
Abstract
Background:
The longest reported follow-up for thermal ablation of papillary thyroid microcarcinoma (PTMC) is 5 years. We evaluated the long-term efficacy and safety of radiofrequency ablation (RFA) in patients with low-risk PTMC with clinical follow-up of more than 10 years.
Methods:
In this retrospective cohort study, we included patients with low-risk PTMC who had more than 10 years of follow-up after ultrasound (US)-guided RFA (performed between May 2008 and December 2013). Sixty-five consecutive patients with 71 low-risk PTMCs who were unsuitable for surgery or declined surgery were included. Before RFA, all patients underwent US and thyroid computerized tomography. Repeat RFA for staged ablation was performed when the first RFA did not secure sufficient safety margins because of the tumor closely abutting the recurrent laryngeal nerve. Follow-up US imaging was performed at 1 week, 3 months, 6 months, every 6 months until 2 years, and then annually afterward. Primary outcomes were the respective cumulative rates of disease progression (defined by local tumor progression, lymph node, or distant metastasis), newly developed thyroid cancer, and conversion surgery. Secondary outcomes were serial volume reduction rate (VRR), complete disappearance rate of ablated PTMC, and adverse events associated with procedures.
Results:
Of 65 patients included in the study, 60 had unifocal and 5 had multifocal PTMCs. The mean number of RFA sessions per tumor was 1.2, and the median follow-up duration was 151 months (interquartile ranges, 131–157). Twenty percent (13/65) of patients required repeat RFA. There were no cases of disease progression. Five patients (5/65, 7.7%) developed a new papillary thyroid cancer (four treated with RFA and one with lobectomy). At 24 months, the mean VRR was 100%, and this was maintained throughout the final follow-up. The complete tumor disappearance rates after one or more RFA treatments were 40.8% (29/71), 74.6% (53/71), and 100% (71/71) at 6, 12, and 24 months, respectively. One major (subclinical hypothyroidism) and three minor adverse events occurred.
Conclusions:
In our experience, RFA of low-risk PTMC is effective and safe. During more than 10 years of follow-up, we observed no incident local tumor progression nor metastases, but 7.7% of patients developed a new papillary thyroid cancer.
Introduction
Papillary thyroid cancer is a typically indolent malignancy with a good prognosis and low mortality rate, and surgery has long been the main treatment. 1,2 In recent decades, the incidence of papillary thyroid cancer has been exponentially increasing worldwide with improvements in the resolution of ultrasound (US) and its utilization. 3 –5 This rapid increase is thought to be related to the increased ability to detect and diagnose small indolent papillary thyroid cancer. 3 –5 Therefore, the management of low-risk papillary thyroid microcarcinoma (PTMC), which is defined as PTMC without evidence of metastasis, local invasion, or convincing cytological evidence of aggressive disease, has recently become an important issue.
The 2015 American Thyroid Association guidelines suggest active surveillance (AS) as a management option for low-risk PTMC. 1 Although AS has shown promising results, a substantial proportion of patients had reported undergoing conversion surgery (3.4%–32%). 6 –9 Furthermore, patient anxiety or patient preference was one of the main reasons (32%–69%) for patients having conversion surgeries, not disease progression. 10,11
Recently, thermal ablation techniques, including radiofrequency ablation (RFA), laser ablation, and microwave ablation, have been reported to have favorable clinical outcomes in the treatment of low-risk PTMC, with low rates of adverse events. In a meta-analysis of 5-year follow-up results of thermal ablation for low-risk PTMC, there was no local tumor recurrence, lymph node (LN) metastasis, distant metastasis, or conversion surgery in 207 patients with 219 PTMCs, 12 and the pooled major complication rate was as low as 1.2%. 12 When comparing outcomes, thermal ablation appears to demonstrate comparable or slightly superior results than AS, as AS patients experienced a mean tumor enlargement of 6.7% and a LN metastasis rate of 1.6% at the 5-year follow-up. 11 Also, Korean Society of Thyroid Radiology and European Thyroid Association guidelines indicate that thermal ablation procedures, such as RFA, may be considered as an alternative treatment option for patients with primary thyroid cancer who are either not surgical candidates or refuse surgery. 13,14
However, the currently reported studies are limited by small patient numbers and relatively short follow-up periods. The longest follow-up term reported for studies of thermal ablation of PTMC is 5 years. 15,16 Additional long-term follow-up studies of thermal ablation outcomes are necessary to build a comprehensive dataset that would enable meaningful and evidence-based comparisons among various management strategies for low-risk PTMC.
The purpose of our study was to evaluate the long-term efficacy and safety of RFA for low-risk PTMC in patients with follow-up duration of more than 10 years.
Materials and Methods
This retrospective study was approved by the Ethics Committee of the Institutional Review Board of Haeundae Sharing and Happiness Hospital (21203202–202312-HR-01). Written informed consent was obtained from all patients before RFA.
Study population
Our team previously published a cohort study of 84 PTMCs in 74 consecutive patients who had follow-up data covering more than 5 years. 15 From the cohort still undergoing postprocedural surveillance, those patients with follow-up data of more than 10 years were identified. The inclusion criteria were as follow 15 : (1) confirmation of PTMC, defined as papillary thyroid carcinoma measuring 1 cm or less in greatest diameter, and the absence of aggressive pathology on pre-RFA biopsy 17,18 ; (2) no evidence of gross extrathyroidal extension on US and computed tomography (CT) 19,20 ; and (3) contraindications for surgery (including comorbidities such as cardiovascular disease, history of stroke, central nervous system vascular malformation, other malignancy, and immunocompromised state) or refusal to undergo surgery. 21 Figure 1 shows the patient flow chart. Of 77 original eligible patients with 87 PTMCs, 12 were excluded because of a follow-up time of less than 120 months. Of these patients, five died of causes other than thyroid cancer (two colon cancers, one breast cancer, one unknown cancer, and one cardiovascular disease), and seven were lost to follow-up (three because of poor ambulation due to stroke and four because of unknown cause). Finally, 65 patients with 71 low-risk PTMCs treated between May 2008 and December 2013 were included in the study population (Fig. 1). All 65 patients included were patients who had been included in the previous 5-year follow-up study. 15

Participant flowchart.
Pre-RFA assessment
All patients underwent a US examination before RFA using either iU22US (Philips Healthcare, Bothell, WA, USA) or EUB-7500 (Hitachi Medical Systems, Tokyo, Japan) system equipped with a linear high-frequency probe (5–14 MHz). Three orthogonal diameters (the largest diameter and two perpendicular diameters) were measured, and the volume of each tumor was calculated using the equation: V = πabc/6 (V is the volume, a is the largest diameter, and b and c are the two perpendicular diameters). 22 After evaluation of the primary PTMC, a screening neck US examination was performed to detect the presence of LN metastasis. For cytopathological confirmation, a US-guided fine-needle aspiration or core-needle biopsy was performed. 17 Thyroid CT was performed in all patients to exclude LN metastasis. 23 Routine laboratory examinations, including thyroid function tests (TSH, T3, and fT4), serum thyroglobulin, thyroglobulin antibody, platelet count, and blood coagulation tests, were performed. All of the patients’ radiological evaluations and procedures, such as US examination, US-guided biopsy, and CT images, and the results of their laboratory tests, were reviewed by one radiologist (S.M.B., with 24 years of experience in thyroid imaging and thyroid procedures).
RFA procedure
All RFA procedures were performed by one expert radiologist (S.M.B.), in an outpatient setting. An SSP-2000 (Taewoong Medical, Gimpo, Korea) or VIVA RF System (STARmed, Goyang, Korea) radiofrequency generator and an 18-gauge thyroid-dedicated internally cooled electrode were used (Well-point RF electrode, STARmed; VIVA RF System). A 0.5-cm active tip was used in all cases except for one, in which a 1-cm active tip was used. 24 Detailed information on the equipment is provided in prior reports. 15 Each patient was placed in a supine position with the neck extended. To prevent bleeding, vessels along with the approach route were evaluated using Doppler US. Relationships between the tumors and critical structures such as nerves, esophagus, and trachea were evaluated to prevent injury. After sterilization, 1% lidocaine was injected into the skin puncture site and the strap muscles/anterior thyroidal capsule. Then, hydrodissection was used to prevent thermal injury by creating a safety margin from critical structures, for which a 23-gauge spinal needle was used to inject a cold dextrose solution between the tumor and critical structures. 8
The electrode was inserted into the tumor using the transisthmic approach, and ablation was performed using the fixed electrode or moving-shot or technique, with 15–30W of radiofrequency power; for tumors less than 3 mm in size, the fixed technique alone was sufficient for ablation. The electrode was accurately targeted at the center of the nodule, and ablation was performed with the electrode fixed in position. For tumors larger than 3 mm, we divided the tumor into three equal parts (posterior, middle, and anterior sections) and performed ablation in each section sequentially, starting from the posterior section and moving to the middle and anterior sections. 22,25 –28 The electrode tip was slowly moved before the impedance spike occurred, that is, before the “roll off” phenomenon. To prevent marginal recurrence, at least 2 mm of adjacent normal thyroid tissue was also ablated. When the tumor was adjacent to the thyroid capsule, ablation was performed including the capsule. The presence of any complications occurring during and immediately after ablation was carefully evaluated, and all patients were observed for several hours in the hospital after ablation.
Definition of outcomes
The primary outcomes were cumulative disease progression, newly developed thyroid cancer, and conversion surgery rate. The secondary outcomes were serial volume reduction rates (VRRs), complete disappearance rates of ablated PTMC, and complications associated with procedures.
Post-RFA evaluation
Patients underwent US monitoring and clinical evaluation according to the following schedule: 1 week, 3 months, 6 months, every 6 months afterward until 2 years, and followed by annual evaluations thereafter. Each follow-up US examination included comprehensive tumor measurements, documenting the volumetric assessment and its orthogonal three-dimensional maximal diameters. Thyroid function tests (TSH, T3, and fT4) were performed immediately after the ablation, and then 6 months afterward. Postprocedural management did not include TSH suppressive therapy in any of the study patients.
We reported the respective rates of cumulative disease progression and conversion surgery (any cause of thyroid surgery during the follow-up period). Cumulative disease progression included the total number of patients who experienced local tumor progression (recurrence and regrowth of the ablated tumor), LN metastasis, or distant metastasis. Thyroid CT was performed in all patients at 2 and 4 years after RFA to evaluate for LN metastasis. Newly developed thyroid cancers (detection of new cancer other than the ablated tumor, with cytological confirmation) and conversion surgery (because of disease progression, newly developed cancer, or anxiety during follow-up) were also evaluated. VRR was calculated as: VRR = ([initial volume − final volume] × 100)/initial volume. 22 Additional RFA for staged ablation was performed when the first RFA did not secure sufficient safety margins because of the tumor closely abutting the recurrent laryngeal nerve. 29
Technical success was defined as complete ablation of the tumor by the planned treatment protocol, which included staged ablation for tumors closely abutting the recurrent laryngeal nerve. 30 Primary efficacy rate was defined as the percentage of tumors successfully treated following initial ablation, and secondary efficacy rate included tumors that have undergone successful retreatment. 30 Complications during the procedure or follow-up were assessed using the reporting standards of the Society of Interventional Radiology. 31 We evaluated early complications (occurring within 30 days after RFA) and delayed complications (occurring more than 30 days after RFA).
Results
Patient demographics and clinical characteristics
The characteristics of the patients and tumors are described in Table 1. The mean age was 45.8 ± 13.1 years (range 19–77), and 35.4% (23/65) were under 40 years of age. Of the 65 patients, 60 had unifocal PTMCs and 5 had multifocal PTMCs (four patients with two PTMCs and one patient with three PTMCs). The median follow-up duration after RFA was 151 months (interquartile range, 131–157). The mean largest tumor diameter was 4.1 ± 1.5 mm (range, 2.3–9.5 mm), and the mean volume was 27.6 ± 36.4 mm3 (range, 0.8–205.4 mm3). Among the 71 tumors, 55 had the largest diameter of less than 5 mm, while the other 16 tumors were between 5 and 10 mm. Among the 71 tumors, 15 had calcifications including microcalcification (n = 12), macrocalcification (n = 1), rim calcification (n = 1), and mixed (micro- and macrocalcifications, n = 1) calcifications. The RFA parameters are described in Table 1. The mean number of RFA sessions per tumor was 1.2 ± 0.4 (range, 1–2), with 58 tumors being treated in one RF session and 13 tumors being treated in two RF sessions because of insufficient safety margins at the first ablation. The mean number of RFA sessions per patient was 1.2 ± 0.4 (range, 1–2), with 13 out of 65 patients being treated in two sessions, and others being treated in one session.
Demographics, Characteristics, and Treatment Parameters of the Patients and Their PTMCs
Data are expressed as mean with standard deviation or median with interquartile ranges. Unless indicated otherwise, data are numbers with percentages in parentheses.
Four patients with two PTMCs and one patient with three PTMCs.
PTMC, papillary thyroid microcarcinoma; RFA, radiofrequency ablation.
Clinical and radiological outcomes
RFA was technically successful in all 65 patients with 71 PTMCs. The primary efficacy rate was 80% (52/65), and the secondary efficacy rate was 100% (65/65), as 20% (13/65 patients) required retreatment, and all retreatments were successful.
During a median follow-up period of 151 months, the cumulative disease progression rate was 0%. There was no local tumor progression, LN metastasis, distant metastasis, and no death related to thyroid cancer. However, five patients developed one newly developed papillary thyroid cancer in the remaining thyroid gland (5/65, 7.7%). The new cancers were separate from the initially ablated tumor (four ipsilateral and one contralateral lobe). Four of these newly developed thyroid cancers were also successfully ablated by RFA (Table 2), whereas one patient with newly developed thyroid cancer was managed by lobectomy. Therefore, this study recorded one conversion surgery because of a newly developed papillary thyroid cancer.
Cumulative Rates of Disease Progression, Newly Developed Thyroid Cancer, and Conversion Surgery After RFA for Papillary Thyroid Microcarcinoma *
This table summarizes the data from 65 patients with 71 papillary thyroid microcarcinomas.
Disease progression is defined as the number of patients with local tumor progression (recurrence and regrowth of the ablated tumor), LN metastasis or distant metastasis. Newly developed thyroid cancer (detection of new cancer other than the ablated tumor, with cytological confirmation) was not included in the cumulative disease progression.
RFA, radiofrequency ablation; LN, lymph node.
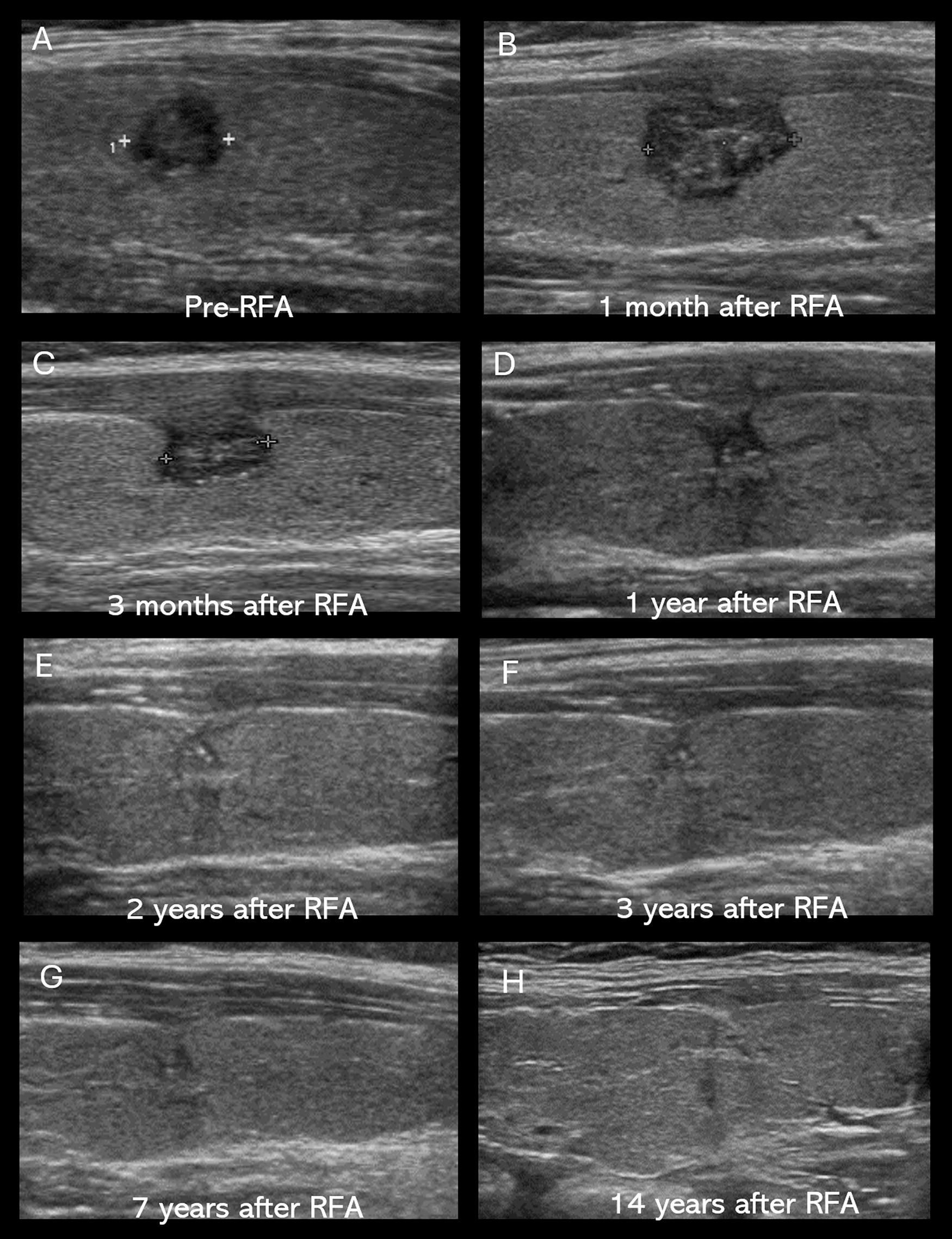
The volumes of ablation zone increased immediately after RFA and then decreased gradually. At 24 months, the mean VRR reached 100, and this complete reduction was maintained through the 120-month follow-up period. The complete disappearance rates after one or more RFA treatments were: 4.2% (3/71), 40.8% (29/71), 74.6% (53/71), 100% (71/71), 100% (71/71), 100% (71/71) and 100% (71/71) at 3, 6, 12, 24, 36, and 120 months, respectively (Table 3, Fig. 2). All ablated tumors had completely disappeared at the 24-month follow-up and afterward. In cases of tumors with calcifications, all calcifications also completely disappeared on follow-up evaluation. In one case of a 7.5-mm tumor with microcalcifications, microcalcifications gradually decreased in size, number on serial follow-up, and had completely disappeared at the 168-month follow-up (Fig. 3). Figures 4 and 5 show representative RFA cases with serial US changes.

Serial mean volume reduction on ultrasonography. The volume of ablation zone increased immediately after RFA and then gradually decreased. The mean volume reduction rate reached 100% at 24 months of follow-up. The interval from −100 to 0 was spaced. RFA, radiofrequency ablation.
The gradual decrease and disappearance of microcalcifications in PTMC after RFA.
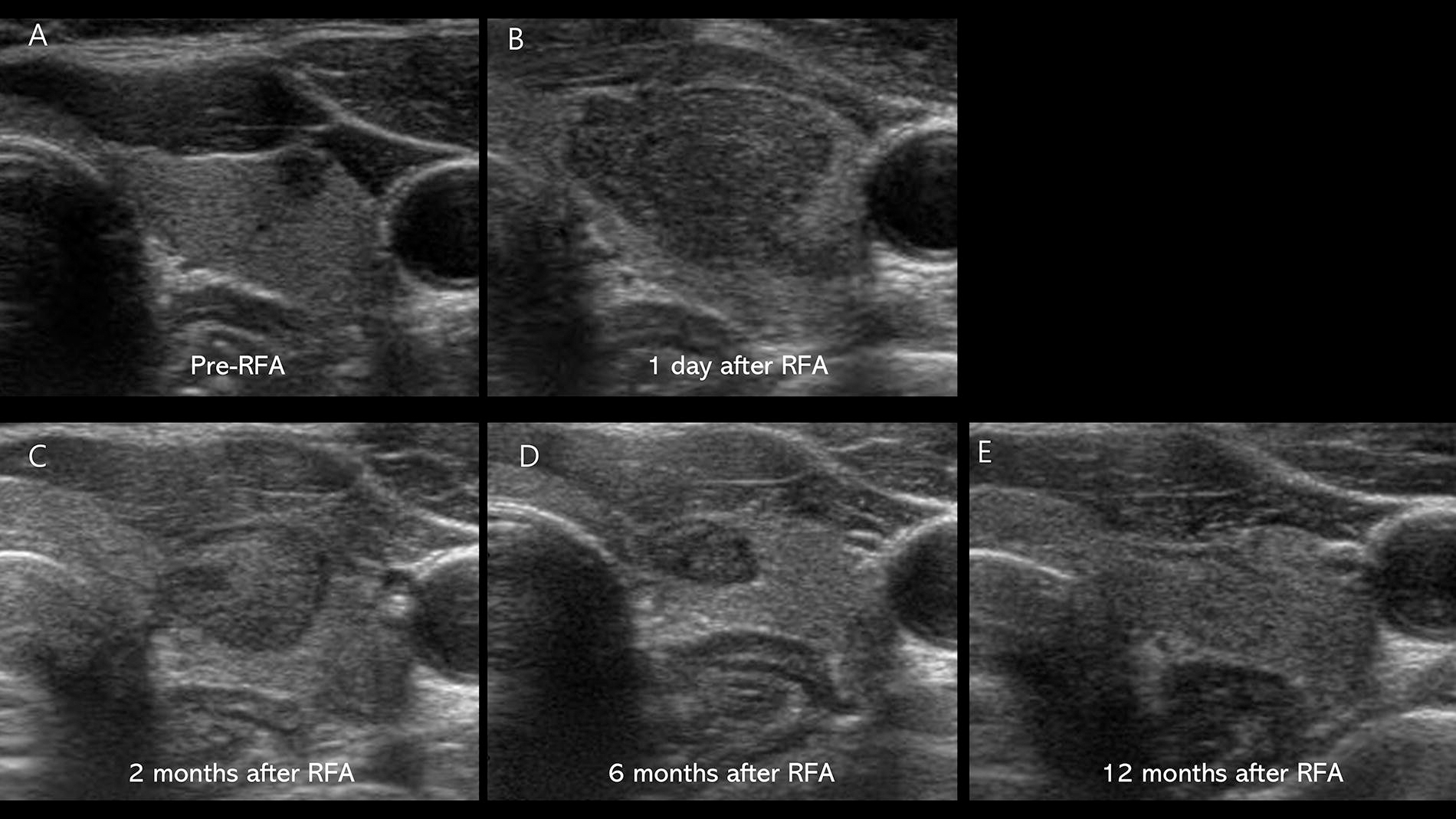
Examples of pre-RFA and post-RFA follow-up of PTMC.

Examples of pre-RFA and post-RFA follow-up of PTMC.
Clinical Outcomes of RFA in Patients with Low-Risk PTMC
RFA, radiofrequency ablation; PTMC, papillary thyroid microcarcinoma; VRR, volume reduction ratio.
The detailed characteristics of the newly developed thyroid cancers are summarized in Table 4. The newly developed thyroid cancers were papillary thyroid carcinomas. The mean largest tumor diameter of the newly developed thyroid cancers was 3.4 ± 0.4 mm (range, 2.6–3.8 mm), and the mean volume was 8.1 ± 4.5 mm3 (range, 1.5–15.5 mm3). The average interval time to development of new thyroid cancer after RFA was 75.2 ± 36.9 months. The development times of the newly developed thyroid cancers (n = 5) were 11, 68, 79, 96, and 122 months. During the follow-up period, there was no LN metastasis in the five patients with newly developed thyroid cancer managed by RFA or lobectomy.
Characteristics of Newly Developed Thyroid Cancers in Five Patients (Five Papillary Thyroid Cancers)
The development times of five newly developed thyroid cancers were 11, 68, 79, 96, and 122 months after RFA.
Ipsilateral and contralateral to initial PTMC.
PTMC, papillary thyroid microcarcinoma; RFA, radiofrequency ablation.
Safety
There was one major complication (1.5%, 1 of 65 patients: subclinical hypothyroidism) and three minor complications (4.6%, 3 of 65 patients: two hematomas with immediate recovery and one second-degree burn). At 6-month follow-up, Subclinical hypothyroidism was detected on thyroid function testing, in one patient and this patient was subsequently treated with thyroid hormone therapy. There were no delayed complications during the mean follow-up period of 145 months.
Discussion
In this study on the long-term outcomes of RFA for PTMC, we demonstrated that RFA successfully treated 71 PTMCs in 65 consecutive patients. Of these 65 patients, 35.4% (23/65) were under 40 years of age. All patients were followed up for more than 10 years, and all tumors had disappeared in US at the final follow-up period, which had a median duration of 151 months. During the follow-up period, there were no cases of disease progression cases as defined by local tumor progression, LN metastasis, or distant metastasis, and there were no procedure-related deaths. However, there were five newly developed papillary thyroid cancers in five patients (5/65, 7.7%). Conversion surgery was performed on one of the five patients with newly developed thyroid cancer, and the other four patients were treated by additional RFA. We observed one major and three minor complications. To our knowledge, this study reports the longest follow-up duration for RFA of PTMC. This study reveals that RFA can successfully treat PTMCs.
The efficacy of thermal ablation of PTMC was reported in several 5-year follow-up studies and a meta-analysis. 12,15,16,32 The meta-analysis demonstrated a 5-year cumulative disease progression rate of 0%. 12 To our knowledge, our study is the first to report on 10-year follow-up (the median follow-up was 151 months). Similar to 5-year outcomes reported in a meta-analysis, our 10-year follow-up study demonstrated a 0% cumulative incidence rate of disease progression.
AS may be considered as one of the treatment options for PTMC. 33 The clinical outcomes of AS for PTMC have been favorable; a meta-analysis of AS for PTMC showed a cumulative disease progression rate of 6.9% at 5-year follow-up (tumor size enlargement in 5.3% and LN metastasis in 1.6%). 11 Recently reported long-term results of AS for PTMC showed a disease progression rate of 5.7% at 10 years and 8.2% at 20 years. 34 However, AS is subject to several limitations. The first is the anxiety experienced by patients and their doctors regarding disease progression. As a result, many patients underwent conversion surgeries because of anxiety, rather than because of disease progression. 11 However, no conversion surgeries because of anxiety without incident cancer or cancer progression were observed in our study. Second, disease progression may be more common in young patients. In a study on AS for PTMC, a younger age (<40 years) was associated with a higher rate of disease progression. 35 In our study, although a relatively large proportion of the patients were young (35.4% were under 40 years old), RFA still achieved good clinical outcomes without local or LN metastasis. Lastly, we observed newly developed thyroid cancers in 7.7% of patients (5/65). In many AS studies, newly developed thyroid cancers were frequently not mentioned in the outcomes and may have been underestimated.
In our study, one patient developed subclinical hypothyroidism at 6 months after ablation. However, it is not clear whether the subclinical hypothyroidism was induced by RFA or coincidentally occurred due to the patient’s natural condition. In the ablation of PTMC, only a very small amount of thyroid tissue is ablated, so the risk of hypothyroidism is expected to be very low. Instead, underlying conditions such as increased levels of anti-TPO antibodies and/or antithyroglobulin antibodies may increase the risk of hypothyroidism after ablation. 36 Patients with elevated levels of these antibodies should be advised about the risk of hypothyroidism before they undergo RFA. 36
This study has several limitations. First, this is a retrospective study that is subject to potential selection bias. Although our study is a retrospective cohort study, we enrolled consecutive patients and tried to minimize follow-up loss. Second, the sample size of our study is small and underpowered for investigating such an indolent disease process of low-risk PTMC. Third, there was no biopsy confirmation of the absence of malignancy in the areas treated with RFA. However, all treated areas showed a progressively decreasing pattern and ultimately achieved a 100% complete disappearance rate on US imaging within 2 years. Fourth, although this study included small PTMCs of less than 5 mm, which were treated mostly in the early study period, the optimal lower limit of tumor size for RFA treatment remains subject to debate.
In our experience, RFA is an effective and safe option for the treatment of low-risk PTMC. We observed no incident local tumor progression, and LN or distant metastasis, but 7.7% of patients developed a new thyroid cancer over 10 years of follow-up. Confirmatory research in other centers is needed. However, we believe that clinical guidelines and consensus statements for the treatment of PTMCs should be expanded to include RFA.
Footnotes
Authors’ Contributions
S.Y.J.: Data curation (lead); formal analysis (lead); and writing—original draft (lead); S.M.B.: Data curation (lead); formal analysis (lead); and writing—review and editing (lead); S.S.: Data curation (equal); J.M.S.: Data curation (equal); H.K.: Data curation (equal); J.H.B.: Data curation (lead); formal analysis (lead); and writing—review and editing (lead).
Author Disclosure Statement
J.H.B. has served as a consultant for one radiofrequency company, STARmed since 2017.
Funding Information
The authors declare that no funds, grants, or other support were received for this article.