
Abstract
Background:
Medullary thyroid cancer (MTC) is a rare cancer with variable disease course. To enable optimal care, centralization and consensus guidelines are essential. This study describes trends in the incidence, organization of care, surgical treatment, and outcomes of MTC over 30 years in the Netherlands.
Methods:
All patients with a histological MTC diagnosis between 1989 and 2018 were identified from the Netherlands Cancer Registry and linked to the Dutch Pathology register (PALGA). Incidence rates, relative to the Dutch population, were assessed throughout time. Clinicopathological parameters and extent of lymph node (LN) surgery were extracted from PALGA pathology reports. Period A (1989–1998), period B (1999–2008), and period C (2009–2018) were compared.
Results:
Throughout 30 years, the population-adjusted incidence remained stable with 0.17 ± 0.04 diagnoses per 100,000 people per year (p = 0.247). Of all 795 patients, 54% were female and 63% were treated in an academic hospital, at a median age of 48 years (interquartile range [IQR] 34–61). Age at diagnosis increased over time from 42 years (IQR 25–61) in period A to 52 years (IQR 42–63) in period C (p < 0.001). The proportion of treatments occurring in an academic hospital increased from 41% of patients in period A to 58% and 86% in period B and C, respectively (both p < 0.001). At primary treatment, a LN dissection was performed in 582 (73%) patients. Of these patients, 88%, 36%, and 20% underwent a central neck dissection (CND), unilateral neck dissection, and bilateral neck dissection, respectively. CND was performed more frequently in period C (93%) than in period A (77%) or B (87%) (p = 0.009, p = 0.027, respectively). Overall survival improved from period A (55%) to C (88%) and B (65%) to C (p = 0.022, p = 0.007, respectively). Locoregional recurrence rates remained stable.
Conclusions:
This study shows a stable incidence and improved survival of MTC in the Dutch population over the last three decades. In addition, these data indicate a transition of treatment to academic hospitals, likely due to centralization, and a higher rate of CNDs, following the introduction of recommendation guidelines.
Introduction
Thyroid cancer is increasingly diagnosed worldwide and is now the ninth most common type of cancer in the Netherlands. 1 This increase, mostly reflected in the incidence of well-differentiated thyroid cancers, is a result of improved medical care access and diagnostic imaging. 2 –4
Medullary thyroid cancer (MTC) is a distinct subtype that originates from the calcitonin-producing C cells in the thyroid gland and is, therefore, a neuroendocrine tumor with specific histological and clinical characteristics. 5 MTC accounts for approximately 3% of all thyroid cancers and has a 13.5% cause-specific mortality rate at 10 years’ follow-up. 6,7 Although increased incidence rates have been reported in certain populations, 8 –12 studies on MTC incidence in the Dutch population are lacking.
MTC is different from other thyroid cancer types in presentation, metastatic potential, and response to treatment. 5,6,13 In addition, 25% of MTCs are diagnosed early, within the hereditary multiple endocrine neoplasia type 2 (MEN2) syndrome, which often requires prophylactic treatment to prevent clinical disease manifestation. 14 MTCs can have a variable clinical course, ranging from indolent disease with long survival to highly aggressive tumors with rapid progression and death. 14,15 These characteristics present challenges in determining the best treatment and follow-up for each patient.
To provide effective treatment for rare cancers, it is deemed important to centralize to expert centers and collaborate internationally to establish consensus guidelines. Throughout time, several organizations have published guidelines to enable an evidence-based approach. 14,16 According to the 2002 British Thyroid Association guideline and successively published international guidelines, MTC patients should undergo at minimum a total thyroidectomy and central neck dissection (CND). 14,17,18 This guideline was the first step toward a uniform approach across different countries and hospitals. Moreover, collaboration among various health care institutions laid the groundwork for standardization and centralization of rare cancers, including MTC, in the Netherlands. 19,20 However, the impact of these developments on the surgical treatment and oncological outcomes of MTC has not been evaluated in the Dutch population yet.
In this study, we evaluated trends in the incidence, organization of care, surgical treatment, and subsequent outcomes in MTC patients diagnosed between 1989 and 2018 in the Netherlands.
Methods
Data acquisition
All patients with a confirmed histopathological diagnosis of MTC in the Netherlands between 1989 and 2018 were identified from the Netherlands Cancer Registry (NCR). The NCR is a nationwide registry of all cancer diagnoses in the Netherlands. Data from the Dutch Nationwide Pathology Database (PALGA) was linked with NCR data on patient level. PALGA was founded in 1971 and has nationwide coverage since 1991. Cytological diagnoses without histological confirmation were not included. Incidence rates were reported in these patients. Patients without a known vital status and data on type and extent of thyroid surgery were excluded from further analyses.
Definitions
Distinct variables were extracted from the pathology reports, including tumor size, multifocality, bilaterality, characteristics for invasive growth, and extent of surgery. If no parathyroid (PT) tissue was described in the reports, it was assumed to be absent. On the contrary, C cell hyperplasia, extrathyroidal growth, or angioinvasion was only considered present or absent when this was clearly described. In all other cases, it was considered unknown.
Primary surgery was defined as all thyroid and lymph node (LN) surgeries within the first year after diagnosis. Reports that described removed LNs were considered to be neck dissections (NDs). No distinction was made between left- and right-sided CND because this was not clearly reported. We defined locoregional recurrence(s) (LR) as histological evidence for MTC during reoperations >1 year after primary thyroid surgery. Sex, age at diagnosis, total follow-up time, and vital status were determined from NCR data. Population and cancer mortality data were accessed by linkage to the Dutch Municipal Personal Records Database. The hospital indicates the location where (first) thyroid surgery took place. Overall survival was defined as the time between first thyroid surgery and death or last follow-up at the time of data collection. The cause of death or heredity of MTC was not registered in either registry. The period of 30 years was divided into three equal periods of 10 years to allow comparison over time. Periods A, B, and C were defined as 1989–1998, 1999–2008, and 2009–2018, respectively (Fig. 1).

Flowchart displaying patient selection and division into groups based on the year of diagnosis.
Ethics
The scientific boards of PALGA and IKNL (Integraal Kankercentrum Nederland) approved using these (anonymized) epidemiological data, which are considered to be outside the restrictions of the Medical Research Involving Human Subjects Act. All study procedures were performed following the Helsinki Declaration.
Statistics
The incidence rate was based on the Dutch population, per year, as reported by the Dutch Central Agency for Statistics (Supplementary Table S1). 21 Incidence rates were displayed per 100,000 people. Descriptive statistics describe the entire cohort and separate groups, frequencies for categorical variables, and median with interquartile range (IQR) or mean ± standard deviation for continuous variables (depending on distribution). Differences between groups were assessed using Chi-Square or Mann–Whitney U. Kaplan–Meier curves were constructed to evaluate differences in survival and LR between groups. Cox regressions were performed to identify prognostic factors. A p value of < 0.05 was considered statistically significant. Analyses were performed in IBM SPSS Statistics Version 28. Graphs were created in GraphPad Prism Version 8.
Results
Incidence
A total of 818 MTC patients with histological diagnosis were identified from merged PALGA and NCR data. The overall incidence of MTC remained stable over time from 1989 to 2018 (p = 0.247), with an average of 27.27 ± 6.96 diagnoses per year (incidence 0.17 ± 0.04/100,000) (Fig. 2). The mean incidence was 0.17 ± 0.05, 0.15 ± 0.04, and 0.18 ± 0.04 per 100,000 people in periods A, B, and C, respectively, and stable throughout time (period A–B p = 0.326, period B–C p = 0.074, period A–C p = 0.585). When comparing patients with and without histologically confirmed metastatic LNs at diagnosis (N1 and N0, respectively), a rising incidence appeared for N1 patients (p = 0.004).
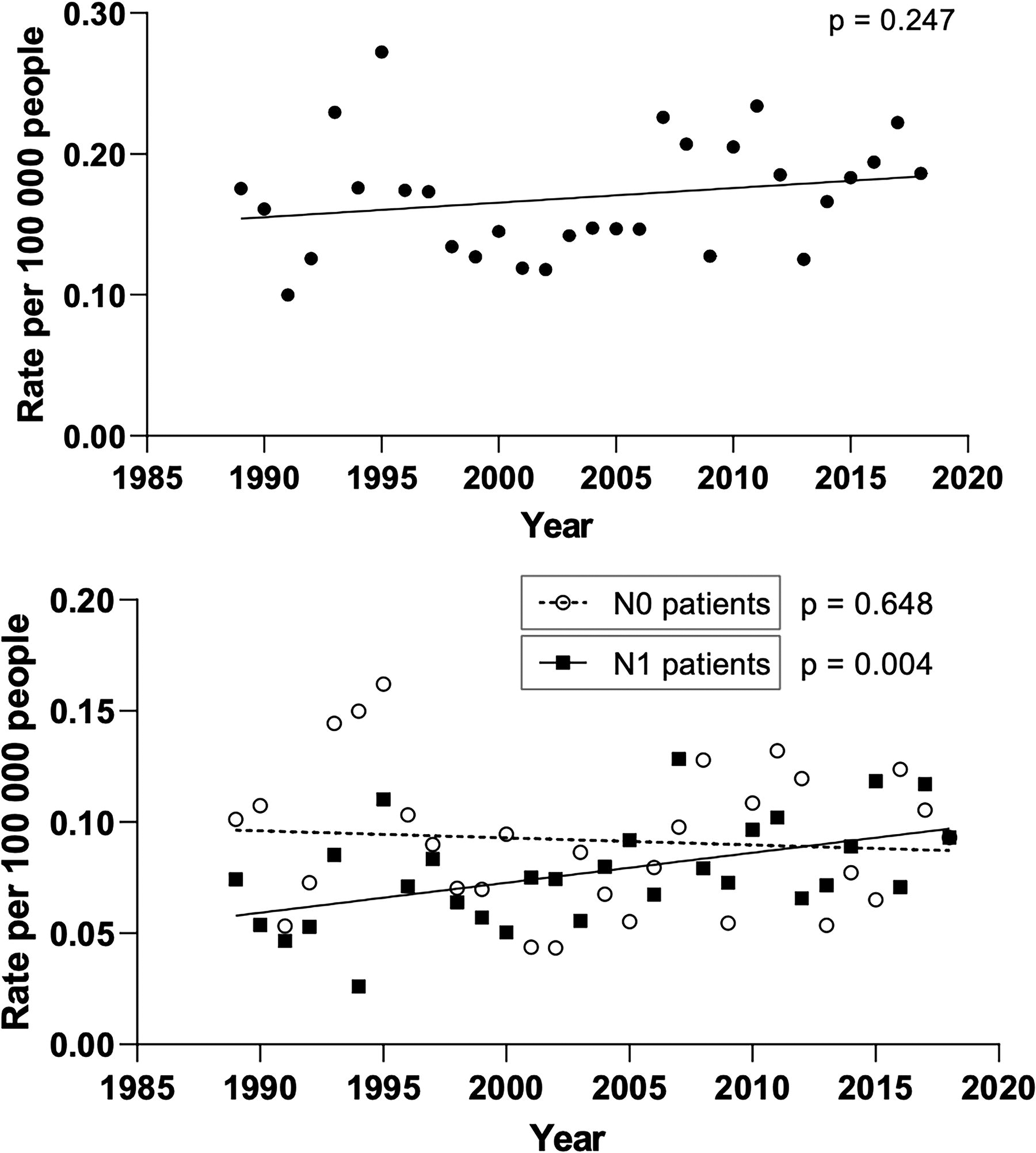
Incidence of medullary thyroid cancer (MTC) patients in the Netherlands between 1989 and 2018, corrected for the Dutch population per year and displayed per 100,000 people. Top graph: all patients. Bottom graph: N0 patients vs. N1 patients. N0 = patients without evidence for metastatic lymph nodes (LNs) upon histopathological examination, N1 = patients with evidence for metastatic LNs upon histopathological examination.
Patient characteristics
For further analyses, we excluded patients without a known vital status (n = 5) and without any details on type and extent of thyroid surgery (n = 18) (Fig. 1). Of the remaining 795 patients, 54% were female and 63% were treated in an academic hospital. The median age at diagnosis was 48 years (IQR 34–61) (Table 1). In periods A, B, and C, MTC was diagnosed in 248 (31%), 242 (30%), and 305 (38%) patients, respectively.
Patients, Surgical Treatment, and Pathology Results—Comparison Between Three Time Periods
The exact extent of the neck dissection was unknown in 21 of all patients. These are excluded in the calculation of p values.
“Available” refers to the number of patients whose data were available from pathology reports.
IQR, interquartile range; TT, total thyroidectomy; CND, central neck dissection; LND, lateral neck dissection; LN, lymph node; ETE, extrathyroidal extension; PT, parathyroid; FU, follow-up; LR, locoregional recurrence.
The sex distribution did not change over time (p = 0.538, p = 0.692, p = 0.802, respectively). However, age at diagnosis increased steadily from 42 years (IQR 25–61) in period A to 52 years (IQR 42–63) in period C (p < 0.001). The proportion of patients treated in an academic hospital increased from 41% in period A to 58% and 86% in period B and C, respectively (p < 0.001, p < 0.001, respectively).
Primary surgery and pathology results
A total thyroidectomy was performed in one or two sessions in 593 (75%) and 158 (20%) patients, respectively. The remaining 44 (6%) patients underwent a subtotal thyroidectomy. A total of 582 patients (73%) underwent an ND during primary treatment; a CND, unilateral lateral neck dissection (LND), and bilateral LND were performed in 509 (87%), 207 (36%), and 118 (20%) patients, respectively. The extent of the primary ND was unknown in 21 (4%) patients, while the laterality of the LND could not be determined in 37 (6%) patients undergoing an ND.
The number of CNDs increased from 101 (77%) and 161 (87%) in period A and B to 247 (93%) in period C (p = 0.009, p = 0.027, respectively), while the number of unilateral or bilateral LNDs remained unchanged throughout time (Table 1).
The average tumor size was 21 mm (IQR 10–39) and remained stable throughout time. Multifocality was more common in period A (85%) and B (79%) than in C (66%) (p < 0.001, p = 0.020 respectively). Similarly, bilateral tumors were most common in period A (46%) in comparison with B (32%) and C (33%) (p = 0.007, p = 0.007). We also identified an increased number of resected PT throughout time (all periods: p < 0.001), which was associated with the number of CNDs (p < 0.001).
The absolute number of metastatic LNs overall, in the central, and in the lateral neck increased over time (Table 1). However, the relative yield of NDs decreased from period A to B and A to C (p = 0.039, p < 0.001, respectively). The same was seen for the proportion of metastatic LNs removed from the lateral neck (p = 0.034, p = 0.003, respectively). In contrast, the yield of CNDs decreased only from period A to C (p < 0.001).
Overall survival and LR
At final follow-up, 109 months (IQR 47–212) after diagnosis, 71% of patients were alive (Table 2). Median time from diagnosis to death was 52 months (IQR 23–120). The 5-, 10-, 15-, and 20-year overall survival rates were 85%, 78%, 75%, and 73%, respectively. Out of all patients, 119 (15%) developed at least one LR requiring surgery, with 77 (65%), 26 (22%), 9 (8%), and 7 (6%) patients requiring one, two, three, and four surgeries for LRs, respectively. The median time to the first LR was 34 months (IQR 18–73) after (first) thyroid surgery. Figure 3 displays the cumulative percentage of all patients that were operated on (at least one) LR and died over time, after primary treatment. Table 2 and Figure 4 show the location of LR in LNs. Out of the 117 patients with at least one LR in locoregional LNs, 50% had a central neck LR and 80% had a lateral neck LR, in any of the LRs.
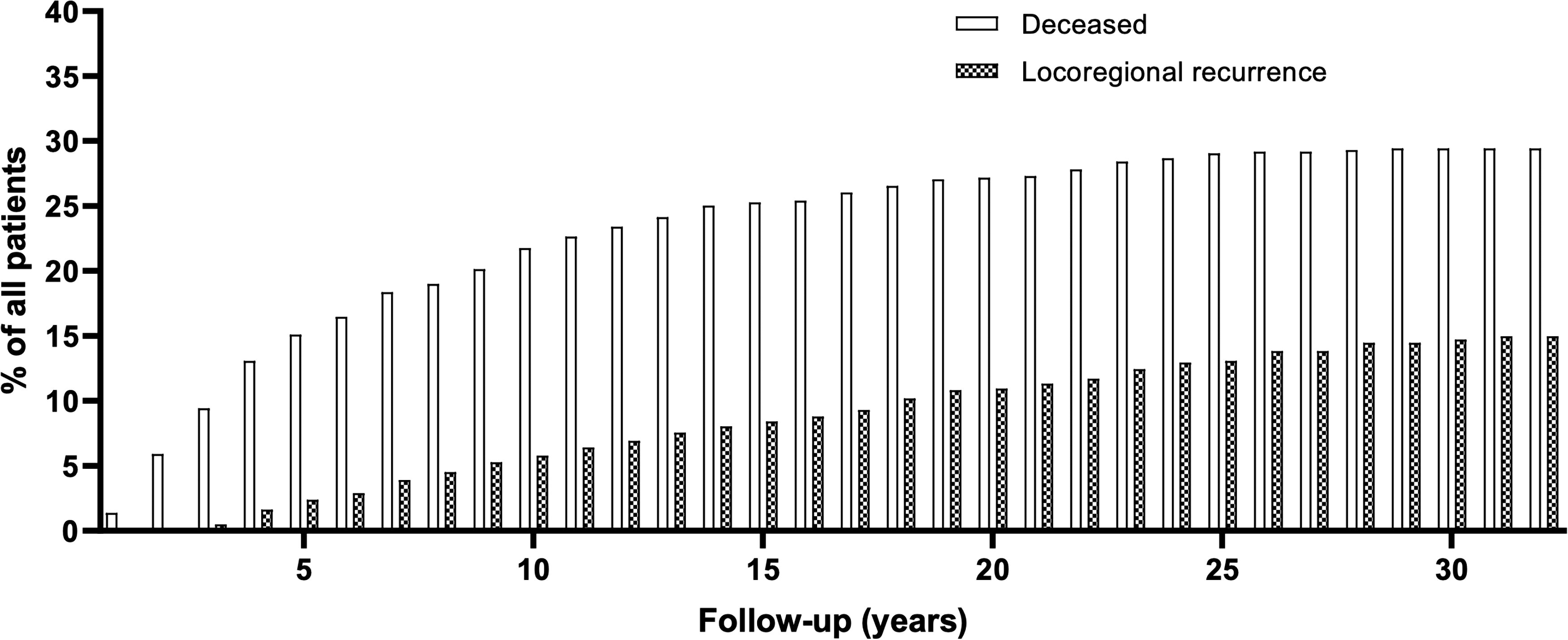
Overall survival and surgeries for locoregional recurrence(s) over time after diagnosis. Cumulative percentages are shown. The cause of death was not known.
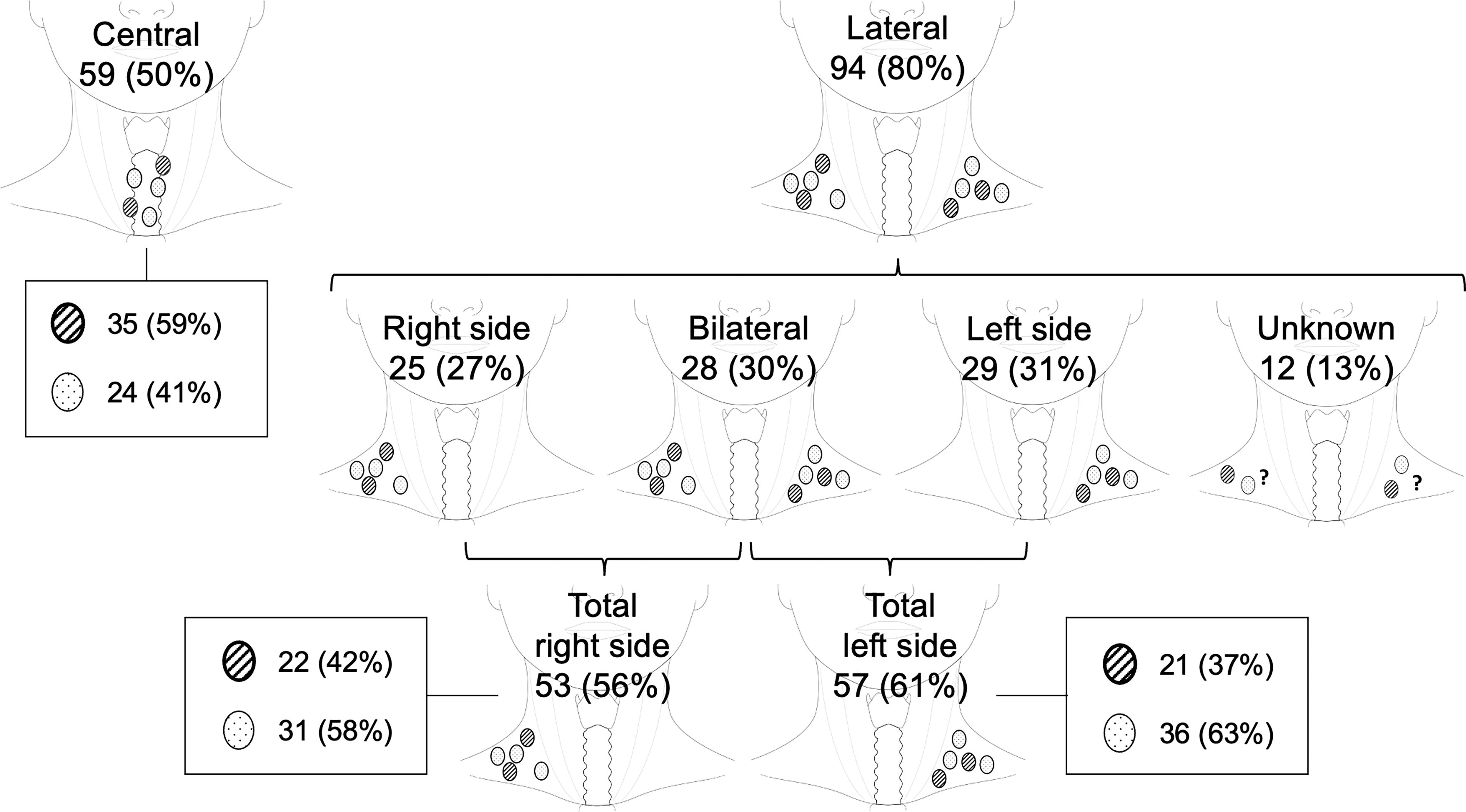
Locations of locoregional recurrences (LRs) in Lymph Nodes. Of 119 patients with at least one LR, 2 patients had a hemithyroidectomy >1 year after primary surgery, while 117 patients had (at least one) LR in locoregional lymph nodes. The latter are displayed here. The circles with diagonal hatching indicate LRs in a neck compartment that was previously operated during primary surgery. Circles with dotted hatching indicate LRs in a neck compartment that was not yet operated on during primary surgery.
Overall Survival and Locoregional Recurrence(s) in Patients After Primary Surgery
Of 119 patients with at least one locoregional recurrence, 2 patients had a hemithyroidectomy >1 year after primary surgery, while 117 patients had (at least one) LR in locoregional lymph nodes.
Log rank test.
Of the 59 patients with an LR in the central neck, the central neck was also dissected during primary surgery in 35 (59%) patients, and in 24 (41%) patients the central neck was dissected for the first time for an LR (Fig. 4). Of 53 patients with an LR in the right lateral neck, 22 (42%) patients had already had a right-sided LND during primary surgery, while 31 (58%) did not. Of 57 patients with an LR in the left lateral neck, 21 (37%) patients had already had a left-sided LND during primary surgery, while 36 (63%) did not.
In period C, overall survival was significantly higher (88%) in comparison with A (55%) and B (65%) (p = 0.022, p = 0.007, respectively) (Table 2, Fig. 5). The number of LRs requiring surgery did not increase (p = 0.111, p = 0.085, p = 0.854, respectively), while the time to first LR did shorten from period A (63 months [IQR 26–133]) to B (27 months [IQR 15–67]) and C (30 months [IQR 17–46]) (p = 0.004, p = 0.007, respectively). Significantly more patients in period C had an LR in an area of the neck that was also operated during primary surgery than in period A (p = 0.019, p < 0.001, p = 0.010, respectively).
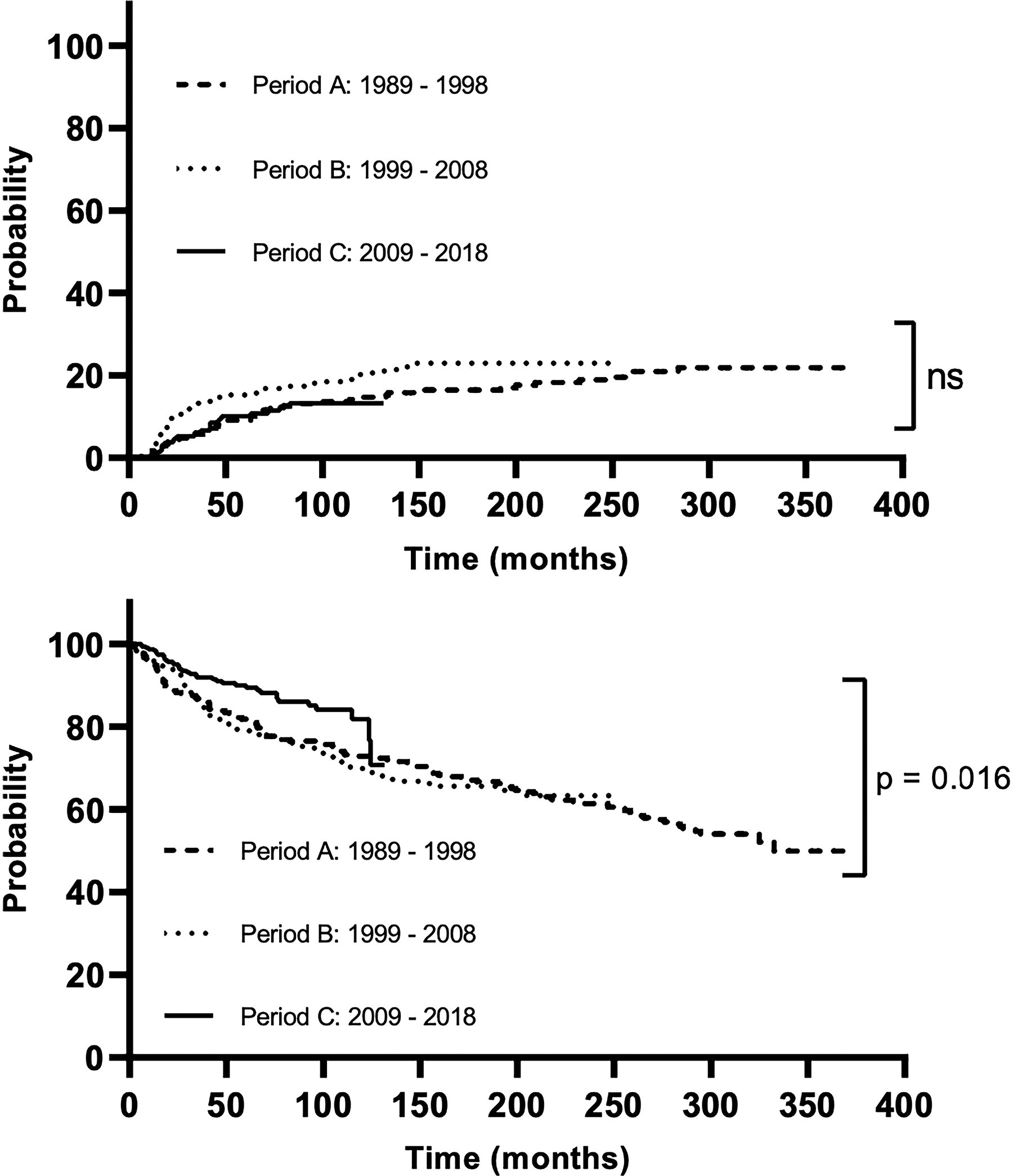
Probability of locoregional recurrence and overall survival in period A (1989–1998), B (1999–2008), and C (2009–2018). Top graph: locoregional recurrence probability. Bottom graph: overall survival probability.
In univariable Cox regression analyses for LR, angioinvasion (hazard ratio [HR] 4.689, p < 0.001) and metastatic LNs at diagnosis (HR 5.565, p < 0.001) gave a higher risk for LR, while female sex (0.726, p = 0.082) and C cell hyperplasia (HR 0.506, p = 0.035) lowered the risk (Table 3). In multivariable Cox regression, only metastatic LNs remained a significant predictor for LR (HR 9.984, p = 0.039). Age >55 years (HR 5.192, p < 0.001), tumor size >2 cm (HR 1.742, p = 0.002), angioinvasion (HR 7.278, p < 0.001), extrathyroidal extension (HR 4.747, p < 0.001), a positive resection margin (HR 4.152, p < 0.001), and metastatic LN at diagnosis (HR 3.901, p < 0.001) increased the risk of death due to all causes in univariable analyses, while female sex (HR 0.609, p < 0.001), treatment in an academic hospital (HR 0.623, p < 0.001), and C cell hyperplasia (HR 0.354, p < 0.001) lowered this risk (Table 4). None of the associations remained significant in the multivariable analysis.
Cox Regression Analysis for Locoregional Recurrence in All Patients
HR, hazard ratio; CI, confidence interval.
Cox Regression Analysis for Death (All Causes) in All Patients
HR, hazard ratio; CI, confidence interval.
Discussion
Over the past decades, there have been significant advancements and new insights in the diagnosis and treatment of MTC. This nationwide study evaluated trends in the incidence, organization of care, and treatment of MTC patients over 30 years in the Netherlands. Despite a general increase in thyroid cancer incidence, MTC incidence remained stable. Moreover, a changed organization of care, with patients increasingly being treated at academic hospitals, and the introduction of management guidelines that advised dissection of the central neck compartment, were apparent. The stable LR rates and improved overall survival highlight the persistent challenge of providing curative surgery and suggest a potentially improved prognosis for MTC patients.
Between 1989 and 2018, the incidence of MTC in the Netherlands remained stable, while other countries showed an increase. 8,9,11,22,23 However, a Danish and an earlier Dutch study (1989–2009) also established a stable incidence. 10,24 Improved diagnostic methods, better access to health care, 2 –4 and routine health screenings may be the reasons for the growing incidence of thyroid cancer. 11,25 Dutch health care is relatively restrictive in the use of diagnostic methods 26 and we do not recommend routinely screening for calcitonin before thyroid surgery, 27,28 possibly explaining the stable incidence and tumor size over time. The improved quality of diagnostic imaging modalities and an increase in CNDs could clarify the rise in patients with metastatic LNs.
Upon analysis of the cohort, we noticed a higher age at diagnosis in the latter decades. Similar findings were seen in studies of Israel and the United States. 11,22 This increase in age can be partially attributed to the aging population, with a higher proportion of elderly people in general. 29 Sporadic MTCs typically manifest at a higher age than hereditary MTCs. 9,10 Combined with less multifocality, bilaterality, and C cell hyperplasia, which are associated with hereditary disease, 30 a potential rise in the prevalence of sporadic MTCs may also be inferred. Previous studies have also indicated a rise in sporadic MTCs. 10,22 A recent study in the Netherlands found a higher incidence of pediatric MTCs in the 1990s compared with the two consecutive decades, possibly due to a relative peak in the number of hereditary diagnoses shortly after the discovery of RET gene mutations responsible for MEN2. 31 The results align with a German study that identified more familial MTC diagnoses in 1991–2000 than in 1951–1991. 32 Although de novo germline RET mutations can still occur, the increase in sporadic MTC cases may be a likely explanation for our findings.
International collaboration and centralization of care in expert centers are crucial to improve the quality of treatment and, ultimately, patient outcomes. 33,34 This is particularly important for rare cancers, where limited hospital cases hinder large prospective studies and robust evidence-based guidelines. In 2002, the British Thyroid Association published the first thyroid cancer guidelines, which recommended total thyroidectomy and CND for MTC patients. 17 Our data reflect the introduction of this and successive guidelines, with an evident rise in CNDs over time.
Likely due to the often prophylactic nature of CNDs, the total number of patients with metastatic LNs increased, while the proportion decreased. The actual rate of metastasis was 50% in the last decade, which is comparable with recent literature (52%), 35 but lower when compared with older studies (78–80%). 36,37 We also show that metastatic LNs at diagnosis raise the risk for an LR during follow-up, which concurs with literature, 34,38,39 and highlights the importance of knowing LN involvement for accurate risk stratification at baseline.
Surgeries in high-volume centers lead to lower postoperative morbidity and mortality rates. 40 Moreover, collaborative networks can result in fewer second opinions, lower readmissions, and reduced costs. 41 –43 Following the Council of the European Union’s 2009 proposal for centralization, the Dutch Foundation for Oncological Collaboration (in Dutch: Stichting Oncologische Samenwerking [SONCOS]), IKNL, and ZonMw, a financial subsidiary of the Dutch government, published several reports advocating for centralization of rare cancers to expert centers. 19,20,44,45 Our data show that centralization of MTC patients to academic hospitals increased from 41% to 86% in the last decade. A recent study in southern Netherlands also noted increased centralization of complex thyroid cancer patients over time. 46 However, anticipated changes in postoperative morbidity were not seen, likely because large cohorts are required to detect rare outcome differences. Although postoperative morbidity was not assessed here, we did observe improved overall survival over time, indicating a possibly improved prognosis for MTC patients. 31 This contrasts with a recent analysis of the MTC population in the United States, which reported an increased mortality from 2000 to 2019. 23 However, due to lacking cause-of-death data in both studies, an association with MTC-related parameters cannot be established.
This study also sheds light on LRs that require surgery after primary treatment. With the enforced definition in this study, an overall LR rate of 15% was determined, which is comparable with recent studies on reoperations for cervical recurrences. 47,48 Papachristos et al. also reported that recurrent surgery occurred most often in a previously unaffected (and unoperated) lateral compartment. 48 This concurs with our data on the total period of 30 years, with 58–63% of lateral LRs being in an area not operated during primary surgery.
However, in recent years, more lateral LRs occurred in an already operated area (62–77%). One could hypothesize that, as imaging improved over time, primary surgery on the lateral neck became more restrictive and precise. The proportion of radical LNDs may have decreased, while the proportion of level-oriented LNDs (level-picking) possibly increased. Since no distinction between level-oriented and compartment-oriented LNDs was made in this article, it could therefore seem as though surgery in an already operated area increased, while this is not necessarily true. This would also explain why the extent of LNDs during primary treatment and rate of LRs remained stable in our study. Altogether, these data highlight the challenges of providing curative surgery once lateral neck LN metastases have been established in MTC patients.
This study has several limitations to report. To exclude the uncertainty in cytology results, cytological MTC diagnoses without histopathological confirmation were excluded, which may have underreported the incidence in all decades. Moreover, patients with biochemical persistent or recurrent disease, without requiring surgery in the follow-up, are missed in the current definition of LR, since no data on tumor markers were available. This may have resulted in an underestimation of LR rates. In addition, due to less elaborate assessment of thyroid specimens in the early years, possibly lacking nationwide coverage from 1989 to 1990, and the deficient uniformity in the histopathology reports, not all intended data could be extracted. However, by presenting the amount of available data in addition to the actual data, the impact on the presented results could be safely overcome without compromising quality. Finally, all reported LNs were considered to have been dissected in an ND, even though some central LNs may have been removed unintentionally. Nevertheless, this large nationwide study provides strong and representative data on the Dutch MTC population that underwent thyroid surgery with very little selection bias.
In conclusion, the evaluation of this extensive cohort of MTC patients demonstrates a strikingly stable incidence of MTC in The Netherlands over 30 years. Treatment of MTC patients shifted to academic hospitals, likely due to centralization, and the number of (prophylactic) CNDs increased, following international guidelines recommendations. Despite the noted changes, the LR rate requiring surgery remained stable, while overall survival improved steadily.
Footnotes
Acknowledgments
The authors would like to express their gratitude to PALGA and IKNL for their ongoing efforts in collecting and providing nationwide data to make the current research study possible. In addition, the authors acknowledge that the abstract was previously published in Endocrine Abstracts (2024) 101 PS1-04–02 | DOI: 10.1530/endoabs.101.PS1-04–02.
Authors’ Contributions
E.C.J.: Conceptualization, data curation, formal analysis, investigation, methodology, project administration, visualization, and writing—original draft. M.J.H.M.: Conceptualization, data curation, investigation, and writing—review and editing. I.A.C.T.: Data curation, project administration, and writing—review and editing. W.T.Z.: Writing—review and editing. L.J.: Writing—review and editing. B.M.v.H.: Data curation and writing—review and editing. L.L.: Writing—review and editing. M.R.V.: Writing—review and editing. M.F.M.v.d.B.: Writing—review and editing. A.F.E.: Writing—review and editing. K.M.A.D.: Writing—review and editing. R.T.N.-M.: Writing—review and editing. T.M.v.G.: Writing—review and editing. R.P.P.: Writing—review and editing. E.d.H.: Writing—review and editing. T.P.L.: Conceptualization, resources, supervision, and writing—review and editing. S.K.: Conceptualization, resources, supervision, and writing—review and editing.
Author Disclosure Statement
The authors declare no conflict of interest.
Funding Information
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Supplementary Material
Supplementary Table S1