average non-neutropenic patients. These findings are not described in the literature as far as most of the studies with pediatric patients had older patients than our cohort (e.g., Litao et al., median range: 14.7 [0.02–19.2] years). 6 We recommend frequent ANC tests, especially in young patients and those with high fT3 levels at diagnosis.
Our study demonstrates that while agranulocytosis is rare, neutropenia is a common side effect of ATD treatment. However, once neutropenia is detected, ANC did not decrease significantly during follow-up.
In our cohort, no patients with pre-treatment neutropenia went on to develop agranulocytosis during ATD. Litao et al. reported similar findings in children with GD and pre-treatment neutropenia. 6 We therefore recommend that neutropenia at diagnosis should not be a contraindication for ATD use. Furthermore, our data show that agranulocytosis is a rare side effect of ATD treatment. Therefore, we recommend that mild to medium neutropenia (>1000 to <1800/µL) under ATD is not an indication for switching to another treatment regime. The most critical measure to prevent severe adverse events resulting from agranulocytosis might be informing patients and families about symptoms and giving indications for emergency medical consultation.
This is the first study comparing ANC under CBZ versus MMI use. As MMI is the active metabolite of CBZ, a similar side effect profile of these drugs is expected. However, a favorable lower dose per kilogram is sufficient for the active metabolite. While the American Thyroid Association (ATA) Guidelines (2016) recommends both ATD agents for children with a similar dose range of 0.2–0.5 mg/kg/day, 16 the European Thyroid Association recommends an initial lower dose of 0.15–0.5 mg/kg/day MMI, versus 0.25–0.75 mg/kg/day CBZ. 2 In our cohort, the daily dose did not differ between the treatment groups, but those patients receiving CBZ developed neutropenia significantly more often than those treated with MMI. We advocate for the use of MMI over CBZ (if available), although this finding of our study needs to be confirmed in further studies.
The complex interplay between pathophysiology and pharmacodynamics causing neutropenia in patients with GD, from immune-mediated to dose-dependent drug-induced autoimmune phenomena, is still a point of investigation. 17,18 Studies on non-chemotherapy idiosyncratic drug-induced neutropenia (IDIN) are rare, and mouse models are not available. 18 Different human leukocyte antigen types (HLA) were identified as genetic risk factors for agranulocytosis under ATD. 19 In 1985, Weitzman et al. described anti-neutrophil antibodies in GD. 20 Bux et al. found CBZ-specific antibodies against the neutrophil-specific Fcg receptor IIIb (Fcg RIIIb, CD16b), erythrocytes and the broadly expressed platelet endothelial cell adhesion molecule 1 (platelet endothelial cell adhesion molecule 1 [PECAM-1], CD31) in adult patients with GD suffering anemia. 21 Interestingly, the same study group found that in patients with drug-induced immune thrombocytopenia, these antibodies were CBZ-specific and did not bind to CBZ metabolites such as MMI. 22 Thus, CBZ seems to have a higher immunogenicity than MMI. These findings could explain why CBZ carries a higher risk for neutropenia than MMI. Pharmacologically, a higher plasma level of ATD could explain a higher rate of side effects. We could not find any studies on how pediatric patients metabolize CBZ and MMI. However, the pharmacokinetics and pharmacodynamics of ATD metabolism may differ between children and adults, as this is known for many other drugs. 23
Our study has a clinical retrospective study design with therefore some limitations. We cannot exclude a referral bias. It is neither double-blind, nor randomized. Furthermore, the individual clinical histories are heterogeneous with great variation in follow-up period. The decision for the type of ATD and the treatment regime was not structural but individualized. Because of the retrospective study design, some data were missing. We cannot rule out possible confounders, such as viral infections or vaccinations, influencing our results, according to the ANC. Although we examined a relatively large pediatric group in total, the number of patients for the subgroup analysis became rather small.
Given the fact that data on pediatric patients on this topic are rare, we believe that our study adds important new insights. Because of our findings that neutropenia occurs more often under CBZ than MMI, we recommend the use of MMI rather than CBZ in pediatric patients with GD. Attention to ANC must be kept even after the first year of treatment and under relapse treatment. Repeated parental and patient education on side effects is crucial to ensure patient safety. Further investigations are necessary to identify risk factors for neutropenia in children with GD under ATD treatment.
Footnotes
Acknowledgment
The authors thank Walburga Vorhoff (independent physician, Duesseldorf), Jutta Wetter (independent physician, Troisdorf), and Beate Karges (Children’s Hospital Stolberg) for the provision of patients’ medical records.
Author Contribution Statement
V.S., N.C., H.D., M.R., and C.R. collected the patients’ data. V.S., B.G., and J.G. analyzed the data. V.S. and B.G. wrote the article. All authors contributed to the article and approved the submitted version.
Author Disclosure Statement
All authors have nothing to disclose and no conflict of interest.
Funding Information
No funding was received for this article.