
Abstract
Introduction:
Among childhood cancer survivors, the cumulative incidence rate of differentiated thyroid carcinomas (DTCs) is estimated to be 8–11%. Although the association of DTC with prior radiotherapy is well-studied, the association with chemotherapy remains less understood. Most studies focused on young adults, leaving a knowledge gap on subsequent DTC occurring in childhood and adolescence.
Methods:
In this retrospective cohort study, we analyzed DTCs in children and adolescents under 18 years of age who were registered with the national multicenter Malignant Endocrine Tumor studies in Germany (1997–2023). We compared patients with first primary DTC to those with subsequent DTC that developed after a history of childhood cancer or hematopoietic stem cell transplantation (HSCT). In the subsequent DTC subgroup, we compared DTCs following chemotherapy only to those following chemo- and radiotherapy.
Results:
Of 505 patients with DTCs, 66 (13.1%) (38 male, 28 female) were subsequent DTCs. The median age at subsequent DTC diagnosis was 12.7 years (range, 5.1–17.9), with a median latency of 7.3 years (range, 2.2–15.6) from the first malignancy or HSCT. The 5-year overall survival (OS) and thyroid-related adverse event-free survival (EFS) estimates from the diagnoses of a subsequent DTC were 100.0% and 82.5%, respectively. Prior treatment included chemotherapy in 64 patients, with 18 receiving chemotherapy alone. In all, 46 subsequent DTC patients had a history of external radiotherapy, including 2 treated with radiotherapy only and 14 with total body irradiation. Two patients received 131I-metaiodobenzylguanidine treatment. Subsequent DTCs versus first DTCs were smaller in size but more frequently multifocal. Subsequent DTCs following chemotherapy only, compared with chemo- and radiotherapy, developed after a shorter latency (median 6.2 vs. 7.8 years), and were larger (median 1.86 vs. 1.18 cm). Patients with subsequent DTCs following chemotherapy only were younger at diagnosis (median 11.5 vs. 13.7 years). No differences were observed for OS and EFS.
Conclusions:
Presenting features of subsequent DTCs differ from primary counterparts, although the prognosis is not significantly different. Subsequent DTCs following chemotherapy only versus chemo- and radiotherapy DTCs were larger and diagnosed in younger patients after a shorter latency. More research is needed to identify risk factors and mechanisms potentially contributing to thyroid tumorigenesis post-chemotherapy.
Introduction
Over the past decades, the outcome of childhood cancer has improved due to diagnostic and therapeutic advances. Accordingly, the number of childhood cancer survivors has been increasing steadily. 1 Currently, survival rates for children and young adults with differentiated thyroid carcinomas (DTCs) are projected to exceed 30 years. 2,3 Adverse late effects of treatment thus become more important. Childhood cancer survivors are at increased risk of subsequent tumors, including DTC. 4 The cumulative incidence of subsequent DTC ranges from 8% to 11.7% in different cohorts, corresponding to 1–2 children and adolescents per million people per year. 5 –7 The incidence is highest in survivors of leukemia, (Hodgkin) lymphoma, and central nervous system (CNS) tumors. 7 –9 Solid tumors, including DTC, are the most common subsequent tumor type after hematopoietic stem cell transplantation (HSCT) with and without total body irradiation (TBI). 10,11 Individuals previously treated for cancer at young ages have a higher incidence compared with other age groups. 12
The excess risk of subsequent DTCs is mainly attributable to prior radiotherapy to the thorax, head, and neck. 8 Radiation doses up to ∼30 Gy linearly increase risk while a downturn in the dose–response relationship is seen above 30 Gy, likely due to cell-killing effects. 8,9,13 –15 A possible joint effect of chemotherapy and radiotherapy has been discussed. 16
Despite advancements in understanding the causes of subsequent DTCs and, consequently, risk prediction, 17 little is known regarding tumor characteristics, survival, and best treatment in this vulnerable population. 18,19 Goldfarb and Freyer reported 1349 adolescents and young adults (AYAs, ages 15–39 years) with subsequent DTCs from the American College of Surgeons National Cancer Database, registered between 1998 and 2010. 20 They demonstrated an inferior overall survival (OS) of AYAs with subsequent DTCs (95.7%) compared with first DTCs (99.3% [confidence interval = 4.97–8.86]; p < 0.0001) with a 6.63-fold increased relative risk of death. Clement and colleagues performed a matched control study on 31 childhood cancer survivors with subsequent DTCs (median age at DTC diagnosis 25.6 years) in the Netherlands. 21 This study demonstrated a trend toward smaller tumor sizes and at the same time higher incidences of bilateral tumors. No differences in recurrence rate and disease-related death were reported. Of note, their series included eight (25.8%) subsequent DTC patients with a history of chemotherapy only. Beyond that, data on subsequent DTCs occurring in childhood and adolescence are scarce.
To fill this gap, we analyzed data on children and adolescents with DTC from the German multicenter Malignant Endocrine Tumor (MET) studies. 22 Our primary research question was to investigate the presentation and outcome of subsequent DTCs compared with first DTCs. Our secondary research question focused on comparing subsequent DTCs occurring following chemotherapy only versus chemo- and radiotherapy.
Material and Methods
Patients and study design
Patients aged <18 years with a histopathologically confirmed diagnosis of DTC were registered prospectively with the national, multicenter MET studies of the German Society of Pediatric Oncology and Hematology (GPOH) between January 1997 and December 2023. Informed consent was obtained from patients and/or legal guardians, as appropriate. Follow-up was completed on December 31, 2023. The GPOH-MET 97 protocol, the GPOH-MET 2013 registry, and the MET registry were approved by the ethics committees of the University of Luebeck (IRB 97125) and the Otto-von-Guericke-University Magdeburg (IRB 174/12 and 52/22), Germany. For this analysis, DTC was classified as subsequent if there was a prior childhood cancer (including nonmalignant CNS tumors) or HSCT for a nonmalignant condition. Patients with synchronous cancers, including DTC, were excluded from the analysis. Patients with first DTCs served as the comparison group. Previously published reports provided details on patients with first DTC. 23
Data collection
The data were collected through nationwide reporting from pediatric oncology departments across Germany. Upon the notification of a cancer diagnosis, pediatric oncologists were asked to complete a standardized case report form provided via the German Pediatric Cancer Registry (DKKR). These data were subsequently entered into the GPOH-MET database. Further demographic, clinical, histopathological, treatment, and outcome data were extracted from original patient-care source documents. Information on family history of DTC was recorded up to the third degree of relationship. Frequencies were calculated based on the available data. “Latency” was defined as the period from the diagnosis of the first malignancy or HSCT to the diagnosis of DTC. Tumors were classified according to the World Health Organization classification of DTC and the American Joint Committee on Cancer/tumor node metastasis (TNM) staging system applicable at the time of diagnosis. Tumor size, multifocality, capsule invasion, lymphovascular invasion, soft tissue infiltration, and lymph node involvement were defined utilizing histopathology. Histopathological information was obtained from the reference pathology reports if available or from local pathology reports. Distant metastases were identified using radioactive iodine (RAI) scans and/or chest computed tomography. Thyroid hormone levels and interpretation according to local reference ranges were accepted for this analysis.
Patients undergoing follow-up for an initial malignancy and treatment with radiotherapy, 131I metaiodobenzylguanidine (MIBG) therapy, or stem cell transplantation received routine thyroid ultrasounds as part of their oncology-directed care. In contrast, patients without an initial malignancy, or those in routine care outside of oncology follow-up, underwent thyroid ultrasounds only when specific clinical indications were present (e.g., clinical symptoms or abnormal laboratory findings).
There were no substantive changes to the data collection procedures during the study period, although the GPOH-MET registry occasionally updated case report forms and coding systems to align with evolving clinical guidelines, without materially affecting the study’s relevant variables.
Patient grouping
Three patient groups were initially identified based on their treatment histories: those who received chemotherapy only, those who received radiotherapy, and those who underwent both treatments. However, for the purposes of subgroup analysis of subsequent DTCs, patients who received “radiotherapy only” were excluded due to the small sample size (n = 2), as this number was insufficient for meaningful statistical analysis. Therefore, the analysis focused on the two remaining groups: chemotherapy only and chemotherapy with radiotherapy. Patients who received radiotherapy exclusively to infradiaphragmatic sites were categorized as “chemotherapy only.” Radiotherapy to the head, neck, and/or mediastinum/thorax is referred to as “radiotherapy to the head and neck.”
Study protocols
Details on the GPOH-MET 97 protocol and the GPOH-MET 2013 registry were published previously. 22,23 Briefly, total thyroidectomy including routine central neck dissection was recommended for all patients with DTC. Lateral lymph node dissection of all affected lymph node compartments was recommended for patients with suspicious lateral lymph nodes. Postoperative treatment with 131I was recommended for all patients. 22 No specific recommendations were predefined for patients with subsequent DTC. RAI therapy was not applied across all cases. In instances of hemithyroidectomy, RAI therapy was not administered. In addition, in some cases of papillary microcarcinoma RAI therapy was omitted. The decision to forgo RAI therapy in these cases was left to the discretion of the treating physicians.
Statistical analysis
Kaplan–Meier estimates were used to determine OS and event-free survival (EFS). OS was defined as the time from the diagnosis of DTC to the patient’s death from the disease. EFS encompasses the period from diagnosis to the thyroid-related first event, which could be failure to achieve complete remission, disease progression, relapse, or death due to the disease, or the appearance of other malignant diseases, whichever occurred first. Individuals still alive were censored at their last known follow-up date.
To assess the differences between groups, the log rank test was employed for survival data, such as OS and EFS, to evaluate the equality of survival distribution. The chi-squared test was utilized for categorical data to examine differences in frequencies or proportions. Given the small sample size and the large number of variables analyzed in this study, a multivariate approach was considered unsuitable due to the risk of generating biased results. To address the issue of multiple testing and to control for the family-wise error rate, we applied the Bonferroni correction. The corrected significance level (α_corr) was calculated as α/k, where α = 0.05 and k = 24 (the number of tests performed), resulting in a corrected significance threshold of α_corr = 0.0021. Consequently, p values ≤ 0.0021 were considered statistically significant in our analyses. This adjustment acknowledges the exploratory nature of our study, while providing a more robust interpretation of our findings. For continuous data not following a normal distribution, the Mann–Whitney U test was used, while the t test was applied to normally distributed continuous data. A p value of < 0.05 was considered statistically significant.
Data analysis was conducted with the IBM® SPSS statistical software (version 29.0.2.0). Charts and graphs were generated using R and R Studio (version R-4.3.3).
Results
Patient cohort
In total, 505 patients with pediatric DTCs were registered, including 439 (86.9%) with first primary DTCs and 66 (13.1%) with subsequent DTCs. Within the cohort of subsequent DTCs, sex ratio demonstrated a small male preponderance (1.3:1). The median latency from first cancer diagnosis or HSCT to subsequent DTC was 7.3 years (range, 2.2–15.6). Detailed information on patients with subsequent and first DTCs is provided in Table 1.
Demographic and Clinical Characteristics of 439 Patients with First and 66 Patients with Subsequent Differentiated Thyroid Carcinoma
Including 9 subsequent DTCs detected during age-specific preventive medical examinations and 32 DTCs detected by neck palpation and/or neck ultrasound during follow-up for childhood cancer.
Including 26 DTCs detected during age-specific preventive medical examinations and 78 DTCs detected by neck palpation and/or neck ultrasound by incidence.
10 patients received thyroxine therapy.
According to the World Health Organization classification of DTC and the American Joint Committee on Cancer (AJCC)/tumor node metastasis (TNM) staging system in the currently valid version.
Including rupture of thyroid capsule.
Maximum gross extrathyroidal extension invading strap muscles (sternohyoid, sternothyroid, or omohyoid muscles).
Includes gross extrathyroidal extension into major neck structures.
DTC, differentiated thyroid carcinoma; FTC, follicular thyroid carcinoma; IQR, interquartile range; NIFT-P, noninvasive follicular thyroid neoplasm with papillary-like nuclear features; NOS, not otherwise specified; PTC, papillary thyroid carcinoma; SD, standard deviation; TSH, thyrotropin.
Previous malignancies
Of the 66 patients with subsequent DTCs, 20 (30.3%) had previously been treated for leukemia, 13 (19.7%) for CNS tumors, 12 (18.2%) for lymphoma (including 11 for Hodgkin lymphoma), 7 (10.6%) for neuroblastoma, and 9 (13.6%) for other malignancies. Five (7.6%) patients developed DTCs following HSCT for a hematological disorder (n = 2) or immunodeficiency (n = 3). Detailed information on prior childhood cancers is depicted in Table 2.
Details on First Childhood Cancer (Including Nonmalignant Central Nervous System Tumors) or Hematopoietic Stem Cell Transplantation in 66 Children and Adolescents with Subsequent Differentiated Thyroid Carcinoma
Including one patient each with severe combined immunodeficiency, severe congenital neutropenia, severe immunodeficiency not further specified, severe aplastic anemia, and Diamond-Blackfan anemia.
HSCT, hematopoietic stem cell transplantation.
Prior treatment modalities
Prior treatment included chemotherapy for 64 (of 66; 97.0%) subsequent DTC patients, with 18 receiving chemotherapy only. Chemotherapy regimens included alkylating agents in 58 (of 62; 93.5%) patients, anthracyclines in 47 (75.8%), and platinum derivatives in 20 (32.3%) (Table 3). Details on chemotherapy were not available in two patients. Approximately half of the subsequent DTC patients had a history of fractionated radiotherapy to the head and neck region (N = 32, 48.5%) including two with radiotherapy only. Another 14 (21.2%) subsequent DTC patients had a history of TBI in the context of HSCT, and 2 (3.0%) had 131I-MIBG treatment for neuroblastoma. No patient underwent brachytherapy. For external radiotherapy (including TBI), the mean and median radiation doses were 31.1 Gy (standard deviation [SD] 21.3) and 20.8 Gy (range, 4.0–78.0). Details on the radiation dose by radiation field are provided in Table 4. According to recent recommendations for diagnostic workup, patients with a history of lymphoma (n = 12), soft tissue sarcoma (n = 4), and bone tumors (n = 1) underwent 18F-fluorodeoxyglucose ([18F]FDG)-positron emission tomography (PET), and patients with neuroblastoma (n = 7) underwent 123I-MIBG scintigraphy for initial staging and response assessment. Of these 24 patients, 16 (66.7%) also received external radiation or MIBG treatment. Of note, of seven affected neuroblastoma survivors, four did not have therapeutic radiation exposure.
Details on Prior Oncological Treatment
Categories of chemotherapeutic drugs in 62 patients.
Details on Prior Oncological Treatment
Administered radiation dose depending on radiation field in 46 patients.
TBI, total body irradiation.
Clinical presentation and tumor characteristics
The mean age at diagnosis of subsequent DTC was 12.7 years (range, 5.1–17.9). No familial history of thyroid diseases other than DTC was reported. Thirty-two (of 53; 60.4%) DTCs were detected by neck palpation or thyroid sonography during follow-up for prior childhood cancer, 9 (17.0%) during age-specific preventive medical examinations (standard in pediatrics in Germany), and 12 (22.6%) via tumor symptoms (difficulty swallowing, globus sensation, hoarseness, swelling, and shortness of breath) reported by the patients themselves. Thirty-nine (of 63; 61.9%) patients presented with lymph node metastases and 10 (of 56; 17.9%) with distant metastases. The predominant histological subtype in subsequent DTCs was papillary thyroid cancer (59; 92.2%), followed by follicular thyroid cancer (3; 4.7%). Median tumor size was 1.1 cm (range, 0.1–4.0), with 23 (of 55; 41.8%) patients presenting with a tumor size ≤1 cm. Histopathology revealed multifocal tumors in 31 (of 54; 57.4%) patients, tumor capsule invasion in 31 (of 45; 68.9%), vascular invasion in 10 (of 43; 23.3%), and soft tissue infiltration in 26 (of 58; 44.8%). An association was observed between tumor size and the presence of distant metastases (p = 0.022), but not with lymph node metastases (p = 0.087).
Surgical and postoperative treatment
Total thyroidectomy was performed in 39 (of 62; 62.9%) patients as initial therapy, subtotal thyroidectomy in 3 (4.8%), hemithyroidectomy in 13 (21.0%), lymph node dissection in 6 (9.7%), and node enucleation in 1 (1.6%). Surgical complications were reported in 31 (of 50; 62.0%) patients, including transient and permanent hypoparathyroidism (n = 27) and recurrent laryngeal nerve injury (n = 12). RAI therapy was administered in 55 (of 59; 93.2%) patients, including 13 receiving 2–5 courses. The median 131I activity of the first RAI therapy was 2.93 GBq (range, 0.42–30.7) corresponding to a 131I activity of 58.85 MBq/kg bodyweight (range, 17–504). The median cumulative 131I activity was 3.7 GBq (range, 0.42–58.3).
Follow-up and outcome
The mean duration of follow-up for patients with subsequent DTCs was 3.0 years (SD 3.3). The OS estimates at 2.5 and 5 years were both 100.0% and the EFS estimates were 86.4% and 82.5%, respectively (Fig. 1). No patient had died of disease or a third neoplasm at the last follow-up. Events occurred at a mean of 1.9 years (SD 1.8) following diagnosis of subsequent DTC in eight patients including local recurrence (n = 2), lymph node metastases (n = 2), pulmonary metastases (n = 1), combined relapse (n = 1), persistent disease (n = 1), and one patient with renal cell carcinoma after 5.9 years. No association between clinical factors and outcome was found.
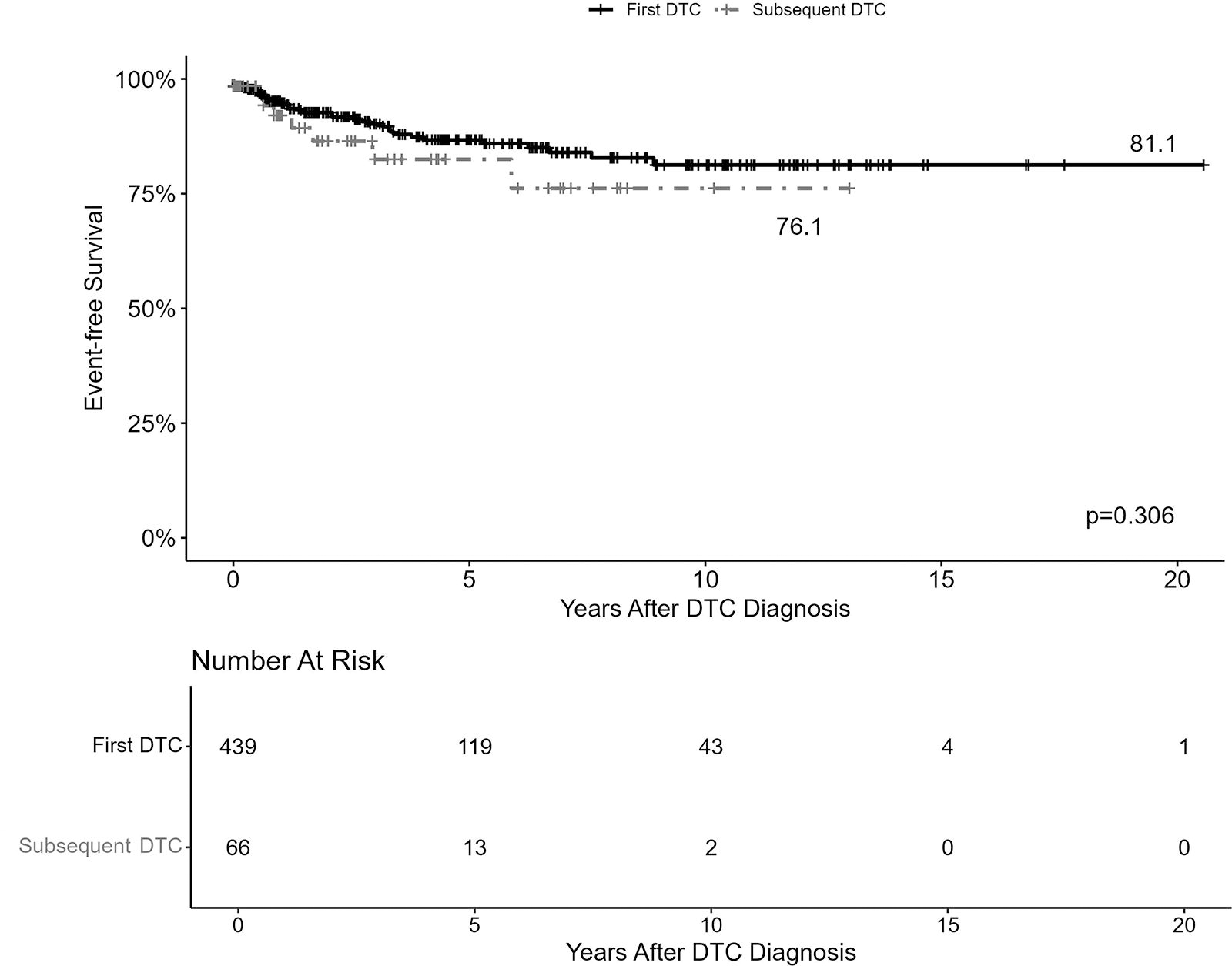
Event-free survival (EFS) in patients with first (n = 439) and subsequent (n = 66) DTC. EFS is defined as the duration from the start of treatment to the occurrence of any of the following events: disease progression, recurrence, or death. DTC, differentiated thyroid carcinoma.
Comparison of subsequent and first DTC
Subsequent DTCs compared with first DTCs occurred less frequently in female patients (28/66, 42.4% vs. 326/439, 74.3%; p < 0.001). Subsequent DTCs, unlike first DTCs, were more frequently detected through surveillance or incidentally, whereas first DTCs were primarily identified due to the presentation of symptoms. No patient with subsequent DTC had preexisting thyroid disease (0/49, 0% compared with 67/342, 19% in the first primary DTC group). Subsequent DTCs were smaller in median size (1.1 vs. 2.2 cm, p < 0.001) and showed less frequent vascular invasion (10/43, 23.3% vs. 112/262, 42.7%; p = 0.016) but more frequently presented as multifocal lesions (31/54, 57.4% vs. 139/350, 39.7%; p = 0.014) as compared with first primary DTCs (Table 1). No statistically significant differences were observed for age at diagnosis of DTC, histological subtype, preoperative thyroglobulin values, stimulated postoperative thyroglobulin values, tumor capsule invasion, lymphatic invasion, presence of lymph node metastases, and distant metastases (Table 1). Patients with subsequent DTC were more likely to undergo total thyroidectomy as the first surgical procedure (39/62, 62.9% vs. 177/400, 44.3%; p = 0.006), while two-step thyroidectomy was more frequent in first DTC cases (36/202, 17.8% vs. 231/259, 88.8%; p = 0.031). No statistically significant differences were observed in the occurrence of hypoparathyroidism and recurrent laryngeal nerve injury, the number of patients undergoing RAI therapy, and the median 131I activity of the first RAI therapy (Table 1). No significant differences in OS (100% vs. 99.0%; p = 0.718) and EFS (76.2% vs. 81.2%; p = 0.306) were observed between patients with subsequent and first DTCs (Fig. 1).
Presentation and characteristics of subsequent DTCs depending on prior treatment
The median latency from the first malignancy to subsequent DTC was 6.2 years (range, 2.2–12.9) in patients with chemotherapy only (n = 18), 7.8 years (range, 3.8–15.6) in patients with chemo- and radiotherapy (n = 46), and 10.9 years in patients with radiotherapy only (n = 2; including one patient with missing data on age at first malignancy). Among the 64 patients with subsequent DTCs who had received chemotherapy only or chemo- and radiotherapy, those following chemotherapy only were younger (11.5 vs. 13.7 years, p = 0.008) and developed subsequent DTC after a shorter latency (6.2 vs. 7.8 years, p = 0.041), and presented with higher preoperative thyroglobulin values (973 vs. 33.4 ng/mL, p = 0.005). Subsequent DTCs following chemotherapy only were larger (1.9 vs. 1.2 cm, p = 0.014). No differences were observed for sex distribution, mode of diagnosis, stimulated postoperative thyroglobulin values, histological subtype, multifocality, T stage, presence of lymph node, and distant metastases (Table 5). No differences in OS (100% vs. 100%, p = not applicable) and EFS (77.9% vs. 79.3%, p = 0.672) were observed between patients with subsequent DTCs following chemotherapy only compared with those following chemo- and radiotherapy (Fig. 2).

EFS in patients with subsequent DTC following chemotherapy only (n = 18) and chemo- and radiotherapy (n = 46). EFS is defined as the duration from the start of treatment to the occurrence of any of the following events: disease progression, recurrence, or death.
Demographic and Clinical Characteristics of 64 Patients with Subsequent Differentiated Thyroid Carcinoma Following Chemotherapy Only (n = 18) and Chemo- and Radiotherapy (n = 46)
No patient received thyroxine therapy.
9 patients received thyroxine therapy.
According to the World Health Organization classification of DTC and the American Joint Committee on Cancer (AJCC)/tumor node metastasis (TNM) staging system in the version valid at diagnosis.
Including rupture of thyroid capsule.
Maximum gross extrathyroidal extension invading strap muscles (sternohyoid, sternothyroid, or omohyoid muscles).
Includes gross extrathyroidal extension into major neck structures.
Discussion
Our analysis represents the largest known published cohort of 66 children and adolescents aged 5.1–17.9 years (mean age 12.7 years) with subsequent DTC. In comparison, the study reported by Clement et al. 21 (n = 31) included only 7 patients under 18 years of age, with a median age significantly higher at 25.6 years. Similarly, Goldfarb et al. 20 reported on AYAs aged 15–39 years, of which only 67 patients were between the ages of 15 and 19 years. This distinguishes our study as the most substantial investigation focused specifically on younger children and adolescents with subsequent DTCs, addressing a critical gap in earlier research that predominantly included older AYAs.
Clement et al. observed that subsequent DTCs were more frequently diagnosed via surveillance rather than patients presenting with symptoms, similar to our study where many cases were detected through routine follow-up. 21 They noted that subsequent DTCs tended to be smaller in size and exhibited a higher frequency of bilaterality, which aligns with our observations. Goldfarb et al. also reported that secondary DTCs were more likely to be multifocal and smaller in tumor size. However, unlike our findings, they reported a significantly decreased OS for subsequent DTCs compared with first DTCs, despite having a similar follow-up period. 20 Our series included 18 (of 66; 27.3%) patients with a history of chemotherapy only, including alkylating agents, anthracyclines, and platinum derivatives. In line with this, Clement et al. reported that eight (25.8%) patients with subsequent DTCs had not been exposed to radiotherapy. 21 Veiga et al. had previously reported on chemotherapy agent-specific risk of subsequent thyroid carcinoma. Details on the underlying mechanisms of tumorigenesis in patients with chemotherapy only are unknown so far. 15,24 Possible mechanisms for the development of subsequent DTCs in patients treated with chemotherapy alone might include direct DNA damage and genomic instability induced by certain chemotherapeutic agents. Alkylating agents cause cross-linking of DNA strands, leading to mutations and chromosomal abnormalities that can predispose to cancer. Anthracyclines are known to generate free radicals and intercalate into DNA, disrupting essential cellular processes and potentially initiating carcinogenesis. Platinum-based drugs, such as cisplatin, form DNA adducts that hinder DNA repair mechanisms, resulting in mutations. Based on our data and corroborated by the findings of Clement et al., we believe that chemotherapy can act as an independent risk factor for subsequent DTC in certain patients. Specifically, this independent risk may be significant with inherited genetic predispositions that influence their susceptibility to the effects of chemotherapy. In our series, 8 (of 18; 44.4%) patients with subsequent DTCs following chemotherapy only repeatedly underwent diagnostic workup including 18F-FDG-PET and 123I-MIBG scintigraphy. The radiation dose in the thyroid due to diagnostic workup procedures and its potential effects on the risk of thyroid carcinoma have previously been reported on. 25 Among patients with subsequent DTCs following chemotherapy only compared with those previously treated with chemo- and radiotherapy, we observed more frequent instances of younger patients and larger tumor sizes. We did not observe other differences, for example, regarding multifocality. Our data are not suitable to determine whether this finding is related to the underlying mechanisms of tumorigenesis or delayed diagnosis of subsequent DTC in patients with chemotherapy only. Caution is necessary when interpreting the age differences. Age at diagnosis of the first childhood cancer is associated with the type of cancer and treatment details, among others, radiation indication, dose, and field. 8,26 In line with this, albeit not being statistically significant, we observed more older patients with lymphoma, sarcoma, and CNS tumors in the chemo- and radiotherapy subgroup compared with the chemotherapy only subgroup. In addition, due to our study design, we did not capture young adults with subsequent DTCs following a first cancer during adolescence. We observed that subsequent DTCs following chemotherapy only occurred after a shorter latency in time.
This study underscores the necessity of refining current surveillance protocols for young patients post-childhood cancer or HSCT treatment. The observed variance in latency periods for DTC development within our cohort, particularly the instances of early onset within five years, suggests that uniform screening recommendations may not adequately address the needs of all patient subgroups. Tailoring screening intervals based on individual risk factors such as age at treatment, type of cancer, and treatment modalities could lead to more effective early detection strategies. We recommend prospective studies to investigate the efficacy and feasibility of earlier and perhaps more frequent surveillance in high-risk pediatric populations, to improve prognostic outcomes through timely interventions. Future research is necessary to elucidate our findings including the potential roles of genetic predisposition and diagnostic radiation exposure, particularly in young childhood cancer survivors.
We also compared the presentation and outcome of subsequent and first DTCs. In subsequent DTCs, we did not observe a female preponderance. Thus, risk factors for the development of subsequent DTC may be independent of sex. As subsequent DTCs were in general small and not locally invasive, the frequent presence of multifocality may be attributable to tumorigenesis induced or at least promoted by chemo- and/or radiotherapy. 16,24,27 This has important implications for the treatment of subsequent DTCs, particularly regarding assumed papillary microtumor measuring ≤1.0 cm, which may be eligible for omission of RAI therapy in AYAs. 28 –30 Considering the high number of patients with multifocal tumors, a recommendation for total thyroidectomy seems reasonable; however, given the short follow-up duration of our study, definitive statements regarding long-term outcomes and the appropriateness of specific treatments should be approached carefully. Although RAI therapy may be deferred in patients whose stimulated postoperative thyroglobulin values remain within normal limits, ongoing close monitoring is imperative. The option to postpone RAI therapy is supported by the favorable OS and EFS reported in similar studies, such as those by Clement et al., and corroborated by our data. 21 It is important to note that both our study and that of Clement et al. have found no differences in outcomes between patients with subsequent DTCs and those with first DTCs, although longer term studies are needed to fully validate these findings. Preoperative thyroglobulin values were elevated in one-third of our patients only and the median tumor size was 1.1 cm. This may hamper detection of subsequent DTCs in children and adolescents at risk by neck palpation and thyroglobulin values only and, thus, encourage additional ultrasound.
In our study, we grouped neck palpation and thyroid sonography together primarily due to the inconsistent sequencing of these diagnostic procedures in the follow-up visits for our patient cohort. Specifically, some patients initially undergo a thyroid ultrasound by a pediatric radiologist, while others first consult with pediatric oncologists before receiving a similar ultrasound assessment. This variation in practice patterns means that our data may not accurately reflect the specific diagnostic modality initially used to suspect or diagnose DTC. Consequently, to ensure a robust analysis without overinterpreting potentially misleading data distinctions, we opted to analyze these modalities as a combined category. We believe this approach maintains the integrity of our findings despite the inherent complexities in clinical workflow.
Although most frequently detected by surveillance instead of tumor symptoms, the outcome of children and adolescents with subsequent DTCs compared with first DTCs by means of OS and EFS was similar. Although we demonstrated higher rates of total thyroidectomy as first surgical procedure and fewer numbers of diagnostic interventions in children and adolescents with subsequent DTC compared with first DTC, surgery-related morbidity was similar in both groups.
Our study has several shortcomings.
An important limitation of this study is the inability to adjust for potential confounders in all analyses due to the small number of events per variable over time and the low prevalence of certain predictors. Multivariable analyses were therefore not feasible, as they would have yielded biased results. 31 Additionally, the Kaplan–Meier analysis is robust to dropouts and time variable missing data that are not event-related. However, the presence of missing data continues to be a limitation regarding the completeness of the data. 32
The absence of a formal national reference standard to assess the completeness of DTC cases across Germany is another limitation. This prevented us from directly measuring data completeness or comparing it to a standardized reference. Moreover, the GPOH-MET database primarily reflects oncology-directed care, with routine follow-up and primary care likely underrepresented. As a result, data completeness may be higher for patients treated in oncology-focused institutions.
We also acknowledge that differences in thyroid ultrasound screening protocols between patients with a history of malignancy and those without could have impacted the detection rates of DTCs. Most patients with prior malignancies received routine thyroid screenings, whereas others were only screened based on clinical indications, which may have led to earlier or more frequent detection in the oncology-directed group. This disparity in screening methodologies should be considered when interpreting the comparisons between the groups.
Further limitations include the study’s retrospective nature, data availability, limited patient numbers (despite being the largest series), and limited follow-up, which may have influenced our results. This short follow-up period limits our ability to draw definitive conclusions about the long-term outcomes and survival differences between first and subsequent DTCs. A recent report utilizing the Surveillance, Epidemiology, and End Results (SEER) database shows a large divergence in survival between first and subsequent DTCs, although not after propensity matching. 33
Additionally, this study combines a spectrum of thyroid radiation doses and a variety of chemotherapy regimens, which represents a limitation in interpreting the specific impacts of each treatment modality. The necessity to aggregate these data was driven by the limited number of patients available, which precluded more detailed subgroup analyses that might have offered finer distinctions in treatment effects. This aggregation may obscure potential differences in the risk profiles associated with individual treatments, thereby limiting a nuanced understanding of their unique contributions to the development of subsequent DTCs.
Finally, due to the specifications of the MET registry, we only registered patients with subsequent DTCs below the age of 18 years. We did not have data on psychosocial aspects in the management of subsequent DTCs in children and adolescents.
This highlights the need for more extensive follow-up and detailed analyses in future studies to validate our findings and understand the long-term implications of subsequent DTCs.
Conclusions
Children and adolescents with subsequent DTCs who have received chemotherapy alone tend to be diagnosed at younger ages, after shorter latency periods, and with larger tumor sizes compared with those who have undergone both chemotherapy and radiotherapy. Patients with subsequent DTC had smaller sized tumors but were more likely to have multifocal disease than patients with primary DTC. No significant differences in morbidity and mortality were observed in children and adolescents with subsequent compared with first DTCs. The smaller size and multifocal occurrence of subsequent DTCs must be taken into account when deciding on surveillance and management strategies.
Footnotes
Acknowledgments
The authors would like to acknowledge all the treating teams for participating in the MET studies and reporting patient data. The authors thank Thomas Hering for statistical advice.
Data Availability Statement
The data presented in this study are available upon reasonable request from the corresponding author. The data are not publicly available due to restrictions.
Authors’ Contributions
Conceptualization: Mi.K., Ma.K., and A.R. Methodology: Ma.K., Mi.K., P.V., and A.R. Formal analysis: Ma.K., C.M.R., Mi.K., and A.R. Investigation: S.H.W., L.L., T.R.R., C.V., K.W.S., K.L., M.L., M.C.F., and P.V. Resources: A.R. and Mi.K. Data curation: Ma.K., Mi.K., and A.R. Writing—original draft preparation: Mi.K. Writing—review and editing: Mi.K., Ma.K., C.M.R., K.L., M.C.F., and A.R. Visualization: Ma.K. and A.R. Project administration: Mi.K., Ma.K., and A.R. Funding acquisition: Mi.K., A.R., and P.V. All authors have read and agreed to the published version of the article.
Disclosure Statement
The authors have no conflicts of interest to declare.
Funding Statement
The German MET studies were funded by Deutsche Kinderkrebsstiftung, grant number DKS 2014.06, DKS 2017.16, DKS 2021.11, Mitteldeutsche Kinderkrebsforschung, and Magdeburger Förderkreis krebskranker Kinder e.V. The German Childhood Cancer Registry is funded by the Federal Ministry of Health and the Health Ministries of the 16 federal states of Germany. The funding sources were neither involved in the conceptualization, design, content, or preparation of the article nor the decision to submit for publication.