
Abstract
Background:
The rearranged during transfection (RET) proto-oncogene fusion is common in papillary thyroid cancer (PTC), varying across ethnic groups. However, comprehensive comparisons of RET fusion types are limited. This study aims to identify predominant RET fusions and analyze their clinicopathological characteristics in a cohort of Chinese thyroid cancer cases.
Methods:
This single-center retrospective cohort study analyzed thyroid cancer data, utilizing next-generation sequencing on formalin-fixed, paraffin-embedded tissue samples. Detailed clinicopathological data of thyroid cancer cases with RET fusions were collected.
Results:
Among 2300 thyroid cancer cases, RET fusions were exclusively found in PTC or differentiated high-grade thyroid carcinoma (DHGTC) cases (2234 cases), absent in other types (66 cases). Of the 2234 PTC or DHGTC cases, 113 (5.06%) exhibited RET fusions, including 100 primary cases. Coiled-coil domain containing 6 (CCDC6)-RET fusions predominated (78.0%, 78/100), with nuclear receptor coactivator 4 (NCOA4)-RET fusions representing 22.0% (22/100). NCOA4-RET fusions were more prevalent in patients aged 45 years and older (54.5% vs. 28.2%, p = 0.021) and DHGTC cases (p < 0.05) and associated with higher rates of lymph node metastases (90.9% vs. 67.9%, p = 0.032). CCDC6-RET fusion exhibited a higher prevalence of Hashimoto’s thyroiditis (HT) (67.9% vs. 22.7%, p < 0.001) and elevated thyroglobulin antibody levels (14.11 [1.86–174.32] IU/mL vs. 2.01 [1.14–15.41] IU/mL, p = 0.018). Moreover, CCDC6-RET fusion predominantly occurred in classical PTC (56.4%, 44/78) and infiltrative follicular PTC (17.9%, 14/78), whereas NCOA4-RET fusion was more frequent in classical PTC (36.4%, 8/22), solid PTC (27.3%, 6/22), and DHGTC (27.3%, 6/22). RET fusions with compound mutations were associated with older age (≥45 years) and bilateral thyroid involvement. Follow-up data showed a higher recurrence rate in the RET fusion group compared with the BRAFV600E mutation group (5.0% vs. 0.0%, p = 0.018). Although the NCOA4-RET group showed a numerically higher recurrence rate compared with CCDC6-RET (9.1% vs. 3.8%), this difference was not statistically significant (p = 0.559).
Conclusions:
RET fusions are specific to PTC or DHGTC cases among Chinese thyroid cancer cases. CCDC6-RET and NCOA4-RET fusions exhibited distinct clinicopathological features, with NCOA4-RET being more aggressive.
Introduction
The rearranged during transfection (RET) proto-oncogene plays a pivotal role in thyroid cancers, characterized by the following two aberrant forms: RET mutation or fusion. 1,2 RET fusions are typically identified in 6.80% of patients with papillary thyroid cancer (PTC), with sporadic occurrences in poorly differentiated thyroid cancer (PDTC) and rare cases of anaplastic thyroid cancer (ATC). 3 –6 Compared to the BRAFV600E mutation, RET fusions are associated with greater aggressiveness, predisposing patients to lymph node and distant metastases in thyroid cancer. 7,8 In addition, RET fusions are related to early recurrence and reduced 5-year disease-free survival rates in thyroid cancer patients. 8
Several studies have demonstrated that RET rearrangements in PTC involve diverse partner genes. 9 –11 Among these, coiled-coil domain containing 6 (CCDC6) and nuclear receptor coactivator 4 (NCOA4) are the most prevalent, accounting for 90% of cases. 12,13 Notably, CCDC6-RET and NCOA4-RET fusions exhibit distinct characteristics in PTC. Specifically, CCDC6-RET fusion is more frequently observed in classical PTC and sporadic thyroid cancer, whereas NCOA4-RET fusion is associated with solid PTC and an advanced stage of disease at diagnosis. 1,14,15
Although RET fusions have been documented in PTC patients of diverse ethnic backgrounds, reports on Chinese thyroid cancer patients remain limited. 16,17 Moreover, the distinct characteristics of CCDC6-RET and NCOA4-RET fusions necessitate further investigation. Therefore, the objective of this study is to determine the predominant RET gene fusions (CCDC6-RET and NCOA4-RET) and analyze their clinicopathological and histological features in a large cohort of Chinese individuals with thyroid cancer.
Materials and Methods
Case identification
This retrospective cohort study collected data from 2300 patients with thyroid cancer who underwent thyroidectomy and next-generation sequencing (NGS) testing at the Fudan University Shanghai Cancer Center from March 2021 to October 2022. Since 2020, NGS has been routinely performed for patients with thyroid cancer undergoing thyroidectomy at our center.
Among the 2300 cases assessed, 2234 were PTC or differentiated high-grade thyroid carcinoma (DHGTC), 24 were medullary thyroid cancer (MTC), 35 were follicular thyroid cancer (FTC), 6 were PDTC, and 1 was ATC. Of these, 113 cases positive for RET fusions were included, with 100 cases of primary tumors confirmed and analyzed and 13 cases of metastasis without primary tumors excluded from this study. Exclusion criteria were as follows: (1) RET fusion-negative (2187 cases) and (2) metastatic tumors without primary tumors in RET fusion-positive (13 cases) (Fig. 1). Clinical and pathological data, including sex, age, primary tumor size, pathological diagnosis, NGS results, presence of distant metastases, thyroid biochemical variables prior to surgical treatment, and date of recurrence, were extracted from electronic medical records.

Patient flow diagram. ATC, anaplastic thyroid cancer; DHGTC, differentiated high-grade thyroid carcinoma; FTC, follicular thyroid cancer; MTC, medullary thyroid cancer; PDTC, poorly differentiated thyroid cancer; PTC, papillary thyroid cancer.
The clinical stage was determined according to the 8th edition of the American Joint Committee on Cancer TNM staging system for thyroid cancer. 18 Histological evaluation was performed by two experienced pathologists and categorized based on the 5th edition of the World Health Organization (WHO) classification. 19 Moreover, RET fusion tumors were classified into BRAF-like or RAS-like subtypes. 19 Ethical approval for this study was obtained from the Ethics Committee of our hospital (Approval Number: 050432-4-2307E). Informed consent was obtained from each patient for the use of their information in this research.
RNA extraction
The postoperative thyroid tissues containing calcifications were decalcified in ethylenediaminetetraacetic acid solution for 12 hours before being fixed in 4% paraformaldehyde and subsequently embedded in paraffin. Tumor regions were assessed by pathologists using hematoxylin and eosin staining. Total RNA was extracted from formalin-fixed paraffin-embedded (FFPE) samples using the QIAamp RNeasy Kit (Qiagen). Detailed RNA quantity and quality information is provided in Supplementary Table S1. RNA concentration, measured using a Qubit 4.0 Fluorometer (Thermo Fisher Scientific), had a median of 36.60 ng/μL (interquartile range: 22.15–58.85 ng/μL), and the median 260/280 ratio, assessed by NanoDrop 2000 spectrophotometer (Thermo Fisher Scientific), was 1.90 (interquartile range: 1.87–1.95). All procedures followed manufacturer’s instructions.
Multiplex PCR-based library preparation and sequencing
Sequencing libraries were generated using the thyroid cancer multigene panel (RigenBio), specifically designed for amplicon-based NGS. A minimum of 8 ng of RNA was reverse transcribed to complementary DNA and then subjected to two rounds of multiplex PCR amplification, resulting in libraries with unique indexes and adapters. The libraries were purified at various concentrations using magnetic beads (0.8×, 1.2×), quantified with a Qubit 4.0 Fluorometer (Thermo Fisher Scientific), and analyzed for fragment sizes with an Agilent 2100 Bioanalyzer (Agilent Technologies). Subsequently, the qualified libraries underwent paired-end sequencing with 150-bp reads on the NextSeq 550 platform (Illumina). The concentrations of the library are detailed in Supplementary Table S1. The RigenBio thyroid cancer multigene panel enabled the detection of mutations, insertions, deletions, and fusions in a total of 28 genes listed in Supplementary Table S2. All experimental procedures were conducted following the manufacturer’s protocols.
Bioinformatics analysis
Raw sequencing data were processed to remove adapters and low-quality regions using Trimmomatic (version 0.38). The cleaned data were then aligned to the human reference genome (hg19) using the Burrows–Wheeler Aligner tool (version 0.7.10). Single nucleotide variants and insertion/deletion variants (indels) were identified using VarScan (version 2.3.9), whereas gene fusions were detected with FusionMap. Variants and genotype calls were annotated using ANNOVAR and the Variant Effect Predictor. This annotation process included the Sorting Intolerant From Tolerant score, conservation scores such as PolyPhen, and clinically relevant information sourced from ClinVar.
Data analysis
The primary analysis focused on the incidence of RET fusions in Chinese thyroid cancer patients, comparing the distinct clinicopathological features between the CCDC6-RET and NCOA4-RET fusion groups. Hashimoto’s thyroiditis (HT) was diagnosed based on histopathological features, which included interstitial infiltration of hematopoietic mononuclear cells, primarily composed of lymphocytes, plasma cells, and macrophages, as well as the formation of lymphoid follicles. 20
The secondary analysis investigated the recurrence rates between the two RET fusion groups, considering the limited availability of follow-up data. In this study, recurrence was defined as the reappearance of structural and biochemical evidence of thyroid cancer in a patient who was initially disease-free postsurgery, necessitating resurgery. 21 Disease persistence was defined as structural and biochemical residual diseases after the initial surgery. 21 Patients with persistent thyroid cancer were not considered to have recurred during follow-up.
Statistical analysis
Statistical analysis was performed using Statistical Package for Social Sciences 25.0 (IBM Corporation, USA). The normality of variables was assessed using the Kolmogorov–Smirnov test. Normally distributed continuous variables were presented as mean ± standard deviation, whereas non-normally distributed variables were expressed as medians with interquartile ranges (25th–75th percentiles). Categorical variables were reported as counts and percentages. Continuous variables were compared using Student’s t-test or Mann–Whitney U test, and categorical variables were compared using chi-squared or Fisher’s exact tests. Univariable analyses were performed to compare clinicopathologic and histological features between CCDC6-RET and NCOA4-RET fusions in order to identify independent factors associated with RET fusion. Variables that showed a predetermined statistical difference were then included in multivariable analysis.
To evaluate the risk of disease recurrence associated with RET fusions, we established a control group consisting of a comparable number of cases with the BRAFV600E mutation and compared the time to disease recurrence between the RET and BRAF groups. In our study, the incidence of the BRAFV600E mutation was 79.57% (1830/2300), with complete medical records for 1640 primary cases. Propensity score matching was performed to balance baseline variables between the RET (n = 100) and BRAF (n = 1640) groups, using a 1:1 protocol with a caliper width equal to 0.01 of the standard deviation of the logit of the propensity score. Kaplan–Meier survival curve analysis was used to assess cumulative thyroid cancer recurrence based on various fusions or mutations, with differences analyzed using the log-rank test.
Results were presented as odds ratios (OR) with confidence intervals (CI). Bonferroni correction was applied for multiple tests and pairwise comparisons between groups. Statistical significance was set at two-sided p-values <0.05.
Results
Clinicopathological features of the CCDC6-RET and NCOA4-RET groups
Out of 2300 cases of thyroid cancer, RET fusions were exclusively identified in PTC or DHGTC cases (2234 cases), with no presence in other thyroid cancer types (66 cases). Among the 2234 PTC or DHGTC cases, 113 (5.06%) exhibited RET fusions, with 88 (3.94%) showing CCDC6-RET fusion and 25 (1.12%) showing NCOA4-RET fusion. This included 100 primary tumors and 13 metastatic tumors without primary tumors. Specifically, this study analyzed a cohort of 100 cases of primary PTC or DHGTC with RET fusions, where 78.0% (78/100) were CCDC6-RET fusions and 22.0% (22/100) were NCOA4-RET fusions (Fig. 1).
Compared with CCDC6-RET fusion, NCOA4-RET fusion was significantly more prevalent in patients aged ≥45 years (54.5% vs. 28.2%) (p = 0.021) and was associated with a higher incidence of lymph node metastasis (LNM) (90.0% vs. 67.9%) (p = 0.032) (Table 1). Multivariable analysis identified age ≥45 years (OR = 3.916, 95% CI = 1.295–11.843, p = 0.016) and LNM (OR = 6.103, 95% CI = 1.093–34.076, p = 0.039) as independent factors associated with NCOA4-RET fusion (Supplementary Table S3).
Clinicopathologic Features of RET Fusions
Italicized p-values are statistically significant.
Comparison with other PTC subtypes, and the p-value was adjusted by Bonferroni test. Therefore, p < 0.05/8 was considered as statistically significant.
The staging system used is the 8th edition of the American Joint Committee on Cancer (AJCC) TNM staging system for thyroid cancer (AJCC, 2017). 18 CCDC6, coiled-coil domain containing 6; LNM, lymph node metastasis; N, lymph node status; NCOA4, nuclear receptor coactivator 4; RET, rearranged during transfection; T, primary tumor.
RET fusions and thyroid function indicators
We compared thyroid biochemical variables prior to surgical treatment between the CCDC6-RET and NCOA4-RET groups. Thyroglobulin antibody (TgAb) levels were significantly higher in the CCDC6-RET group compared with the NCOA4-RET group (14.11 [1.86–174.32] IU/mL vs. 2.01 [1.14–15.41] IU/mL) (p = 0.018). In addition, the CCDC6-RET group tended to have higher thyroid peroxidase antibody (TPOAb) levels than the NCOA4-RET group (5.47 [1.00–198.50] IU/mL vs. 1.11 [1.00–8.79] IU/mL), although this difference did not reach statistical significance (p = 0.055). No significant differences were observed in free triiodothyronine (FT3), free thyroxine (FT4), thyrotropin (TSH), or thyroglobulin (Tg) levels between the two groups (Table 2).
Thyroid Function Indicators of the Study Cohort
Italicized p-values are statistically significant.
FT3, free triiodothyronine; FT4, free thyroxine; Tg, thyroglobulin; TgAb, thyroglobulin antibody; TPOAb, thyroid peroxidase antibody; TSH, thyrotropin.
Histological features of cases with RET fusions
The distribution of RET fusion among histological types of thyroid cancers is summarized in Supplementary Table S4. The incidence of RET fusions varied among different PTC subtypes: 15.4% (8/52) for diffuse sclerosing PTC (DS-PTC), 7.0% (14/199) for solid PTC, 6.7% (1/15) for clear-cell PTC, 4.0% (52/1286) for classical PTC, 3.2% (14/439) for follicular PTC (FVPTC), and 3.0% (2/66) for oncocytic PTC. In addition, RET fusion was detected in 14.5% (9/62) of DHGTC cases. After analyzing the nuclear findings of PTC, all RET fusion cases were classified as BRAF-like tumors.
Among the 100 primary PTC or DHGTC cases, the CCDC6-RET and NCOA4-RET groups exhibited distinct pathological subtypes. Specifically, CCDC6-RET fusion cases primarily showed classical PTC (56.4%, 44/78) or infiltrative FVPTC (17.9%, 14/78), whereas NCOA4-RET fusion cases were associated with classical PTC (36.4%, 8/22), solid PTC (27.3%, 6/22), or DHGTC (27.3%, 6/22) (Fig. 2). Notably, among DHGTC cases with PTC growth patterns, the prevalence of NCOA4-RET fusion (6 cases) was significantly higher compared with CCDC6-RET fusion (3 cases) (p = 0.003) (Table 3). Multivariable analysis revealed DHGTC (OR = 11.847, 95% CI = 2.184–64.265, p = 0.004) as an independent factor associated with NCOA4-RET fusion (Supplementary Table S3). The CCDC6-RET group exhibited a higher prevalence of HT compared with the NCOA4-RET group (67.9% vs. 22.7%) (p < 0.001) (Table 3). Further details regarding the pathological and morphological characteristics of these subtypes are provided in Supplementary Table S5.

Pathological features of primary PTC or DHGTC with RET fusion.
Histological Features of RET Fusions
Italicized p-values are statistically significant.
Comparison with other PTC subtypes and the p-value was adjusted by Bonferroni test. Therefore, p < 0.05/8 was considered as statistically significant.
DHGTC, differentiated high-grade thyroid carcinoma; DS-PTC, diffuse sclerosing PTC; FVPTC, follicular PTC; PTC, papillary thyroid cancer.
Compound mutations in PTC with RET fusions
In PTC, five cases with RET fusions also exhibited other gene mutations of uncertain significance. These compound mutations included TERT (c.−157T > G, c.−112C > T), CHEK2P2 (n.243T > G), and CTNNB1 (c.2217G > A) in four CCDC6-RET fusion cases and TP53 (c.1120G > A) in one NCOA4-RET fusion case. Notably, cases of RET fusions with compound mutations were associated with older age (≥45 years, 80.0% vs. 20.0%) (p = 0.044) and a higher incidence of bilateral thyroid involvement (60.0% vs. 9.5%) (p = 0.012) compared with those without compound mutations.
Recurrence of PTC or DHGTC with RET fusions
Following propensity score matching, the study included 100 patients with BRAFV600E mutation. The RET and matched BRAF groups demonstrated similar baseline characteristics postmatching (Supplementary Table S6). The median follow-up periods were 15.2 (6.4–23.2) months for the RET group and 17.0 (6.1–24.0) months for the BRAF group. Specifically, median follow-up periods for the CCDC6-RET and NCOA4-RET groups were 14.1 (4.6–22.2) months and 18.1 (11.0–26.2) months, respectively. Disease persistence was observed in two cases in the CCDC6-RET group, one in the NCOA4-RET group, and three in the BRAF group. No patients with BRAFV600E mutation experienced recurrence. Among patients with RET fusions, five cases (5.0%, 5/100) experienced recurrence between 7.1 and 21.9 months (Table 4). Specifically, two (9.1%, 2/22) cases with NCOA4-RET fusion and three (3.8%, 3/78) cases with CCDC6-RET fusion experienced recurrence. The RET group exhibited a significantly higher recurrence rate than the BRAF group (5.0% vs. 0.0%, p = 0.018) (Fig. 3). Bonferroni correction (p < 0.05/3) indicated a significantly higher recurrence rate in the NCOA4-RET group (9.1% vs. 0.0%, p = 0.004) compared with the BRAF group but not in the CCDC6-RET group (3.8% vs. 0.0%, p = 0.033). Although the recurrence rate in the NCOA4-RET group was numerically higher than that in the CCDC6-RET group (9.1% vs. 3.8%), there was no statistical difference (p = 0.559) (Fig. 4).

Kaplan–Meier curve comparing recurrence rates between RET fusions and BRAFV600E mutation.
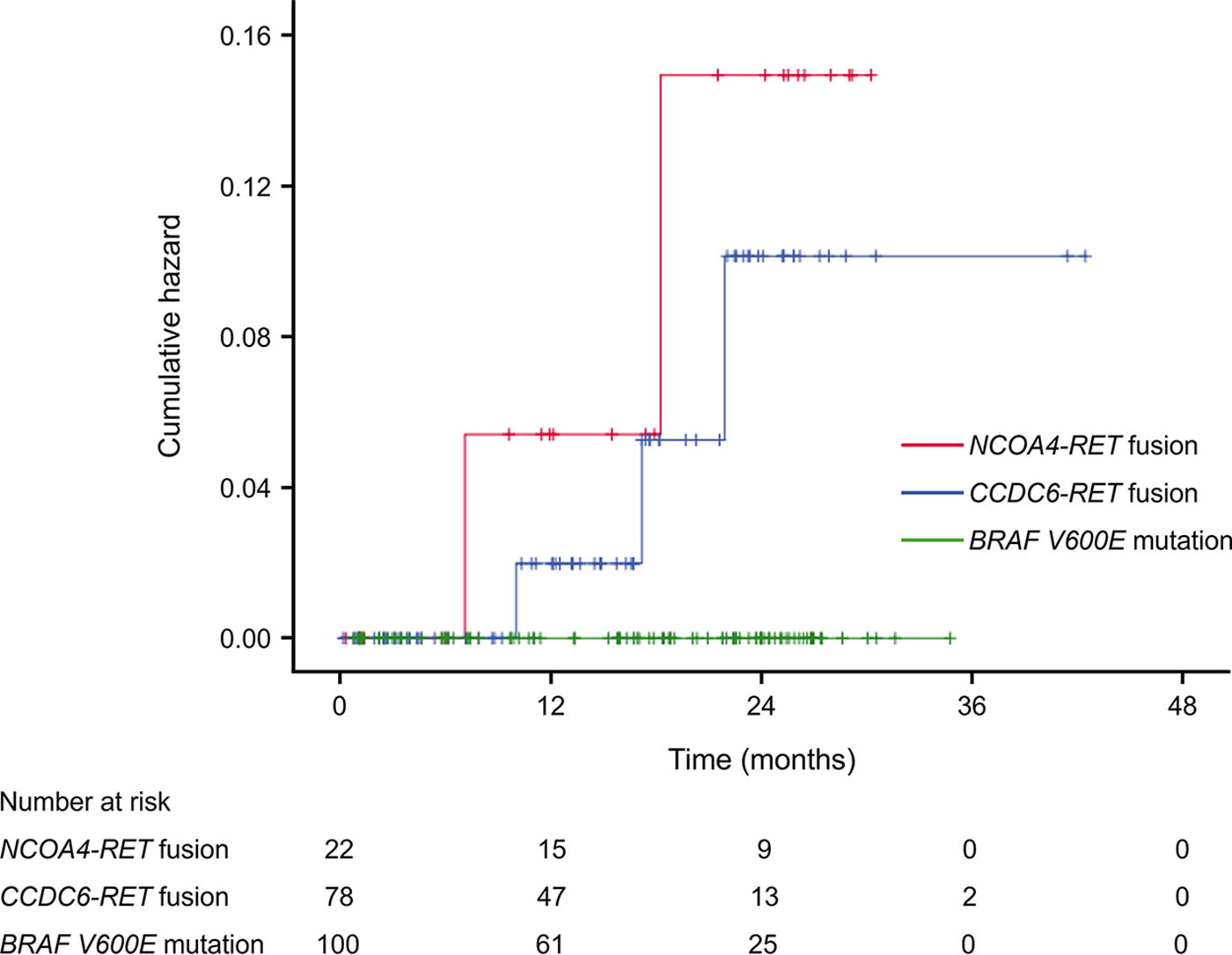
Kaplan–Meier curve comparing recurrence rates among CCDC6-RET fusion, NCOA4-RET fusion, and BRAFV600E mutation.
Clinical Characteristics of Recurrent Cases with RET Fusions
B, bilateral thyroid gland; L, left thyroid gland; R, right thyroid gland; TNM, tumor-node-metastasis.
Discussion
RET fusion has been identified as a crucial gene in PTC. Previous research has highlighted that there are no significant differences in the prevalence of RET fusion between Western populations (ranging from 2.50% to 8.70%) and Eastern populations (ranging from 4.35% to 10.81%) with sporadic thyroid cancer. 7,8,22 –30 However, the incidence of RET fusion notably escalates to 55.0% in pediatric patients with thyroid cancer induced by nuclear exposure. 31 Data from The Cancer Genome Atlas (TCGA) database have revealed that RET fusion occurs in 6.80% (33/485) of PTC cases, with CCDC6-RET fusion identified in 4.33% (21/485) and NCOA4-RET fusion in 1.03% (5/485) of cases. 3 Our previous study found that the incidence of RET fusion was 7.8% in 217 PTC FFPE samples. 32 In the present expanded study involving 2234 PTC or DHGTC FFPE samples, RET fusions were detected in 5.06%, with CCDC6-RET fusions in 3.94% (88/2234) and NCOA4-RET fusions in 1.12% (25/2234) of cases. These findings are consistent with TCGA data and indicate that there is no difference in the incidence of RET fusion between Chinese and Western populations.
Age is an important factor associated with the prevalence of PTC cases with RET fusion. 33,34 Previous studies have indicated a higher prevalence of RET rearrangements in thyroid cancer patients under 45 years old. 28,35 However, differences in age distribution between CCDC6-RET and NCOA4-RET fusions remain unclear. A meta-analysis suggested that children and adolescents exhibit a higher proportion of NCOA4-RET fusions compared with adults. 33 In contrast, our study found a notably higher proportion of patients older than 45 years in the NCOA4-RET group compared with the CCDC6-RET group. In addition, age over 45 years is independently related to NCOA4-RET fusion. Given the limited research in this area, further investigations are warranted.
TgAb and TPOAb levels are essential markers for diagnosing HT, a condition known to increase the risk of developing PTC. 36,37 Elevated TgAb levels (>1150 IU/mL) have been associated with central lymph node metastasis in patients with concurrent PTC and HT. 38 However, the differences in TPOAb and TgAb levels between CCDC6-RET and NCOA4-RET fusions have not been extensively studied. Our research found significantly higher TgAb levels in the CCDC6-RET group compared with the NCOA4-RET group. In cases of CCDC6-RET fusion, elevated TgAb levels are associated with a high prevalence of HT. This could be attributed to the following two possible mechanisms: (1) the inflammatory process might facilitate the formation of CCDC6-RET rearrangements or (2) the CCDC6-RET fusion might directly influence the inflammatory response in PTC with HT. 39,40 Further studies are necessary to ascertain whether CCDC6-RET fusion cases with HT and elevated TgAb levels have a better prognosis due to immune system activation.
Previous studies have highlighted that CCDC6-RET fusions frequently occur in classical PTC, 41 infiltrative FVPTC, 42,43 hobnail PTC, 44,45 and DS-PTC, 46 whereas NCOA4-RET fusions are more commonly found in solid PTC 47,48 and have also been reported in DS-PTC. 49,50 Our investigation revealed that both CCDC6-RET and NCOA4-RET fusions were predominantly detected in classical PTC. Interestingly, CCDC6-RET fusion was more often found in infiltrative FVPTC, whereas NCOA4-RET fusion was frequently observed in solid PTC and DHGTC. Multivariable analysis confirmed an independent association between NCOA4-RET fusion and DHGTC. Importantly, all RET fusions were classified as BRAF-like tumors. According to the 5th WHO classification, DHGTC was categorized as a highly aggressive form of thyroid cancer with a significantly poor 5-year overall survival rate. 50 –52 This implies that NCOA4-RET fusion may contribute to the dedifferentiation of PTC, leading to a poorer prognosis. Given that DHGTC typically shows resistance to radioactive iodine, patients with RET fusions in DHGTC might benefit from treatment with RET kinase inhibitors. 4,53
PTC harboring driver gene fusions, co-occurring with other gene mutations, has been documented to have a higher likelihood of progressing into dedifferentiated and aggressive forms of thyroid cancers. 54,55 RET fusions and BRAF mutations, the most common mutations in PTC, are generally mutually exclusive. 26 However, a few reports have documented their co-occurrence in advanced-stage PTC, which is associated with a poor prognosis. 56 –58 In PTC, TERT mutation is a frequent concomitant alteration with RET fusion, occurring in up to 31.11% (14/45) of cases. 59 RET fusions combined with TERT hotspot mutations (c.−124C>T or c.−146C>T) have been identified as indicators of progression from PTC to PDTC and even to ATC. 60 In our study, no TERT hotspot or BRAF mutations were detected in cases of PTC or DHGTC with RET fusion. However, we observed a low incidence (5%, 5/100) of compound mutations with uncertain significance. RET fusions with compound mutations were associated with older age (≥45 years) and a higher incidence of bilateral thyroid involvement.
Previous studies have demonstrated that PTC with RET fusions exhibited the highest prevalence of LNM, compared with PTC with BRAF or RAS mutations. 61 Specifically, PTC with RET fusions (involving CCDC6 and NCOA4) was significantly associated with LNM in young adults. 62 Recent findings suggest that the NCOA4-RET fusion results in a higher incidence of LNM than CCDC6-RET fusion. 24,41 Similarly, our study found a significantly higher incidence of LNM in the NCOA4-RET group compared with the CCDC6-RET group.
In a recent study of 57 patients with PTC over a 250-month follow-up, the recurrence rate did not significantly differ between the CCDC6-RET group and the NCOA4-RET group, with both at 33.33%. 24 Our follow-up data indicated an overall recurrence rate of 5% (5/100) for RET fusions. Specifically, the NCOA4-RET group exhibited a higher recurrence rate (9.1%, 2/22) than the CCDC6-RET group (3.8%, 3/78). However, this difference was not statistically significant. Furthermore, comparing recurrence rates between the RET and BRAF groups, a higher recurrence rate was observed in the RET group, suggesting a potentially poorer prognosis. Recurrence rates for the BRAFV600E mutation have been reported to range from 5.45% to 25.8%. 63,64 However, none of the BRAFV600E mutation cases in our study experienced recurrence. Given the short follow-up periods for the BRAFV600E mutated thyroid cancer cases in our study, these conclusions should be interpreted cautiously, and further research is necessary to validate these findings.
Limitations
This study has several limitations, including its inherent retrospective design. This study focuses on RET fusions, omitting other fusion genes like neurotrophic tropomyosin receptor kinase fusion, which have also been reported in thyroid cancer. Moreover, the study’s scope was limited to the two most common RET fusion types (CCDC6-RET and NCOA4-RET), as other RET fusion types were not included in our multigene panel. Furthermore, the low incidence of NCOA4-RET fusion in thyroid cancer resulted in a small sample size, potentially leading to statistical underpowering for some comparisons and analyses. We acknowledge that the sample size did not meet the recommended criteria for multivariable analysis, which typically requires at least 10 events per variable. 65,66 Consequently, caution is warranted in interpreting these findings. In addition, the study was limited by short-term follow-up and a restricted number of cases analyzed for recurrence rates. The survival curve analysis was based on limited data, precluding the conduct of Cox regression analysis. Future investigations should incorporate long-term follow-up to more accurately compare recurrence rates between CCDC6-RET and NCOA4-RET fusions.
Conclusion
This single-center study examined the most common RET fusions in thyroid cancer and provided an in-depth analysis of their histological and clinicopathological characteristics. RET fusions were specifically found in PTC and DHGTC and exhibited distinct clinicopathological features between the CCDC6-RET and NCOA4-RET fusion groups. Notably, the NCOA4-RET group was associated with higher aggressiveness than the CCDC6-RET group. These findings may inform risk stratification of thyroid cancers with RET fusions and highlight the need for timely appropriate treatment.
Footnotes
Authors’ Contributions
Z.W.: Conceptualization, data analysis, methodology, experiment performance, writing—original draft, review, and editing. Q.Y., L.B., H.C., T.X., M.R., Q.W., C.Y., R.W., Y.W., B.P., Q.B.: Experiment performance. Xiaoyan Z.: Conceptualization, funding acquisition, supervision, methodology, writing—original draft, review, and editing. Xiaoli Z.: Conceptualization, funding acquisition, supervision, methodology, writing—original draft, review, and editing.
Author Disclosure Statement
There are no competing financial interests.
Funding Information
This work was supported by the Innovation Program of Shanghai Science and Technology Committee (
Supplementary Material
Supplementary Table S1
Supplementary Table S2
Supplementary Table S3
Supplementary Table S4
Supplementary Table S5
Supplementary Table S6