
Abstract
Background:
Normal brain development, mood, and cognitive functions depend on thyroid hormone (TH) action. However, little is known about how TH mediates its actions in the human brain. This is due to limited access to human brains deprived of TH during fetal and early postnatal life, as well as from adults with altered thyroid status. One way to partially bypass these limitations is by using magnetic resonance imaging and spectroscopy, two neuroimaging techniques that provide detailed, noninvasive information on human brain structure and function. Another way is using human-induced pluripotent stem cell (hiPSCs)-derived three-dimensional in vitro systems, known as brain organoids, which allow for the study of fundamental aspects of the early stages of human brain development.
Summary:
This narrative review focuses on neuroimaging and brain organoid studies. Neuroimaging of human brains performed in individuals with different thyroid conditions provides information on the volume, myelination, blood flow, neural activity, and connectivity of different areas. Such studies show that suboptimal thyroid status can impact human brain development and its normal function throughout life. This is true not only for patients with sporadic congenital hypothyroidism, during pregnancy or early after birth, but also for adult patients with hypo- or hyperthyroidism, patients carrying mutations that manifest as impaired sensitivity to TH, and even for normal individuals during aging. Studies using brain organoids generated from hiPSCs of healthy individuals or patients with thyroid genetic conditions provide insights into how TH can impact the early development of the human cerebral cortex.
Conclusions:
The developmental alterations in children born to mothers with different degrees of gestational hypothyroidism or who developed hypothyroidism early in life are remarkable, affecting multiple brain regions and pathways, including the cerebral cortex, hippocampus, cerebellum, interhemispheric and corticospinal tracts, and associative nuclei. The data connecting such changes to poor neurological outcomes in adult patients with hypothyroidism represent an objective link between thyroid-specific functional brain alterations and behavior. Growing brain organoids require TH, which is critical for human neurogenesis and oligodendrogenesis. These models have proven useful in screening drugs with potential therapeutic effects for patients with genetic thyroid diseases.
Introduction
The fact that the human brain responds to thyroid hormone (TH) and that TH is important for normal human brain development are well-established concepts. However, with a few exceptions, 1,2 these conclusions are based on observational studies of manifested symptoms of hypothyroidism and hyperthyroidism, as well as the assessment of cognitive outcomes of children born with congenital hypothyroidism. 3 –7 There is a large volume of literature focused on the brain of animal models (mostly mice and rats), and indeed, these animals with congenital hypothyroidism exhibit many brain alterations, including smaller size, thinner cerebral cortices with decreased blood vessel networks, hypomyelinated interhemispheric commissures, and arrested migration and growth of neural cells. 7 –13 However, the brain cytoarchitecture differs greatly between humans and mice, 14 making these models poorly applicable to humans. Thus, having access to the brains of humans with thyroid dysfunction would be the ultimate resource for scientists who study TH and the brain, but the invasive nature of the available methods limits such an approach.
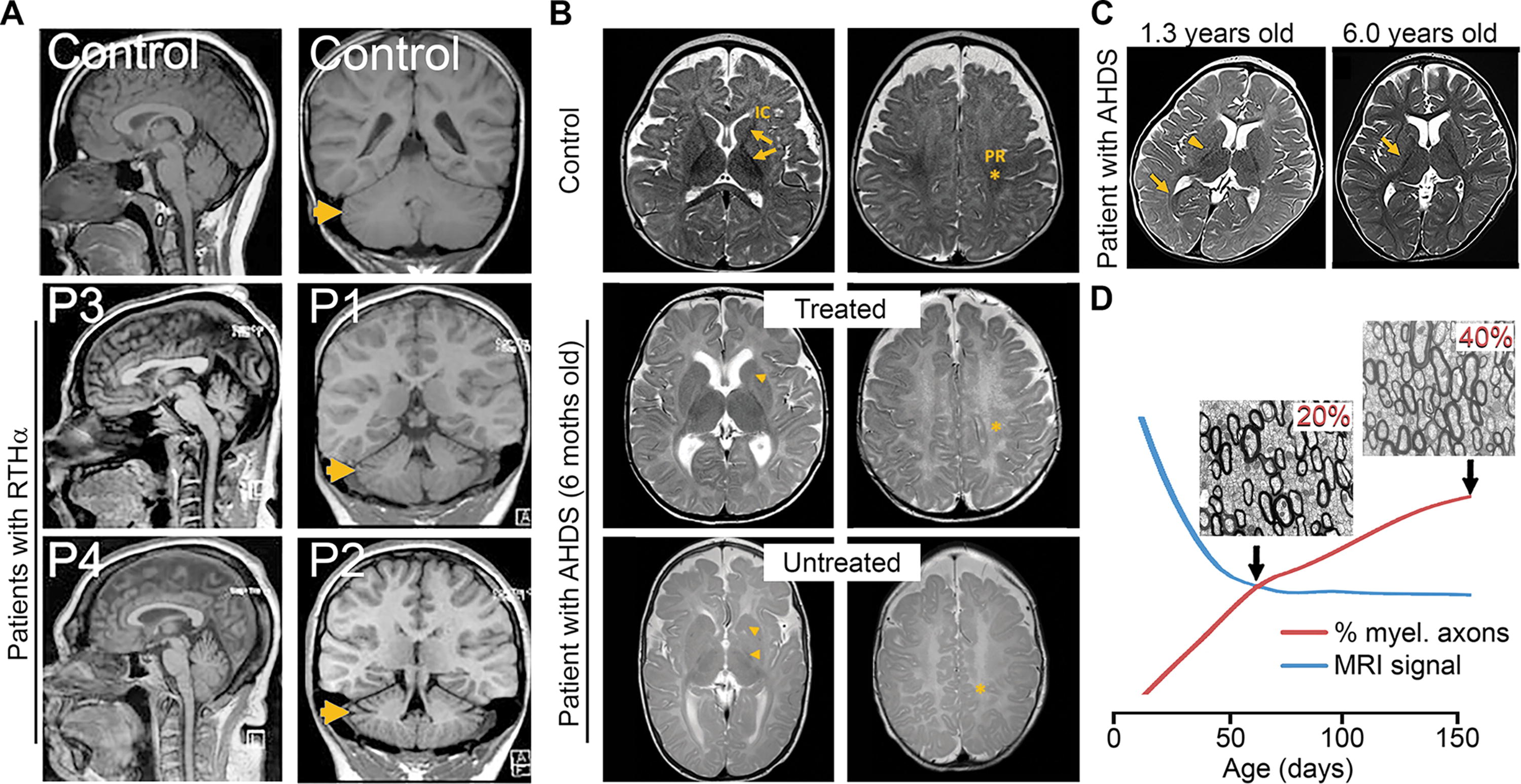
To overcome this limitation, noninvasive studies can use magnetic resonance imaging (MRI) to visualize the human brain. Routinely acquired anatomical MRIs (Fig. 1) create images of the brain with a resolution of less than 1 mm and can distinguish brain areas with different water content, discriminating between grey and white matter (less water content in the latter 15 ) and even degrees of myelination. Anatomical images are also used to measure the thickness and volume of brain regions, which may be influenced by changes in the number and size of neural cells in these areas 16 and other physiological factors. 17 MRI diffusion tensor images (DTI) detect changes in the freedom of water movement derived from changes in the brain structure and can produce images reflecting the organization of axonal bundles, as in the white matter tracts. 18 The availability of functional imaging techniques (fMRI) makes it possible to measure the energy demand of activated brain areas by detecting changes in the blood’s oxygen levels. 19 Moreover, magnetic resonance spectroscopy (MRS) can measure changes in the concentration of critical brain metabolites in vivo, allowing the detection of neuronal damage or demyelination. 20
Examples of studies using anatomical MRIs.
Unfortunately, neuroimaging studies do not provide direct mechanistic insight into how TH acts in the brain and are insufficient to study the role of TH during the early stages of brain development. To overcome this hurdle, a possible approach is the use of human-induced pluripotent stem cell (hiPSCs)-derived three-dimensional neural cultures, so-called human brain organoids. As the name implies, a human brain organoid is not the same as a human brain, but it can be considered a reductionist model that allows the study of some of the early stages of fetal brain development.
This narrative review presents neuroimaging and brain organoid studies and aims to build a comprehensive catalog relating brain alterations to thyroid conditions and neurological outcomes. The review criteria included a search for original articles published in English until February 2024 using PubMed with the following search terms: “thyroid hormones” and “magnetic resonance imaging or spectroscopy.” The search terms “resistance to thyroid hormone,” “Allan–Herndon–Dudley,” “hypothyroidism,” “hyperthyroidism,” and “organoids” were also used alone or in combination with “brain.” The reference lists of identified papers were also used to identify additional material.
Disruption of TH Action Early in Life
This review intends to distinguish between congenital and adult hypothyroidism. Congenital hypothyroidism can be endemic or sporadic. Endemic is caused by iodine deficiency. In contrast, sporadic hypothyroidism is caused by a genetic abnormality of the fetus, impairing thyroid gland development or hormone biosynthesis. The former is almost always severe because it affects both mother and fetus, while the latter form is usually mild or even asymptomatic because the fetal thyroid gland malfunction is minimized by the placental transfer of TH and prompt postnatal treatment. 24,25
Pregnancy and neonatal period
An example of how devastating endemic congenital hypothyroidism can be is illustrated in a unique brain MRI study of three patients with mental deficiency, deaf mutism, and a spastic-rigid motor disorder (aged 33–39) showing alterations in two connected regions: the substantia nigra and globus pallidus, 26 which correlate well with their motor disorders. Two additional neuroimaging studies of patients (6–16 years old) with late-treated sporadic congenital hypothyroidism described mild cerebral cortical atrophy in the frontal and parietal lobes 27 and elevated choline-containing compounds and N-acetylaspartate in the hippocampus, cerebellum, and temporal lobe, suggesting abnormal myelination and neural function. Remarkably, the level of these metabolites reverted to normal with TH replacement. 27
The outcome of a child with sporadic congenital hypothyroidism depends on the severity of the thyroid defect. In severe cases, neurological symptoms may persist even when the diagnosis is made at birth. 28 In all cases, time is of the essence, and a delayed diagnosis of sporadic congenital hypothyroidism, even mild forms, may result in neurological abnormalities. 29 Alterations in the brains of children with sporadic congenital hypothyroidism who started receiving treatment between the second and fourth weeks of life include reduced function and volume of the hippocampus and disruptive associative processing. 30 –33 Interestingly, music lessons ameliorated the hippocampal reductions, 31 suggesting structural neuroplasticity. 34 Sporadic congenital hypothyroidism is also associated with changes in the thickness of cortical areas, leading to altered language, motor, auditory, and visual functions, 35 and with structural abnormalities in their white matter tracts—despite timely and adequate treatment. 36 Conversely, one study found no alterations in MRI brain examination or myelination in this population. 37
Less severe alterations are expected in children born to mothers with poorly controlled gestational hypothyroidism. Both low and high maternal free thyroxine (FT4) levels during pregnancy have been associated with low child’s (∼9 years old) IQ score and reduced total grey matter and cortex volume 38 (representative studies associating abnormal thyroid status with MRI brain alterations and neurological outcomes are shown in Table 1). A similar association exists between maternal TSH and their children’s total brain and cortical grey matter volume. 45 In another study, the maternal FT4 has also been associated with changes in the male offspring’s (∼26 years old) DTI values in three projecting fibers: (i) the corticospinal tracts (motor control), (ii) the anterior and superior thalamic radiations, (memory and limbic system and sensory and motor information, respectively), and (iii) the forceps minor of the corpus callosum (the biggest interhemispheric commissure of the brain, helping integrate sensory, motor, and cognitive information). 39
Representative Studies Associating Abnormal Thyroid Status With MRI Brain Alterations and Neurological Outcomes
Compared to subjects exposed during pregnancy to FT4 levels within the normal range. T1-w, T1-weighted; rs-fMRI, resting-state functional magnetic resonance imaging; DTI, diffusion tensor images; FA, fractional anisotropy; FT4, free thyroxine.
In other studies of children born to mothers exhibiting elevated TSH values and autoimmune thyroiditis, children (∼10 years old) exhibited abnormal development of the corpus callosum. 40 Their anterior corpus callosum, which connects regions involved in attention, was smaller and correlated with increased difficulties in shifting attention. The posterior corpus callosum, which connects areas involved in forming and storing language information (e.g., Wernicke’s area), was larger and was inversely correlated with vocabulary performance. Two follow-up studies demonstrated that in this scenario, maternal TSH values are associated with changes in the thickness of the cerebral cortex within multiple brain regions and reductions in the offspring’s hippocampus. The latter plays a central role in memory, and these patients also obtained lower scores in memory indices. 30,46 In addition, DTIs of preterm infants (36–41 weeks) with subclinical hypothyroidism (elevated circulating TSH with FT4 in reference range) showed shorter thalamocortical axon fibers lengths in the bilateral superior temporal and Heschl’s gyrus (auditory processing), lingual gyrus, the calcarine cortex (visual cortex/processing), and the cuneus. 47
Impaired sensitivity to thyroid hormone
Defects at different steps along the pathway leading to TH action at the cellular level 48 can manifest as impaired sensitivity to TH. A peculiarity is that, albeit specific to some organs and cells, the defect has been present in the fetus since conception. Thus, these defects have the potential to affect the early stages of fetal brain development and cause severe neurological damage.
Resistance to thyroid hormone alpha
Pathogenic mutations in the THRA gene cause resistance to TH alpha (RTHα), and patients exhibit growth retardation with skeletal dysplasia and mild-to-moderate intellectual disability, notably affecting nonverbal IQ and sensorimotor processing. MRI shows reduced cerebellar volume and microencephaly in two adult cases 49 (Fig. 1A) and DTI in two young patients (9 and 13 years old), shows a global increase in the mean water diffusivity in white matter tracts, including those connecting the cerebellum to the neostriatum and the cerebral cortex. These patients also exhibit reduced N-acetylaspartate in the frontal white matter and thalamus. There is also one study describing a 2-year-old girl with RTHα presenting neurological manifestations and normal brain MRIs. 50 In the same study, a different girl with RTHα who was born prematurely presented altered myelination but no morphological abnormalities. Other cases exhibit general brain atrophy with the widening of the sulci (fissures) and normal ventricles. 51
Resistance to thyroid hormone beta
About one-half of subjects with resistance to TH beta (RTHβ; caused by dominant loss-of-function mutations in the THRB gene) have a learning disability, mental retardation (IQ <60) is present in ∼3% of cases, 52 and ∼50% are diagnosed with attention deficit hyperactivity disorder. 53 Notwithstanding, the course of the condition is variable, and most individuals achieve normal stature and development and lead a normal life at the expense of high TH levels and a slight thyroid gland enlargement. In others, especially those with biallelic mutations, low stature, hyperactivity, and intellectual impairment persist.
There are three MRI studies of the brains of these patients. One scanned 43 subjects with RTHβ 54 and described dramatic alterations consisting of extra or missing gyri (the bumps and ridges on the cerebral cortex) in the parietal bank of the Sylvian fissure and multiple Heschl’s transverse gyri. These areas are involved in auditory and language function and, thus, could contribute to the common, albeit variable, language disorders or the much less common hearing loss observed in patients with RTHβ. 55 However, these alterations were not present in a second study that scanned 21 patients with RTHβ. 21 Instead, they describe alterations in the corticospinal tract, an increased cortical thickness in the bilateral superior parietal cortex, and a decreased grey matter volume in the bilateral inferior temporal cortex and thalamus. These patients obtained higher scores in a self-rating questionnaire for attention deficit hyperactivity disorder, and a certain degree of correlation is described between the MRI alterations and these behavioral results. The third one is a case report of a severe case of RTHβ in a 22-year-old female with MRI evidence of demyelination and bilateral ventricular enlargement, 56 alongside neurological symptoms such as deafness, hypotonia, mental retardation, visual impairment, and a history of seizures. The clinical implications of having RTHβ also include negative pregnancy outcomes, 24,57 but we do not know if the brains of the progeny of mothers with RTHβ are affected.
Defects in TH cell membrane transporters
Different proteins can carry TH through cell membranes. Among them, the monocarboxylate transporter 8 (MCT8) is a potent and specific TH transporter, particularly important in supplying TH to the human brain. Loss-of-function mutations in the SLC16A2 gene (encoding MCT8) produce TH deprivation in the brain, with a paradoxical increase in TH levels in peripheral tissues. The result is Allan–Herndon–Dudley syndrome (AHDS), and patients present TH abnormalities accompanied by severe and irreversible neurological deficits and hypermetabolism. 58 –61 Moreover, with advancing age, microcephaly becomes apparent. 62
While the brains of patients with AHDS exhibit normal gross anatomy, alterations in neural populations and hypomyelination are well documented in a landmark study of a post-mortem examination of brain sections of a 30-gestational week fetus and an 11-year-old boy with AHDS. 2 MRIs from patients with AHDS show hypomyelination during the first years of life (Fig. 1B), sometimes extending into early adulthood. 23,63,64 For instance, a report presented a 6-year-old patient with hypomyelinated axonal tracts, including the subcortical U-fibers and periventricular tracts. 64 Alterations in the latter are also described in three other studies. 65 –67 In some cases, however, hypomyelination improves with age 2,64,68,69 (Fig. 1C), making it unclear whether hypomyelination in these patients persists into adulthood. 70 Deficits in myelination may not be detected in adult patients due to a lack of MRI sensitivity, as illustrated in two preclinical studies (using MRIs much more sensitive than the ones used in clinical settings) in which the MRI signal could not detect a ∼20% increase in the percentage of myelinated axons in two interhemispheric commissures in adult rats (Fig. 1D). 8,9 Also, DTI alterations in the cerebral cortex and striatum are described in 11 patients (3–13 years old) with AHDS, and a reduction in the cerebral blood flow in the bilateral frontal cortex and the cerebellum is described in two patients. 71 The latter can be partly influenced by an altered blood vessel network. 72 In addition, MRS detected an increase in choline and myoinositol and a decrease in N-acetylaspartate levels in the supraventricular grey and white matter of patients with AHDS. 73
Another example supporting the clinical relevance of suffering suboptimal TH transport into the brain is the juvenile neurodegeneration and cerebral hypometabolism detected in the case of a 15-year-old patient harboring a missense mutation in the gene codifying for the TH cell membrane organic anion transporter polypeptide 1C1. 74 Notwithstanding, the relevance of this transporter for TH uptake by human brain cells is unclear since its expression in the blood-brain barrier is low, 75,76 and its role in other expressing neural cells, including astrocytes and tanycytes, 77 is undetermined.
Defects in TH metabolism
In the brain, deiodinases activate (type 2 deiodinase [D2]) or inactivate (D3) TH. 78 D2 is expressed in astrocytes and tanycytes, 79,80 whereas D3 is expressed in neurons. 81 Alterations in the function of these enzymes can unbalance TH action in the brain. 78 The Thr92Ala-DIO2 single nucleotide polymorphism reduces D2 catalytic activity, 82 leading to hypothyroidism in distinct brain areas in mice. 83 This defect in the D2 pathway has been linked to a higher proneness to suffering anxiety or depression. 84 Still, no MRI alterations have been described in this population. 85 Deiodinases are selenoproteins, and the rare selenocysteine amino acid is located in the catalytic active center of the enzymes, making it critical for enzymatic activity. Patients with loss-of-function mutations in the SBP2 gene, an important protein involved in the synthesis of all selenoproteins (including the deiodinases), exhibit severe neurological abnormalities, including impaired mental and motor coordination development and hearing loss; 86,87 however, routine MRIs have failed to detect brain alterations in these patients.
Disruption of TH Action in Adult Life
Hypothyroidism
Fortunately, with appropriate treatment, the effects of thyroid dysfunction in the adult brain are notable but reversible, so one would not expect to find severe permanent structural alterations in these patients. According to this hypothesis, subtle alterations in the white matter tracts, including the cingulum, the corpus callosum, and the corticospinal tracts, 88 –90 have been described in patients who also performed worse in cognitive assessments. Moreover, the concentration of the inhibitory neurotransmitter gamma-aminobutyric acid (GABA) is also reduced in the medial prefrontal and posterior cingulate cortices of adult patients with hypothyroidism. Still, the GABA levels normalized when patients received adequate levothyroxine (L-T4) treatment. A reduction in GABA is likely to cause an imbalance between the inhibitory and the excitatory brain networks, 91 which may result in many neurological symptoms, including mood alterations. Of note, patients on L-T4 exhibited fewer depressive symptoms and better memory function. 92
Similarly, the reduced levels of glutamate and myoinositol in the hippocampus of these patients reverted to normal values after adequate treatment. 93 Along these lines, two fMRI studies 41,43 detected a reduced connectivity between the cuneus and (i) the cerebellum (ii) the medial prefrontal cortex, and (iii) bilateral angular gyri, and in the posterior cingulate cortices (among other regions). This brain network is important for cognitive and self-awareness processes, and indeed, these alterations were accompanied by slightly longer reaction times and less accuracy in working memory tasks. A decrease in the global brain blood perfusion is also associated with high and low FT4 levels, suggesting that thyroid dysfunction could lead to stroke or dementia through suboptimal brain circulation. 94 However, a population study failed to associate TSH values (high/low) with cerebral small vessel disease. 95
A few studies found changes in the volume of the brain of patients with hypothyroidism. One described reduced total cerebellar and subcortical volumes of areas that regulate motor, cognitive, and affective function. 96 Another two studies describe a volume reduction in different areas of the hippocampus, 97 alongside significant alterations in cognitive and emotional scale scores. 42 Other brain areas may present decreased grey matter volumes and reduced activity, including the prefrontal and cingulate cortex, precuneus, and insula, which may lead to longer reaction times and lower performance accuracy, 98 suggesting impaired attentional/executive function in these patients. A study of patients with newly diagnosed hypothyroidism demonstrates a reduction in the cerebral cortex volumes in five regions, including the middle frontal gyrus and the supplementary motor area; 99 other areas also exhibit elevated activity. Similar results were found in patients with subclinical hypothyroidism, presenting reductions in the volume of the cerebral cortex in some areas of the frontal, central, and occipital gyrus 100 and elevated activity in some of these areas. In agreement, patients with major depressive disorders comorbid with subclinical hypothyroidism (high TSH vs healthy euthyroid controls) 101,102 exhibited reduced grey matter volume in areas including the left rectus and middle frontal gyrus and performed worse than controls in executive function tests.
Hyperthyroidism
Adult hyperthyroidism is mainly caused by autoimmune Grave’s disease, which involves hyperactivity of the thyroid gland, leading to high levels of circulating TH. 103,104 Cognitive impairment is common in adult patients with hyperthyroidism. 105 Compared to controls, adult patients with hyperthyroidism exhibited grey matter volume reductions in several brain regions, including the hippocampus, the left temporal pole, 106 the amygdala, 107 and the sulci. 108 Differently, one study found no reductions in the hypothalamus volume and limbic structures in these patients. 108 DTI parameters are also altered in white matter tracts that connect distal areas of the brain, 44,109 and one study shows altered functional connectivity between several brain networks. 102 In this study, cognitive functions such as visual retention, recognition of objects, and performance on neuropsychological tests were also reduced. Remarkably, after these patients received an anti-thyroid treatment (carbimazole), they improved the connectivity in the frontoparietal network (other networks remained altered), and some of the memory, executive, visuospatial, and motor functions. 110 More studies have described changes in the functional connectivity between different brain regions, 111 –114 including one that experimentally made the participants thyrotoxic (250 g L-T4 for 8 weeks), which caused increased connectivity between the left temporal pole and different parts of the cerebral cortex. 115
A compilation of studies has examined the brains of patients with Grave’s disease presenting ophthalmopathy and found alterations in the volume and connectivity between different brain areas 116 –120 and the neurovascular system. 121 A caveat of these studies is that this autoimmune condition involves various autoantigens and antibodies that can affect these patients’ optic nerves and brains, 122 making it difficult to attribute a causal relationship between the neuroimaging alterations and their TH status.
Aging
The prevalence of minor abnormalities in serum TSH and TH concentrations is common among elderly individuals. Cognitive impairments are particularly severe in older patients with hypothyroidism, presenting dementia and confusion in 33% and 18% of the cases. 123 Therefore, the possibility of an age-dependent association of thyroid function with brain alterations has been explored. For instance, an association between higher FT4 levels and MRI of ∼4600 participants aged 45 to 90 showed that the total intracranial and total brain and white matter volumes increased in younger individuals but decreased in the older group. 124 TSH levels in the high normal range are also associated with cortical atrophy and a higher proportion of infarct-like vascular lesions in male subjects aged 65–83. 125 Similarly, in ∼900 subjects aged 60 to 90, higher FT4 and reverse T3 were associated with a reduced hippocampus and amygdala volume. 126
Brain Organoids to Study TH Action in the Developing Human Brain
Human brain organoids recapitulate the gene expression programs of the fetal neocortex 127 and allow the study of fundamental aspects of its early development (this explains why they are often referred to as cerebral organoids). Although determined empirically, brain organoids seem to mirror the fetal cortex at gestational weeks 6.5–14. 128 However, long-term maturation (∼300 days in vitro) allows brain organoids to mature beyond the late mid-fetal stages. 129
Common to current hiPSCs-derived brain organoid protocols is that to promote the induction, proliferation, and maturation of the neural cell lineage, brain organoids require the addition of supraphysiological amounts of T3 to the medium. 128,130 Even higher doses of T3 for more extended periods are required to generate brain organoids containing robust populations of oligodendrocytes. 131,132 The induction cocktail also includes insulin-like growth factor 1 and platelet-derived growth factor-AA, which act downstream of the T3 signaling pathway. 133,134 These requirements represent a limitation to studies on the involvement of specific TH transporters in cellular processes. For instance, human oligodendrocytes express MCT8 with no other TH transporter to compensate for MCT8 deficiency, 135,136 but with the use of the current protocols, MCT8 mutations do not affect the in vitro differentiation of hiPSCs into oligodendrocytes. 137
An array of hiPSCs derived from patients with thyroid genetic conditions, including mutant THRB, THRA, and SLC16A2 (encoding MCT8), are currently available 49,138 –140 and can be used to generate brain organoids. Such disease-specific brain organoids can then be used to explore mechanistic explanations for the pathophysiology of these disorders. Following this approach, MCT8-deficient brain organoids—from hiPSCs obtained from corresponding patients—have demonstrated that MCT8 mediates the bulk of T3 transport in developing neural cells, 141 providing evidence that the role of this transporter in the human brain goes beyond facilitating the passage of TH through the blood-brain barrier. 140 This also seems to be the case in neurons, as demonstrated in a mouse study showing that, partly facilitated by MCT8, TH can act in these cells, entering hidden inside endosomes that act akin to a Trojan horse—protecting TH from degradation from the axonal termini to the nucleus. 81 Due to the altered T3 transport, MCT8-deficient brain organoids exhibit altered neurogenesis, 141 pointing to an MCT8-mediated TH transport into the neural precursor cells (the source of most human cortical neurons 142 ) that can trigger developmental programs in these cells. 143 This is supported by the fact that MCT8 is expressed in neural precursor cells in fetal brains and brain organoids. 77,144,145 Further evidence comes from a study that used hiPSCs from patients with RTHα showing premature neurogenesis and neural precursor cell depletion. 49
Regulation of gene expression is central to our understanding of how TH acts in the developing brain, but most of what we know is inferred from mouse studies. 79,146 –151 Brain organoids have shown that TH in these models regulates genes critical for cerebral cortex development. 141 Many of these genes are altered in MCT8-deficient brain organoids, making the case that TH action could be severely altered during the neurodevelopment of these patients.
In addition, studies on MCT8-deficient brain organoids have validated the TH-analogs 3,5-diiodothyropropionic acid and 3,3’,5-triiodothyroacetic acid as treatments that can elicit similar responses as TH in human MCT8-deficient neural cells. 141 These findings are exciting, considering that treating intraamniotically with a high dose of L-T4 a fetus with MCT8-deficiency from gestational age of 18 until birth at 35 weeks 22 improved myelination (Fig. 1B) and neuromotor and neurocognitive function. The results from MCT8-deficient brain organoids support the idea that early prenatal treatment with TH analogs that can be available to a fetus when given to the mother 152 might further rescue the AHDS phenotype.
Conclusion
Neuroimaging studies strengthen the concept that the human brain responds to TH and that TH is important for human brain development. The alterations in children born to mothers with different degrees of gestational hypothyroidism or who developed hypothyroidism early in life are noteworthy, affecting multiple brain regions and circuits. The cerebral cortex, hippocampus, cerebellum, interhemispheric and corticospinal tracts, and associative nuclei are among the most sensitive ones. The data connecting such changes to poor neurological outcomes in adult patients with hypothyroidism represent an objective link between thyroid-specific functional brain alterations and behavior. Neuroimaging studies prove that alterations in the brain are in play in the syndromes of impaired sensitivity to TH. However, many of the studies reviewed here are based on a small number of subjects (partly due to the rare clinical occurrence of some conditions), and prospective investigations need to include more subjects with detailed thyroid function test monitoring and experimental paradigms to evaluate neurological outcomes.
An approach for studying the mechanisms of TH action in the developing human brain constitutes a “holy grail” for the field. Brain organoids fit this purpose and have highlighted the importance of TH for early human neurogenesis, cerebral cortex maturation, and myelination. Observations in specific brain organoids modeling thyroid genetic diseases carry significant physiological implications and constitute a new groundwork for developing new treatments. Many scientific efforts aim to improve the protocols and experimental designs necessary to level up the current neuroimaging and stem cell technologies. Future advances will transform the way we investigate how TH orchestrates human brain development and regulates its function through life—ultimately helping to improve the treatment options for patients with hypothyroidism or inherited thyroid diseases.
Footnotes
Acknowledgments
The author thanks Profs. Samuel Refetoff and Antonio Bianco for their critical reading of the article, and Deb Werner for her assistance with some aspects of the search strategy.
Author Contribution
F.S.-L. is solely responsible for writing, editing, and approving this review article.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
National Institutes of Health grants