
Abstract
Background:
Thyroid cancer (TC) is infrequently encountered in Birt–Hogg–Dubé (BHD) syndrome. We describe three BHD patients with TC and review the relevant literature.
Patient Findings:
Patient 1, a 55-year-old male with BHD, developed dedifferentiated oncocytic TC with distant metastases, requiring systemic therapy and radiation. Genetic testing revealed pathogenic variants (PVs) in FLCN, DAXX, and TP53. Patient 2, a 51-year-old female, and her 30-year-old daughter (patient 3) were diagnosed with papillary TC and treated with surgery and radioiodine. Tumor testing in patient 3 demonstrated PV in BRAF (V600E). Gene query analysis (n = 2285 patients) identified 2% FLCN PV prevalence in sporadic TCs, but the prevalence increased to 23% in anaplastic TCs. Literature review revealed 15 TC cases in BHD with diverse clinical presentations.
Conclusions:
TCs are rare in BHD. FLCN PVs may not be the sole molecular drivers in TCs but may have a substantial role in the development of aggressive TCs.
Introduction
Birt–Hogg–Dubé (BHD) 1 syndrome is a rare, autosomal dominant disorder due to germline loss-of-function pathogenic variant (PV) in the folliculin gene (FLCN). 2 Clinical manifestations include multifocal, bilateral pulmonary cysts, spontaneous pneumothorax, cutaneous manifestations (such as fibrofolliculomas, trichodiscomas), and renal cell carcinoma (RCC). 2 Insertion, deletion, and nonsense mutations lead to premature truncation and loss of function of the FLCN protein. 3 Although the precise mechanism is unclear, FLCN likely functions as a tumor suppressor gene (Supplementary Data). 4 –7
Tumors of other sites are rare in BHD; however, colorectal, lung, and breast cancers and parotid oncocytomas have been described. 8 Thyroid cancer (TC), although reported, is not one of the classical manifestations of BHD. 1,8 –15 Due to the rarity of this association and the undeciphered potential interactions between FLCN and molecular drivers of TC, currently no causal link between BHD and TC exists. 16
We report a series of three BHD patients: one with oncocytic thyroid cancer (OTC) and two patients (mother and daughter) with papillary thyroid cancer (PTC), and review the current literature on TC in BHD (Table 1). We also perform a gene query analysis of FLCN PVs in TC on cBioPortal (www.cbioportal.org). Our study’s objectives were to report BHD and associated TC and hypothesize that FLCN may be an oncogenic driver in TC. The patients were enrolled under the National Institutes of Health Institutional Review Board-approved research protocols (77-DK-0096 and 10-DK-0102), and all patients signed informed consent.
Summary of Clinical and Pathological Data from Our Case Series and from the Literature
Patient was diagnosed based on strong family history, but FLCN mutation in tissue serves as confirmation for BHD in patient.
OTC, oncocytic thyroid cancer; MTC, medullary thyroid cancer; PTC, papillary thyroid cancer; FTC, follicular thyroid cancer; N/A, not available; LOH, loss of heterozygosity; PTx, pneumothorax; LLL, left lower lobe; PFT, pulmonary function test; RCC, renal cell cancer.
Patient 1
A 55-year-old Caucasian male with BHD, identified through pulmonary cysts and family history of BHD, was referred to our center for management of metastatic TC. Originally, TC presented as a neck swelling upon routine examination. He denied symptoms of hyper- or hypothyroidism, family history of TC, or radiation exposure. Thyroid ultrasound (US) revealed a 3.9 cm right lobe hypoechoic nodule with punctate echogenic foci (Fig. 1a). Fine needle aspiration (FNA) biopsy of the nodule revealed follicular lesion of undetermined significance with oncocyte-like cells (Bethesda III) (Fig. 1b). After a total thyroidectomy with central neck dissection, histopathology revealed OTC (Fig. 1c–e) measuring 3.9 cm, with capsular and lymphovascular invasion, involving three out of six central lymph nodes (American Thyroid Association [ATA] high-risk for recurrence 17 ; American Joint Committee on Cancer 8th Edition [AJCC 8th Ed.] 18 pT2N1aM0, Stage II). He received 156 mCi (5.8 GBq) of [131I]-radioactive iodine (RAI) therapy.
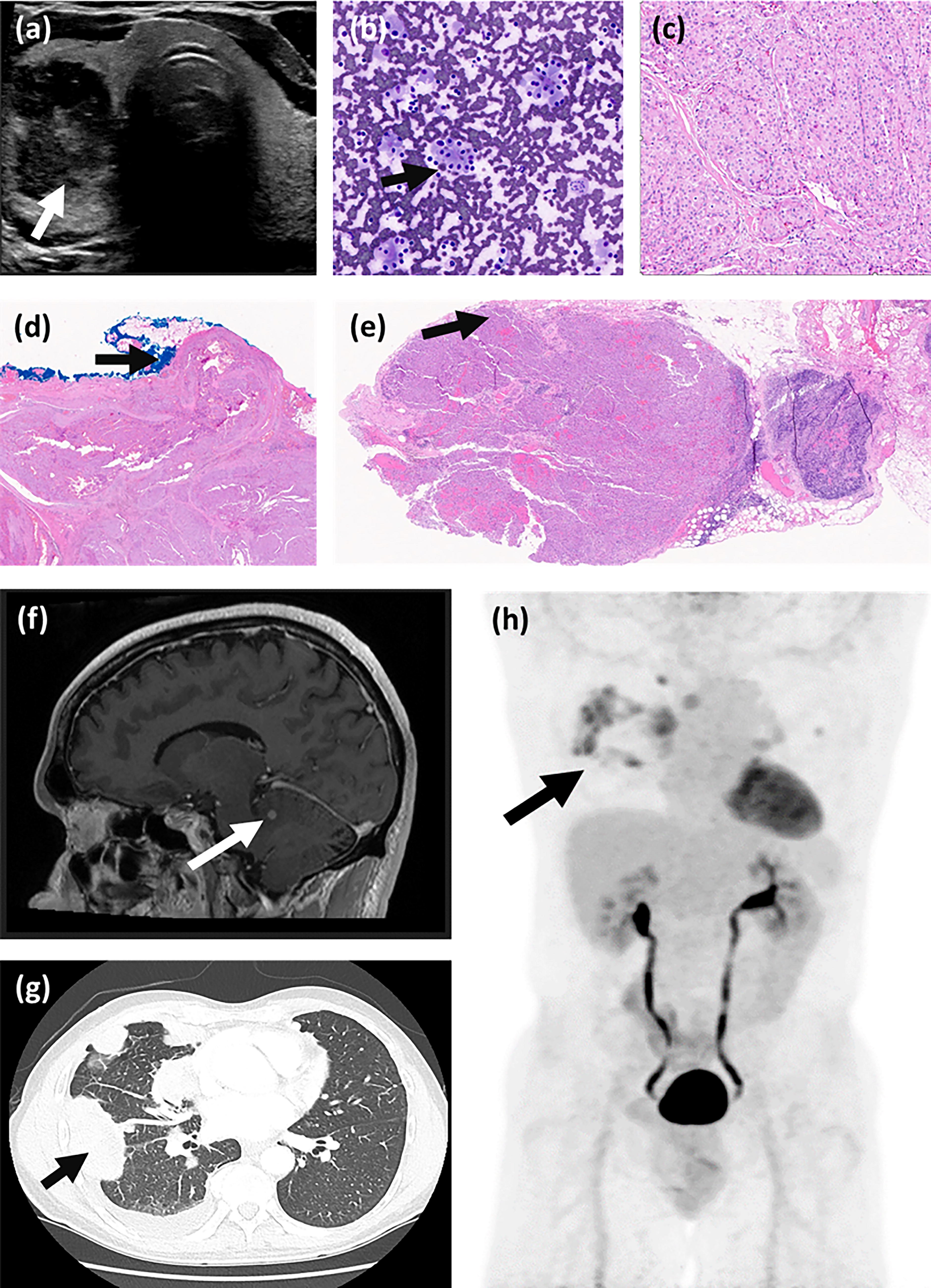
Thyroid US, FNA of thyroid nodule, histopathology, and imaging for distant metastases in patient 1.
One-year post-therapy scan revealed residual neck disease. Lymph node dissection revealed a 1.8 cm metastatic OTC, involving 3 out of 28 nodes. Tumor genetics revealed FLCN (H429fs*27), DAXX (L666fs*29), and TP53 (R248Q) PVs. Inoperable, bulky right parapharyngeal disease encasing the carotid artery was noted one year later, and he was treated with 4000 cGy ×5 fractions of stereotactic radiotherapy. Two years later, brain magnetic resonance imaging (MRI) (Fig. 1f) showed right cerebellar metastasis, which was treated with 2000 cGy gamma knife radiation. Computed tomogram (CT) of the chest and an [18F]-fluorodeoxyglucose positron emission tomography/CT (Fig. 1g and h) demonstrated hilar, pulmonary, and pleural metastases. Biopsy of one pleural nodule confirmed poorly differentiated TC (PDTC) bearing histopathological similarity to the initial OTC. Systemic therapy with everolimus and lenvatinib was initiated due to rapid disease progression, but everolimus was discontinued due to pneumonitis. He is currently undergoing evaluation for immune checkpoint inhibitor therapy.
Patient 2
A 51-year-old Caucasian female with BHD harboring germline FLCN PV (H429Tfs*39) presented with a neck lump. BHD manifested as bilateral pulmonary cysts and nodules, and two exophytic lesions from the left kidney. Medical history included bipolar disorder and uterine fibroid; family history included TC and pulmonary disease. Thyroid US and FNA confirmed PTC. After total thyroidectomy and central neck dissection, histopathology revealed multifocal classical PTC, with the largest focus measuring 1.2 cm, involving surgical margins, with microscopic involvement of strap muscles and lymphovascular invasion, involving 11 out of 14 central lymph nodes (AJCC 8th Ed. pT1bN1aM0, Stage II). Due to inadequate material, tumor genetic testing was not performed. Two RAI treatments with a cumulative dose of 130 mCi (4.81 GBq) were administered, and excellent response to therapy was noted three years after initial therapy.
Patient 3
A 30-year-old Caucasian female, daughter of patient 2, visited our center for evaluation of one-year history of throat discomfort, dysphagia to solids, and voice changes. Medical history included pulmonary cysts, spontaneous pneumothorax, bipolar disorder, gestational diabetes, and Guillain–Barré syndrome without residual deficits. Physical examination was unremarkable without palpable cervical adenopathy. Genetic testing confirmed germline FLCN PV similar to her mother (H429Tfs*39). Thyroid US showed a 1.9 × 1.8 cm heterogeneous nodule with punctate echogenic foci, and a suspicious 2.4 cm left level III lymph node. FNA of the nodule was inconclusive (Bethesda I). After total thyroidectomy and central lymph node dissection, histopathology revealed multifocal PTC, with the largest focus being 2.2 cm, without surgical margin involvement or gross extrathyroidal extension, but all seven central neck lymph nodes harbored metastases, with the largest metastatic deposit of 0.6 cm (AJCC 8th Ed. pT2N1aM0, Stage I). RAI with 100 mCi (3.7 GBq) was administered under thyrotropin stimulation. Post-therapy scan revealed uptake in the left neck without local or distant metastasis. Tumor genetics identified BRAFV600E and the known FLCN germline PVs.
FLCN as a somatic driver in TC
We analyzed 2334 TC samples from 2285 patients with PTC, PDTC, and anaplastic TC (ATC) on cBioPortal (www.cbioportal.org). FLCN PVs were found in 2% of all the TC cases; however, FLCN PV prevalence was as high as 23% in ATC samples. While the overall survival in TC patients with FLCN PVs was significantly worse compared with those without FLCN PVs (hazard ratio: 19.86, 95% confidence interval: 2.91–135.76), the overall survival was similar between ATC patients with FLCN PVs and ATC patients without FLCN PVs (Supplementary Data). 19,20
Discussion
We describe three patients with BHD and TC, along with associated molecular driver data. We then show FLCN PVs are more likely to be found in highly aggressive TC subtypes, such as ATC.
Over 400 families affected with BHD have been described, 21 and there are 15 documented TC cases in BHD (Table 1), with a median age of presentation of 47 years (range: 28–72), and similar sex predilection (50% female, four out of eight subjects). 1,8 –15 Eight of the 15 patients had confirmed germline FLCN PVs.
Among the reported cases, 1,8 –15 the TC subtypes were as follows: two OTC, 9,15 seven medullary TC, 1,12 two PTC, 8 two follicular TC, 13,14 one primary clear cell TC, 11 and one unspecified TC subtype. 10 Three out of six patients with lymph node involvement had evidence of lymphovascular invasion. 8,13 Three patients had distant metastasis. 1,11,13 OTC is associated with a poorer prognosis among differentiated TCs. 22 Ten-year disease-free interval for FTC and OTC is about 75% and 41%, respectively. 22 Furthermore, OTC has a higher recurrence rate, as evidenced in patient 1 from our series. 23 These findings may corroborate with our cBioPortal analysis revealing FLCN PVs predominating in aggressive tumors like ATC.
In a five-year prospective French study, thyroid nodules were prevalent in (13 out of 20) 65% of patients with BHD 16 ; however, all of these nodules were benign, and no TC cases were identified. 16 Additionally, 9 out of 10 (90%) families affected by BHD with germline FLCN PVs had individuals with thyroid nodules, but this increased prevalence may be due to selection bias. 16
To date, there are two other reported cases of patients with BHD and OTC. 9,15 One case was discovered when an 18FDG-PET scan was conducted to investigate RCC, but further details on OTC were not provided. 9 The second OTC case was noted in a BHD cohort of 120 families from Japan and Taiwan. 15 Although the clinical details on this patient were not provided, interestingly, somatic mutation analysis of the OTC tissue demonstrated the FLCN PV (c.1285dupC) almost entirely replacing the wild-type FLCN, indicative of loss of heterozygosity (LOH). 15
FLCN haploinsufficiency may enhance apoptosis, impair cellular attachment, and alter cell adhesion protein function as evidenced in pleural mesothelial cells. 24 Whether such FLCN haploinsufficiency could have caused defective cell adhesion in TC needs further research. Haploinsufficiency in the FLCN gene may not be the predominant molecular driver for TC tumorigenesis but might synergize with coexisting PVs to promote tumorigenesis. For instance, patient 1 in our cohort harbored PVs in TP53 and DAXX, which are known PVs in OTC, and these PVs may have contributed toward tumorigenesis along with FLCN haploinsufficiency. 25 However, LOH in FLCN gene may possess a higher potential to be the sole molecular driver rather than FLCN haploinsufficiency in the pathogenesis of TC. 15
Among seven patients with known renal disease, 8 –13 five had renal manifestations, including three with confirmed RCC, 8,11,13 one with bilateral renal masses, 9 and one with a renal cyst. 12 Renal tumors exhibit LOH in FLCN due to somatic second-hit mutation in about 53% of cases. 26 Therefore, LOH in the FLCN gene might play a substantial role in the pathogenesis of renal tumors in BHD; however, this may not be the case with other BHD tumors. 26 For example, skin fibrofolliculomas in BHD were shown to strongly express FLCN mRNA, and LOH was not detected in these tumors, 21 suggesting that LOH in FLCN is not the sole oncogenic driver in these tumors, and such might be the case with other nonrenal BHD tumors, including TC.
An additional case of BHD with noninvasive follicular thyroid neoplasm with papillary-like nuclear features (NIFTP) has been described. 27 This case was not included in Table 1, as NIFTP is no longer considered a malignancy. 28 Patient was a 44-year-old female with BHD, a germline FLCN PV (A90S), skin tags, bilateral pulmonary cysts, and clear cell RCC, without family history of TC or history of radiation exposure. 27
The canonical pathway associated with FLCN function is RAS-PI3K-Akt-mTOR, and loss of FLCN function may lead to overactivation of mTOR (Supplementary Data). 29 Tyrosine kinase inhibitors (sorafenib, lenvatinib, and cabozantinib) remain the mainstay of therapy in RAI-refractory, progressive TC. However, mTOR inhibitors may be utilized in patients with FLCN-mutated TCs. In fact, treatment with mTOR inhibitor, everolimus, led to an unusually prolonged treatment response in a patient with ATC harboring FLCN, TSC2, and TP53 PVs. 30 FLCN may also function through noncanonical pathways. 4 For instance, cuboidal cells resembling type II pneumocytes that are frequently observed in the innermost layers of BHD-associated lung cysts exhibit activation of mTORC1 and hypoxia-inducible factor (HIF)–vascular endothelial growth factor pathways. 4 HIF-1α is a well-known oncogenic driver, with overexpression in tumors linked to poor prognosis and treatment response. 31 Utilizing HIF-1α inhibitors may be a therapeutic option, having demonstrated promising in vitro results by inhibiting TC growth. 31 Another potential mode of abnormal FLCN-mediated tumor growth could involve increased Wnt-β-catenin signaling, which is often observed in late-stage TCs, and in vitro siRNA-mediated knockdown of FLCN can be associated with increased Wnt signaling. 32 Several inhibitors of Wnt signaling are being evaluated in clinical trials that may hold promise in treatment of TCs with defective FLCN function. 32 –34
In conclusion, BHD may be associated with TC, including aggressive histological subtypes. The molecular signature of TC in BHD patients suggests that FLCN is likely not the only oncogenic driver. But in instances of LOH, FLCN may indeed become a prominent molecular driver for TC tumorigenesis, but this warrants further research. The rarity of TC in BHD, and of BHD in general, precludes provision of a tailored, comprehensive guidance toward management of TC in BHD population. Continued accrual of knowledge on this condition and TC data from larger BHD cohorts is needed in order to delineate a true pathological association between FLCN and TC. Our data on FLCN prevalence should also be interpreted with a caveat that cancer databases such as cBioPortal undergo constant revision, and pathogenic status of a gene variant may be reassigned thereby affecting the prevalence of the said variant. Larger sample sizes, along with improved molecular characterization and mechanistic studies evaluating the downstream effects of mutated FLCN in TCs, may assist with tailoring the monitoring and with optimizing therapy of TC in BHD patients.
Footnotes
Acknowledgments
The authors would like to thank the patients for participating in the study and the health care providers who cared for them at the authors’ institution and referred them for evaluation through the authors’ clinical protocol.
Authors’ Contributions
S.V. and E.C. are joint co-first authors. S.G. and J.K. conceptualized and designed the study. S.V., E.C., J.K., S.G., K.B., and P.V. were involved in patient care and formal evaluation, as well as supervising the study subjects. All authors contributed to the acquisition and interpretation of clinical data. S.V., E.C., J.K., and S.G. drafted the article. M.J. assisted in creating ‘figure 1' in the supplementary material. All authors revised the report and approved the final version before submission. S.V. and E.C. are the guarantors and attest that all listed authors meet authorship criteria and that no individuals meeting the criteria have been omitted.
Author Disclosure Statement
All authors declare no competing interests.
Funding Information
This research was supported by the Intramural Research Programs of the National Institute of Diabetes and Digestive and Kidney Diseases and the Center for Cancer Research, National Cancer Institute, National Institutes of Health. Clinical trial registration number: NCT-01109420.
Principal Investigator: J.K., Intramural Funding #ZIA DK047053-17.
Supplementary Material
Supplementary Data
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.