
Abstract
Background:
Active surveillance (AS) of papillary thyroid microcarcinomas (PTMC) is emerging as an alternative to immediate surgery. While thermal ablation has also shown promise for low-risk PTMC, it has not been prospectively studied in patients appropriate for AS. This study aimed to evaluate the efficacy and safety of ultrasound (US)-guided radiofrequency ablation (RFA) for tumor control and quality of life (QoL) management in patients with PTMC who favored AS over immediate surgery.
Methods:
This prospective clinical trial was conducted at a single tertiary referral hospital from 2018 to 2021. Of 227 adult patients aged ≤60 years with low-risk unifocal PTMC favoring AS over immediate surgery, 100 patients underwent RFA for their management. The primary endpoint was the disease progression rate, and secondary endpoints were technical success, volume reduction rate (VRR), complication rates, and QoL.
Results:
The median age of the study population was 42 years (range, 27–59 years), and 83% (83/100, [CI: 66.1–100]) were female. The median follow-up was 30 months (range, 12–56 months). All 100 patients underwent RFA with technical success. Most of the ablation zones showed continuous volume reduction, and 95.9% (94/98, [CI: 77.5–100.0]) showed complete disappearance at the last follow-up. The median VRR was 100.0% at 1-year follow-up and persisted throughout the last follow-up. The cumulative disease progression rate among 98 patients who underwent at least 1-year follow-up was 3.1% (3/98, [CI: 0.6–9.0]); one patient had lymph node metastasis (treated with surgery), and two patients had new PTMC (1 treated with RFA, 1 ongoing AS). Major complications were not observed. Psychological (baseline vs. last follow-up, 7.3 vs. 8.0, p = 0.002) and social (8.0 vs. 8.7, p = 0.005) QoL scores significantly improved during follow-up without compromising physical QoL (8.6 vs. 8.5, p = 0.99).
Conclusions:
RFA can be a reasonable strategy for effectively and safely controlling tumors and improving QoL in non-elderly patients with low-risk PTMC appropriate for AS.
Clinical Trial registration: This trial is registered with ClinicalTrials.gov: NCT03432299.
Introduction
Papillary thyroid microcarcinomas (PTMCs) are characterized by slow growth and high cancer-specific survival rates. 1 Hence, the most recent societal guidelines for management of thyroid nodules and differentiated thyroid cancer have considered active surveillance (AS) as a reasonable option for management. 2 –5
AS may appeal to a subset of individuals who are especially risky and surgery-averse. However, there are concerns regarding the adoption of AS in clinical practice, particularly in younger patients. Recent studies have consistently reported higher progression rates in younger patients compared to older patients. 6,7 In addition, cost-effectiveness studies from several countries have shown that direct medical costs of AS surpass those of surgery after long term follow up 8 –10 Therefore, there may be concerns for younger patients who have a longer life expectancies and a higher risk of disease progression. In addition, many patients are apprehensive about just observing their “cancer.” A meta-analysis reported that 32%–69% patients underwent delayed surgery without tumor progression during AS 7,11 In another large population long-term study, 28.2% of patients were lost to follow-up after AS, 12 and patient anxiety is suggested as a one of the major causes. 11,13,14 Thus, long-term AS may pose challenges especially in physically and socially active patients with long life expectancies.
There is a pressing need to identify approaches for treating malignant diseases less invasively. Introduced in the early 2000s, various ultrasound-guided percutaneous ablation methods emerged as potential alternatives to surgery in patients with cancer. 15 –20 Recent evidence has demonstrated excellent outcomes of thermal ablation in patients with low-risk thyroid cancer. 21 –23 However, a recent study demonstrated that AS may be a viable option compared to radiofrequency ablation (RFA) in patients over 60 years old, based on the lower progression rates observed in this group. 24 Therefore, RFA could be particularly beneficial for younger patients under 60. Nevertheless, no prospective study has investigated the outcomes and quality of life (QoL) of patients with PTMC, excluding those over 60 years old. 22,23,25 –29 Furthermore, most existing studies have focused solely on thermal ablation in patients for whom surgery is challenging. 23,25 –30
Therefore, we aimed to evaluate the efficacy and safety of ultrasound (US)-guided RFA for tumor control and QoL management in patients ≤60 years with PTMC eligible for AS.
Methods
Study design and patients
This investigator-initiated single-center prospective study (ClinicalTrials.gov identifier: NCT03432299) was approved by the Institutional Ethics Committee of Seoul National University Hospital (IRB No. 1711-029-897 and 1801-116-917), followed the consolidated standards of trials (CONSORT) reporting guidelines. This study was funded by
Between November 2018 and November 2021, low-risk PTMC patients were screened with the following inclusion criteria: (i) thyroid nodule with suspicious for papillary thyroid carcinoma (PTC) or PTC results on fine needle aspiration or core needle biopsy (CNB), with no cytopathologic features with poor prognosis; (ii) maximal nodule diameter ≤1 cm (iii) 19 years ≤ age ≤60 years; (iv) no sonographic evidence of extrathyroidal extension (ETE) 31,32 (Supplementary Data S1); (v) no pathologically proven cervical lymph node (LN) metastasis or distant metastasis; and (vi) no prior neck irradiation or surgery.
The exclusion criteria included hyperthyroidism, pregnancy, pacemaker insertion, uncorrectable bleeding diathesis, and uncooperative patient characteristics. For patients with low-risk PTMC, physicians (S.W.C., Y.J.P., and D.J.P., with more than 10 years of expertise in thyroid endocrinology) provided detailed information about PTMC, explaining about surgery and AS as the current standard management options by using a decision aid. 33 For patients who chose AS, the physician explained the characteristics, pros, and cons of each option (Supplementary Data S1). After careful consideration of each management option, patients who accepted RFA and agreed to participate signed a consent form and were enrolled.
Preablation evaluations
Details of the preablation evaluations, including baseline laboratory tests and imaging studies used to evaluate the feasibility of RFA, are provided in Supplementary Data S1.
RFA procedure
RFA was performed by a thyroid radiologist with 10 years of experience in thyroid intervention (J.-h.K.). Details of the equipment, patient positioning, monitoring, and anesthesia are described in Supplementary Data S1. For most tumors, a transisthmic approach using the moving-shot technique was adopted. 34,35 The procedure started by circumferentially ablating the normal thyroid parenchyma just peripheral to the tumor margin and progressed centripetally toward the center of the tumor (Supplementary Figure S1). Ablation was repeated 3–4 times, with small overlapping ablation units. 36 For subcapsular tumors near tracheoesophageal groove, or patients with periprocedural voice changes, hydrodissection technique was performed by injecting cold 5% dextrose water to create a fluid gap between the tumor and the critical structures and prevent thermal injury. 34,37 Immediately after the procedure, US examination was performed to evaluate the technical success of RFA, defined as when the tumor ablation zone completely covered the original tumor, with the outer edge of the ablation exceeding the tumor by at least 2 mm, except for subcapsular PTMCs. In addition to grayscale US, Color Doppler US and microvascular imaging (X-microviewTM, Alpinion, Seoul; MV flowTM, Samsung, Seoul, Korea) were performed to ensure avascularity within the ablation zone. After RFA, all patients were observed for at least 30 minutes in the hospital. Treatment parameters, including ablation time, energy, and pain scores (scaled from 0 to 10 using a visual analog scale), were recorded.
Post-ablation assessment and follow-ups
Postprocedural follow-up examinations were performed at 2 months, every 6 months until 3 years, and every year thereafter to evaluate complications, serial hormonal changes, and the ablation zone. Details of the post-ablation evaluations are provided in Supplementary Data S1. On imaging, the volume of the ablation zone, presence of local tumor recurrence (LTR), new thyroid cancer, LN, and distant metastasis were evaluated. LTR was defined as biopsy-confirmed cancer within and around the ablation-zone margin. A US-guided biopsy was performed to determine whether LTR, new cancer, or LN metastasis developed. Biopsy for LTR was considered when the ablation zone showed persistent nodular appearance in more than one year of follow up.
Complications during the procedure and follow-up were assessed by the operator (J.-h.K.) according to the reporting standards of the Society of Interventional Radiology. 38 The appropriate management methods were verified and recorded. After performing RFA, there were no restrictions on pregnancy. We recorded any pregnancy and delivery events after RFA. During the follow-up period, no specific TSH level was targeted. Instead, follow-up was conducted in accordance with the general guidelines for treating hypothyroidism or during pregnancy. 39,40 Patients who could not visit for their follow-up appointments were contacted for a phone interview for their outcomes.
Assessment of quality of life
We used the Korean version of the thyroid-specific QoL questionnaire originally developed by Dow et al, 41 and further developed and validated by Ryu et al., 42,43 consisting of physical, psychological, social, and spiritual domains (Supplementary Data S1). Each domain includes several secondary questions. The QoL score for each dimension is the average score for the questions related to each dimension. Responses to the QoL survey were obtained by a trained clinical research coordinator at enrollment and every 6 month follow-up visit after the procedure. The patients were divided into low and high QoL groups based on the baseline psychological QoL score according to the cutoff value of 6.8 points, which is the average score in the surgery group reported in a previous study. 44 Their longitudinal changes of QoL in these groups were also assessed.
Outcome definitions and statistical analysis
The primary endpoint was the disease progression rate, Disease progression was defined as the occurrence of LTR, new thyroid cancer, LN metastasis, distant metastasis, or thyroid cancer-related deaths. The secondary endpoints were technical success, volume reduction rate (VRR), complication rates, and patient-reported QoL. Except for the assessment of the technical success rate, patients who underwent at least 1 year of follow-up were included in the analysis.
A chi-square test was used to compare categorical variables, and Student’s t-test or Mann–Whitney U test was used to compare continuous variables. A repeated-measures analysis of variance (ANOVA) general linear model was applied to detect changes in QOL over the time points and differences between patient factors. A two-tailed p < 0.05 was considered statistically significant. All statistical analyses were performed using the MedCalc software package (version 22.2) and PASW software (version 17.0; SPSS Inc., Chicago, Illinois, USA). Outcomes such as tumor size, volume, and VRR were compared using the Wilcoxon signed-rank test. Continuous variables are reported as means ± SD.
Results
Patient and tumor characteristics
Among 559 patients diagnosed as low-risk PTMC from November 2018 to November 2021, nine were excluded who did not meet the inclusion criteria, 289 patients (52.5%) chose surgery, and 34 were lost to follow-up (Fig. 1). Of 227 patients who preferred AS over surgery, 127 declined RFA. Of the 100 (38.3%) patients who underwent the RFA, (M:F = 17:83, median age 42 years, range 27–59 years), two were lost to follow-up at the 2 month and 1 year visit after the successful RFA procedure. They showed no complications or disease progression during the follow-up period. The remaining 98 patients underwent follow-up for one year or longer and were included in the analysis of the RFA clinical outcomes. The baseline characteristics of 100 patients are summarized in Table 1. The median follow-up duration after RFA was 30 months (range, 12–56 months). The median of largest tumor diameter was 0.62 cm (range, 0.23–1.0 cm), and the median volume was 0.18 mL (range, 0.009–0.64 mL). All patients underwent thyroid function tests in their follow-up visits.
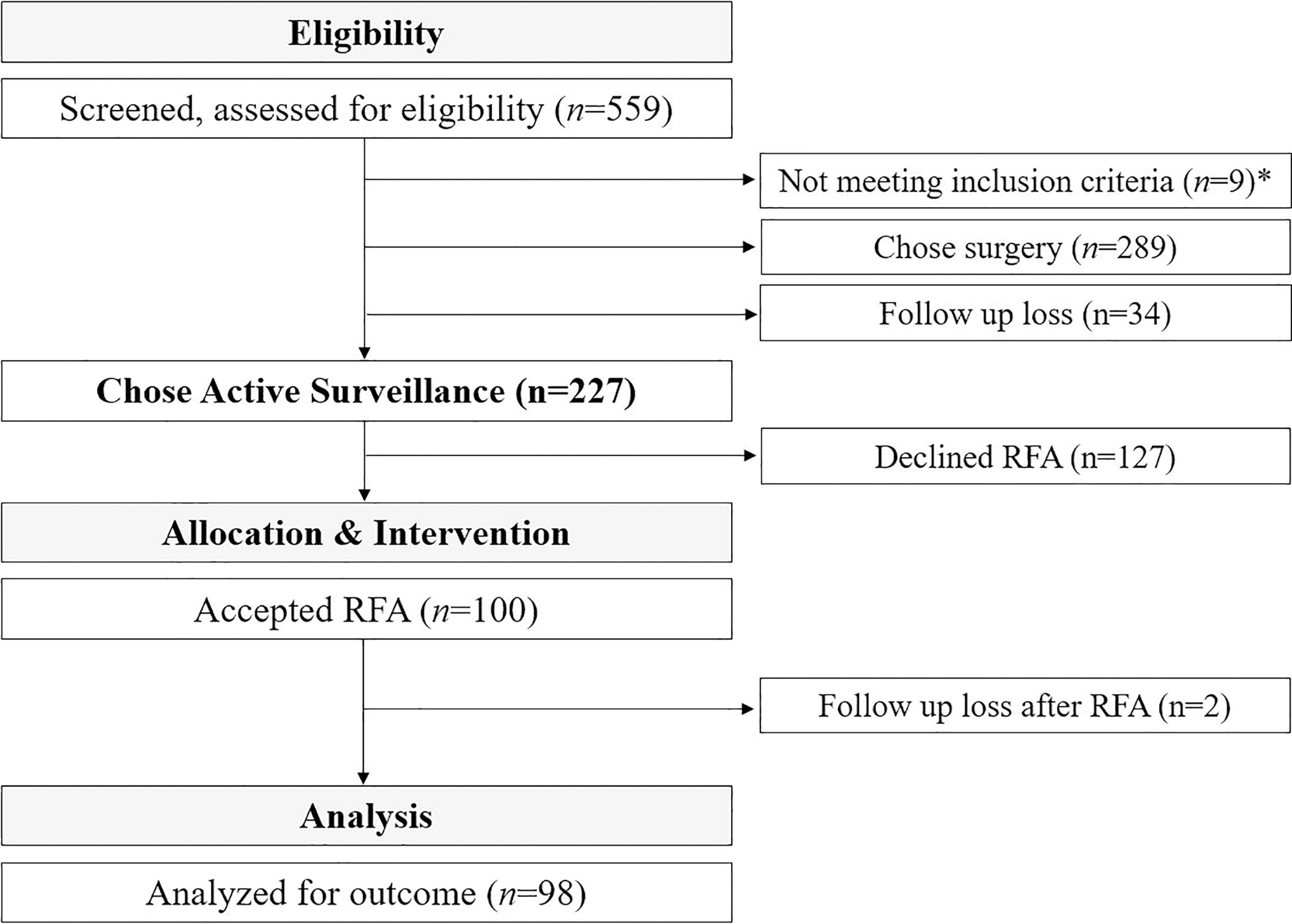
Flowchart for this prospective clinical trial on the radiofrequency ablation for low-risk papillary thyroid carcinoma. *Patients were excluded upon the results of US reassessment (tumor larger than 1 cm, extrathyroidal extension or lymph node metastasis suspected).
Demographics of the Patients (n = 98)
Numbers in parentheses are ranges.
FNA, fine needle aspiration; CNB, core needle biopsy; PTMC, papillary thyroid microcarcinoma; TSH, thyrotropin.
Treatment parameters
The RFA procedure was successfully performed in a single session for all 100 patients, achieving a technical success rate of 100%. Hydrodissection was performed in 86 patients. The mean pain score was 4.6 (range, 1–8). The median ablation power and ablation time were 15W (range, 10–20 W, total delivered energy, 0.59 kcal [2468.6 J] range, 0.02–2.03 kcal [83.7–8193.5 J]), and 4 minutes 12 seconds (range, from 1 minute 30 seconds to 9 minutes 4 seconds). The median size and volume of the immediate ablation zone were 1.55 cm (range, 0.85–2.4 cm) and 1.75 mL (range, 0.3–5.15 mL), respectively.
Changes in ablation zone
Of the 98 tumors with more than 1 year of follow-up, the median volume of the ablation zone at each examination and VRR are shown in Figure 2 and Table 2. Because the PTMCs were treated including the safety margin, the ablation zones increased immediately and gradually decreased in volume afterward. The median VRR was 100.0% at 1-year follow-up and persisted throughout the last follow-up. Most of the ablation zones showed continuous volume reduction, and 95.9% (94/98, [CI: 77.5–100.0]) showed complete disappearance at the last follow-up. Four patients showed residual focal lesions in the ablation bed with median VRR of 95.5% (range, 87.3–99.6%) at the last follow-up (mean, 2.4 years; range 2–3 years). Among them, CNB was performed in two patients who showed persistent nodular calcified lesions in the residual ablation zones one year after RFA. The biopsy revealed benign postprocedural changes, comprising fibrous tissue with some macrophages and chronic inflammatory cells. The lesion volume continued to decrease during subsequent follow-up (Supplementary Figure S2). The remaining two patients underwent observation because of the small size of the calcified ablation zone and showed continuous volume decrement.
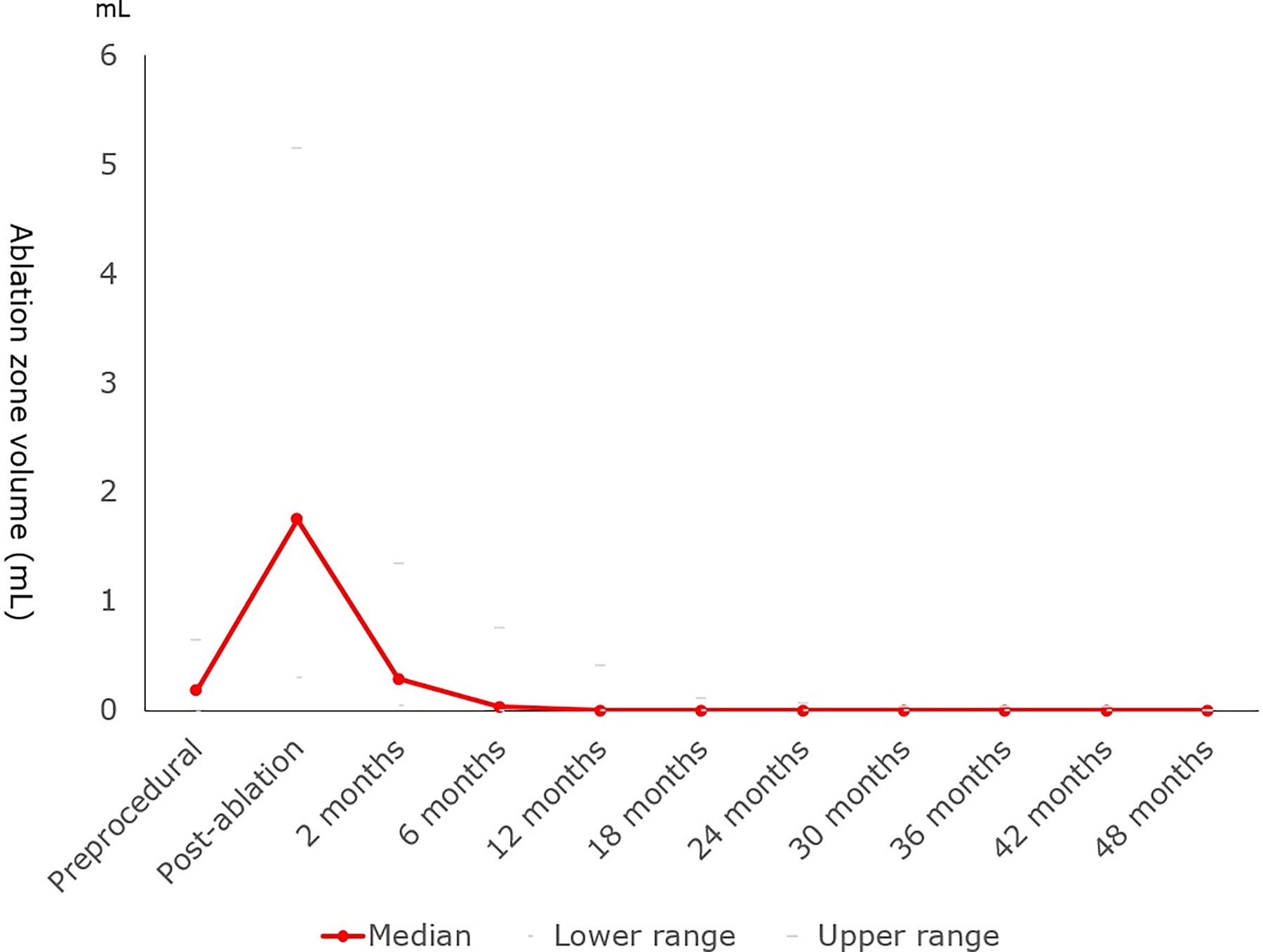
Changes in tumor/ablation zone volumes before and after the radiofrequency ablation procedure.
Changes in Tumor and Ablation Zone Volume at Each Follow Up
Numbers in parentheses are ranges.
VRR was calculated relative to preablation tumor volume.
VRR, volume reduction rate.
Oncologic outcomes
At the last follow-up (median 30 months), disease progression rate was 3.1% (3/98, [CI: 0.6–9.0]). One patient (1.0%, 1/98, [CI: 0.2–5.7]) showed new LN metastasis in the ipsilateral neck level 4, which was detected at 24 months after RFA, and underwent delayed surgery and radioactive iodine ablation. Otherwise, there were no other instances of delayed surgery. Two patients (2.0%, 2/98, [CI: 0.2–7.4]) showed new PTMCs in the contralateral lobe at 30 months and 17 months after RFA, respectively. The initial ablated PTMCs disappeared 6 months and 1 year after RFA. One patient was successfully managed with additional RFA, and the ablation zone disappeared 1 year after the additional RFA. The other patient chose AS, and the new PTMC showed stability at the 2-year follow-up. The average TSH levels (range) during the follow-up period for these three patients were 2.7(mIU/L) (range, 1.05–4.4, patient with LNM), 10.4(mIU/L) (range, 2.86–58.0, new PTMC), and 3.1(mIU/L) (range, 1.0–4.9, new PTMC), respectively, while the non-recurrence group had an average of 1.8 ± 0.88(mIU/L). There were no cases of LTR, distant metastases, or thyroid cancer-related death.
For the two patients who were lost to follow-up visits at our institution, we conducted follow-up telephone interviews to determine their outcomes at 30 or 36 months after RFA, respectively. Both patients underwent surveillance US examinations at another hospital. To date, there has been no evidence of disease progression.
Complications and quality of life
One patient experienced voice change, which spontaneously recovered at 6 months follow-up. No RFA-related life- threatening complications were observed.
Figure 3 shows the change in the QoL scores of patients at baseline and follow-up visits after treatment. Among the four domains (physical, psychological, social, and spiritual), psychological (7.3 vs. 8.0, p for trend = 0.002), social (8.0 vs. 8.7, p for trend = 0.005), and overall QoL scores (7.4 vs. 7.6, p for trend = 0.001), showed significant improvement. Benefits were observed early at 6 months post-procedure and increased further. No statistically significant differences were observed for the physical (8.6 vs. 8.6, p for trend = 0.99), and spiritual QoL domains (5.8 vs. 5.5, p for trend = 0.132). Notably, a significant increase in psychological QoL was observed in both the low (5.6 ± 0.9 vs. 7.8 ± 1.2, p for trend < 0.001) and high QoL subgroups (7.8 ± 0.8 vs. 8.5 ± 0.9, p for trend = 0.048). Although the difference in QoL between the low and high groups persisted until the last follow-up, QoL in the low group increased significantly, with an average rise of 2.2 points compared to a 0.7-point increase in the higher QoL group (Fig. 4).
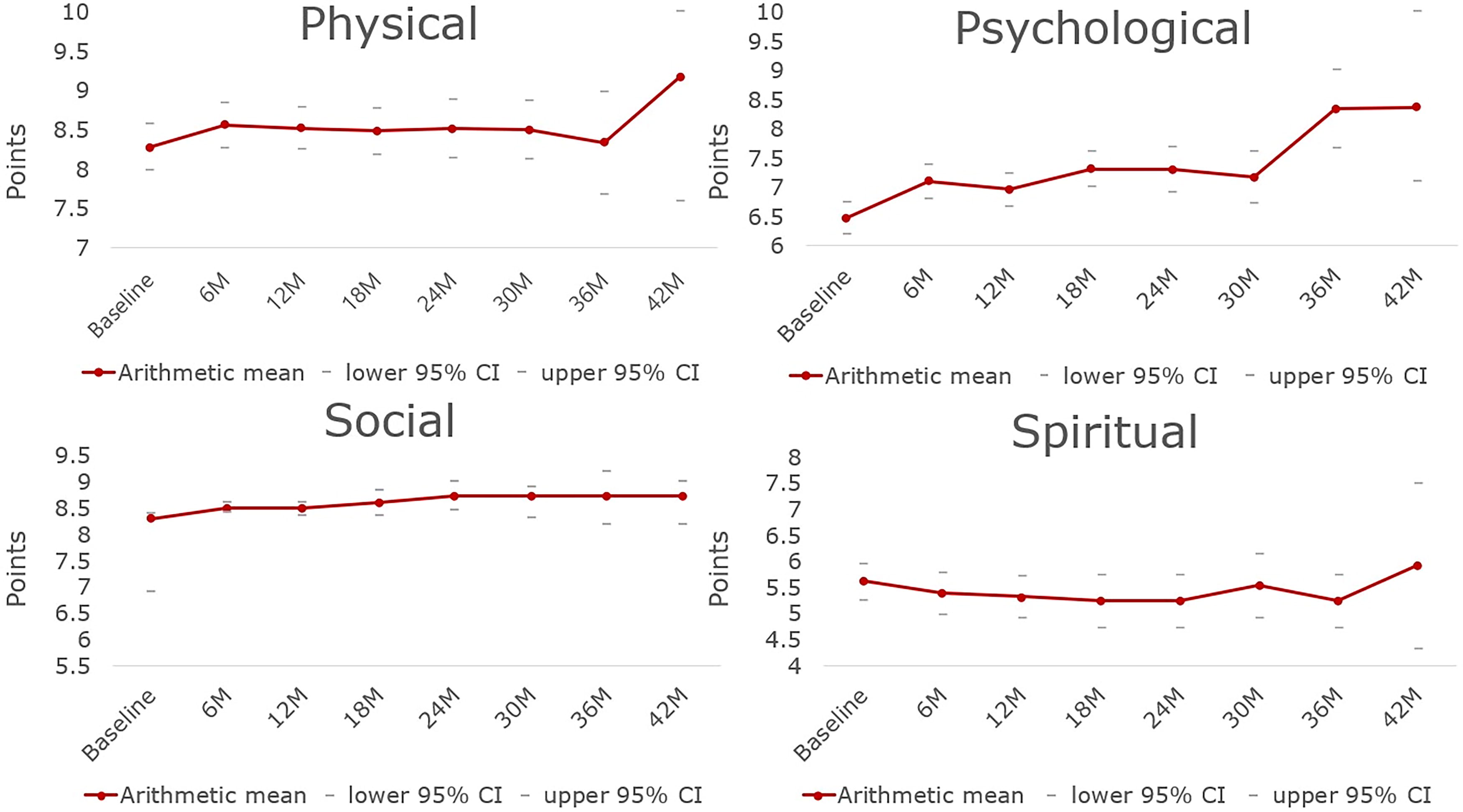
Longitudinal changes of quality of life at baseline and after radiofrequency ablation procedure.
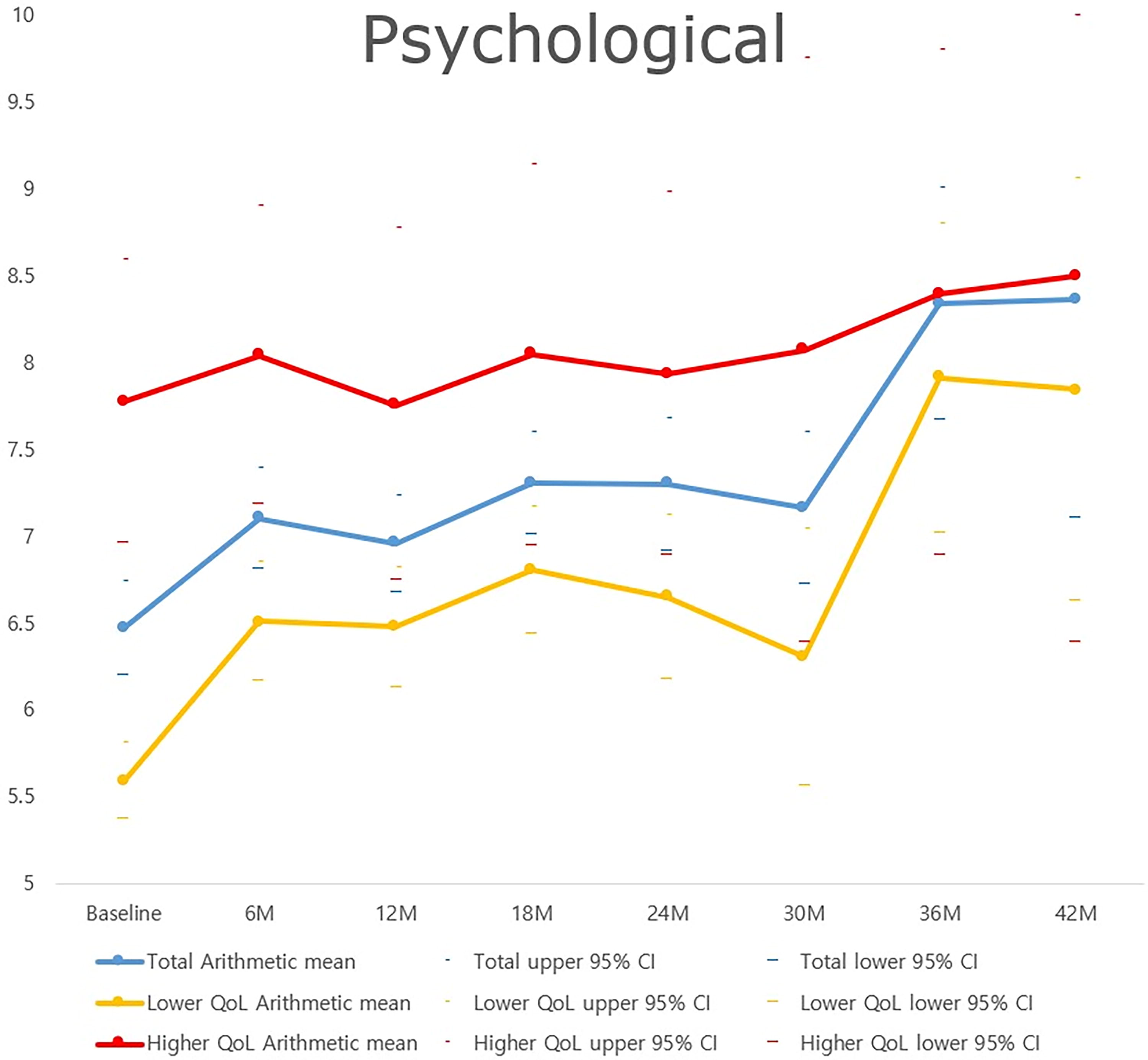
Longitudinal changes of quality of life (QoL) at baseline and after radiofrequency ablation in patients with lower and higher baseline psychological QoL scores.
Meanwhile, nine patients became pregnant (median, 15 months after RFA; range, 4–23 months) and delivered at full term (Table 3). There were no perinatal or fetal complications associated with pregnancy and delivery. Additionally, there were no cases of tumor progression during or after pregnancy. The patients who completed pregnancy also demonstrated an improvement in psychological QoL scores (7.0 ± 1.0 vs. 8.8 ± 0.9, p for trend = 0.006) similar to other subjects during the follow-up period. Figure 5 shows a representative example.
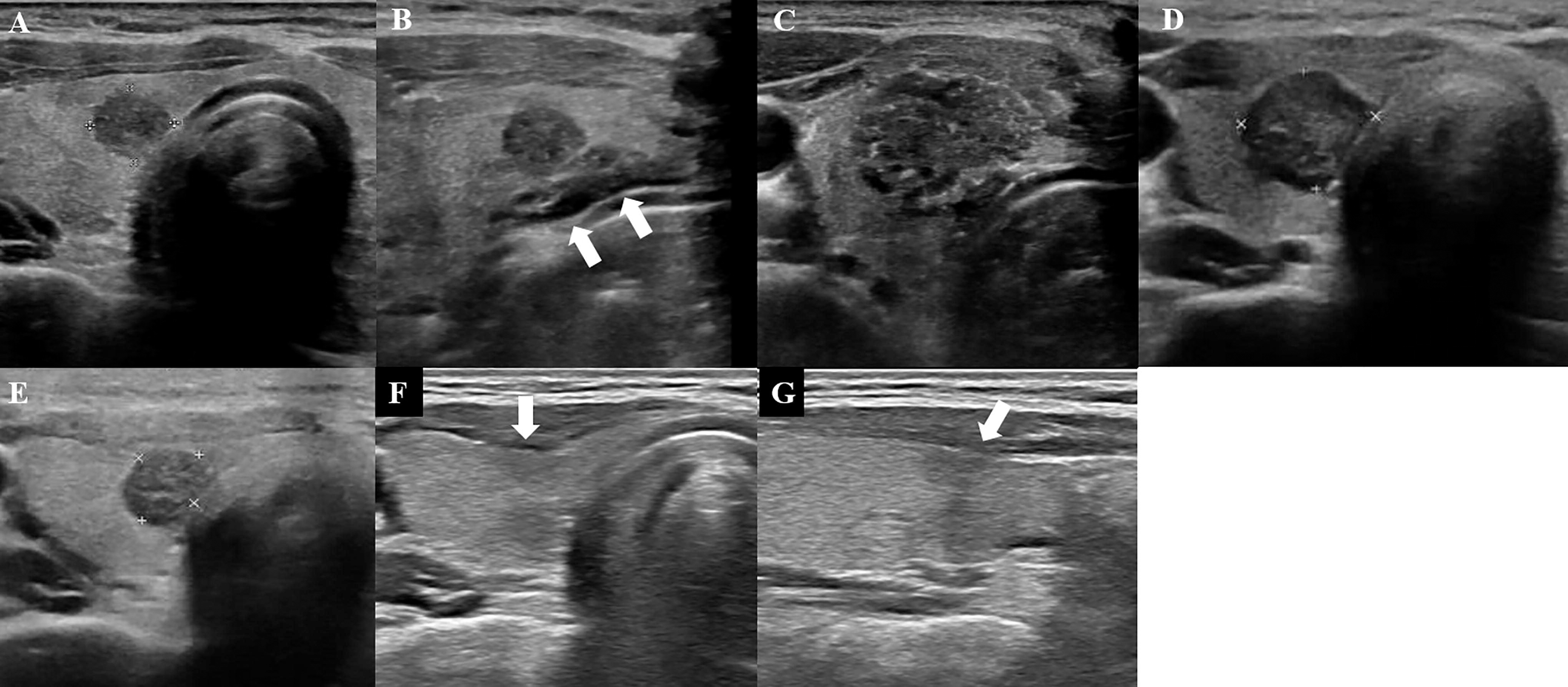
A 29-year-old female patient with 6 mm sized papillary thyroid microcarcinoma. Preprocedural ultrasound (US) image shows a tumor in the mid portion of right thyroid gland
Characteristics of Patients Who Became Pregnant after the RFA Procedure
Two pregnancies after RFA.
No significant pre- or perinatal adverse events.
Quality of life scores obtained during pregnancy.
RFA, radiofrequency ablation; GA, gestational age; VRR, volume reduction ratio; QoL, quality of life.
Discussion
Our prospective cohort study showed that RFA is a reasonable option for the management of low-risk PTMC in patients aged 19≤ and ≤60 eligible for AS. RFA resulted in the complete disappearance of ablated tumors in the majority of cases, and there was no need for delayed surgery except in one case with LN metastasis and no significant complications. We found serial improvements in psychological and social QoL that were sustained for over two years after ablation. The progression rate was similar to the results of various other thermal ablation studies that treated the general population with PTMC irrespective of patient age, 23,25,26,45 although we targeted relatively young patients who are known to have higher progression rates of PTMC under AS. In contrast to other studies, 23,25,26,45 we performed RFA exclusively on patients who were candidates for AS and did not include those who chose surgery. While showing a similar improvement in QoL as the AS group, 43,46 we also demonstrated that patients who chose RFA instead of surgery could achieve similarly favorable oncologic outcomes compared to those who underwent surgery. 23,25,26,45 Compared to the surgical group, RFA not only resulted in comparable oncologic outcomes but also offered other advantages, such as shorter hospital stays, less scarring, lower rates of complications (e.g., hypoparathyroidism, recurrent laryngeal nerve injury, hypothyroidism), and better QoL. 47 –49
We adopted the technical strategy of first ablating the peripheral normal parenchyma of the tumor to its center because immediate echo change produced during central tumor ablation could hinder effective discrimination between the ablated tumor and the ablated normal parenchyma. This method was called as the centripetal ablation technique in early hepatocellular carcinoma and has been known to provide an optimal ablation margin which could improve local tumor control. 50 Moreover, this technique can target the peritumoral feeding and draining vessels early in the ablation process and thus reduce the possibility of tumor spread caused by increased intratumoral pressure due to vaporization during ablation. 51 While we cannot definitively determine how much our method contributed to the prevention of recurrence or metastasis, it is cautiously inferred that the aforementioned technique might have positively contributed to the outcome of RFA for PTMC.
Safety outcomes in our study were also favorable, as in previous studies. 23,25,26,45 The complications associated with ablation were minimal and transient from combining of hydrodissection and cooling. Transient voice changes were observed in 1% of patients, a significantly lower incidence compared to the postoperative complication rate observed in a recent cohort with similar clinical profile. 52
Except for the two patients who developed new PTMCs in the contralateral lobe, disease progression related to the original tumor occurred in only one patient with LN metastasis. In this patient, the LN metastasis might have existed in an occult form at the time of diagnosis before RFA and slowly progressed to clinically apparent LN metastasis. This underlines the importance of careful follow-up for patients, even when no clinical LN metastasis is detected at the time of diagnosis, considering the possibility of undetectable micrometastasis.
In our study, the incidence of LN metastasis (1%) was similar to the AS group in our recent multicenter low-risk PTMC cohort (MAeSTro cohort; 1.3% during 3.5 years), which had similar baseline characteristics to our RFA study group. 53 The incidence of new PTMC was also similar between this study (2%) and the MAeSTro cohort (1.5%). In the AS group, however, additional disease progression was observed related to tumor size enlargement (5.8%) and ETE of the original tumor (0.4%), eventually resulting in delayed surgery in 9% of cases. Importantly, unlike the AS group, there was no LTR in this RFA group, resulting in no disease progression from the primary tumor. Consequently, the rate of conversion to surgery or additional treatments was lower in this study compared to the MAeSTro AS group. Similarly, despite the younger age of our RFA group compared to the other AS studies, the disease progression and surgery conversion rates were also significantly lower. 6,12,46,54
Although AS is continuously widening its indications, 2,4,55 one of the main concerns is the anxiety experienced by both the patient and physician. Anxiety and QoL are important clinical outcome measures in patients with PTMC undergoing AS because they live lifelong with indolent tumors. In our study, approximately 40% of patients who chose AS further opted for RFA at the time of enrollment, indicating that many patients who favored AS rather than surgery still feel apprehensive about solely monitoring the cancer without intervention. The knowledge of having cancer and the uncertainty of tumor progression can exacerbate the anxiety of the patient and may lead to unnecessary early surgery. However, there were no cases of delayed surgery due to patient anxiety or a change of mind after RFA. Our results contrast with those of previous studies reporting 10–30% surgery conversion rate without progression during AS. 11 Patients who select delayed surgery without progression during AS have lower QoL scores 43 and higher anxiety levels. 46 The gradual improvement in psychological and social QoL scores without compromising physical QoL observed in our study clearly demonstrates the advantages of RFA in controlling these populations’ treatment.
The gradual improvement in psychological and social QoL scores after RFA was observed not only in the high QoL group but also in the low QoL group, whose scores were similarly low to those of the surgery or delayed surgery conversion AS groups. This improvement occurred without compromising physical QoL, as observed in our study, and this clearly demonstrates the advantages of RFA in this population.
Notably, nine patients became pregnant within a few years after RFA, and none of them demonstrated tumor progression, recurrence, or delayed surgery. In addition, all of these patients showed similar improvements in QoL as observed in other patients. As it remains unclear whether pregnancy is a risk factor for progression, 56,57 our results demonstrate the potential of RFA as an option for female patients who desire to bear children, by reducing the risk of progression and controlling anxiety.
RFA is a more invasive management strategy than AS. However, considering the very low complication rates and preserved physical QoL in RFA patients, RFA could serve as a good management option for the socially and biologically active patients who favor AS but are still anxious about keeping the “cancer,” including women intending to become pregnant.
This study had some limitations. First, although this study was one of the few studies demonstrating longer-term follow-up data among prospective studies, 58 it was a single-center study with a relatively small number of patients and a limited follow-up period. However, it is notable that this study focused on patients under 60 years old, a group for whom AS can be challenging in terms of disease progression and cost-effectiveness. Moreover, by including only patients who chose AS, whose baseline QoL is known to be higher than those who chose immediate surgery, it allowed for more meaningful comparisons of QoL with the AS group. QoL is an important issue in managing indolent tumors like PTMC, and this aspect has not been previously published in a prospective cohort. Therefore, the observed increase in QoL after RFA in this study may help to provide significant insights for choosing a treatment method. However, this study did not include an AS group or an immediate surgery group, so a direct comparison of oncologic outcomes or QoL of the RFA group with others was not possible. Future head-to-head comparisons are needed. In addition, this study did not perform a cost-effectiveness analysis. Given that this study investigated QoL, including an economic evaluation would have enabled to provide comprehensive information for health policy planning. Furthermore, since the sonographic assessment and technical aspects of RFA depend largely on the operator’s experience, multicenter studies with longer-term follow-up results are necessary to validate the actual clinical impact of RFA. In this study, no specific target was set for TSH level during follow-up, since establishing a TSH target might complicate the interpretation of the oncologic outcomes of RFA itself. Because it was reported that thyroid hormonal supplementation can reduce the risk of disease progression during AS, 59 further research is needed to determine whether setting a TSH target or supplementing thyroid hormones after RFA also could benefit oncologic outcomes. Studies should assess the benefits of TSH targeting against the potential risks of thyroid hormone supplementation, which would be important in RFA group.
Conclusions
This prospective trial showed that RFA for low-risk PTMC could be a reasonable option to achieve an effective and safe outcome for tumor control and improvement of QoL in patients appropriate for AS. Although AS is recommended as an alternative to surgery for low-risk PTMC, RFA can be a favorable option, particularly for younger patients who may be biologically active or at high risk of disease progression, or for those who have concerns about QoL or anxiety. Physicians should consider various sources for the best personalized management of low-risk PTMCs. Patients must be fully informed, including about the impacts on QoL, when choosing a treatment option.
Footnotes
Acknowledgment
The authors thank Yoo Rim Baek for her assistance in data collection.
Availability of Data and Material
Data generated or analyzed during the study are not publicity available, however are available from the corresponding author on reasonable request.
Authors’ Contributions
Study conception and study design: J-h.K., Y.J.P. Data collection: D.G.N., J.Y.S., J.S.S, S.W.C., D.J.P., J-h.K., Y.J.P. Data analysis and interpretation: J.Y.L., J-h.K. Article drafting: J.Y.L., J-h.K., Y.J.P. Revising or critically reviewing the article: J.Y.L., D.G.N., J.Y.S., J.S.S., S.W.C., D.J.P., J-h.K., Y.J.P.
Author Disclosure Statement
The authors have no conflicts of interest to declare that are relevant to the content of this article.
Funding Information
This research was funded by the
This research was also supported by a grant of the Korea Health Technology R&D Project through the Patient-Doctor Shared Decision Marking Research Center (PDSDM), funded by the
Supplementary Material
Supplementary Data S1
Supplementary Figure S1
Supplementary Figure S2