
Abstract
Background:
Differentiated thyroid cancer (DTC) is the most common pediatric endocrine malignancy. The utility of ultrasound (US) surveillance after initial treatment has not been clearly delineated. We sought to evaluate the clinical utility of US for the detection of residual or recurrent disease in pediatric patients with thyroid cancer beginning 1 year after initial therapy.
Methods:
This is a retrospective cohort study of pediatric patients (<19 years) diagnosed with DTC between 1998 and 2022 whose response to therapy (RTT) one year after initial treatment (thyroidectomy ± radioactive iodine) was excellent or indeterminate. We evaluated the association between sonographic and biochemical findings (thyroglobulin [Tg] and Tg antibodies [TgAb]) at one year with the subsequent diagnosis of residual/recurrent structural disease in the neck (SDN).
Results:
In total, 112 patients had 1-year RTT that was excellent (n = 61, 54.5%) or indeterminate (n = 51, 45.5%). Median length of subsequent follow-up was 6.4 (interquartile range 3.8–8.9) years. Overall, 683 surveillance neck US were performed, with a mean ± standard deviation of 1.0 ± 0.4 US per patient per year. Of 61 patients with excellent RTT, none developed SDN during follow-up. Eighteen patients (29.5%) had a false-positive indeterminate or abnormal US finding. Of 51 patients with indeterminate RTT, 9 (17.6%) developed SDN during follow-up. SDN was detected by US in 7/9 cases (77.8%). SDN was detected by I-123 scan, but not by US, in two cases (22.2%), both with abnormal Tg/TgAb. 7/9 (77.8%) cases of SDN were detectable by Tg/TgAb. Overall, fine-needle aspiration (FNA) was performed in 17/112 (15.2%) patients and diagnosed SDN in six patients. Overall, 11/112 patients (9.8%) underwent FNA but were not diagnosed with SDN.
Conclusions:
In pediatric DTC patients with excellent response to initial therapy, the utility of serial US surveillance is limited by the low risk of SDN and frequent false-positive US findings. In children with indeterminate RTT, SDN occurs in a significant proportion and may be detected by US or by abnormal Tg/TgAb levels. These patients may benefit from the combination of US and biochemical surveillance.
Introduction
Differentiated thyroid cancer (DTC) is the most common endocrine malignancy in children and the most common solid cancer diagnosed in adolescence. 1 –3 Although mortality from pediatric thyroid cancer is rare, local and regional recurrences occur in up to 20% of patients. 4 Consensus guidelines from the American Thyroid Association (ATA) classify children with DTC as low, intermediate, or high risk for recurrence based on the extent of disease at the time of initial surgical resection. 5 For children with DTC, in addition to biochemical surveillance of thyroglobulin (Tg) levels, the ATA recommends surveillance ultrasound (US) every 6–12 months for at least 5 years to detect locoregional recurrence. 5 However, the utility of US surveillance in this population has not been clearly delineated. In one study evaluating US surveillance of pediatric DTC, no patient with an excellent response to therapy (RTT) at initial postoperative follow-up was diagnosed with structural disease in the neck (SDN) during an average follow-up of 2–3 years. 6 In addition, US evaluation of the neck post-thyroidectomy has the potential for false-positive findings that may generate unnecessary anxiety, investigations, and procedures. 7,8 This study aims to assess the utility of US for detecting residual/recurrent SDN in pediatric patients with DTC at a single referral center over an extended follow-up period.
Materials and Methods
This is a retrospective cohort study. It is Health Insurance Portability and Accountability Act-compliant and was approved by the institutional review boards of Boston Children’s Hospital (M10-08-0444) and Brigham & Women’s Hospital (2017P000660). The requirement for written informed consent was waived.
Patients
We reviewed the medical records of all patients diagnosed with DTC before 19 years of age who were evaluated in the integrated Pediatric Thyroid Center at Boston Children’s Hospital and Brigham and Women’s Hospital between 1998 and 2022. Patients were included in the study if they underwent an initial assessment of RTT at 1 year (±6 months) following initial surgical treatment (either total or hemithyroidectomy) and if subsequent follow-up with neck US was performed for at least 1 year after the initial assessment of RTT (Fig. 1).
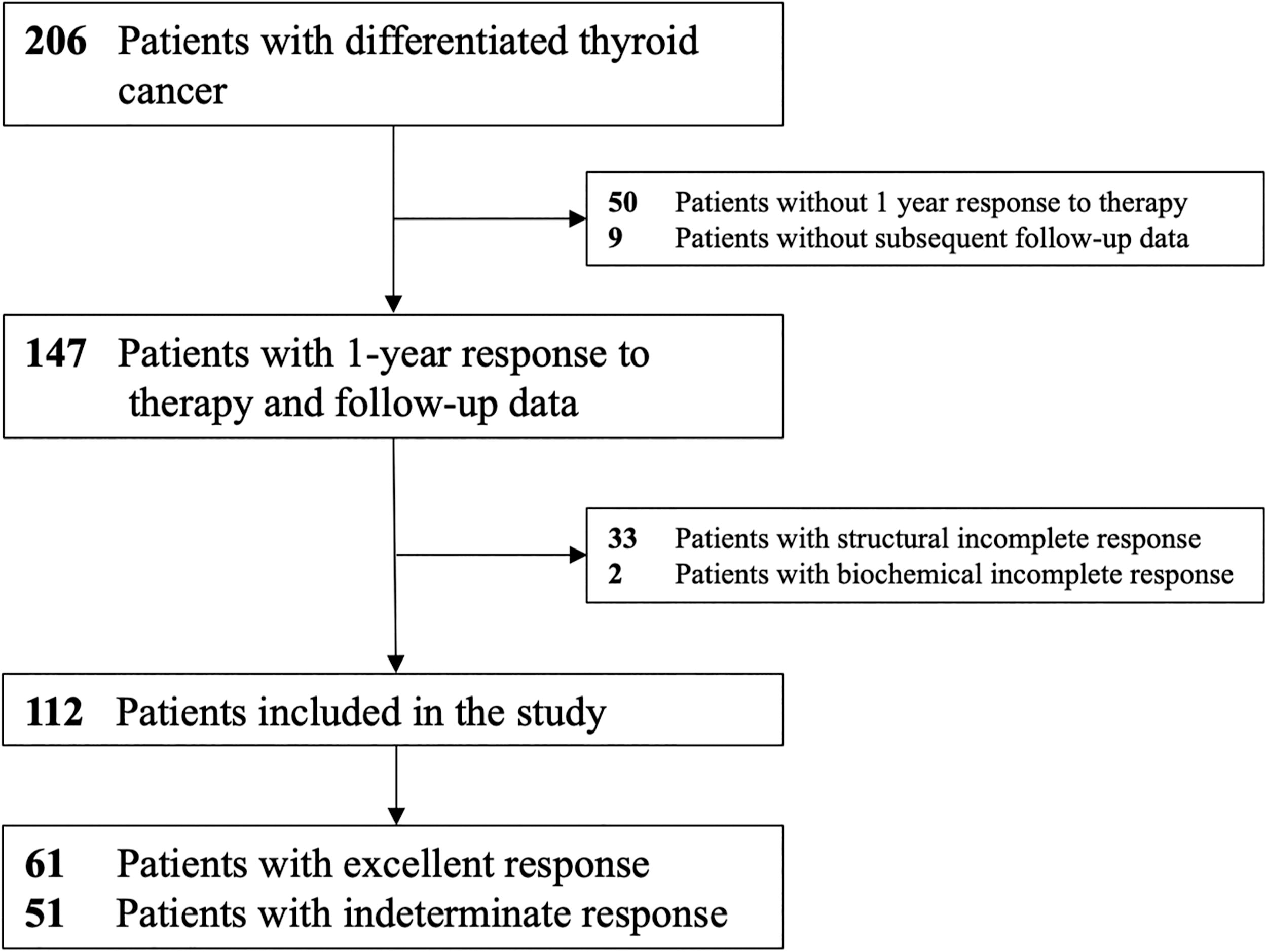
Study flow diagram with inclusion and exclusion criteria.
Subsets of this patient cohort have been previously reported. One study assessed US characteristics of thyroid cancer in children, another described a diagnostic and management approach to thyroid nodules, and one study assessed TI-RADS classification of pediatric thyroid nodules. 9 –11 None of these studies assessed long-term US or laboratory surveillance or included the entire cohort.
Thyroid cancer characteristics
Thyroid cancer tumor (T), lymph node (N), and distant metastasis (M) staging were assigned according to the American Joint Committee on Cancer Staging Manual, 8th Edition, and ATA pediatric risk level was assigned according to consensus guidelines. 5,12 RTT was defined by methods similar to ATA consensus guidelines as excellent, indeterminate, biochemical incomplete, or structural incomplete response (Supplementary Table S1). 13 Patients were included in the study if their RTT at 1 year was excellent or indeterminate; patients with biochemical or structural incomplete response were excluded.
Imaging classification
Neck US was performed using 10–15 MHz or 12–18 MHz linear transducers (Acuson, Sequoia, Siemens Healthineers, Mountain View, Calif; Logiq E9 or E10, GE Healthcare, Milwaukee, Wis). At our institution, each neck US assesses the post-thyroidectomy bed and the central and lateral neck. US reports were reviewed, and the following information was recorded: surgically absent thyroid lobes, presence and characteristics of thyroid bed lesions, and presence and characteristics of lymph nodes. Abnormal features of thyroid bed lesions or lymph nodes were defined as punctate echogenic foci, abnormal shape, or cystic areas. Thyroid bed lesions were classified as: benign if they were homogenous, oval, and had no abnormal features; indeterminate if they were round and had no abnormal features; and abnormal if they had any abnormal feature. Lymph nodes were classified as benign if they were homogenous, hypoechoic, oval, and had a visible hilum; indeterminate if they had no abnormal feature but had no visible hilum (Fig. 2A); and abnormal if they had any abnormal feature (Fig. 2B). Indeterminate and abnormal thyroid bed lesions and lymph nodes were further characterized by size in largest dimension, laterality, and stability from prior imaging. Based on the report, each US exam was classified as negative, indeterminate, or abnormal. For US reports that were unclear, direct image review was conducted by radiologists with expertise in thyroid and neck US and categorizations determined collaboratively (C.B.B., M.C.F., with 38 and 34 years of experience in thyroid US, respectively). Reports of all additional imaging during the follow-up period (I-123 or I-131 whole-body scans and CT) were reviewed and classified as negative, indeterminate, or abnormal. Fine-needle aspiration (FNA) cytology and surgical pathology of any thyroid bed lesions or lymph nodes were recorded.
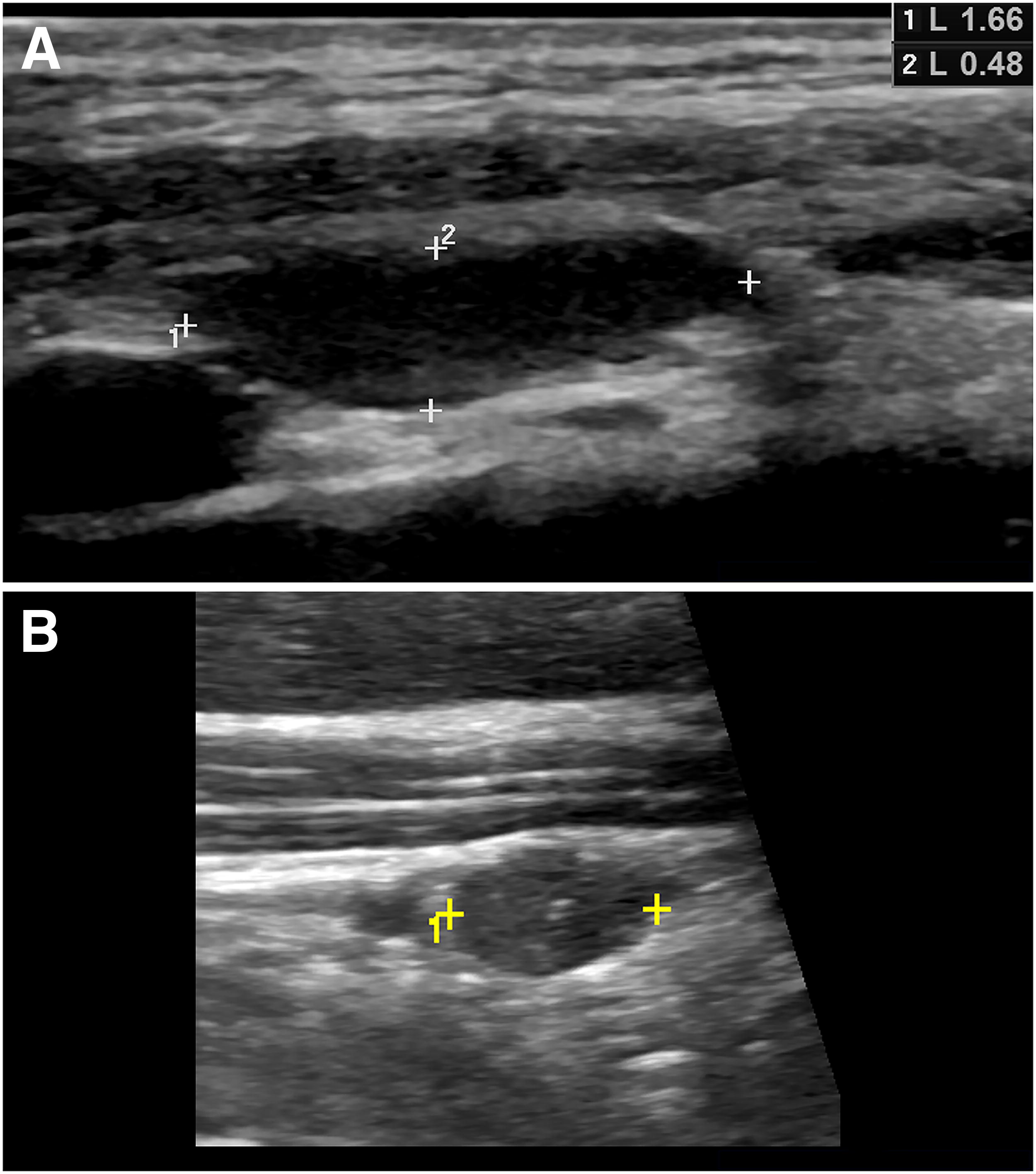
Representative sonographic images of lymph nodes.
Clinical outcome
The follow-up period for each patient began at the initial assessment of RTT and extended until the last available follow-up or the diagnosis of SDN, defined as (1) cytologically or histologically proven thyroid cancer or (2) abnormal radioiodine uptake in the lateral neck (with or without a sonographic correlate) and abnormal Tg or Tg antibodies (TgAb).
Analysis
The primary outcome of this study was the proportion of patients with SDN identified by US during follow-up. Test characteristics of US for detecting SDN were calculated considering an indeterminate or abnormal US as a positive test. Secondary outcomes included the association between diagnosis of SDN and initial RTT at 1 year. Categorical variables were compared using Fisher exact analysis, with a two-tailed p < 0.05 considered significant.
Results
Patient cohort
The study cohort included 112 patients (Table 1), of whom 88 (78.5%) were female. The median (range) age at diagnosis was 14.9 (7.0–18.9) years. Ninety-seven patients (86.6%) had papillary thyroid carcinoma (PTC), 11 (9.8%) had follicular thyroid carcinoma (FTC), three (2.7%) had oncocytic carcinoma (OCC), and one (0.9%) had a well-differentiated thyroid carcinoma, not otherwise specified (NOS). Additional tumor characteristics, including TNM staging and ATA pediatric risk level, are summarized in Table 1. The median (interquartile range [IQR]) length of follow-up after initial assessment of RTT was 6.4 (3.8–8.9) years.
Patient Characteristics
Data are presented as n (%) or median (range).
ATA, American Thyroid Association; NOS, not otherwise specified; y, years.
Among the 112 patients, a total of 683 US studies were performed, a mean ± standard deviation of 1.0 ± 0.4 US per patient per year (Table 2). During follow-up, 55 patients (49.1%) had at least one indeterminate and/or abnormal US: 34 patients (30.3%) had at least one indeterminate US, 7 patients (6.3%) had at least one abnormal US, and 14 patients (12.5%) had at least one indeterminate and one abnormal US. Among 119 indeterminate US studies, the indeterminate finding consisted of lateral neck lymph nodes in 66 studies (55.5%), thyroid bed or central neck lymph nodes in 42 studies (35.3%), and both central and lateral neck findings in 11 studies (9.2%). Among 44 abnormal US studies, the abnormal finding consisted of lateral neck lymph nodes in 21 studies (47.8%), thyroid bed or central neck lymph nodes in 19 studies (43.2%), and both central and lateral neck findings in 4 studies (9.1%). Seventeen patients (15.2%) underwent a total of 22 FNA biopsies of a thyroid bed nodule or cervical lymph node. Eleven of these patients were not diagnosed with SDN, representing 64.7% (11/17) of those who underwent FNA and 9.8% (11/112) of all patients.
Follow-Up Ultrasound Characteristics
Data are presented as n (%), median (interquartile range), or mean ± standard deviation.
Three other patients were diagnosed with SDN without a positive FNA. Two patients had nondiagnostic FNA cytology with malignant histopathology on resection, and one patient had abnormal I-123 uptake in the lateral neck without US correlate and abnormal TgAb.
FNA, fine-needle aspiration; LN, lymph node; US, ultrasound.
SDN was diagnosed in nine patients (8.0%), six by FNA cytology, two by surgical resection, and one by abnormal I-123 uptake without a sonographic correlate (Tables 2 and 3). The median (IQR) time to diagnosis was 2.5 (2.3–4.8) years after initial assessment of RTT. All cases of SDN were diagnosed in patients with indeterminate initial RTT and none in patients with excellent response (p < 0.001).
Characteristics of Patients with Residual/Recurrent Structural Disease in the Neck
Abnormal lateral neck uptake on I-123 study with elevated TgAb and without US correlate, treated with radioactive iodine and subsequently resolved.
ATA, American Thyroid Association; F, female; FNA, fine-needle aspiration; I-123, I-123 whole-body scan; M, male; PTC, papillary thyroid cancer; RTT, response to therapy one year after initial therapy; Tg/TgAb, thyroglobulin/thyroglobulin antibodies; US, ultrasound; y, years.
Outcomes based on initial RTT
Excellent response
Sixty-one patients (54.5%) had an excellent RTT one year after initial surgery (Table 2) and were followed subsequently for a median (IQR) of 6.3 (4.3–8.2) years. In this group, 347 surveillance US studies were performed, a mean ± SD of 0.9 ± 0.3 US per patient per year. No patient was diagnosed with SDN during follow-up.
Eighteen patients (29.5%) had at least one indeterminate US, and three of these 18 patients also had an abnormal US. Two patients had no correlation to their abnormal US findings on I-123 whole-body scan, had normal Tg/TgAb, and the abnormal US finding subsequently resolved. In the remaining patient, the abnormal US finding had no correlation on I-123, Tg/TgAb were normal, and FNA was benign. FNA was performed in two patients for abnormal I-123 uptake in the central neck in the setting of benign-appearing US correlates and normal Tg/TgAb. One lesion had benign cytology, and the other lesion had nondiagnostic cytology and resolved without treatment.
Indeterminate response
Fifty-one patients (45.5%) had an indeterminate RTT one year after initial surgery (Table 2, Fig. 3) and were followed subsequently for a median (IQR) of 6.4 (3.6–9.0) years. In this group, 336 USs were performed, a mean ± SD of 1.1 ± 0.5 US per patient per year.
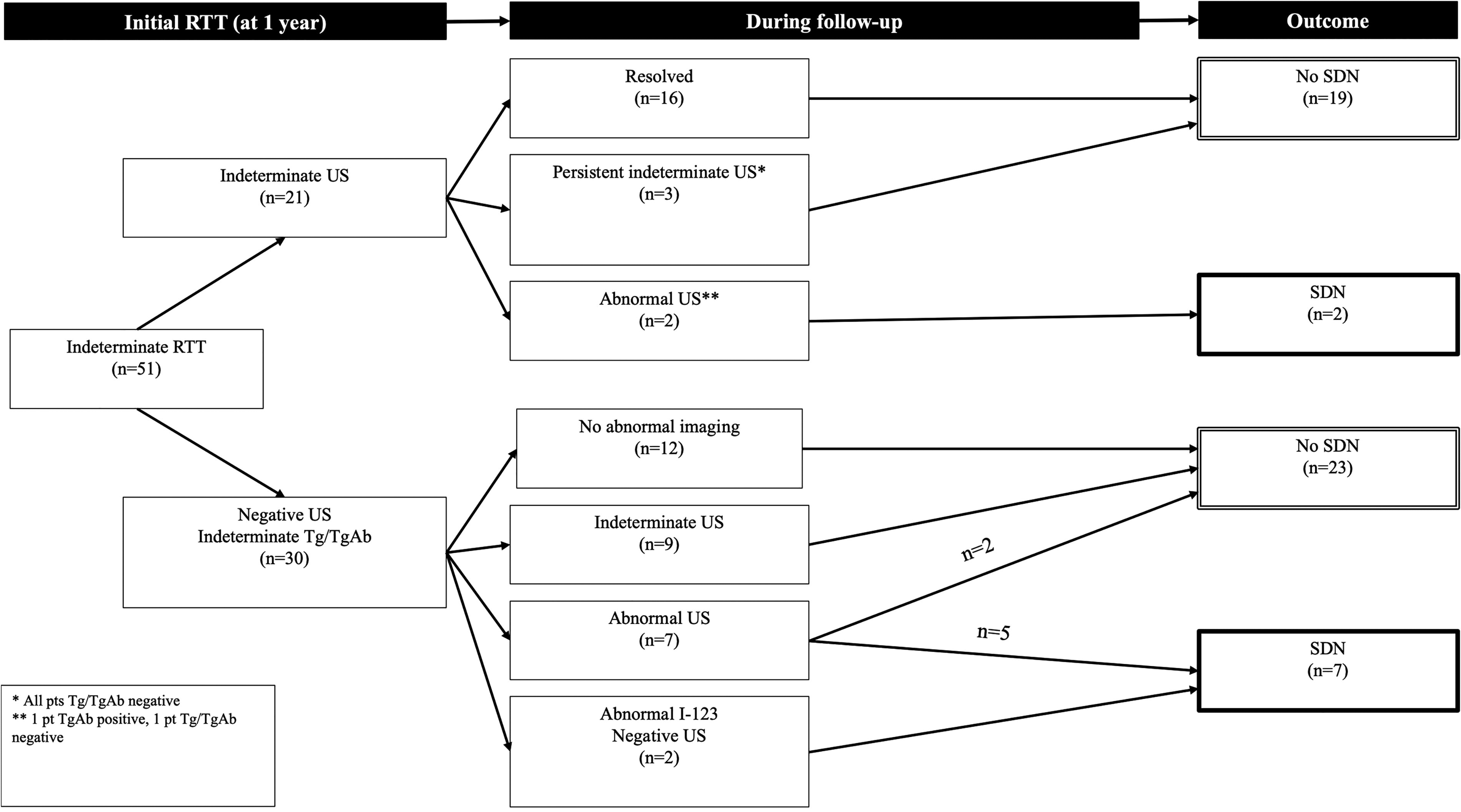
Outcomes of pediatric thyroid cancer with indeterminate initial response to therapy (RTT). Tg, thyroglobulin; TgAb, thyroglobulin antibody; US, ultrasound.
Thirty patients (58.8%) had at least one indeterminate US, 11 of whom also had an abnormal US. Seven patients (7/51, 13.7%) had an abnormal US without an indeterminate US. Nine patients (17.6%) were diagnosed with SDN during follow-up, all of whom were initially stratified as intermediate (n = 5) or high risk (n = 4) for recurrence by ATA criteria (Table 3). In seven patients, SDN was detected by an US that was indeterminate (n = 2) or abnormal (n = 5). The other two cases of SDN were detected by persistently elevated TgAb leading to I-123 scans that showed abnormal uptake in the lateral neck. One of these had no US correlation, and the other correlated on US with a benign-appearing lymph node that had nondiagnostic cytology but was malignant upon resection.
Among 51 patients with indeterminate RTT, 16 (31.4%) were so classified due to indeterminate US findings alone, 30 (58.8%) by abnormal Tg/TgAb alone, and 5 (9.8%) due to both indeterminate US and Tg/TgAb (Supplementary Table S2). The prevalence of SDN at follow-up was lower among patients initially classified as indeterminate RTT based solely on US findings (1/16, 6.3%) than among those with abnormal Tg/TgAb either with (1/5, 20%) or without (7/30, 23.3%) US findings, although this difference was not statistically significant (p = 0.34).
Indeterminate US findings present at the initial assessment of RTT resolved in most patients (16/21, 76.2%), after a median (IQR) of 1.6 (1.3–2.7) years (Fig. 3). Among the other five patients, the indeterminate US finding became abnormal in two cases, and SDN was diagnosed histologically in both (2/21, 9.5%) after 1.6 and 2.3 years, respectively. In one patient with SDN, the indeterminate-appearing lymph node was associated with positive TgAb and abnormal I-123 uptake, and in the other patient, the node was associated with negative Tg/TgAb but an abnormal appearance on contrast-enhanced neck CT. Three patients had indeterminate US findings that persisted throughout the study period, all with normal Tg/TgAb. In one patient, FNA cytology of the indeterminate finding was nondiagnostic twice. The three indeterminate findings remained stable on US for 3.0, 3.8, and 12 years, respectively. Overall, 8/14 patients (57.1%) with indeterminate RTT who underwent FNA were not diagnosed with SDN.
Among 30 patients with negative US and indeterminate Tg/TgAb one year after initial therapy, 7 patients (23.3%) were diagnosed with SDN after a median (IQR) of 3.0 (2.4–5.2) years of additional follow-up. SDN was detected in five patients by an abnormal US finding and in two patients by abnormal I-123 uptake without an US correlate. In 6/7 patients with SDN, the Tg/TgAb remained abnormal over the study period, but in one patient, the initial Tg/TgAb elevation normalized and SDN was detected only by follow-up US.
Outcomes based on thyroid cancer type
All nine cases of SDN occurred in patients with PTC (9/97, 9.3%) during a median (IQR) follow-up of 6.4 (4.1–8.6) years after initial assessment of RTT. Of the 15 patients with FTC, OCC, or well-differentiated carcinoma NOS, 14 (93.3%) had excellent initial RTT, one patient (6.7%) had indeterminate RTT, and none developed SDN during a median (IQR) subsequent follow-up of 7.6 (3.0–9.5) years.
Sensitivity and specificity of US
The overall sensitivity and specificity of an indeterminate or abnormal US for the detection of SDN were 0.78 [confidence interval, CI 0.40–0.97] and 0.53 [CI 0.43–0.63], with positive predictive value (PPV) and negative predictive value (NPV) of 0.13 [CI 0.05–0.24] and 0.96 (CI 0.88–1.00), respectively (Table 4).
Test Characteristics of Ultrasound for Diagnosing Residual/Recurrent Structural Disease in the Neck More than One Year After Initial Therapy
Data are presented as ratio (95% confidence interval), [n/N]. N/A, not applicable, no cases of structural disease in the neck in this subgroup.
In patients with indeterminate initial RTT, the sensitivity and specificity of US were 0.78 [CI 0.40–0.97] and 0.31 [CI 0.18–0.47], with PPV and NPV of 0.19 [CI 0.08–0.36] and 0.87 [CI 0.60–0.98], respectively (Table 4). Tg or TgAb was elevated in 7/9 patients (77.8%) with SDN and absent in 2/9 (22.2%). In patients with excellent initial RTT, the specificity of US was 0.70 [CI 0.57–0.81], PPV was 0 [% CI 0–0.19], and NPV was 1 [% CI 0.92–1]; sensitivity could not be calculated because no cases of SDN were diagnosed in this subgroup.
Discussion
In pediatric DTC, US surveillance is recommended to detect the local disease persistence or recurrence that occurs in a substantial proportion of patients. Current guidelines recommend US surveillance every 6–12 months for at least 5 years, depending on postoperative risk stratification. 5 In adults, initial risk estimates are modified by periodic reassessment of RTT, and the frequency of surveillance is decreased in patients at low risk. 13 Recent data support the accuracy of similar dynamic risk stratification in pediatric DTC, but how RTT should influence subsequent US surveillance remains unclear, particularly for children at low risk of recurrence. 14 –19
In this cohort of children with DTC and excellent or indeterminate RTT followed for up to 20 years, the risk of residual or recurrent SDN in the neck was low (8.0%). Annual US surveillance in this cohort had high sensitivity and NPV but low specificity and PPV for identifying SDN. US surveillance had minimal utility in patients with excellent RTT one year after initial therapy, none of whom developed SDN over a median of 6.3 years of additional follow-up. Moreover, US surveillance yielded false-positive indeterminate or abnormal findings in nearly half of the patients without disease, prompting unnecessary FNA procedures in 11/112 patients (9.8%). These findings are consistent with those of a prior study that demonstrated no recurrent or residual cervical disease but a high false-positive rate over an average follow-up of 2.3 years in 25 children with normal initial postoperative US. 6 Our data from a larger cohort over a longer follow-up period suggest that children with an excellent initial RTT are unlikely to benefit from ongoing US surveillance and that decreasing the frequency of US surveillance may reduce anxiety, unnecessary investigations, and costs without missing local recurrences.
Among patients with initial indeterminate RTT, we observed a substantial rate of SDN (17.6%). Most of these were detectable by US, usually in combination with abnormal Tg/TgAb but in two cases by US alone; conversely, two cases not visualized by US were detected by Tg/TgAb and functional imaging. In this group, serial US and biochemical testing appear complementary and both contribute to effective surveillance.
Rates of SDN differed slightly based on whether initial indeterminate RTT was determined by US findings alone or by abnormal Tg/TgAb. Patients with indeterminate US findings but normal Tg/TgAb had lower rates of SDN (6.3%) than those with abnormal Tg/TgAb (22.9%), although the difference was not statistically significant. Therefore, the presence of abnormal Tg/TgAb may warrant greater concern for SDN, of which most (but not all) are eventually detectable by US. Notably, in this group, SDN was diagnosed after a median of 4 years, and up to 10 years, of additional follow-up. Therefore, serial US surveillance may be advisable for at least 5 years in children with indeterminate Tg/TgAb levels.
In contrast, indeterminate US findings present at 1-year postoperatively subsequently resolved in most cases (76.2%), generally in under 2 years. No SDN was observed in this subgroup, whereas indeterminate findings that persisted were more likely to represent SDN (2/5, 40%), particularly if their appearance became more abnormal over time. Thus, initial indeterminate US findings unaccompanied by Tg/TgAb elevation appear unlikely to represent SDN, and continued observation for resolution or persistence may be warranted before pursuing further evaluation. Patients who revert to excellent RTT due to resolution of indeterminate US findings may benefit from decreased frequency of US surveillance.
Nearly half of pediatric DTC patients in this cohort were classified postoperatively as intermediate- or high risk for recurrence. However, their rates of local recurrence were more consistent with those predicted by their 1-year RTT than by postoperative risk stratification. In prior studies, rates of local recurrence were 0–4% in patients with excellent initial RTT and 2.7–25% in patients with indeterminate initial RTT. 14 –19 Our findings are similar and provide additional support for the utility of dynamic risk stratification to individualize surveillance regimes over time in children with DTC. Of note, among adult PTC patients who have an excellent RTT, the risk of recurrence is increased in those with ATA high-risk cancers compared to those with low-risk cancers. 20 No such difference was detected in our pediatric cohort, but the small number of high-risk cancers with excellent RTT (n = 5) precludes drawing meaningful conclusions about this question in children.
Strengths of this study include its large size for a pediatric DTC cohort, comprehensive data collection, and substantial duration of follow-up. A limitation due to the retrospective design and long study period was the lack of standardized criteria for reporting US findings as benign-appearing, indeterminate, or abnormal. This resulted in heterogeneity in classifying findings among radiologists, although this heterogeneity is reflective of typical clinical practice. Additionally, image review was required to classify some findings, and this reclassification may not reflect accurately the effect of US on clinical decision-making at the time. Third, since our patient population is primarily pubertal, our findings may not be generalizable to younger children.
In summary, our findings demonstrate that in pediatric DTC patients with excellent or indeterminate response to initial therapy, further US surveillance detects SDN in only a small number of cases (8%) but detects many false-positive indeterminate or abnormal findings that may lead to unnecessary anxiety, interventions, and cost. US surveillance has very limited utility in children with an excellent initial RTT. In these patients, surveillance of Tg and TgAb, with US performed less frequently or only for rising Tg or TgAb, appears likely to reduce unnecessary studies without missing clinically significant local disease. For children with indeterminate RTT, combined surveillance with US and Tg/TgAb appears appropriate and will detect local persistence or recurrence in a significant proportion.
Footnotes
Authors’ Contributions
S.R.: Investigation, data curation, formal analysis, and writing—original draft. M.C.F.: Conceptualization, methodology, investigation, data curation, and writing—review and editing. C.B.B.: Methodology, investigation, data curation, and writing—review and editing. C.E.C.: Investigation, and writing—review and editing. J.R.S.: Investigation and writing—review and editing. A.J.W.: Conceptualization, methodology, investigation, data curation, formal analysis, writing—review and editing, and supervision.
Author Disclosure Statement
The authors have no relevant financial relationships or conflicts of interest to disclose.
Funding Information
This work was not supported by any funding sources.
Supplementary Material
Supplementary Table S1
Supplementary Table S2