
Abstract
Background:
Overtreatment with thyroid hormone is common and is associated with multiple adverse health outcomes, especially in older adults. Higher overtreatment rates have been reported among women. Understanding this sex difference could lead to better clinical utilization of therapy in at-risk populations.
Methods:
We performed a retrospective cohort study to examine the relationship between iatrogenic thyrotoxicosis and patient sex, adjusting for demographics, comorbidities, body composition, and thyroid hormone dosing using electronic health records for adults age 50 and older in a large community health system in the United States.
Results:
A total of 20,724 patients met all inclusion criteria, of whom 77% were female and 23% non-White. Women were more likely to have a low thyrotropin (TSH) compared to men (36.7% vs. 23.9%; unadjusted hazard ratio [HR] = 1.67 [95% confidence interval {CI} 1.56–1.79]). Many covariates varied by sex, including rates of several comorbidities, and there was a small but statistically significant difference in the median daily levothyroxine dose per actual body mass: 1.1 μg/kg in male patients compared with 1.2 μg/kg in female patients (p < 0.001). Adjusting for covariates other than dose did not significantly change the sex-related risk of iatrogenic thyrotoxicosis. In fully adjusted Cox models including dose per actual body mass, the female versus male HR = 1.50 [CI 1.34–1.69] was also not different from models which did not account for dose (p = 0.422). However, the association between female sex and thyrotoxicosis risk was partially mediated when adjusting for dose per ideal body mass (HR = 1.30 [CI: 1.16–1.46]; p < 0.001) and was fully mediated by dose calculated using lean body mass (HR = 1.06 [CI: 0.95–1.19]; p < 0.001). That is, women had higher risk of iatrogenic thyrotoxicosis compared to men receiving similar actual body mass doses, whereas women and men receiving comparable lean body mass doses had comparable risk.
Conclusions:
Mediation analysis demonstrates that the increased risk of iatrogenic thyrotoxicosis in older women may be attributable to differences in body composition between men and women. The use of ideal or lean body weight-based dose calculators in place of actual body weight dosing could reduce this potential source of iatrogenic thyrotoxicosis risk in older women.
Introduction
Thyroid hormone supplementation is among the most commonly prescribed medications in the United States, with levothyroxine currently ranking fourth. 1 Unfortunately, only about two-thirds of those on therapy are typically treated with euthyroid targets 2 and in many thyrotoxicosis from overtreatment can persist for years. 3 This has the potential to result in harm, particularly for older adults, who are more vulnerable to the risks of iatrogenic thyrotoxicosis, which has been associated with an increased risk of fracture, 4,5 atrial fibrillation, 6 –8 cardiovascular mortality, 9 and dementia. 10 It is therefore critical to understand why some of these patients are overtreated, who is at the highest risk, and how overtreatment may be avoided.
Women have been reported to be at increased risk of iatrogenic thyrotoxicosis compared to men. 3 Some of this gap may be attributable to increased rates of prescribing among women. For example, in 2020, Jonklaas and DeSale found that female patients were prescribed thyroid hormone approximately four times more frequently than male patients (2.9% vs. 0.7%). 11 However, even restricting the analysis to those on thyroid hormone and euthyroid at baseline, female participants in the Baltimore Longitudinal Study of Aging had a significantly higher cumulative incidence of thyrotoxicosis than male participants (4.8 men vs. 25.2 women per 1000 person-years). 3 Moreover, prescribing rates are unlikely to be the sole cause of the sex differences in iatrogenic thyrotoxicosis.
Alternative hypotheses include sex differences in (1) the selection of the prescribed dose based on patient characteristics, prescriber biases, or expressed preferences; (2) the dosing titration intensity resulting from variation in engagement with health care; or (3) physiological variables that are not accounted for when dosing decisions are made. For example, if there are sex differences in the rates of comorbid conditions such as depression or atrial fibrillation, which in turn lead to higher or lower therapeutic targets, which could translate into a sex-specific risk for overtreatment. Alternatively, the reliance on actual body mass when calculating thyroid hormone dose might introduce a sex bias because of the higher percent body fat among women. 12
We used electronic health records (EHRs) from older primary care patients in the Johns Hopkins Health System who were prescribed thyroid hormones. We examine associations between sex and iatrogenic thyrotoxicosis, adjusting for demographics, comorbidities, medications, body composition estimates, and thyroid hormone dosing to understand which factors mediate the sex-specific risk of iatrogenic thyrotoxicosis.
Materials and Methods
Study setting and population
This is a retrospective cohort study conducted using EHRs for older primary care patients in the Johns Hopkins Health System, which has clinics throughout Maryland and Washington D.C. The Epic Systems EHR was adopted in mid-2013; however, we included data for patients with visits between January 1, 2014, and February 29, 2024. Patients were included if they (1) had two or more internal or family medicine visits, at least 30 days apart at which they were aged 50 or older, (2) had a prescription for levothyroxine on or after the first of these visits, and (3) had at least one height and one weight measurement on or before the date of their first documented levothyroxine prescription. In order to standardize weight-based dose calculations, patients were excluded if they had prescriptions for liothyronine or desiccated thyroid product on or before their first levothyroxine prescription. Patients were also censored after inclusion if they were switched to T3-containing regimens. Because patients with thyroid cancer may be deliberately treated to lower TSH targets, patients were excluded if they had a hospital billing code, encounter diagnosis code, or documented history of thyroid cancer (ICD-10 codes C73.X, D09.3, Z85.850). We also excluded patients with pituitary disease, pituitary surgery, or central hypothyroidism in whom TSH measures are not a reliable indicator of thyroid hormone replacement (ICD-10 codes C75.2, D35.[2,3], D44.3, D22.[0,8,9], E23.[0,6,7], E24.0, E27.[1,3,4], E89.3, or an ICD-10 code of E03.8 along with “central,” “secondary,” “deficiency,” or “pituitary” in the diagnosis name). This study was approved by the Johns Hopkins University IRB (Nos. IRB00228485, IRB00258816, and IRB00269466), and a waiver of consent was granted.
Variables
Patient characteristics including age, sex, race, and Hispanic ethnicity were determined from clinical intake forms. Race was categorized as White, Black, and other (Asian, American Indians, Pacific Islanders, Native Hawaiians, and multiracial). Patient weight and height were extracted from chart measurements as part of routine care with ideal and lean body weight calculated using common formulas (details in Supplementary Data). 13,14
Thyroid hormone prescriptions and dosing
We included all prescriptions for levothyroxine (RxCUI 10582) ordered by Johns Hopkins providers on or after a patient’s first included primary care visit. Due to the complexity of thyroid hormone prescriptions, the patient’s total daily dose was calculated using text processing of the medication instructions as described in the Supplementary Data. Body mass adjusted daily dose (μg/day/kg) was calculated for actual, ideal, and lean body mass using the most recent weight and height measurements at the time of each prescription.
TSH measurements
Our primary outcome was iatrogenic thyrotoxicosis, indicated by a low TSH measurement in the context of an active prescription for thyroid hormone therapy using the algorithm described previously. 10 Low TSH measurements were identified based on the assay-specific reference range or below 0.45 mU/L if no reference was available. Where the sample collection date was unavailable (1.6% of all TSH measurements), we used the result date (date entered into the EHR). We excluded TSH measurements ordered during hospital inpatient stay or emergency department visits, as acute medical stress can cause a low TSH. Since FT4 was not available frequently enough to determine subclinical and overt thyrotoxicosis, we categorized severity based on TSH alone as either moderate (≥0.1 mU/L < lower limit) or severe (<0.1 mU/L).
Analyses
We estimated the distributions of thyroid hormone dosages and TSH measurements using kernel density estimation and estimated the cumulative incidence of iatrogenic thyrotoxicosis relative to the first included levothyroxine prescription using Kaplan–Meier estimation. Details on these methods, as well as methods for estimating the conditional distribution of TSH at different thyroid hormone doses, are in Supplementary Data.
To estimate the association between patient sex and risk of iatrogenic thyrotoxicosis, we used a time-varying Cox model. The time of event was taken as the time of the first observed thyrotoxicosis following the first prescription for levothyroxine following the patient’s first primary care visit. Patients were right-censored after their last observed primary care visit or if they received a prescription for liothyronine (RxCUI 10814) or desiccated thyroid product (RxCUI 10572). To examine potential mediation by thyroid hormone dose, we estimated four time-varying Cox models. In the first (reference) model, thyroid hormone dose information was not included as a covariate. In the remaining three models, thyroid hormone dose per actual, ideal, and lean body mass, respectively, were included as time-varying covariates. We used a decile binning of dose (μg/day) per kg body mass. For each model, we tested the hypothesis that the estimated hazard ratio for female sex was the same as that of the reference model using patient-level nonparametric bootstrapping with 500 bootstrap samples. To account for potential confounding, all models also included static variables for patient race (categories described above), Hispanic ethnicity, age, height, and weight at first documented prescription. Furthermore, we included time-varying indicators for diagnoses of diabetes, fatigue and/or chronic pain, depression, atrial fibrillation, ischemic heart disease, and heart failure, as well as prior prescriptions for proton pump inhibitors, glucagon-like peptide-1 agonists, calcium, magnesium, iron, and estrogen (RxCUIs available in Supplementary Table S1). Finally, to account for potential differences in testing rates based on sex, we included the number of TSH measurements taken in the prior year as a time-varying variable. ICD-10 code lists for comorbidities were based on the Chronic Conditions Data Warehouse Chronic Conditions Algorithms (revised 07/2023). Age, weight, height, and dose were all transformed using centered natural cubic splines with five degrees of freedom.
We conducted sensitivity analyses restricting the cohort to patients with at least one TSH measurement above 10 mU/L (irrespective of whether the patient was prescribed thyroid hormone at the time), using severe thyrotoxicosis as the outcome, restricting to patients over 60 who were never prescribed estrogen (women in menopause), restricting to confident new thyroid hormone starts, adding a 6-month offset to time zero, and treating patients as right-censored after any prescription for potential TSH altering medications. Details for each of these analyses are in the Supplementary Data. All analyses were conducted in Python using the “lifelines” (v 0.27.0) package for modeling, “scikit-learn” (v 1.5.1) package for data preprocessing, and “patsy” (v 0.5.3) for calculating splines.
Results
Patient characteristics
Of the 203,305 patients aged 50 and over with a primary care visit during the study period, 20,724 patients met all inclusion criteria (Fig. 1). Of these, 15,894/20,724 (77%) were female, the average age was 65 (STD 11.2) at the first documented prescription, and 4878/20,724 (24%) were non-White, with the most common non-White racial identity being Black (2656/20,724; 13%). The average time from the first levothyroxine prescription to the last visit was 4.7 (STD 3.3) years, and patients had on average 1.6 (STD 3.3) TSH measurements per year. The average body mass at first thyroid hormone prescription was 79 kg (STD 20.9) for female patients and 93 kg (STD 21.5) for male patients (p < 0.001). The average estimated percent lean body mass was 58% (STD 6.1) among female patients and 71% (STD 6.8) among male patients (p < 0.001). Finally, 5174/20,724 (25%) of patients had a history of at least one TSH ≥10 mU/L, whereas 6995/20,724 (34%) experienced iatrogenic thyrotoxicosis (TSH below reference) and 2871/20,724 (14%) experienced severe iatrogenic thyrotoxicosis (TSH < 0.1). Additional cohort statistics and comparisons between male and female patients are in Table 1. Male and female patients had statistically significant differences in nearly every patient variable considered except the number of TSH measurements per year. Among the comorbidities, male patients had significantly higher rates of diabetes (M: 34% vs. F: 26%), atrial fibrillation (M: 21% vs. F: 11%), ischemic heart disease (M: 31% vs. F: 14%), and heart failure (M: 16% vs. F: 11%), whereas female patients had higher rates of fatigue or chronic pain (M: 49% vs. F: 58%), obesity (M: 31% vs. F: 36%), and depression (M: 22% vs. F: 34%).
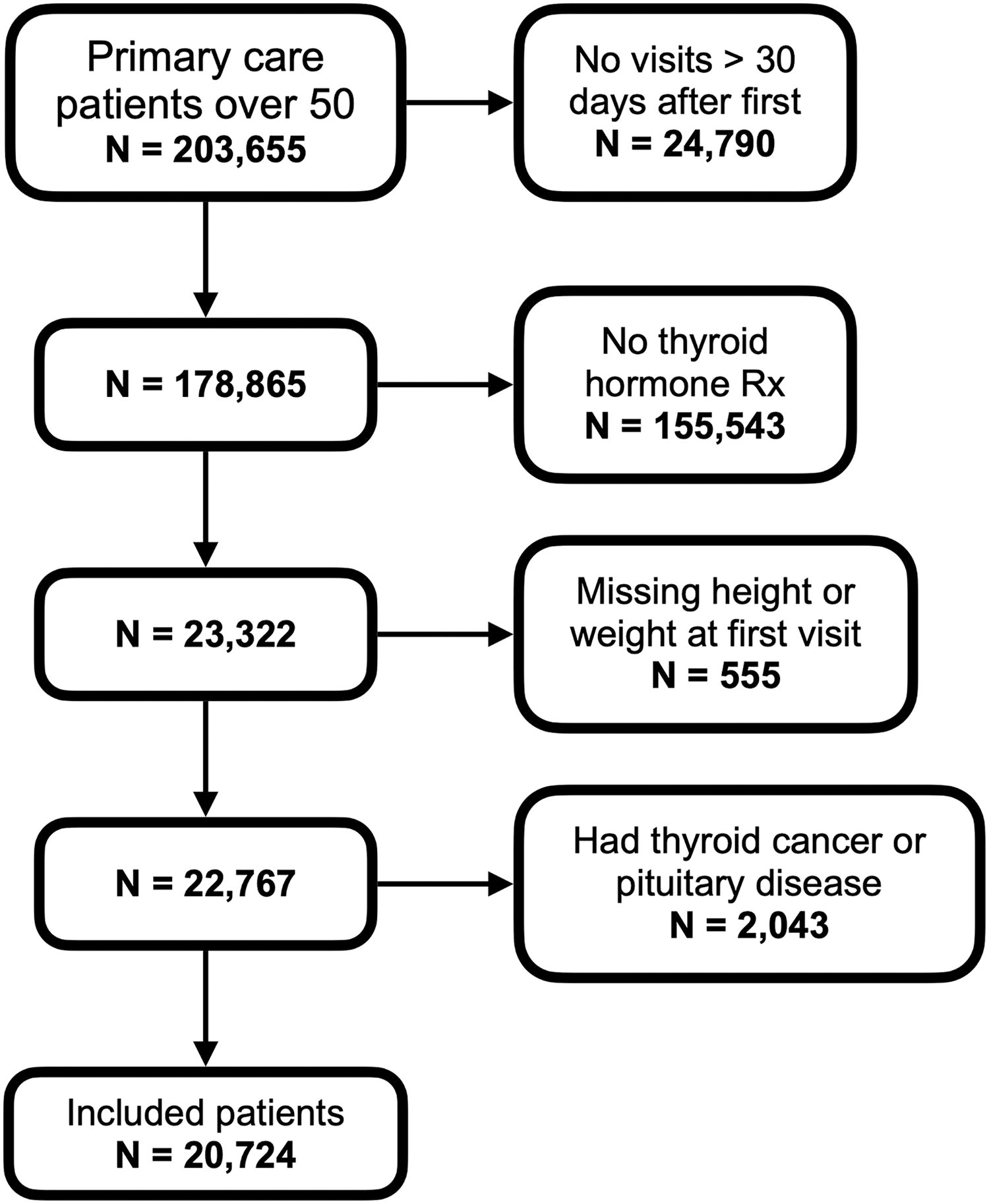
Participant flow diagram. This figure shows a flow diagram for the cohort in this study. The initial group of eligible patients (N = 203,305) includes all patients with a primary care visit between January 1, 2014, and February 29, 2024, at which they were age 50 or older.
Patient Characteristics
For all body composition measurements, the last measurement before the patient’s first levothyroxine prescription was used.
Counted as positive if true (e.g., diabetes was diagnosed) at any point during the study.
Glucagon-like peptide-1 receptor agonist.
Categorical variables are summarized as “total (percent)” and continuous variables are summarized as “mean (std).” p-values were estimated using two-sided Pearson’s chi-squared tests and Mann–Whitney U tests for categorical and continuous variables, respectively.
TSH, thyrotropin; PPI, proton pump inhibitor.
Risk of iatrogenic thyrotoxicosis by sex
The average TSH for female patients was lower, and the TSH distribution was left-shifted relative to the TSH distribution for male patients (p < 0.001; Fig. 2). Moreover, female patients generally have lower TSH measurements following the initiation of a thyroid hormone prescription than do men, and a higher proportion of men were observed to have a TSH >10 mU/L (3790/15,894 [23.8%] vs. 1384/4830 [28.7%]; p < 0.001). Iatrogenic thyrotoxicosis risk was significantly higher among female patients (unadjusted hazard ratio [HR] 1.67 [1.56–1.79], Table 2). Adjusting for demographics, comorbidities, healthcare utilization, and other medications did not impact the significance of this association (HR 1.55 [1.41–1.69]; Table 2 and Supplementary Table S2). The distributions of TSH measurements stratified by thyroid hormone dose per kg lean body mass are in Figure 3, with increased rates of low TSH measurements corresponding to higher doses.
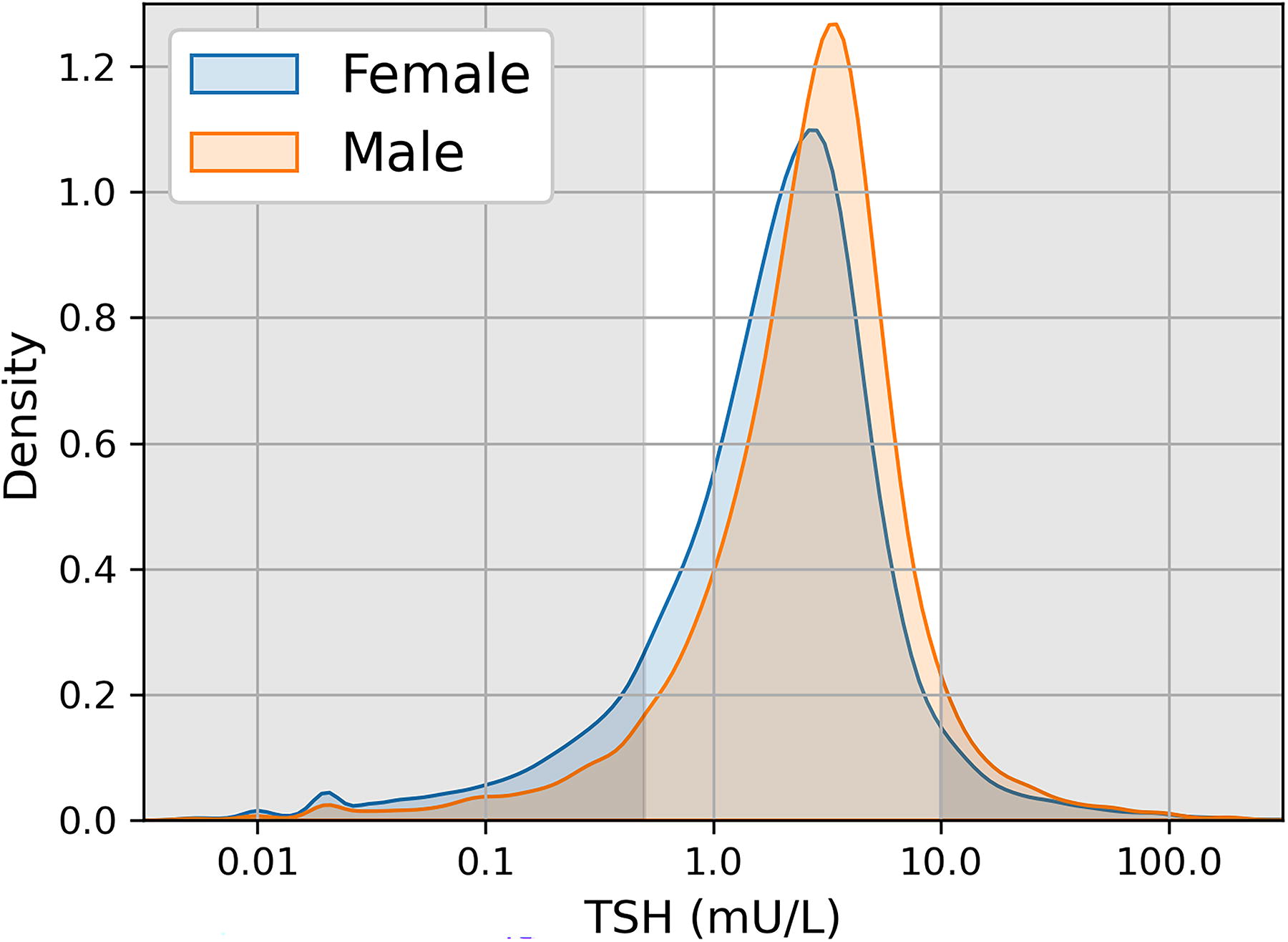
Distribution of TSH measurements by sex. This figure shows the distributions of TSH measurements (mU/L) for male and female patients on levothyroxine. Gray regions represent typical high and low reference ranges. TSH, thyrotropin.

Distribution of TSH measurements by thyroid hormone dose (per kilogram lean body mass). Distribution of TSH measurements by thyroid hormone dose (per kilogram lean body mass): This figure shows percentiles of the TSH (mU/L) distribution at thyroid hormone doses ranging from 0.3 to 4.0 µg/kg lean body mass. Gray regions represent typical high and low reference ranges. Additionally, the vertical lines mark the distribution at a daily dose of 1.6 µg/kg lean body mass (dashed) and actual body mass translated to in µg/kg lean body mass for the average male (dot and dash) and female (dotted) participants.
Associations Between Female Sex and Iatrogenic Thyrotoxicosis
HR, hazard ratio; CI, 95% confidence interval.
Thyroid hormone dosing by sex
The median daily levothyroxine dose per actual body mass was 1.1 (interquartile range [IQR] 0.8–1.5) μg/kg in male patients compared to 1.2 (IQR 0.7–1.4) μg/kg in female patients (p < 0.001). However, this gap was larger when calculated by ideal (M: 1.4 [IQR 0.8–1.9] vs. F: 1.7 [IQR 1.2–2.1] μg/kg; p < 0.001) or lean (M: 1.6 [IQR 1.0–2.2] vs. F: 2.2 [IQR 1.5–2.8] μg/kg; p < 0.001) body mass. The increasing separation in the male and female distributions for dose per kg body mass when the reference shifts from actual to ideal or lean body mass are illustrated in Figure 4A–C. This is true for both the peaks associated with prescriptions for 25 and 50 μg doses and the more normally distributed prescriptions for higher doses.

Distribution of thyroid hormone dosing by sex. This figure shows the distributions of daily levothyroxine doses prescribed to male and female patients. Doses are calculated in µg/kg body mass and the distributions for doses calculated using actual (top), ideal (middle), and lean (bottom) body mass are shown separately.
In our primary analysis, we tested whether the observed association between sex and iatrogenic thyrotoxicosis remains when female patients are compared against male patients receiving similar levothyroxine doses calculated using actual, ideal, and lean body mass, respectively (Table 2). In the fully adjusted Cox models, adjusting for dose per actual body mass did not significantly change the association (HR 1.50 [1.34–1.68]; p = 0.422) relative to the otherwise fully adjusted model. However, the association between female sex and thyrotoxicosis risk was significantly reduced (partial mediation) when adjusting for dose per ideal body mass (HR 1.30 [1.16–1.46]; p < 0.001). Furthermore, when adjusting for dose per lean body mass, the risk of thyrotoxicosis among females was statistically indistinguishable (full mediation) from that of males (HR 1.06 [0.95–1.19]; p < 0.001).
This analysis is graphically illustrated in Figure 5. The unadjusted 5-year cumulative incidence of iatrogenic thyrotoxicosis was 37% among female patients compared to 24% among male patients (Fig. 5A). When the cumulative incidence curves were stratified by dose per actual body mass tercile (Fig. 5B), iatrogenic thyrotoxicosis was more common among patients receiving higher doses. However, a gap persisted between female and male patients across all three dose terciles and was fully mediated by body composition at all dose levels (Fig. 5C). For example, female patients in the highest dose-per-body mass tercile had 5-year cumulative incidence of 66% compared with 56% among male patients in the same strata. In contrast, when the cumulative incidence curves were stratified by dose per lean body mass tercile, female and male patients in the highest dose per lean body mass tercile had 5-year cumulative incidence of 65% and 64%, respectively.

Cumulative incidence of iatrogenic thyrotoxicosis by sex.
Sensitivity analyses
Results from the sensitivity analyses are in Supplementary Table S3. When (a) severe thyrotoxicosis was used as the outcome, (b) the cohort was restricted to patients over 60 and not on estrogen (N = 11,229), (c) time zero included a 6-month run-in period, or (d) patients were censored after any prescriptions of potentially TSH altering medications, the association with patient sex remained fully mediated by dose per lean body mass. When the cohort was restricted to new starts (N = 4013), the sex association was fully mediated by both dose per ideal body mass and dose per lean body mass. When the cohort was restricted to patients with at least one TSH measurement above 10 mU/L (N = 5174), the association with sex was no longer fully mediated by dose per lean body mass (HR = 1.24 [1.01–1.52]).
Discussion
Using clinical data from over 20,000 older primary care patients, we report a significant, 54% higher rate of iatrogenic thyrotoxicosis in women versus men that could be explained to a large extent by overestimation of dosing requirements in women using the standard initial dosing algorithms that incorporate actual body mass. 15 We find, based on our models, that women have a significant 1.5 times higher rate of iatrogenic thyrotoxicosis than comparable men receiving the same dose per actual body mass. This difference does not appear to be explainable based on differences in demographics, comorbidity rates, medications, or frequency of TSH measurement. However, owing to differences in average body composition, the same dose per actual body mass translates to a higher dose per lean body mass for the woman, and this difference can account for the entirety of the observed difference in iatrogenic thyrotoxicosis risk.
This result appears to persist when looking both at the period immediately following initial levothyroxine prescription and 6 months later, following initial dose titration (Supplementary Table S2). This finding suggests that sex differences in thyrotoxicosis, which occur both early and later during LT4 therapy, have the same origin. Since initial doses are often chosen by weight according to guidelines, 15 the early dependence of sex difference on body composition appears relatively straightforward to explain. The persistence of the importance of body weight with longer exposures in older populations could result from the declines in lean mass with aging, accompanied by a failure to appropriately react to overtreatment by adjusting levothyroxine dose. This hypothesis is consistent with a prior study of overtreatment 3 in which a third of those with low TSH were found to have persistently low TSH on subsequent annual study visits. In addition, the primary mediation result appears consistent at both high and low doses (Fig. 5), which suggests that even using a conservative strategy of low, fixed doses (e.g., 25 or 50 μg daily), which do not account for body mass at the time of prescription, women are at higher risk of overtreatment because of difference in effective dose as a result of body composition. Further study is needed to confirm this hypothesis in clinical data.
Several additional observations are notable. First, we observed an independent risk of iatrogenic thyrotoxicosis from GLP-1 agonist use. This is potentially consistent with our finding as these therapies are known to affect body composition, lowering both lean and fat mass. Second, when we attempted to isolate patients with true hypothyroidism by requiring at least one observed TSH > 10, the sex differences in thyrotoxicosis risk were partly mediated rather than fully mediated by lean body mass. However, this cohort contains all of the patients who are undertreated, which is more common among men, leading to a greater sex difference before adjustment. None of the covariables that we measured affected the sex difference in this group either, so the small residual difference must be due to variables that we have not identified. For example, we did not test whether prior undertreatment is a risk factor for later overtreatment.
The use of EHR data in this study allowed us to examine prescribing practices at scale in a real patient population but comes with several limitations. Extraction of dosing information in this study relied on imperfect text processing, though we have no reason to believe that text processing errors were more common among men or women. Diagnosis codes may contain errors and do not reflect all symptoms (e.g., fatigue) relevant to diagnosis and treatment of hypothyroidism. Additionally, we can observe only what medications were prescribed to a patient and not what was taken. If there are sex biases in adherence to prescribed levothyroxine doses, this may have impacted our results. Similarly, if there are sex biases in the detection of thyrotoxicosis, this could impact our results, though we think this unlikely given the similar per-year rates of TSH testing and duration of follow-up (Table 1). A relevant limitation for clinical practice is the lack of direct measures of lean body mass in the data. Instead, we relied on prediction equations which generally reduce sex differences in lean body mass to one or two constant terms. However, our results are broadly concordant with existing studies using direct measures of lean body mass. 12 Finally, we have focused on adults age 50 and older, which means that other variables may be more relevant in younger populations.
One important observation is that, despite significant sex-based differences in numerous comorbid conditions that could have been driving dosing decisions, none of these factors explained the sex difference in iatrogenic thyrotoxicosis risk. Specifically, we looked at comorbidities such as depression and fatigue that have a sex-specific distribution and have been hypothesized to be associated with lower therapeutic TSH targets, as well as risk factor like atrial fibrillation that might mitigate against aggressive dosing and are also associated with sex-specific distributions. None of these comorbidities explained the female-predominant risk of iatrogenic thyrotoxicosis, again arguing against physician–patient interactions being the dominant risk factor for iatrogenic thyrotoxicosis.
Lean body mass has been recognized as an important determinant of euthyroid hormone requirement for 40 years. 16 The recommendations to dose thyroid hormone based on actual body mass derives from studies including patients with thyroid cancer, with no active thyroid hormone remaining, younger in age than the general population with hypothyroidism, and with variable goals of care, 17 all of which may contribute to recommendations that trend toward more aggressive dosing choices, which are not appropriate in all populations. Recommendations to use ideal body mass as a better proxy than actual body weight in dosing calculations have been published, but are not widely adopted, perhaps due to barriers to use. For example, we recently demonstrated that weight-based dosing recommendations derived from younger populations are highly likely to lead to overtreatment in older adults and obesity. That study recommended ideal body-weight-based algorithms, although also provided reduced actual body mass dose recommendations adjusted for age and body mass index (BMI) as a more readily adopted alternative. 18 Similarly, Baehr et al. looked at the determinants of thyroid hormone dose requirements and found that the differences in μg/kg body mass requirements between men and women, depending on pre- and postmenopausal status, were resolved by using ideal body mass. 19 In contrast, a second group has reported sex differences that emerged only when correcting for the differences in body mass, but these are focused on euthyroid patients and lack repeat measures which may lead to some methodological flaws. 20,21
Based on our estimates, reducing the iatrogenic thyrotoxicosis rate among women to be comparable to that found among men would prevent approximately two cases of thyrotoxicosis per 100 female patients on levothyroxine per year. It is also likely that switching to dosing guidelines based on lean body mass would reduce the overtreatment rate among both men and women, resulting in an even larger reduction in the overall iatrogenic thyrotoxicosis rate. As illustrated in Figure 3, an initial dose of 1.6 μg/kg actual body mass translates to lean body mass adjusted dose of 2.3 μg/kg for the average male patient in our data (71% lean body mass) and 2.8 μg/kg for the average female patient in our data (58% body mass). For both men and women at the relevant dose level, 14.8% of TSH measurements in men and 21% in women fell below 0.45 mU/L, whereas, at a dose of 1.6 μg/kg lean body mass, only 4.4% did. Fortunately, in the electronic medical record era, switching to a lean body mass–based dose calculation may be handled relatively easily. While most patients do not have direct measurements of lean body mass, several prediction equations exist that rely only on standard measurements such as weight, height, and BMI. Such equations can be implemented, either automatically or via calculators, in EHR systems. In the near term, physicians may use available online tools to obtain lean body mass from patient height and weight when deriving weight-based doses in order to mitigate the increased risk of overtreatment in older women.
Footnotes
Acknowledgment
The authors would like to thank Dr. David Cooper for his generous and valuable feedback on this work.
Authors’ Contributions
R.A.: Concept, design, statistical analysis, interpretation, and drafting the article. He has approved the final version and agrees to be accountable for all aspects of the work. J.S.M.: Concept, design, interpretation, and drafting the article. She has approved the final version and agrees to be accountable for all aspects of the work.
Data Sharing
The data used in this study comprise EHRs which have not been made publicly available to protect patient privacy. These data can be made available only under appropriate data use agreements. Please contact R.A. for additional details.
Author Disclosure Statement
J.S.M. has in-kind research support from Interpace Diagnostics.
Funding Information
This work was supported by the Turock Family Foundation and the Richman Family Precision Medicine Center of Excellence in Alzheimer’s Disease, including significant contributions from the Richman Family Foundation, the Rick Sharp Alzheimer’s Foundation, the Sharp Family Foundation, and others. R.A. is supported by NIH grant K25AG083064, and J.S.M. was supported by NIH grant R01AG064256 and R01AG088251.
Supplementary Material
Supplementary Data
Supplementary Table S1
Supplementary Table S2
Supplementary Table S3