
Abstract
Background:
Several meta-analyses have found no association between Graves’ disease (GD) and an increased risk of incident diabetes; however, the intricate relationship between thyroid dysfunction and diabetes remains underexplored. In this study, we aimed to evaluate the risk of incident type 2 diabetes (T2DM) in a population newly diagnosed with GD, focusing on different treatment methods and treatment duration.
Methods:
This was a retrospective population-based study utilizing data from the Korean National Health Insurance database. We included 36,243 patients with GD and 36,243 controls, matched with age and sex. We calculated the incidence of T2DM among patients and controls based on treatment methods, such as medical therapy, radioactive iodine therapy (RAIT), and surgery. We examined the cumulative dose and duration of antithyroid drug (ATD) use for each patient.
Results:
The majority of patients (34,867, 96.2%) were treated with ATDs, followed by RAIT (1093 patients, 3%), and surgery (283 patients, 0.8%). After adjusting for age; sex; income; comorbidities, including hypertension, dyslipidemia, and cancer; body mass index; smoking; drinking; and exercise, patients with GD exhibited a higher risk of developing diabetes (hazard ratio [HR] = 1.13 [95% confidence interval 1.06–1.21]) than controls (5.1% vs. 4.5%, respectively). While the risk was the highest within the first six months after GD diagnosis (HR = 3.21), it was significant between six months and two years (HR = 1.36) and was comparable with the controls two years after GD diagnosis (HR = 0.93). A longer duration of ATD treatment and a higher cumulative dose were associated with an increased risk of diabetes. However, the risks for T2DM did not differ according to treatment modality or clinical outcomes, which was probably related to the small number of patients in each subgroup.
Conclusions:
Our findings highlight the negative impact of GD on the development of T2DM. Patients newly diagnosed with GD can be considered for diabetes screening to facilitate early detection and intervention.
Introduction
In the last decade, the prevalence of diabetes mellitus (DM) has doubled in the adult population, from 4.7% in 1980 to 10.5% in 2021. 1 Its incidence has rapidly increased in the Republic of Korea, 2,3 particularly among individuals aged <40 years. 4 The United States Preventive Services Task Force (USPSTF) and the Korean Diabetes Association (KDA) have updated and lowered the age for screening diabetes from 40 to 35 years. This is based on the data indicating a sharp increase in the incidence of diabetes at the age of 35 years and the benefits of early interventions for newly diagnosed diabetes. 5,6
Thyroid hormones play a significant role in glucose metabolism and its regulation. Recently, meta-analyses of prospective studies investigated the association between thyroid disease and the risk of incident diabetes. 7 –9 One of them reported no elevation in the risk for diabetes in patients with subclinical hypothyroidism or hyperthyroidism. 7 For overt thyroid diseases, patients with hypothyroidism face a higher risk (17–26%) of developing diabetes, 8,9 whereas the role of hyperthyroidism in the onset of diabetes remains inconclusive. A study utilizing nationwide Danish health registers assessed the risk of various comorbidities before and after hyperthyroidism diagnosis, concluding a heightened risk of diabetes (hazard ratio [HR] = 1.46). 10 Another study employing continuous glucose monitoring (CGM) demonstrated that individuals with uncontrolled Graves’ disease (GD), even those with normal glucose metabolism, exhibited greater glucose variability than healthy controls. 11
Considering that GD and type 1 DM (T1DM) are frequently co-occurring autoimmune conditions, the American Diabetes Association recommends evaluating thyroid function upon T1DM diagnosis and subsequently every 1–2 years, even for asymptomatic individuals. 12 However, the risk of developing type 2 DM (T2DM) in GD has not been thoroughly investigated. 13 Given that individuals with GD are typically younger and exhibit an elevated risk of cardiovascular complications compared to the general population, 14,15 it is important to ascertain whether GD itself constitutes a risk factor for diabetes and whether it warrants diabetes screening.
Herein, we aimed to determine whether GD increases the risk of new-onset T2DM. We also assessed the risk of incident T2DM according to treatment modality for GD and the period from GD diagnosis, using nationally representative data from the National Health Information Database (NHID).
Methods
Data source
This retrospective population-based cohort study used data from the Korean National Health Insurance Service (NHIS) database, covering approximately 97% of the Korean population. It encompasses anonymized personal data, health examination details, demographics, diagnoses coded according to the International Classification of Diseases Tenth Revision (ICD-10), inpatient and outpatient claims data, and medical treatment details. 16 Citizens enrolled in the NHIS are encouraged to undergo health examinations at least biannually, with results and lifestyle questionnaires recorded in the National Health Screening Database.
The study protocol was approved by the Institutional Review Board of the Samsung Medical Center (2019-01-034). The need for informed patient consent was waived due to the utilization of publicly available and de-identified patient data. All procedures complied with the relevant patient confidentiality guidelines.
Study population
We identified 86,287 individuals diagnosed with GD between January 2010 and December 2014 using the ICD-10 code for hyperthyroidism (E05). As in previous studies on GD in Korea, 15,17,18 we excluded cases of transient thyrotoxicosis by enrolling individuals who had received antithyroid drugs (ATDs) for ≥60 consecutive days or who had undergone thyroid surgery or radioactive iodine therapy (RAIT). We applied a washout period from January 2006 to the time of study enrolment to identify newly diagnosed cases of GD or diabetes. Participants <20 years of age, patients with thyroid carcinoma (C73), or individuals with missing data for the NHIS health checkup were excluded (Fig. 1). Finally, we included 36,243 patients with GD matched to 36,243 controls (1:1 ratio) according to age and sex. The study period ended in December 2018.

Selection of the study population.
Clinical outcomes for GD
Cumulative ATD doses were classified as <4603 mg (lowest tertile), 4603–16500 mg (middle tertile), and >16,500 mg (highest tertile). The ATD prescription duration was classified as <11.2 months (lowest tertile), 11.2–31.4 months (middle tertile), and >31.4 months (highest tertile).
In the ATD group, remission was defined as the discontinuation of ATD prescriptions, with no further initiation during the study period. In the RAIT group, hypothyroid status was defined as patients receiving levothyroxine following RAIT. All thyroidectomized patients received levothyroxine after surgery.
Diabetes can be detected incidentally at the time of GD diagnosis. Therefore, we analyzed the risk of diabetes according to the period after GD diagnosis (<0.5 years, 0.5–2 years, and ≥2 years).
Definition of diabetes
Diabetes was defined as a combination of ICD-10 codes (E11, E12, E13, and E14), the prescription of antidiabetic drugs, and/or fasting blood glucose ≥126 mg/dL. We excluded participants who were aged <20 years or had the ICD-10 code (E10) for T1DM. 19
Definitions of covariates
Hypertension was defined as a combination of ICD-10 codes (I10, I11, I12, I13, and I15), prescription of antihypertensive drugs, systolic blood pressure ≥140 mmHg or diastolic blood pressure ≥90 mmHg. Dyslipidemia was defined as a combination of the ICD-10 code (E78), prescription of drugs for dyslipidemia, and/or total cholesterol ≥240 mg/dL. Household income was classified into quartiles (Q1–Q4), and absolute poverty was defined as monthly household income less than the minimum cost of living. All covariates were evaluated before GD diagnosis in patients and before the inclusion of controls in the program.
Statistical analyses
Categorical baseline characteristics were compared using the chi-square test. Conventional Cox proportional hazard regression analyses were performed to evaluate the association between GD and incident diabetes. Model 1 did not adjust for the HR, whereas Model 2 incorporated adjustments for age; sex; household income; and comorbidities, including hypertension, dyslipidemia, and cancer. Model 3 further adjusted for age; sex; household income; comorbidities, including hypertension, dyslipidemia, and cancer; body mass index (BMI, kg/m2); smoking; drinking; and exercise as potential confounders. The Kaplan–Meier curve was used to visually summarize time from GD diagnosis to T2DM diagnosis. Statistical significance was defined as p <0.05. All statistical analyses were performed using the SAS software (version 9.4; SAS Institute Inc., Cary, NC, USA).
Results
Baseline demographics
This study included 36,243 patients with GD and 36,243 age- and sex-matched control subjects. The mean age of the participants was 49 years, and most (89%) aged <65 years. In both the groups, 70% were women. Patients with GD exhibited a lower BMI, a higher prevalence of hypertension, a lower prevalence of dyslipidemia, and higher concentrations of fasting glucose compared to controls (Table 1). The mean follow-up period was 6.3 years for both groups.
Baseline Demographics of Patients with Graves’ Disease and Controls
Controls and patients with Graves’ disease were matched by age and sex.
Continuous data are presented as mean ± SDs, median (interquartile ranges), and categorical data are presented as n (%).
Individuals who had smoked more than five packs in their lifetime were classified as smokers. Former smokers were distinguished from current smokers based on their present smoking status as individuals who had stopped smoking at the time of the survey, regardless of the duration.
Heavy drinkers were defined as males who consumed >30 g of alcohol/day and females who consumed >20 g of alcohol/day. Mild drinkers were defined as males who consumed <30 g of alcohol/day and females who consumed <20 g of alcohol/day. Nondrinkers were defined as those who drank 0 g of alcohol/day.
Regular exercise was defined as (1) high-intensity exercising more than thrice weekly for >20 minutes each time or (2) moderate-intensity exercising more than five times a week for >30 minutes each time.
BMI, body mass index; DBP, diastolic blood pressure; GFR, glomerular filtration rate; SBP, systolic blood pressure.
Association between GD and incident diabetes
Among the 36,243 patients with GD, we noted 1851 cases of incident diabetes over 227,899 person-years (PYs). Patients with GD had a higher risk of new-onset diabetes compared to controls, which persisted after adjusting for age; sex; household income; comorbidities, including hypertension, dyslipidemia, and cancer; BMI; smoking; drinking; and exercise (HR = 1.13 [95% confidence interval, CI: 1.06–1.21]) (Fig. 2).
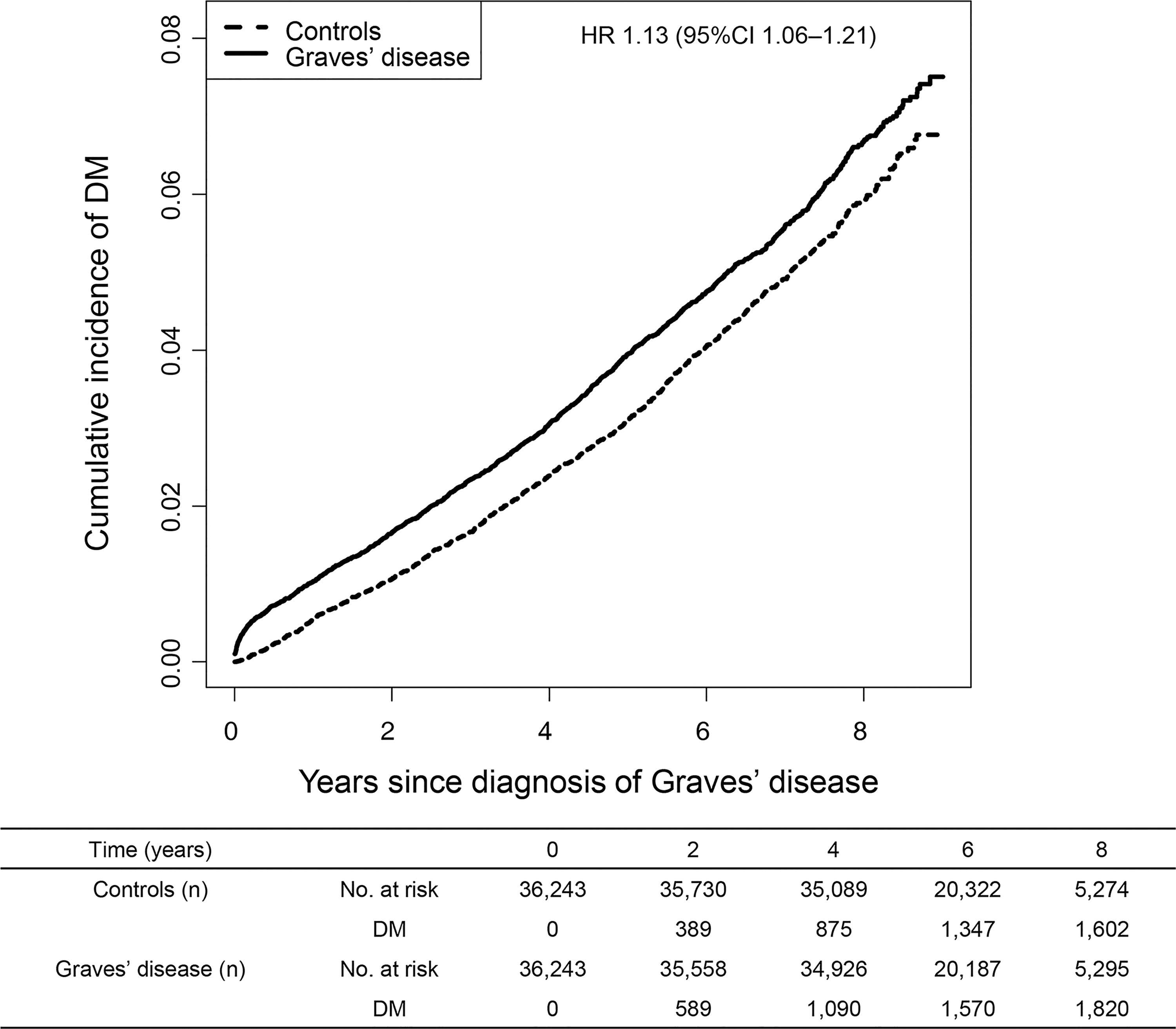
Risk of type 2 diabetes among patients with Graves’ disease and control subjects. The HR was adjusted for age; sex; household income; comorbidities, including hypertension, dyslipidemia, and cancer; body mass index; smoking; drinking; and exercise. CI, 95% confidence interval; DM, diabetes mellitus; HR, hazard ratio.
Subgroup analyses were performed based on age, sex, comorbidities, and BMI (Table 2). The incidence rates (IR) of diabetes were the highest in groups aged ≥65 years, with hypertension, dyslipidemia, and obesity (BMI ≥25 kg/m2) (IR per 1000 PYs, 13.6–18.5). Individuals with GD tended to have a higher risk of diabetes, regardless of multiple clinical parameters (p for interaction, not significant).
Subgroup Analysis of Diabetes Risk among Patients with Graves’ Disease and Controls
The hazard ratios were adjusted for age; sex; income; comorbidities, including hypertension, dyslipidemia, and cancer; BMI; smoking; drinking; and exercise.
CI, 95% confidence interval; DM, diabetes mellitus; IR, incidence rate; PYs, person-years.
Association between GD and incident diabetes according to treatment modality and outcomes
In the Korean population, between 2010 and 2018, the majority of patients (96.2%) were treated with ATDs, followed by RAIT (3%) and surgery (0.8%) (Supplementary Table S1). The HRs for incident T2DM were 1.12 [CI: 1.05–1.20] for the ATD group, 1.38 [CI: 1.08–1.77] for the RAIT group, and 1.32 [CI: 0.82–2.13] for the surgery group. No significant differences were seen in the risk of T2DM between groups based on clinical outcomes, that is, GD remission after ATDs or hypothyroid status after RAIT or surgery.
Association between GD and diabetes according to cumulative ATD dose and treatment duration
When we categorized patients with GD according to the cumulative ATD dose and treatment duration, the risk of incident diabetes increased with the cumulative dose and duration of ATD (Table 3). A longer duration of ATD therapy and a higher cumulative dose were associated with a significant risk of developing diabetes in patients with GD than in the controls.
Risk of Diabetes among Patients with Graves’ Disease according to Cumulative Dose and Treatment Duration of Antithyroid Drug
The cumulative ATD doses were <4603 mg (lowest); 4603–16,500 mg (middle); and >16,500 mg (highest).
The cumulative ATD treatment durations were <11.2 months (lowest), 11.2–31.4 months (middle), and >31.4 months (highest).
Model 1: Not adjusted.
Model 2: Adjusted for age; sex; income; and comorbidities, including hypertension, dyslipidemia, and cancer.
Model 3: Adjusted for age; sex; income; comorbidities, including hypertension, dyslipidemia, and cancer; body mass index; smoking; drinking; and exercise.
ATD, antithyroid drug.
Association between GD and diabetes according to the period since GD diagnosis
We classified patients with GD according to the period from GD diagnosis. After adjustment for clinical variables, the risk was the highest soon after GD diagnosis (<0.5 years) (HR 3.21 [CI: 2.15–4.80]) The risk was elevated during the 0.5–2 years (HR = 1.36 [CI: 1.06–1.75]). However, no significant risk was noted ≥2 years after GD diagnosis (HR = 0.93 [CI: 0.83–1.05]) (data not shown).
Discussion
In our cohort of individuals newly diagnosed with GD without diabetes at enrolment, approximately 5.1% developed incident T2DM during the 227,899 PYs of follow-up (4.5% in controls during 228,789 PYs). GD itself was an independent risk factor for diabetes, even after adjusting for age; sex; income; comorbidities, including hypertension, dyslipidemia, and cancer; BMI; smoking; drinking; and exercise. However, the risk of developing T2DM did not vary significantly with treatment modality or clinical outcomes (remission or hypothyroid status). The overlap of CIs for subgroups suggested no significant differences in the risks for incident T2DM between the different treatment groups. Nevertheless, the risk of new-onset diabetes increased gradually in a dose- and duration-dependent manner in patients with ATDs. Of note, the risk of diabetes was the highest in the early period after GD diagnosis, while there was no significant risk two years after GD diagnosis. Hence, diabetes screening at the time of GD diagnosis can be considered.
Thyroid dysfunction, encompassing hypothyroidism and hyperthyroidism, modulates glucose homeostasis via different mechanisms. In patients with hypothyroidism, alterations in glucose transport 4 and elevated free fatty acid levels may induce insulin resistance, leading to hyperglycemia. 20 Similarly, hyperthyroidism contributes to hyperglycemia via various pathways. Increased catecholamine-induced lipolysis stimulates hepatic gluconeogenesis and upregulates glucose transport 2 levels in the liver, promoting hepatic glucose output. 21 Additionally, shortened insulin half-life and enhanced glucose absorption in the gut contribute to a hyperglycemic state. 21
Clinical evidence linking thyroid dysfunction and diabetes remains inconclusive. A meta-analysis of 12 prospective studies reported a 17% higher risk of diabetes in populations with high TSH levels than in those with normal TSH levels. 9 This meta-analysis indicated a J-shaped relationship between serum TSH and incident diabetes, suggesting that lower TSH levels (hyperthyroidism) may entail an elevated diabetes risk, albeit insignificantly. 9 Another meta-analysis of six prospective studies reported that hypothyroidism was related to the development of diabetes (HR = 1.26), whereas hyperthyroidism was not. 8 In this meta-analysis, four studies on hyperthyroidism had a pooled HR of 1.16 [CI: 0.90–1.49] and moderate heterogeneity (I 2 = 45%). Chang et al. concluded that low TSH was not linked to diabetes development (HR = 1.05 [CI: 0.80–1.39]), based on their findings from 2246 Taiwanese patients with low TSH (60 diabetes, 2.7%) and 65,499 participants with normal TSH (1461 diabetes, 2.2%) over a median 2.6-year follow-up. 22 Another study included in this meta-analysis 8 used an observational cohort from the nationwide Danish health register and concluded that patients with hyperthyroid had a higher risk for diabetes (HR = 1.46 [CI: 1.16–1.84]) using 2631 patients with hyperthyroid (283 diabetes, 10.8%) and 10,524 controls (795 diabetes, 7.6%) during a six-year follow-up. 10 Notably, previous longitudinal studies have yielded conflicting results due to the low incidence of GD and smaller study samples, our study included the largest cohort with GD and incident T2DM, with a longer follow-up duration.
Patients with GD exhibited higher risks of developing T2DM than controls (HR = 1.06–1.22), spanning various demographic subgroups. As expected, individuals with established risk factors for diabetes, such as old age (≥65 years), hypertension, dyslipidemia, and obesity, displayed higher IRs of diabetes (IR, 13.6–18.5 per 1000 PYs), irrespective of the presence of GD. However, the risks for incident diabetes were comparable in each subgroup. Notably, approximately two-thirds of patients with GD (24,530 patients, 68%) were diagnosed between 40 and 64 years, and 77% of them were not obese (BMI <25 kg/m2). Since hyperthyroidism can induce hyperglycemia via mechanisms other than obese T2DM, clinicians should closely monitor patients with GD for T2DM. Given these findings, it is notable that the screening age for T2DM is lowered to 35 years based on recommendations from the USPSTF and KDA. 5,6
Importantly, the risk of T2DM was increased soon after GD diagnosis (<0.5 years) but reduced significantly two years after GD diagnosis. T2DM can be detected incidentally at the time of GD diagnosis. However, we excluded participants without health examination data within two years before study enrolment. Thus, the patients and controls were offered equal opportunities for diabetes screening. One recent Japanese study showed that glucose variability and mean glucose measured by CGM improved after successful medical treatment (a mean period of three months) of GD in newly diagnosed patients with GD. 23 We cautiously assumed that uncontrolled hyperthyroidism at the time of GD diagnosis has a negative effect on glucose metabolism in individuals prone to diabetes. However, after proper treatment for GD, the risk of incident diabetes in this population is comparable to that in controls. However, we cannot fully eliminate the reverse causation between GD diagnosis and the development of T2DM, given the retrospective design of our study. Nevertheless, early detection and management of diabetes are crucial because a large number of individuals have no hyperglycemia symptoms a few years before they are diagnosed with diabetes. Appropriate and timely interventions for diabetes can improve glycemic control and cardiovascular outcomes in these patients. 4 –6
The risk of incident diabetes in patients with GD increased in a dose- and duration-dependent manner in the ATD group. Song et al. assessed the risks of diabetes based on treatment duration of ATDs in 4593 Korean patients with long-standing GD from the NHIS database. 24 In their study, 751/4593 (16.3%) patients had diabetes (HR = 1.17), and the risk increased with prolonged ATD therapy, 24 similar to the findings of our study. Considering the approximately 50% recurrence rate of GD with ATD treatment, 25 longer treatment duration or higher doses of ATD suggest intractable GD necessitating sustained medical therapy, with continuous thyrotoxicosis potentially inducing glucose intolerance.
The risk of diabetes did not vary significantly according to treatment modality or clinical outcomes. The risk of developing diabetes was comparable in patients who experienced GD remission after ATD, RAIT, or surgery. In contrast, patients who did not achieve remission post-therapy had a slightly higher risk of diabetes (HR = 1.13 [CI: 1.05–1.21]). We included a small number of patients with GD remission after ATD treatment (1442 patients), resulting in the overlap of CIs between the ATD groups with or without remission. As a result, we cannot conclude that patients in remission after ATDs have a similar risk for diabetes compared to control subjects.
No significant differences were seen in risk for developing diabetes between patients with or without hypothyroid status after RAIT, which was probably due to the small number of participants in each subgroup (663 and 430 patients, respectively). Song et al. reported a higher risk of diabetes in the RAIT group (HR = 1.88) compared to the ATD group (HR = 1.17) 24 ; despite including a small number of patients (RAIT, 102 patients) in their study. Thus, further studies with a larger sample size are warranted to confirm the risk of diabetes in patients with GD receiving RAIT or surgery.
As autoimmune thyroid dysfunction occurs frequently (17–30%) with T1DM, 20 we excluded T1DM using ICD-10 codes and age at enrolment. A recent study reported an overall T1DM incidence of 4.5 per 100,000 persons in Korea, notably lower than Western countries (≥20/100,000 per year). 19,26 Furthermore, patients with an ICD-10 code (E10) for T1DM in Korea are not eligible for oral hypoglycemic agents and are exclusively prescribed subcutaneous insulin to manage hyperglycemia. Moreover, the peak incidence of T1DM in the Korean population occurs between ages 10 and 14 years. 19 Therefore, we excluded T1DM by including individuals aged ≥20 years in our study.
This study has a few limitations. First, to identify individuals with GD, we used a combination of ICD-10 codes and prescriptions for medication and/or procedure codes for RAIT/surgery. To exclude patients with transient thyrotoxicosis, we employed consecutive prescriptions ≥60 days of ATDs, a criterion adopted in previous epidemiological studies in Korea. 15,17,18 In Korea, as an iodine-sufficient area, GD accounted for 82.7% of thyrotoxicosis cases, followed by transient thyrotoxicosis (16.8%), and toxic adenomas (0.5%). 27 On the contrary, toxic multinodular goiter and toxic adenoma account for 50% of all cases of hyperthyroidism in iodine-deficient areas. 28 Consequently, the hyperthyroid population in this study may be regarded as having GD, although there is a critical limitation in identifying accurate etiologies of thyrotoxicosis based on ICD-10 codes. Second, the NHID lacks information on thyroid function or autoantibody titers, representing a major weakness of our study. However, we used prescription information of ATDs and levothyroxine to assess thyroid function status and clinical outcomes of GD following treatment. Third, the population treated with definitive therapy was small, which limited the statistical power to evaluate the development of diabetes, especially in the surgical group. Thus, further studies with a larger population of patients with GD who receive definitive treatment are needed to clarify the risk of diabetes in these cohorts. Nevertheless, the present study is based on a large population-based sample and utilizes a single cohort to compare the effects of the three treatment methods for GD on the risk of diabetes.
Conclusions
Individuals with GD exhibited a higher risk of incident diabetes compared to controls, especially in the two years after GD diagnosis. Diabetes risk increases with a dose- and duration-dependent manner of ATD treatment, although we observed no differences in the risks of T2DM according to treatment methods. Given the exponential increase in diabetes risk, particularly in the younger population, screening for diabetes can be considered in individuals with newly diagnosed GD.
Footnotes
Authors’ Contributions
Y.Y.C.: Design and interpretation of data for the work, drafting the work, and agreement to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. B.K.: Acquisition, analysis, and interpretation of data for the work, and agreement to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. S-.M.J.: Interpretation of data for the work, reviewing it critically for important intellectual content, and agreement to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. C-.H.J.: Reviewing it critically for important intellectual content and agreement to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. J.O.M.: Interpretation of data for the work, reviewing it critically for important intellectual content, and agreement to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. S.W.K.: Design of the work, reviewing it critically for important intellectual content, and agreement to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. J.H.C.: Design of the work, reviewing it critically for important intellectual content, and agreement to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. K-.D.H.: Design of the work, acquisition, analysis, and interpretation of data for the work, and final approval of the version to be published. T.H.K.: Design and interpretation of data for the work, and final approval of the version to be published. All authors have reviewed the article critically for intellectual content and agreed to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. Tae Hyuk Kim had full access to all the data in the study and took responsibility for data integrity and accurate data analysis.
Author Disclosure Statement
The authors have no conflicts of interest to declare.
Funding Information
This work was supported by a National Research Foundation of Korea (NRF) grant funded by the Korean government (MSIT) (No. RS-2022-00166846). This study was supported by the Soonchunhyang University Research Fund.
Supplementary Material
Supplementary Table S1