
Abstract
Background:
The 2022 World Health Organization classification introduced the term high-grade follicular cell-derived nonanaplastic thyroid carcinoma (HGFCTC) to define invasive/infiltrative nonanaplastic thyroid carcinoma with high-grade features, including poorly differentiated thyroid carcinoma and high-grade differentiated thyroid carcinoma. Our objectives were to compare clinicopathological characteristics, oncologic outcomes, and mutation profiles among HGFCTC subgroups to better inform prognostication and treatment.
Methods:
In this single-center, retrospective cohort study of 252 patients who had surgery for HGFCTC from 1986 to 2020, we categorized HGFCTC and its related entity, “encapsulated noninvasive neoplasms of follicular cells with high-grade features,” into five subgroups: (A) encapsulated noninvasive, (B) encapsulated with capsular invasion only (minimally invasive), (C) encapsulated angioinvasive with focal vascular invasion (VI), (D) encapsulated angioinvasive with extensive VI, and (E) infiltrative tumors. Next-generation sequencing with Memorial Sloan Kettering Cancer Center-Integrated Mutation Profiling of Actionable Cancer Targets was available for 117/252 patients to investigate differences in mutation profiles.
Results:
The cohort comprised 50% infiltrative, 33% encapsulated angioinvasive, and 18% encapsulated noninvasive/minimally invasive tumors. No patients with encapsulated noninvasive or minimally invasive disease had regional or distant metastases at presentation. Patients with infiltrative tumors were significantly more likely to present with T3/T4 disease (71%), regional metastases (55%), and distant metastases (25%) (p ≤ 0.003). Five-year disease-specific survival was poorer in patients with infiltrative disease (67.7%), compared to encapsulated angioinvasive focal VI (90.4%), encapsulated angioinvasive extensive VI (88.1%), and encapsulated noninvasive/minimally invasive (100%) (p = 0.0002) subgroups. Common mutations were TERT (42%), BRAFV600E (29%), NRAS (27%), EIF1AX (11%), and TP53 (9%). Pathways altered included RTK/RAS/RAF/MAPK (69%), PI3K/AKT/MTOR (14%), histone methyltransferases (9%), and SWI/SNF chromatin remodeling complex (8%). Subgroup analysis showed the infiltrative subgroup was mainly BRAFV600E -driven, and the encapsulated angioinvasive and minimally invasive subgroups were NRAS-driven. Encapsulated noninvasive tumors had a different mutation profile, with DICER1 as the main driver mutation.
Conclusions:
HGFCTC comprises different subgroups with different clinical behaviors determined by the extent of vascular invasion and degree of infiltration. Excellent recurrence and survival outcomes occur in encapsulated noninvasive and minimally invasive tumors compared to infiltrative tumors. Infiltrative tumors are largely “BRAF-like,” whereas encapsulated angioinvasive tumors are “RAS-like.” Encapsulated noninvasive tumors have a particularly unique molecular profile consisting of DICER1 mutations and a lack of BRAFV600E mutations.
Introduction
The 2022 World Health Organization (WHO) defines high-grade follicular cell-derived nonanaplastic thyroid carcinoma (HGFCTC) as an invasive/infiltrative nonanaplastic thyroid carcinoma with high-grade features, including both poorly differentiated thyroid cancer (PDTC) and high-grade differentiated thyroid carcinoma (HGDTC). 1,2 PDTC is defined by the Turin criteria, 3 which include (i) presence of a solid/trabecular/insular pattern of growth, (ii) absence of conventional nuclear features of papillary carcinoma, and (iii) presence of at least one of the following: convoluted nuclei, mitotic count ≥3 per 2 mm2, and/or tumor necrosis. HGDTC is defined as having cytoarchitectural features of well-differentiated thyroid carcinoma (WDTC) but with elevated mitotic count (≥5 per 2mm2) and/or tumor necrosis. Lesions that exhibit high-grade features but do not meet the criteria for HGDTC definition due to their noninvasive nature are defined as “encapsulated noninvasive neoplasms of follicular cells with high-grade features”. 1,4 HGFCTC has an intermediate prognosis between WDTC and anaplastic thyroid carcinoma (ATC), 4,5 but encapsulated HGFCTC appears to have better outcomes than the more common unencapsulated or infiltrative HGFCTC. 4,6,7 More data on recurrence and survival outcomes are needed for patients with encapsulated HGFCTC, with or without vascular invasion, to better inform treatment decisions following lobectomy, particularly whether to decide for or against completion of thyroidectomy and radioactive iodine (RAI).
In this study, we categorized HGFCTC and tumors designated as “encapsulated noninvasive neoplasms of follicular cells with high-grade features” into subgroups based on encapsulation and extent of invasion. These subgroups include (A) encapsulated noninvasive (i.e., encapsulated noninvasive neoplasms of follicular cells with high-grade features), (B) encapsulated with capsular invasion only (minimally invasive), (C) encapsulated angioinvasive with focal vascular invasion (VI) (<4 foci), (D) encapsulated angioinvasive with extensive VI (≥4 foci), and (E) infiltrative tumor lacking complete encapsulation. Our objectives were to compare tumor characteristics and oncologic outcomes between these subgroups and use next-generation sequencing (NGS) data to investigate differences in mutation profile to better inform prognostication and treatment.
Materials and Methods
Patients and tumor samples
Following approval from the institutional review board (17-103) at Memorial Sloan Kettering Cancer Center (MSK) for this retrospective cohort study, we queried our prospectively maintained database and identified 252 patients who had surgery for HGFCTC from 1986 to 2020. Paraffin-embedded tissue blocks from primary tumors were available for all patients. Hematoxylin- and eosin-stained tumor sections and immunostains were evaluated by two head and neck pathologists (R.A.G. and B.X.). The tumors were labeled according to the most recent WHO classification. Briefly, a tumor was labeled HGFCTC if it fulfilled the Turin criteria for PDTC or the WHO criteria for HGDTC 1,3 (Supplementary Table S1). The term “encapsulated noninvasive neoplasms of follicular cells with high-grade features” was utilized for lesions that exhibit high-grade features (necrosis and/or high mitotic count) yet do not meet the definition of HGDTC due to lack of invasion. 1,4 HGFCTCs and “encapsulated noninvasive carcinoma with high-grade features,” were subclassified as follows: (A) encapsulated noninvasive (i.e., encapsulated thyroid carcinoma with high-grade features noninvasive), (B) encapsulated with capsular invasion only (minimally invasive), (C) encapsulated angioinvasive with focal vascular invasion (VI) (<4 foci), (D) encapsulated angioinvasive with extensive VI (≥4 foci), and (E) infiltrative tumor lacking complete encapsulation. The infiltrative subgroup is defined by the lack of complete encapsulation and the presence of infiltration in the adjacent thyroid parenchyma. Figures 1 and 2 show microscopy images of each subgroup.

Patient and tumor characteristics
Data were collected on age, sex, tumor-node-metastasis (TNM) stage, tumor necrosis (present or absent), mitotic count (number of mitosis/2 mm2), microscopic and gross extrathyroidal extension, margin status, multifocality, and extranodal extension, as previously described. 4
Next-generation sequencing
DNA from tumor and matched normal (non-neoplastic) tissue specimens was available for 117 of the 252 patients. These were sequenced using the MSK-IMPACT (MSK-Integrated Mutation Profiling of Actionable Cancer Targets) platform, a deep-coverage, targeted NGS assay encompassing 505 cancer-related genes. 8 cBioPortal for Cancer Genomics (http://www.cbioportal.org/) was used to analyze mutation profiles. 9
Oncological outcomes and statistics
Patient and tumor characteristics of 252 patients were compared between subgroups using the Pearson χ2 test or Fisher’s exact test for categorical variables and Kruskal–Wallis rank-sum or Mann–Whitney U test for continuous variables. Significance was considered at p < 0.05. Recurrence was defined as a new disease after completion of treatment, proven on biopsy or identified by computed tomography, ultrasound, magnetic resonance imaging, positron emission tomography (PET), or RAI scanning. Survival analyses were performed with Cox proportional hazards models, calculated using the Kaplan–Meier method and log-rank tests to compare overall survival (OS), disease-specific survival (DSS), and recurrence-free survival probability (RFSP). Factors found significant in the univariable analysis were included in the multivariable analysis. All analyses were performed in R version 4.2.0 (R Core Team, 2022).
The mutational landscape was compared between subgroups for patients whose DNA was available (n = 117) for NGS. Survival analyses were performed using the Kaplan–Meier method for specific gene mutations and compared using the log-rank test.
Results
Patient, tumor, and treatment characteristics
Table 1 shows the clinical, pathological, and treatment characteristics of the cohort of 252 patients. The median age was 57 years (interquartile range [IQR], 42–70 years), and 62% (157/252) were female. The tumor stage was pT3/4 in 54% of patients. Metastatic spread to central compartment neck lymph nodes (pN1a disease) was present in 14% of patients and to lateral compartment lymph nodes (pN1b disease) in 16%; 69% of patients had no regional lymph node metastasis, and 21% had distant metastases. Postoperative histopathology identified positive margins in 29% of patients, gross extrathyroidal extension in 36%, microscopic extrathyroidal extension in 48%, and extranodal extension in 46%. Marked increase in mitotic count (≥5/2 mm2) was identified in 52% and mild to moderate mitotic count (1–4/2 mm2) in 33%. Necrosis was identified in 59% and multifocality in 45%. Patients were treated with total thyroidectomy in 75% of cases and thyroid lobectomy or isthmusectomy in 24%. Neck dissection was performed in 32% of patients (18% central and lateral; 13% central only; 0.8% lateral only). Adjuvant RAI was given in 74% of cases and adjuvant radiotherapy in 8%.
Clinical, Pathological, and Treatment Characteristics
Unknowns excluded from table.
ENE, extranodal extension; ETE, extrathyroidal extension; HGFCTC, high-grade follicular cell-derived nonanaplastic thyroid carcinoma; IQR, interquartile range; RAI, radioactive iodine; RT, radiotherapy; VI, vascular invasion.
Comparison of clinical and tumor characteristics of subgroups
Sixteen tumors could not be classified because slides were unavailable, rendering the assessment of invasion impossible, leaving 236 patients to be categorized as follows: (A) encapsulated noninvasive in 12% (28/236), (B) encapsulated with capsular invasion only (minimally invasive) in 5.5% (13/236), (C) encapsulated angioinvasive with focal VI in 9.3% (22/236), (D) encapsulated angioinvasive with extensive VI in 24% (56/236), and (E) infiltrative in 50% (117/236).
Table 2 presents a comparison of clinical and pathological characteristics among the five subgroups, categorized by the presence of encapsulation and extent of invasion. Patients with infiltrative disease were older at presentation (median 59 years) than patients with minimally invasive disease and encapsulated noninvasive disease (median 47 and 50 years, respectively; p = 0.074). There was a significant difference in sex distribution, with a higher proportion of male patients in the infiltrative (43%) and encapsulated angioinvasive with extensive VI (45%) and focal VI (41%) subgroups than in the minimally invasive (7.7%) and encapsulated noninvasive (14%) (p = 0.005) subgroups. T3 or T4 disease was significantly more common in patients with infiltrative tumors (82/116; 71%) than in patients with encapsulated angioinvasive with extensive VI (30/55; 55%), encapsulated angioinvasive with focal VI (7/22; 32%), minimally invasive (2/13; 15%), and encapsulated noninvasive (3/27; 11%) tumors (p < 0.001). There was a significant difference in incidence of regional lymph node metastases across subgroups (p < 0.001): no patients with encapsulated noninvasive (0/28; 0%) or minimally invasive disease (0/13; 0%) had regional lymph node metastases, compared to 4.5% (1/22) of patients with encapsulated angioinvasive tumors with focal VI, 8.9% (5/56) with encapsulated angioinvasive tumors with extensive VI, and 55% (63/115) with infiltrative tumors. There was a significant difference in incidence of distant metastases across subgroups (p = 0.003): no patients with encapsulated noninvasive (0/28; 0%) or minimally invasive (0/13; 0%) tumors had distant metastases at presentation, compared to 23% (5/22) of encapsulated angioinvasive with focal VI, 25% (14/56) of encapsulated angioinvasive with extensive VI, and 25% (29/117) of infiltrative tumors. Significantly more patients with infiltrative disease had positive margins on histopathology (55/110; 55%) than patients with encapsulated noninvasive (0/28; 0%), and minimally invasive disease (0/13; 0%) (p < 0.001).
Clinical, Pathological, and Treatment Characteristics by Subgroup
Kruskal–Wallis rank-sum test; Pearson’s chi-squared test; Fisher’s exact test. Unknowns excluded.
VI, vascular invasion; IQR, interquartile range, ENE, extranodal extension; RT, radiotherapy; RAI, radioactive iodine.
Table 2 also presents a comparison of treatment characteristics among the five subgroups. Patients with infiltrative disease were more likely to undergo total thyroidectomy (100/117; 85%) than other subgroups; total thyroidectomy was least likely in patients with encapsulated noninvasive disease (11/28; 39%; p < 0.001). Similarly, neck dissection was significantly more common in patients with infiltrative disease (51% vs. ≤18% in other subgroups; p < 0.001). Postoperative RAI was administered in 36% of patients with encapsulated noninvasive disease, compared to ≥70% of other subgroups (p < 0.001). Forty patients with distant metastases at presentation had postoperative RAI treatment: RAI uptake was evident in at least one metastatic foci in 100% of distant metastases in the encapsulated angioinvasive extensive VI subgroup (12/12), encapsulated angioinvasive focal VI subgroup (3/3) and minimally invasive subgroup (1/1). RAI uptake was evident in 81% (17/21) of distant metastases in the infiltrative subgroup. Postoperative radiotherapy was only administered to patients with infiltrative (17/116; 15%) and encapsulated angioinvasive with extensive VI (3/56; 5.4%) tumors (p = 0.028).
Comparison of survival and recurrence outcomes of each HGFCTC subgroup
The median follow-up was 62.8 months (IQR, 32–115 months). Figure 3A shows OS stratified by subgroup. There were statistically significant differences between groups (p = 0.0022). Patients with encapsulated noninvasive (96.4% 5-year OS) and minimally invasive (90.9% 5-year OS) disease had superior OS. Patients with infiltrative disease had the worst 5-year OS at 62.7%. Patients with encapsulated angioinvasive disease with extensive VI had similar OS to patients with encapsulated angioinvasive disease with focal VI (82.2% and 81.6% 5-year OS, respectively).
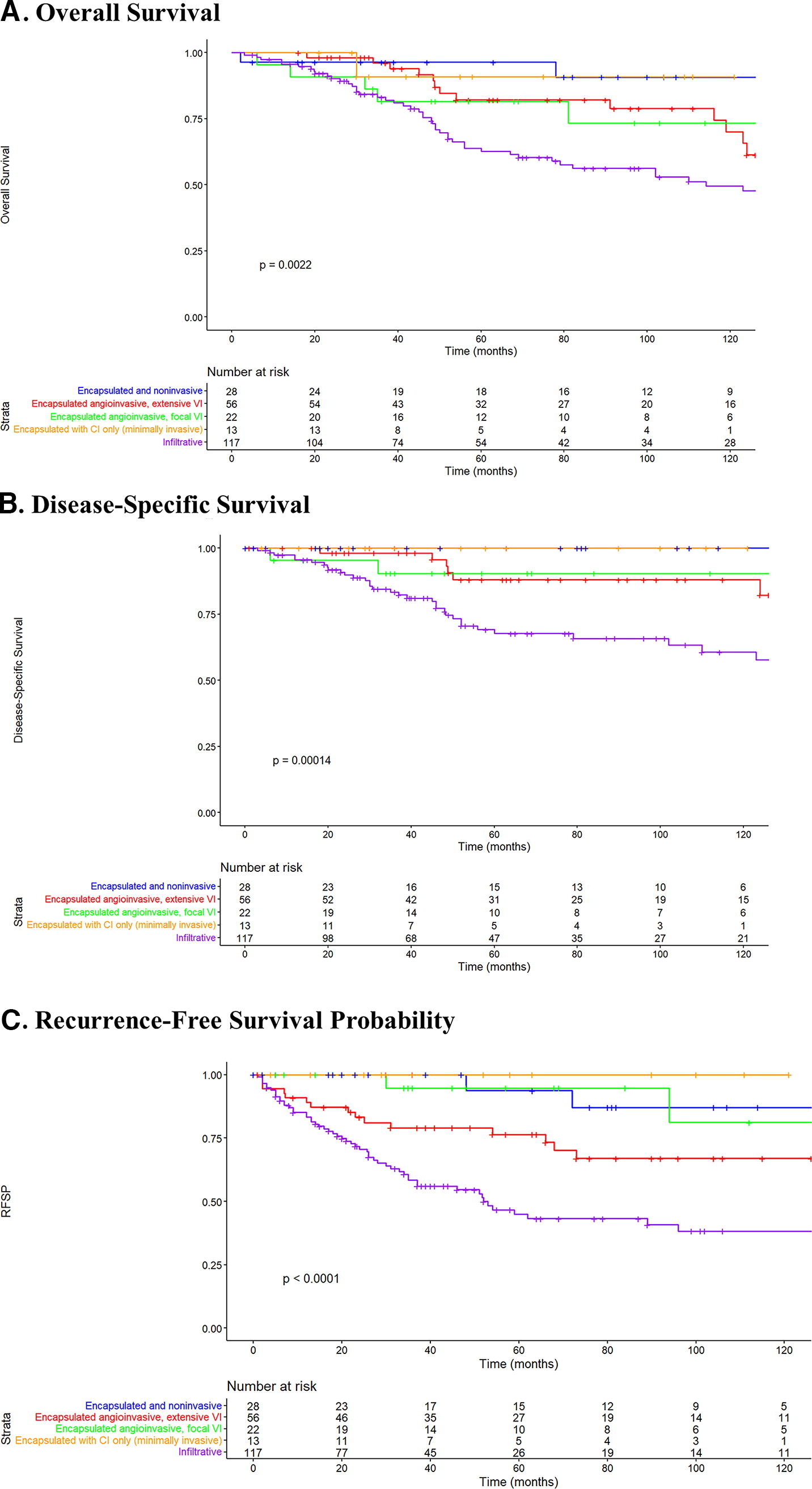
There were statistically significant differences in 5-year DSS between subgroups (p = 0.00014) (Fig. 3B). Patients with encapsulated noninvasive and minimally invasive disease had 100% 5-year DSS, compared to 67.7% DSS in patients with infiltrative tumors. Patients with encapsulated angioinvasive with extensive VI disease and encapsulated angioinvasive with focal VI disease had similar DSS (88.1% and 90.4% 5-year DSS, respectively).
There were also significant differences in recurrence between subgroups (p < 0.0001). Figure 3C shows the 5-year RFSP across subgroups: 100% (13/13) in minimally invasive disease, 96.4% (27/28) in encapsulated noninvasive disease, 94.7% (21/22) in encapsulated angioinvasive with focal VI disease, 76.4% (44/56) in encapsulated angioinvasive with extensive VI, and 45% (65/117) in infiltrative disease. When broken down by location of recurrence, 5-year local RFSP was 100% in encapsulated noninvasive, minimally invasive, and encapsulated angioinvasive with focal VI tumors, 94.7% in encapsulated angioinvasive with extensive VI and 86.7% in infiltrative tumors (p = 0.055). Five-year regional RFSP was 89.2% in encapsulated noninvasive, 100% in minimally invasive and encapsulated angioinvasive with focal VI tumors, 89.2% in encapsulated angioinvasive with extensive VI, and 69.1% in infiltrative tumors (p < 0.0001).
Five-year distant RFSP was 93.8% in encapsulated noninvasive, 100% in minimally invasive, 94.7% in encapsulated angioinvasive with focal VI, 83.4% in encapsulated angioinvasive with extensive VI, and 61.4% in infiltrative tumors (p = 0.0011).
Two patients with encapsulated noninvasive tumors experienced distant recurrence: One 42-year-old female patient with a 2.9 cm encapsulated follicular variant of papillary carcinoma with 7 mitoses per 2 mm2 primary tumor developed a unifocal metastasis to a thoracic vertebra 4 years after diagnosis, despite lobectomy followed by completion thyroidectomy and RAI therapy. This was treated with external beam radiation. On the latest follow-up, there is no structural evidence of recurrence, but she does have a biochemically incomplete response. The primary tumor harbored NRASQ61K and SMARCA4 G1232D mutations, while the distant deposit also contained NRASQ61R as well as MAP2K2 and TERT C228T promoter mutations. The second patient is a 54-year-old female with a 2.5 cm encapsulated follicular variant of papillary carcinoma with 5 mitoses per 2 mm2 primary tumor who was treated by lobectomy alone and recurred in the femur 6 years later, presenting with a pathological fracture and treated with surgery. She then underwent a completion thyroidectomy (benign pathology) and radioactive iodine treatment. She was subsequently treated with radiation to humeral and adrenal metastases before being commenced on pazopanib due to increased bone and hepatic metastases. She is currently alive with distant disease. The primary tumor carried NRASQ61R, EIF4A2I252V, and FOXA1E421K mutations. Both patients had the entire primary tumor thyroidectomy specimen submitted for microscopic examination and their distant metastasis confirmed histologically.
Prognostic impact of subgroup category on recurrence and survival
Univariable and multivariable analyses were carried out to determine whether the extent of invasion was a predictor of outcome. Table 3 lists variables affecting OS, DSS, and RFSP for 252 patients.
Univariable and Multivariable Cox Regression Analysis of Survival
CI, 95% confidence interval; HR, hazard ratio; NA, not applicable.
Univariable analysis showed that increasing age (hazard ratio [HR], 1.06; 95% confidence interval [CI]: 1.05–1.08; p < 0.001), T3/T4 stage (HR, 3.71; CI: 2.20–6.26; p < 0.001), N1a/N1b (HR, 1.92; CI: 1.25–2.95; p = 0.003), distant metastases (HR, 4.29; CI: 2.74–6.72; p < 0.001), and positive margin (HR, 3.56; CI: 2.27–5.58; p < 0.001) were associated with poorer OS. Patients with infiltrative disease also had worse OS than patients with encapsulated noninvasive and minimally invasive disease (HR, 4.98; CI: 1.80–13.8; p = 0.002). Multivariable analysis showed that increasing age (HR, 1.06; CI: 1.04–1.08; p < 0.001), T3/T4 stage (HR, 2.16; CI: 1.10–4.21; p = 0.024), and distant metastases (HR, 2.40; CI: 1.43–4.03; p < 0.001) were significantly independently associated with death.
Univariable analysis revealed that increasing age (HR, 1.05; CI: 1.03–1.07; p < 0.001), T3/T4 stage (HR, 5.17; CI: 2.19–12.2; p < 0.001), N1a/N1b (HR, 2.27; CI: 1.29–4.01; p = 0.005), distant metastases (HR, 4.98; CI: 2.80–8.87; p < 0.001), and positive margin (HR, 3.16; CI: 1.72–5.80; p < 0.001) were associated with poorer DSS. Patients with the infiltrative disease also had poorer DSS than patients with noninfiltrative disease (HR 3.55; CI: 1.64–7.65; p = 0.001). Multivariable analysis revealed that increasing age (HR, 1.03; CI: 1.01–1.06; p = 0.009), T3/T4 stage (HR, 2.90; CI: 1.06–7.93; p = 0.037), and distant metastases (HR, 3.37; CI: 1.75–6.50; p < 0.001) were independently associated with disease-specific death.
Univariable analysis showed that increasing age (HR, 1.03; CI: 1.02–1.05; p < 0.001), T3/T4 stage (HR, 3.69; CI: 2.19–6.22; p < 0.001), N1a/N1b (HR, 3.13; CI: 2.03–4.84; p < 0.001), distant metastases (HR, 2.38; CI: 1.47–3.85; p < 0.001), and positive margin (HR, 3.78; CI: 2.39–5.99; p < 0.001) were associated with poorer RFSP. Patients with infiltrative or encapsulated angioinvasive disease had worse RFSP than patients with encapsulated noninvasive or minimally invasive disease (infiltrative: HR, 26.9; CI: 3.72–194; p = 0.001; encapsulated angioinvasive: HR, 9.40; CI: 1.25–70.4; p = 0.029). Multivariable analysis revealed that increasing age (HR, 1.02; CI: 1.01–1.04; p = 0.003), T3/T4 stage (HR, 1.99; CI: 1.08–3.68; p = 0.028), and N1a/N1b stage (HR, 1.95; CI: 1.12–3.4; p = 0.018) were independently associated with disease recurrence.
Mutation landscape of HGFCTC subtypes
NGS data was available for 117/252 (46.4%) patients. Of these, tumors were classified as infiltrative in 58.1% (68/117), encapsulated angioinvasive with extensive VI in 27.4% (32/117), encapsulated noninvasive in 9.4% (11/117), encapsulated angioinvasive with focal VI in 3.4% (4/117), and encapsulated with capsular invasion only (minimally invasive) in 1.7% (2/117). Supplementary Figure S1 shows the mutation profiles of all 117 patients. Supplementary Figure S2 shows the key pathways altered. Common genetic mutations were TERT (42%), BRAFV600E (29%), NRAS (27%), EIF1AX (11%), and TP53 (9%). Pathways altered included RTK/RAS/RAF/MAPK (69%), PI3K/AKT/MTOR (14%), histone methyltransferases (9%), and SWI/SNF chromatin remodeling complex (8%).
Figure 4 shows the mutation profile of each subgroup. The infiltrative subgroup is mainly BRAF-driven, with the remaining driver mutations being NRAS, EIF1AX, TP53, ATM, HRAS, NF1, RET fusions, and ALK fusions. The encapsulated angioinvasive subgroups (extensive and focal VI) and encapsulated minimally invasive subgroup were NRAS-driven, with the other driver mutations being EIF1AX, TP53, HRAS, DICER 1, PTEN, and PAX8 fusions. The encapsulated noninvasive subgroup had a much different mutation profile, with the main driver mutation being DICER1; other driver mutations were EIF1AX, HRAS, NRAS, TP53, and PTEN.
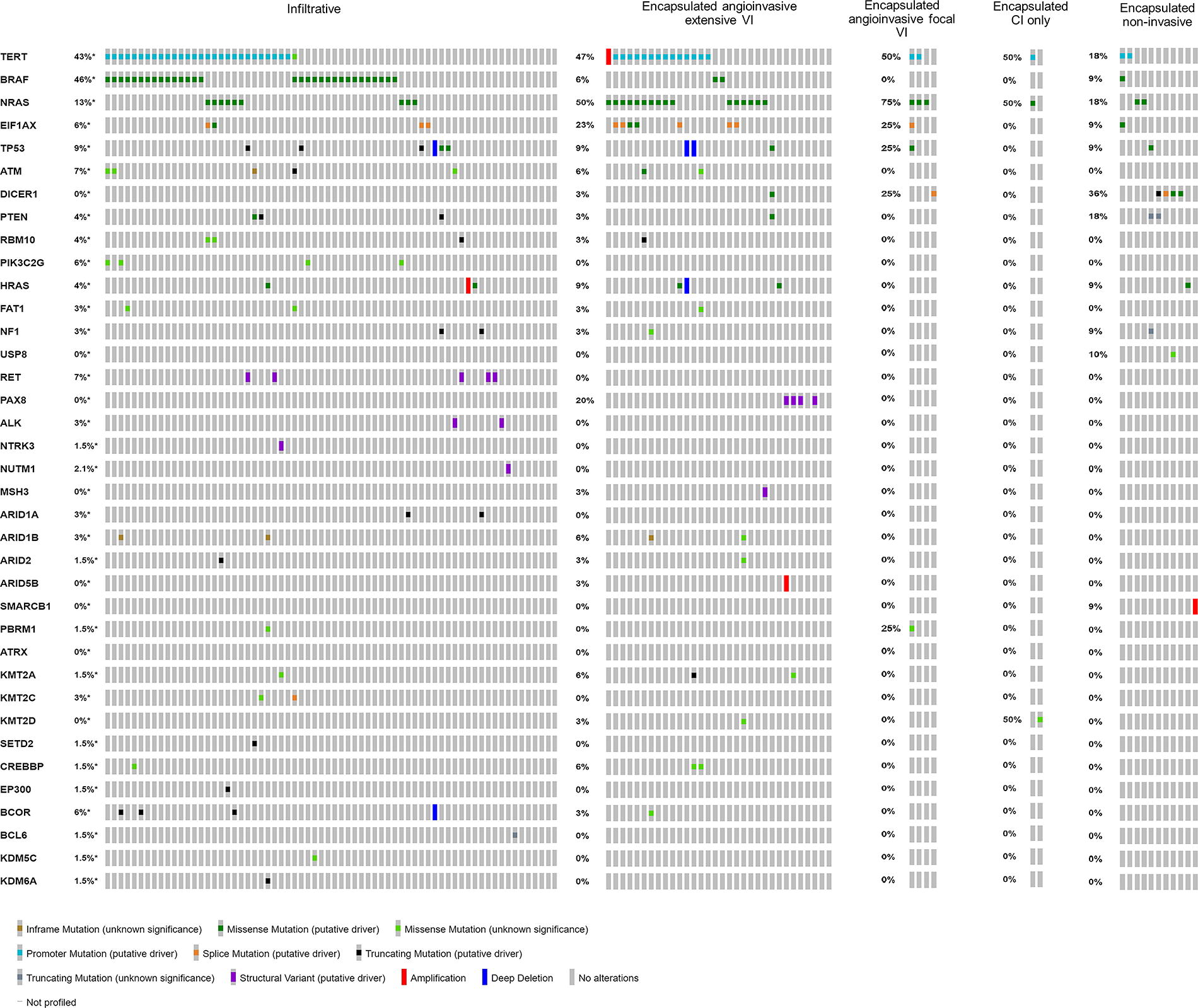
Oncoprint showing mutational landscape of different HGFCTC subgroups.
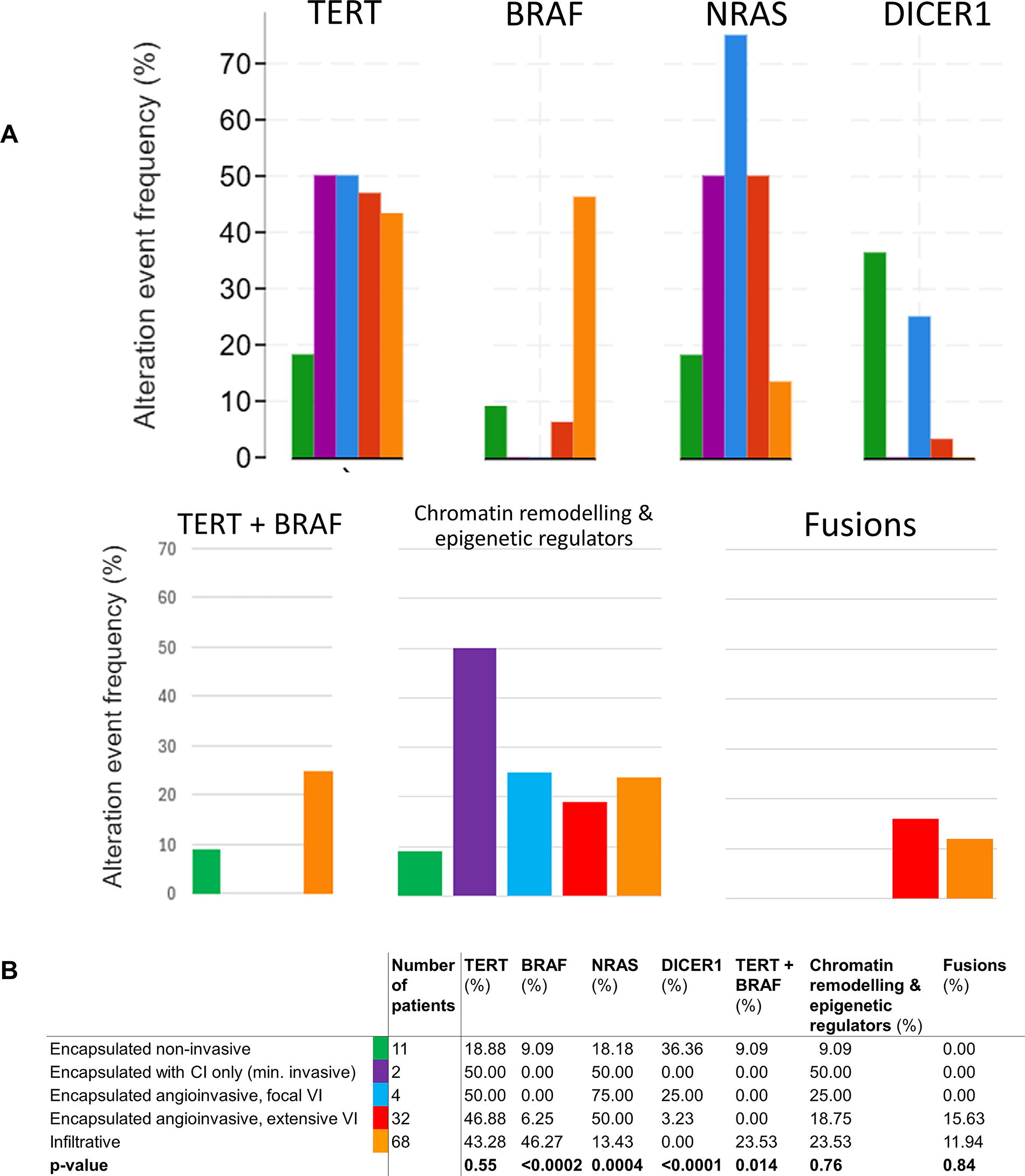
Figure 5A and B shows a comparison of the frequency of key mutations between subgroups. TERT mutations occurred in 19% of encapsulated noninvasive tumors, compared to 43–50% of other categories (p = 0.55). BRAFV600E mutations were significantly more common in infiltrative tumors (46%) than in encapsulated noninvasive (9%), encapsulated angioinvasive with extensive VI (6%), minimally invasive (0%), and encapsulated angioinvasive with focal VI (0%) tumors (p < 0.0002). Synchronous TERT + BRAFV600E mutations occurred significantly more in infiltrative tumors (24%; 16/68) than in encapsulated noninvasive (9%; 1/11), encapsulated angioinvasive with extensive VI (0%), encapsulated angioinvasive with focal VI (0%), and minimally invasive (0%) tumors (p = 0.014). Two of 11 (18%) patients with encapsulated noninvasive tumors had NRAS mutations and were the only 2 in the subgroup who experienced distal recurrence. NRAS mutations occurred in 13% of infiltrative tumors and at least 50% of each of the other three subgroups (p = 0.0004). DICER1 mutations occurred in 36% (4/11) of encapsulated noninvasive, 25% (1/4) of encapsulated angioinvasive with focal VI, 3% (1/32) of encapsulated angioinvasive with extensive VI, and 0% (0/68) of minimally invasive and infiltrative (p < 0.0001) tumors. Compared to the rest of the HGFCTC cohort, patients with DICER1 mutations were significantly younger (median 38 years, range 22–50) than patients without DICER1 mutations (median 59 years, range 23–87; p < 0.05). Patients with DICER1 mutations had excellent oncological outcomes, with 100% OS, 100% DSS, and 83.3% RFSP. Fusion genes were identified in encapsulated angioinvasive tumors with extensive VI (15.63%) and infiltrative tumors (11.94%) but did not occur in encapsulated noninvasive, encapsulated angioinvasive with focal VI, or minimally invasive tumors (p = 0.84). RET fusions were the most common fusions, occurring in six patients, followed by PAX8-PPARgamma fusions (4 patients), ALK fusions (3 patients), NTRK, NUTM1, and MSH fusions (1 patient each, respectively). There was no significant difference in the frequency of TP53 gene mutations (8.96% infiltrative; 9.38% encapsulated angioinvasive with extensive VI; 25% encapsulated angioinvasive with focal VI; 0% minimally invasive; 9% encapsulated noninvasive; p = 0.852) and EIF1AX mutations (6% infiltrative; 23% encapsulated angioinvasive with extensive VI; 25% encapsulated angioinvasive with focal VI; 0% minimally invasive; and 9% encapsulated noninvasive; p = 0.142).
Discussion
The 2022 WHO classification has introduced HGFCTC as a new entity, encompassing HGDTC and PDTC (Turin criteria), to reflect an intermediate prognosis between WDTC and ATC. 1 In addition to these tumor types, previous work from our institution 4,7 has also identified another entity, called “encapsulated noninvasive neoplasms of follicular cells with high-grade features,” as a rare but unique cohort with an excellent prognosis. To help inform prognostication and treatment—particularly of non-infiltrative tumors—this study sought to establish how the extent of invasion in HGFCTC impacted oncologic outcomes. Patients were classified into 5 HGFCTC subgroups based on encapsulation, capsular invasion, and vascular invasion. We found that encapsulated noninvasive and minimally invasive tumors (i.e., with capsular invasion only) had significantly lower T-stage, N-stage, and risk of distant metastases at presentation than encapsulated angioinvasive and infiltrative tumors. We show that there is a progressive decrease in OS, DSS, and RFSP from encapsulated noninvasive to angioinvasive to infiltrative tumors. These findings, supported by univariable analysis, indicate that infiltrative and encapsulated angioinvasive disease are negative prognostic indicators for recurrence and disease-specific death.
The differences in oncological outcomes were also reflected in the mutational landscape of these five subgroups, with each histological subgroup having specific mutations. Compared to WDTC, HGFCTC and ATC are characterized by an incremental increase in mutations of TERT, TP53, the PIK3CA-AKT-mTOR pathway, mismatch repair genes, and chromatin modifier genes such as the SWI/SNF nucleosome, remodeling complex, and histone methyltransferase mutations. 10 –12 TERT promotor mutations were common, occurring in ∼50% of tumors in each subgroup, with the exception of encapsulated noninvasive tumors. Tumors classified as infiltrative disease were more likely to harbor BRAFV600E mutations (BRAF-like), whereas NRAS mutations were significantly more likely in encapsulated angioinvasive tumors (RAS-like). Infiltrative HGFCTCs are enriched with high-grade tall-cell PTC (TCPTC) tumors (infiltrative 28% high-grade TCPTC vs. noninfiltrative 2% high-grade TCPTC), which accounts for the high incidence of BRAFV600E mutations. Coexistent BRAFV600E and TERT mutations have a synergistic adverse impact on outcome in PTC 13 –16 ; we found BRAFV600E and TERT mutations to coexist more commonly in infiltrative tumors than in other subgroups. Fusions were only observed in infiltrative and encapsulated angioinvasive tumors with extensive VI.
The encapsulated noninvasive tumors subgroup had a more unique mutation profile, with a high incidence of DICER1 mutations. TERT and BRAFV600E mutations were infrequent. DICER1 mutations result in impaired miRNA processing, increased MAPK signaling, and loss of differentiation in thyroid malignancy. 17 –19 DICER1 mutations have recently been described in adult HGFCTC. 20 In childhood and adolescent PDTC, DICER1 is a distinct driver with uncertain prognostic association. 21,22 In our study, DICER1 occurred significantly more in encapsulated noninvasive tumors (44%) than in other subgroups. We found that DICER1 mutations also correlated with excellent survival and recurrence outcomes in adult HGFCTC, with a significantly lower median age of 38 years.
Mutations in genes encoding components of the SWI/SNF chromatin remodeling complex (ARID1A, ARID1B, ARID2, ARID5B, SMARCB1, PBRM1, and ATRX) are a feature of advanced thyroid cancer, found most frequently in ATC, followed by PDTC. 11 This group of mutations was altered in 8% of our HGFCTC cohort, with no difference between subgroups, and ARID1B was the most common SWI/SNF alteration.
Most patients with infiltrative or angioinvasive tumors were treated with total thyroidectomy and adjuvant RAI. Although we cannot quantify the therapeutic benefits of RAI in patients treated due to distant metastasis in our cohort, over 81% demonstrated RAI uptake in at least one metastatic foci. Further studies are needed to determine if the uptake of RAI had a significant therapeutic effect on those lesions that concentrated RAI and, more importantly, if the destruction of RAI-avid lesions would have a significant impact on DSS given the heterogeneity of metastatic lesions with regard to RAI avidity and FDG PET avidity within an individual patient. While an increased likelihood of RAI avidity was expected in the predominantly RAS-driven encapsulated angioinvasive and minimally invasive tumors, it is an interesting finding in the predominantly BRAF-driven infiltrative tumors. Of patients with encapsulated noninvasive disease and those with capsular invasion only, a significant number were managed mainly with thyroid lobectomy alone and did not receive RAI treatment. In general, these patients all did well. However, although encapsulated noninvasive tumors appear to be very indolent, distant metastasis can occur, as evidenced by the development of bone metastasis in two of these patients, both of whom had NRAS mutations. In patients who harbor an NRAS mutation either alone or with TERT mutation, total thyroidectomy and adjuvant RAI may be of benefit.
Limitations of this study include the inherent limitations of retrospective data analysis, such as slide unavailability for 16 patients. The number of tumors in the minimally invasive subgroup is small, due to their rarity. Although the noninfiltrative subgroups tend to have superior outcomes, the median follow-up was only 62 months, and therefore late recurrences might not have been captured in these patients. Further confirmatory studies are required with longer follow-up, along with data on the effect of RAI on outcomes for each subgroup.
Conclusions
HGFCTC comprises different subgroups with different clinical behaviors determined by the occurrence and extent of vascular invasion and the presence of infiltration. Encapsulated noninvasive and minimally invasive (i.e., capsular invasion only) subgroups have much better recurrence and survival outcomes despite undergoing less aggressive treatment. The difference in OS, DSS, and RFSP between subgroups is reflected by their mutation profile. Mutations in the TERT promoter gene are common in all subgroups. Infiltrative tumors are largely “BRAF-like,” whereas encapsulated angioinvasive tumors are “RAS-like.” Encapsulated noninvasive tumors have a particularly unique molecular profile consisting of DICER1 mutations and no BRAFV600E mutations.
Footnotes
Acknowledgments
The authors thank Dagmar Schnau and Abby Rauso for editorial assistance with the article.
Authors’ Contributions
D.W.S.: Conception and design, collection and assembly of data, data analysis and interpretation, writing, editing, and review. B.X.: Collection and interpretation of data, editing, review. H.L.: Data analysis and interpretation, editing, and review. A.E.: Collection of data, data analysis and interpretation, editing, and review. A.R.S.: Data interpretation, editing, and review. J.P.S.: Data interpretation, editing, and review. R.M.T.: Data analysis and interpretation, editing, and review. J.A.F.: Gata analysis and interpretation, editing, and review. R.J.W.: Data analysis and interpretation, editing, and review. S.G.P.: Data analysis and interpretation, supervision, editing, and review. R.G.: Collection of data, data analysis and interpretation, supervision, editing, and review. I.G.: Conception and design, collection and assembly of data, data analysis and interpretation, supervision, writing, editing, and review. All authors approved of the final version of the article and agreed to be accountable for all aspects of the work.
Authors Disclosure Statement
The authors have no conflicts of interest to declare.
Funding Information
This research was funded in part through the NIH/NCI Cancer Center Support Grant P30 CA008748, which supports the research infrastructure at Memorial Sloan Kettering Cancer Center.
Supplementary Material
Supplementary Figure S1
Supplementary Figure S2
Supplementary Table S1