
Abstract
Background:
The management of indeterminate thyroid nodules (ITNs), classified as Bethesda III and IV, is challenging due to biopsy limitations in distinguishing benign from malignant nodules. While diagnostic lobectomy is the standard, thermal ablation (TA) is increasingly considered for patients ineligible or unwilling to undergo surgery. This systematic review and meta-analysis therefore evaluate the efficacy and safety of TA for ITNs.
Methods:
A comprehensive search of MEDLINE, EMBASE, and COCHRANE databases was conducted through May 11, 2025, for studies on ITNs treated with TA, with ≥12 months of follow-up and reported clinical or safety outcomes. Case reports, abstracts, and reviews were excluded. Two radiologists independently performed data extraction and quality assessment. Outcomes included volume reduction rate (VRR), regrowth, delayed surgeries, malignancy detection, and complications. The Risk of Bias for Nonrandomized Studies (RoBANS) tool was used for quality assessment. A random-effects model synthesized pooled estimates, with heterogeneity quantified by Higgins’ I 2.
Results:
A total of 15 studies with 1149 nodules were analyzed, showing progressive VRR increase, plateauing at 48 months. The pooled 12-month VRR was 81.0% (confidence interval: 76.0–85.9%). Hydrodissection significantly improved VRR at 6 months (p = 0.03), while larger nodules were more prone to regrowth. Major complications occurred in 1.8% (21/1149), with no reported metastasis. Regrowth and delayed surgery occurred in 2.3% (26/1149) and 0.3% (4/1149), respectively, with three malignancies upon delayed surgery.
Conclusions:
TA may be considered a minimally invasive alternative for ITNs who are not candidates for or decline surgery, demonstrating favorable efficacy and safety. However, study limitations, short follow-up, and residual malignancy risk necessitate careful follow-up, particularly for larger nodules. Advanced TA techniques such as hydrodissection may enhance outcomes by increasing the likelihood of complete ablation. Long-term prospective studies and randomized trials are needed to confirm TA’s role in clinical practice.
Introduction
Thyroid nodules are increasingly common in clinical practice, with reported incidence rates in adults reaching up to 67%. 1 These nodules can be classified as benign, malignant, or indeterminate, with indeterminate cases accounting for 19.7%. 2 The pathological findings for these indeterminate nodules range from benign to malignant and include low-risk neoplasms. 3 The Bethesda system estimates the risk of malignancy for indeterminate nodules as 13–30% for Bethesda III and 23–34% for Bethesda IV. 4
The management of indeterminate thyroid nodules (ITNs) remains a challenge because biopsy methods such as fine-needle aspiration (FNA) and core needle biopsy (CNB) cannot reliably differentiate between benign and malignant nodules. FNA has low sensitivity, whereas CNB offers greater diagnostic accuracy but still has a high rate of false-positive results. 5 –8 This limitation leads to the recommendation for diagnostic lobectomy. Surgery provides a definite diagnosis because it allows the detection of vascular, capsular, and extrathyroidal tissue invasion, but comes with potential complications such as vocal cord palsy, hypothyroidism, and hypocalcemia. 9 Furthermore, the majority of surgically removed nodules turn out to be benign. 10
Thermal ablation (TA), such as radiofrequency ablation (RFA) and microwave ablation (MWA), is increasingly being used for minimally invasive treatment of thyroid lesions. 11 –18 Current international guidelines recommend TA for benign nodules, recurrent thyroid cancers, and papillary thyroid microcarcinomas (PTMCs). 18 –23 However, the guidelines do not recommend TA for ITNs because of insufficient evidence. 24,25 Although diagnostic hemithyroidectomy is the standard management for ITNs, recent studies suggest that TA may be an option for patients who cannot undergo or refuse surgery. To further investigate this possibility, we conducted a systematic review and meta-analysis to evaluate the feasibility and safety of TA for ITNs.
Materials and Methods
This systematic review and meta-analysis was reported in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA). 26
Literature search
A search was conducted of the MEDLINE, EMBASE, and COCHRANE databases to identify original literature on patients with ITNs treated with TA. The following search terms were used: ((Indeterminate OR Bethesda III OR Bethesda IV OR Atypia of undetermined significance OR AUS OR Follicular neoplasm) AND (Thyroid) AND (Thermal ablation OR Radiofrequency ablation OR Radio-frequency ablation OR RFA OR Microwave ablation OR Microwave coagulation OR MWA)). The literature search had no set start date and was updated on May 11, 2025. Only English-language publications were included. In addition, the bibliographies of relevant articles were reviewed to find any further appropriate articles.
Inclusion criteria
Studies satisfying the following criteria were included: (1) patients with ITN(s) (Bethesda III, Bethesda IV, AUS, or follicular neoplasm) on FNA or CNB treated with any kind of TA, such as RFA or MWA; and (2) follow-up data for at least 12 months after ablation.
Exclusion criteria
Studies or subsets of studies were excluded on the basis of the following criteria: (1) letters, editorials, conference abstracts, case reports or series, systematic reviews or meta-analyses, consensus statements, guidelines, and review articles; (2) articles not directly focused on the topic of ITNs treated with TA; and (3) articles with a suspected overlap of populations.
Two radiologists, H.L. and J.H.B., with 7 and 30 years of experience in thyroid imaging, respectively, independently conducted the literature search and selection process, which included two stages: First screening (abstract review) and second screening (full-text review). In the first stage, each reviewer independently evaluated abstracts based on predefined criteria. In the second stage, full-text articles were reviewed, and the results were compared. Any discrepancies were resolved through discussion between the reviewers.
Data extraction
Data extraction was performed using standardized forms developed specifically for this study, and included the following: (1) characteristics of the articles, including author, year of publication, country of origin, study design (prospective or retrospective), duration of patient recruitment, ultrasonography (US) follow-up protocol, mean follow-up, follow-up loss, ablation method, number of patients, number of nodules, mean patient age, male-to-female ratio, diagnosis method, number of nodules categorized by Bethesda categories, detailed inclusion criteria, and baseline nodule volume; (2) details of the TA, including ablation methods, generator, electrode, applied power, mean ablation time, number of ablation sessions, type of anesthesia, and use of sedation; (3) results of ablation and follow-up details, including serial changes in the posttreatment volume reduction rate (VRR) of the index nodule (1-, 3-, 6-, 12-, 24-, 36-, 48-, and 60-month data), with VRR during follow-up calculated as ([initial nodular volume − final nodular volume] × 100)/initial nodular volume) 27 ; and (4) clinical and safety outcomes, including the number of biopsies performed post-TA, reported number of regrowths, delayed surgery, malignancy at delayed surgery, metastasis, and complications related to the ablation procedure.
Complications were assessed according to the reporting standards of the Society of Interventional Radiology. 28 Major complications were defined as adverse events that resulted in significant morbidity or disability, required intensive medical care or hospital admission, or significantly extended hospital stays. Any other complications, including unintended or undesired outcomes of the procedure that did not require therapy or medical treatment, were classified as minor complications, as described in previous studies. 29,30 Voice changes were classified as a major complication because in all studies the duration was reported as “within 6 months.” Immediate postablation events, such as parenchymal edema and tolerable mild pain or discomfort that did not require medication, were not considered to be complications.
Quality assessment
Two authors (H.L. and J.H.B.) independently conducted data extraction and quality assessment using the Risk of Bias for Nonrandomized Studies (RoBANS) tool for nonrandomized controlled trials. 31,32
Data synthesis and analyses
The primary outcome of the current systematic review and meta-analysis was the serial VRRs of ablated nodules. The secondary outcomes focused on detailing the clinical and safety outcomes, including regrowth, delayed surgery, pathologically confirmed malignancies after ablation, and complications during postablation follow-up. We estimated pooled proportions using an inverse-variance weighted approach, 33 –35 applying a random-effects model to calculate the overall proportions. The degree of heterogeneity was quantified using Higgins inconsistency index (I 2), where values above 50% were considered indicative of substantial heterogeneity. 36 Given the substantial heterogeneity observed, we conducted sensitivity analyses to identify its potential sources. If significant heterogeneity persisted after excluding outlier studies, we applied a random-effects model to account for the variability. Post hoc subgroup analysis was also performed according to the baseline nodule volume, the presence or absence of hydrodissection, the ablation method (RFA vs. MWA), and genetic alteration testing. Subgroup analysis based on baseline nodule volume was performed to assess its impact on procedural efficacy, as larger nodules are less likely to achieve complete ablation and effective volume reduction compared with smaller nodules. Subgroup analysis by hydrodissection was conducted to evaluate its potential to enhance safety and minimize complications by creating a protective margin between critical structures and the target lesion, thereby reducing unablated margins and improving ablation completeness. Subgroup analysis by ablation method was included to compare the clinical outcomes of RFA and MWA, as the two modalities differ in mechanisms of energy delivery, heat distribution, and tissue interactions, which may influence treatment efficacy and complication rates. Subgroup analysis based on molecular testing was conducted, considering its potential impact on outcomes such as regrowth and the risk of malignancy. Metaregression was used for these subgroup analyses. All statistical analyses were performed by one author (S.J.C., with 9 years of experience in conducting systematic reviews and meta-analysis), using the “meta” package in R version 4.4.1 (http://www.r-project.org/).
Results
Literature search
The article selection process is described in Figure 1. The initial search for the systematic literature review identified 235 articles (Supplementary Data). After removing 42 duplicates, 193 articles remained for screening on the basis of their titles and abstracts, resulting in 29 potentially eligible articles. Upon reviewing the full text of the 29 provisionally eligible articles (Supplementary Table S1), it was found that one was a case report, 37 six were conference abstracts, 38 –43 three were review articles, 44 –46 one potentially involved overlapping data, 47 and three were not relevant to the field of interest. 48 –50 Ultimately, 15 articles were included in this study.
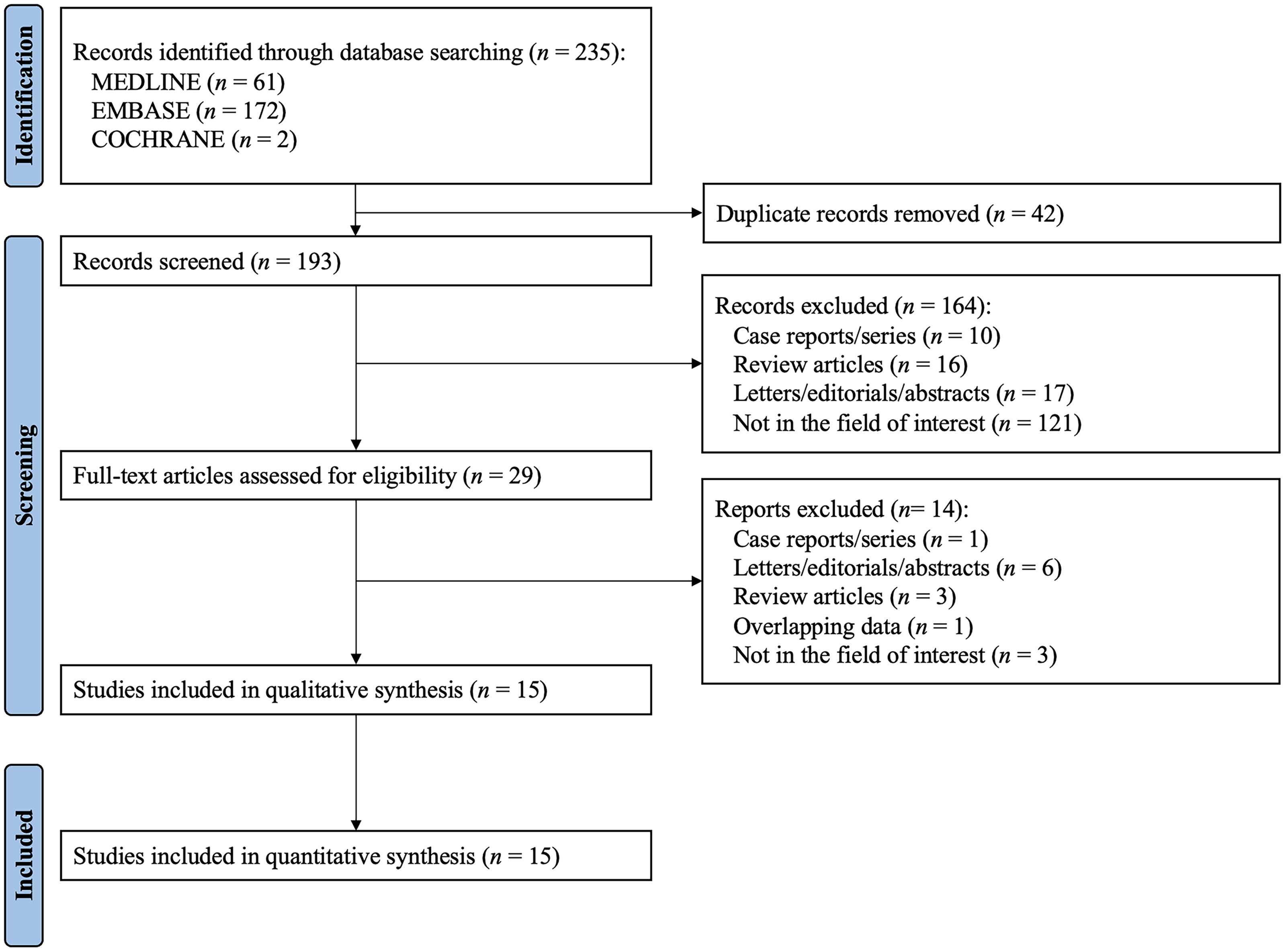
Flow diagram of the study selection process.
Characteristics of the included studies
Table 1 details the characteristics of the 15 included studies. 51 –65 A total of 1015 patients were enrolled, with 1149 nodules undergoing TA. The study populations ranged in size from 6 to 375 patients, with an average patient age between 38 and 63 years. The overall male-to-female ratio was 651–364. The mean baseline nodule volume varied between 0.6 and 17.9 mL. The US follow-up protocol varied from simple checkups at 6 and 12 months to comprehensive follow-up spanning 1, 12, 24, 36, 48, and up to 60 months after TA. The studies predominately originated from China, the United States, and Italy, with additional contributions from Taiwan and Korea. Among the 15 studies, 11 were retrospective in design 51,52,55,57 –60,62 –65 and four were prospective. 53,54,56,61 All studies confirmed the Bethesda III or IV classification of nodules through pathology, using various biopsy methods, including two FNAs, two CNBs, or at least one FNA or CNB. The total number of nodules reported was 745 for Bethesda Category III and 345 for Bethesda Category IV. In addition, 59 nodules were classified as either Bethesda Category III or IV but were not individually distinguished.
Characteristics of the Included Studies
The numbers in parentheses represent the number of nodules corresponding to each grade.
This study presents the cytopathologic results based on the British and Italian reporting systems for thyroid cytopathology. All the included nodules in this study are classified as Thy3, corresponding to Bethesda Categories III and IV.
Only BRAF- and NRAS-negative nodules were included.
Using the AllPrep DNA/RNA Micro Kit (Qiagen), genetic alterations, including BRAFV600E , TERT, and RET/PTC1 (RET/CCDC6), were investigated. Only mutation-negative nodules were included.
Two molecular platforms—Afirma (GEC and GSC) and ThyGenX/ThyraMIR—were used for cytological analysis, but the study did not specify whether only mutation-negative nodules were included.
Standard deviation was estimated using either the interquartile range (SD ≈ IQR/1.35, assuming a normal distribution) or the range rule of thumb (SD ≈ [maximum − minimum]/4).
Molecular tests (Afirma® or ThyroSeq® v3) were used to confirm benignity before ablation. Only mutation-negative nodules were included.
The standard deviation was not reported.
The total number of nodules was not reported; however, 103 single and 58 multiple nodules were documented. For the purpose of analysis, the total number was assumed to be 161.
Molecular testing was conducted using an eight-gene panel, including BRAF, KRAS, NRAS, HRAS, TERT, RET, PAX8, and NTRK3, to identify point mutations and gene fusions such as BRAFV600E , TERT C228T/C250T, and RET/PTC or PAX8-PPARγ fusions. Only mutation-negative nodules were included.
Preablation BRAFV600E PCR testing was performed, and 29.5% of patients were found to be mutation-positive.
FNA, fine-needle aspiration; CNB, core needle biopsy; M, month; MWA, microwave ablation; NA, not available; No., number; Pro., prospective; Retro., retrospective; RFA, radiofrequency ablation; TI-RADS, Thyroid Imaging Reporting and Data System; US, ultrasonography.
Characteristics of the ablation methods
Table 2 summarizes the technical specifications of the ablation procedures, including the generator type, electrode characteristics (gauge, tip length, and cooling mechanism), power settings, number of sessions performed, anesthesia type, and sedation use. The electrode gauge used was 18G for RFA and 16G to 17G for MWA. The applied power ranged from 3 to 60 W for RFA (15–60 W for monopolar electrodes and from 3W for bipolar electrodes), and from 25 to 35 W for MWA. The majority of the included studies (9 out of 15) used RFA for TA. 51 –57,59,61 Three studies used either RFA or MWA, 58,60,64 while the remaining three studies used MWA. 62,63,65 The mean ablation times ranged from 161 to 876 seconds. Most studies conducted a single session, although some reported 1–2 sessions. Most studies used local anesthesia, and only one study reported the use of sedation (midazolam). 52
Characteristic of the Ablation Methods
C., cooled; MDZ, midazolam; s, second; UC., uncooled; W, watt.
Volume reduction rate after ablation
Table 3 displays the mean VRRs for the ablated nodules during the follow-up period, as well as the pooled proportions derived from the meta-analysis. The pooled VRRs at 1, 3, 6, 12, 24, 36, 48, and 60 months were 15.9% (confidence interval [CI]: −10.3–42.1%), 50.0% (CI: 40.1–59.8%), 68.0% (CI: 63.6–72.3%), 81.0% (CI: 76.0–85.9%), 85.1% (CI: 73.5–96.7%), 90.6% (CI: 73.2–108.0%), 93.8% (CI: 81.3–106.2%), and 93.0% (CI: 78.9–107.1%), respectively, based on 701, 653, 785, 769, 256, 77, 43, and 47 nodules (Fig. 2). Supplementary Figure S1 shows the trends of the pooled VRRs for nodules treated with TA. The pooled VRR progressively increased, showing a significant reduction in volume within 12 months, with a gradual increase thereafter, plateauing around 48 months. Substantial heterogeneity persisted across all time periods: 1 month (I 2 = 99.8%, p = 0), 3 months (I 2 = 99.1%, p < 0.01), 6 months (I 2 = 93.5%, p < 0.01), 12 months (I 2 = 93.9%, p < 0.01), 24 months (I 2 = 99.5%, p < 0.01), 36 months (I 2 = 96.3%, p < 0.01), 48 months (I 2 = 89.6%, p < 0.01), and 60 months (I 2 = 89.7%, p < 0.01).
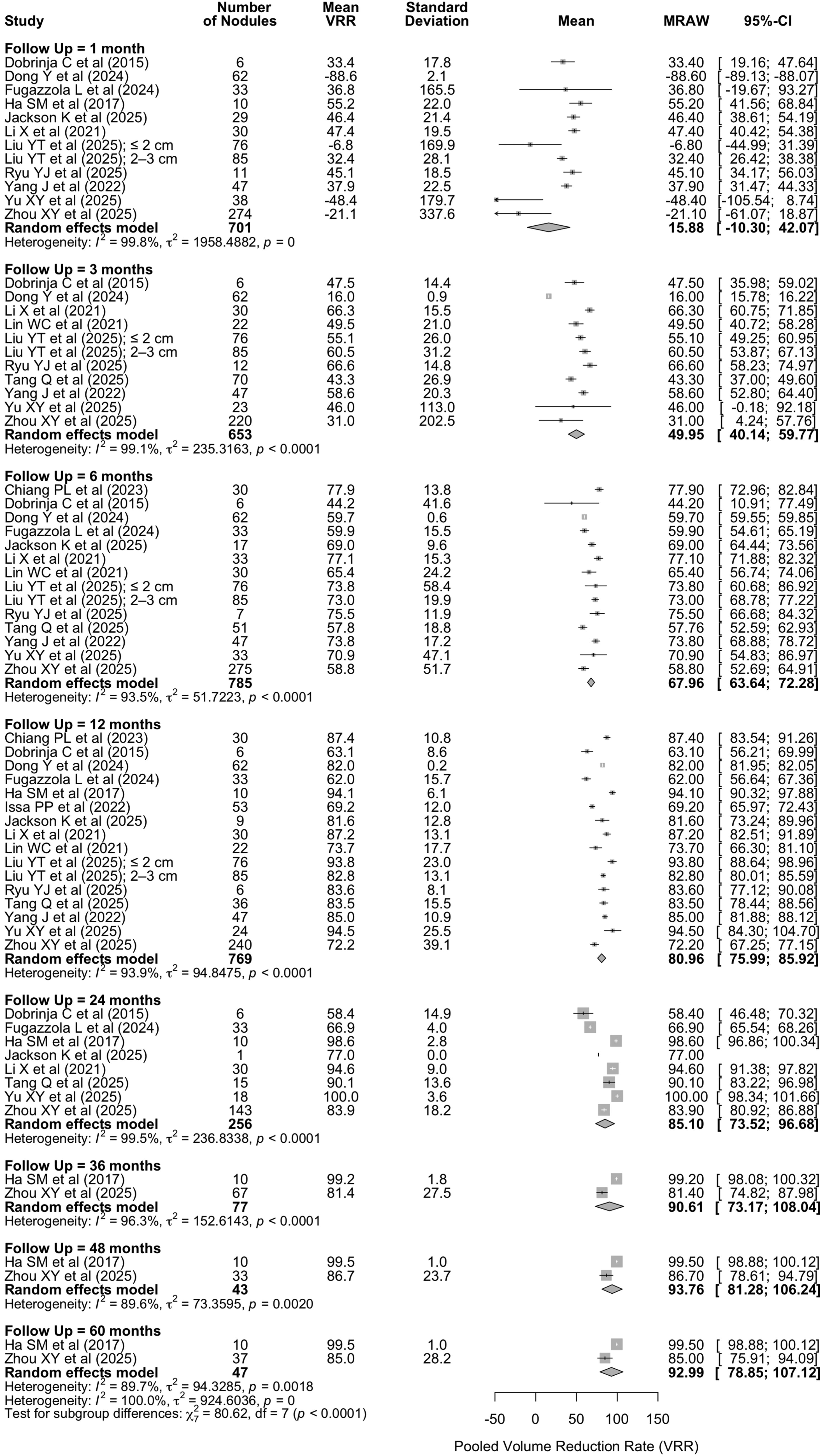
Forest plots of pooled volume reduction rates at 1, 3, 6, 12, 24, 36, 48, and 60 months of follow-up.
Ablation Results (Volume Reduction Rate)
The data were estimated using figure.
Standard deviation was estimated using either the interquartile range (SD ≈ IQR/1.35, assuming a normal distribution) or the range rule of thumb (SD ≈ [maximum − minimum]/4).
While only the overall mean was reported for the entire cohort, serial mean VRRs and standard deviations were separately provided for two subgroups based on baseline nodule volume (≤2 cm and 2–3 cm), and these were used for data pooling.
CI, confidence interval; VRR, volume reduction rate.
Clinical and safety outcomes
Table 4 presents the details of clinical outcomes and complications following the procedures. Of the 15 included studies, three performed post-TA biopsies according to their own protocols. Of these three studies, one conducted biopsies on nodules larger than 1 cm at the 6-month post-RFA follow-up, one performed biopsies on all nodules, and the protocol for the third study was unspecified. A total of 35 biopsies were performed after TA, with no malignancy being detected in the postablation biopsy groups. There were 26 cases of regrowth, among which four patients underwent delayed surgery. Malignancy was confirmed in three of them: one had a follicular neoplasm of indeterminate malignant behavior (baseline volume: 24.5 mL) with regrowth at 24 months; another had a minimally invasive follicular carcinoma (baseline volume: 39.5 mL) with regrowth at 6 months; and the third had metastatic disease from a rare urethral cell carcinoma with regrowth at 36 months accompanied by PET avidity. The remaining patient underwent thyroidectomy due to anxiety, with no malignancy confirmed. No cases of cervical or distant metastasis were reported.
Clinical and Safety Outcomes
For eight nodules larger than 1 cm at the 6-month post-RFA follow-up, post-RFA FNA was performed to rule out malignancy.
All cases resolved within 3 months without any treatment.
A minimal isthmic rupture occurred 1-month post-RFA. The patient was closely monitored at the outpatient department and treated with only oral medication, ultimately recovering.
During postthermal ablation follow-up, an increase in VRR compared with prior VRR is defined as regrowth. In one case, regrowth was observed at the 6-month follow-up, while in the other case, it was noted at the 24-month follow-up.
After surgery, one (regrowth at 6-month follow-up) was a minimally invasive follicular carcinoma (baseline volume: 39.5 mL), and the other (regrowth at 24-month follow-up) was a follicular neoplasm of indeterminate malignant behavior (baseline volume: 24.5 mL).
For five patients, 6–12 months after RFA, the FNA results were Bethesda III.
Regrowth is defined as an increase in volume assessed by ultrasound, where the postoperative volume is greater than the preoperative volume. Of the nodules that regrew, the majority (42.1%) did so within the first month.
In Jackson K et al. (2025), 57 reported complications included skin burn, fever, and transient hyperthyroidism. Yu XY et al. (2025) 63 reported dysphagia. Zhou XY et al. (2025) 64 noted cough, back pain, and hypothyroidism.
All 22 patients underwent postablation fine needle aspiration within 6–12 months, with each cytology result consistent with Bethesda category I.
In this study, two residual tumors were identified and considered to result from regrowth of residual thyroid tissue within the ablation zone.
All cases resolved within 6 months without any treatment.
One case of regrowth at 36 months was later diagnosed as metastatic urethral cell carcinoma following thyroidectomy.
Number of cases of local recurrence.
Among the two patients with local recurrence, one underwent thyroidectomy due to anxiety, and the other continued regular follow-up.
FNwIMB, follicular neoplasm of indeterminate malignant behavior; MIFTC, minimally invasive follicular carcinoma.
Major complications were reported in 21 out of 1149 cases (1.8%). 51,56,57,59,60,63,64 Voice changes were the most common complication, with 20 cases reported. 51,56,57,59,60,63,64 All of them resolved within 6 months without any treatment. Nodule rupture occurred in one case and was treated with only oral medication at the outpatient department, with the patient ultimately recovering. 51 Eight cases (0.7%) of minor complications were reported, including skin burn, fever, transient hyperthyroidism, hypoparathyroidism, dysphagia, and back pain.
Subgroup analysis
Subgroup analysis was conducted post hoc to evaluate the impact of hydrodissection, the baseline nodule volume, ablation method, and genetic alteration testing (Supplementary Figs. S2–S7). A significant difference was noted in the pooled VRR according to the presence 51,53,58,60,61,63 –65 or absence 52,54 –57,59,62 of hydrodissection at 6 months (p = 0.03), and the gap progressively increased throughout the 24-month follow-up period, as shown in Figure 3. Table 5 shows the subgroup analysis based on baseline nodule volume. Using a cutoff volume of 10 mL, VRR showed a significant difference at 12 and 24 months (p < 0.05). However, no significant difference in pooled VRR was observed between ablation methods (RFA vs. MWA) over the 24-month follow-up. Similarly, there was no significant difference between the molecularly tested and untested groups.
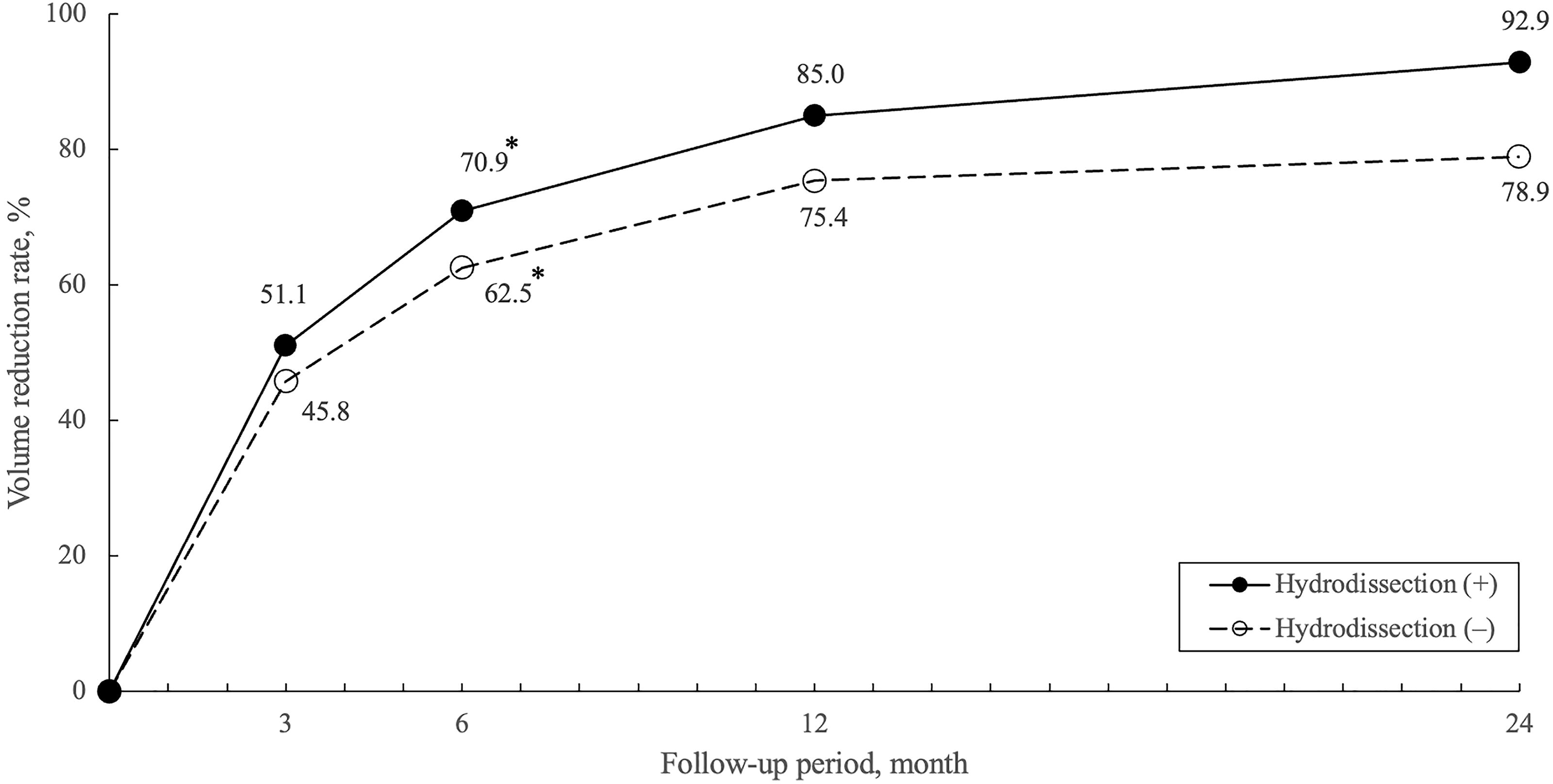
Trends in pooled volume reduction rates based on the presence or absence of hydrodissection. A significant difference in pooled VRR was observed at 6 months (70.9% with hydrodissection vs. 62.5% without hydrodissection, p = 0.03). VRR, volume reduction rate.
Subgroup Analysis Based on Baseline Nodule Volume
Indicates a statistically significant difference.
CI, confidence interval; No, number.
Sensitivity analysis
Sensitivity analysis was performed by sequentially excluding each study and reanalyzing the remaining data (Supplementary Fig. S8). No single study had an undue influence on the overall meta-analysis results.
Publication bias
The funnel plot (Supplementary Fig. S9) shows a generally symmetrical distribution, with a few studies outside the pseudo 95% confidence limits. Egger’s test showed no significant asymmetry (p = 0.76), suggesting no evidence of publication bias.
Quality assessment of the studies
The quality of the 15 included studies was assessed using the RoBANS tool. As detailed in Figure 4, all studies showed a low risk of bias in areas such as selective reporting, outcome evaluation, and measurement exposure. However, there were concerns in five areas. Eight studies had a high risk of bias in participant comparability because of inadequate baseline characteristics. 51,53 –55,59,62,64 All studies showed a high risk in the selection of participants, either because the outcome was unconfirmed at the time of enrollment or because recruitment strategies did not reflect the intended target population. Eleven studies demonstrated a high risk related to confounding variables, as they lacked appropriate identification or control of confounders. 51 –53,55,56,58 –60,63 –65 In terms of blinding, all studies showed high risk due to the absence of outcome assessor blinding or uncertainty regarding whether blinding was maintained. In addition, seven studies were found to have follow-up losses, leading to a high risk of bias in the incomplete outcome data. 57,58,61 –65
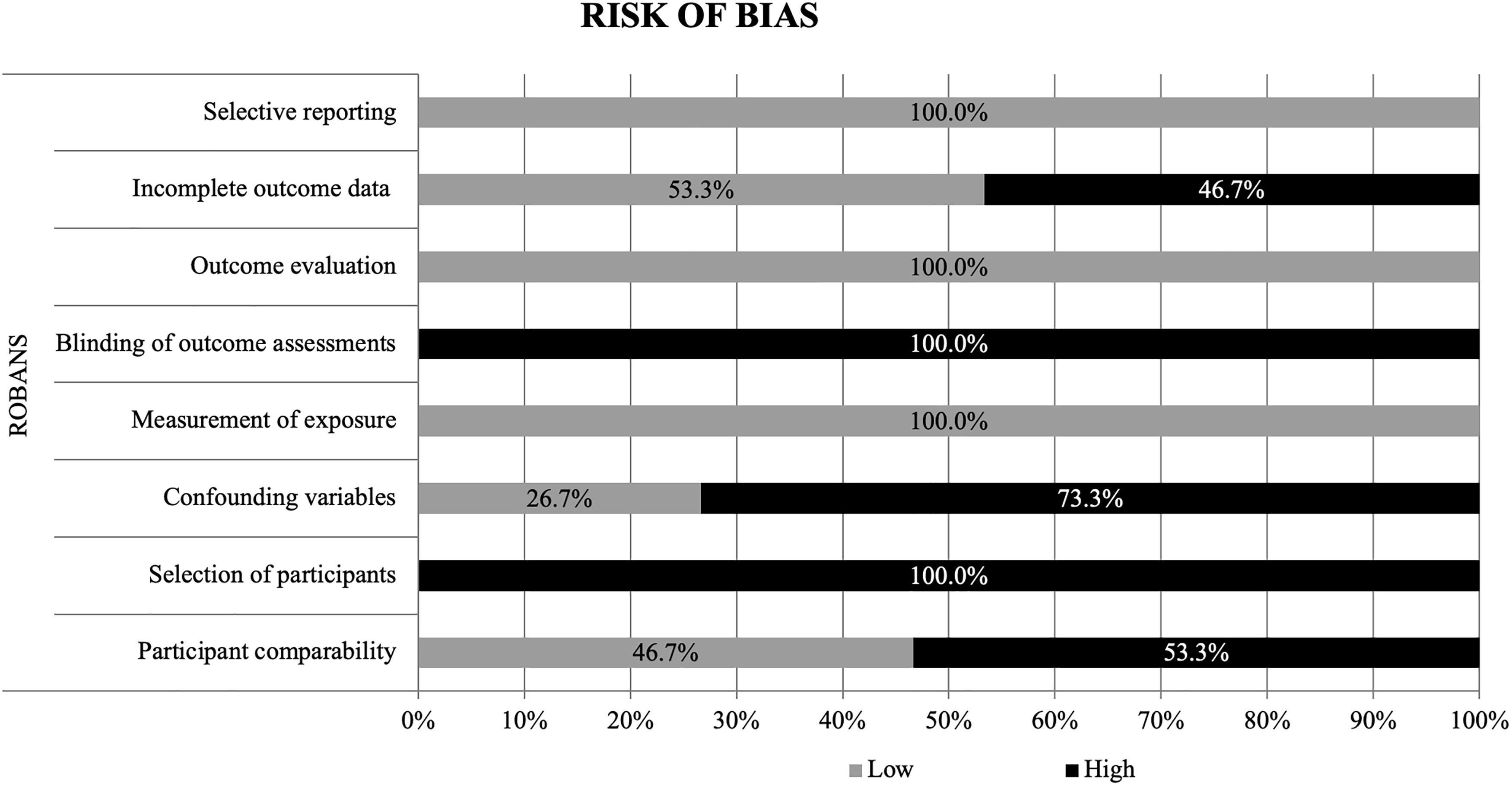
Quality assessment of the included studies according to the Risk of Bias for Nonrandomized Studies (RoBANS) assessment tool.
Discussion
Our study suggests that TA may be an effective and safe treatment for ITNs, with a sustained decrease in nodule volume observed during the 60-month follow-up. The 6-month pooled VRR with hydrodissection is significantly higher than that without hydrodissection. Although the incidence of regrowth (2.3%) and delayed surgery (0.3%) was very low, three cases that underwent delayed surgery were confirmed to be malignant, raising concerns, although no metastasis occurred. In addition, the overall major complication rate was 1.8%, ranging from 1.2% to 12.5%.
According to the Bethesda system, the indeterminate categories of Bethesda III and IV carry a malignancy risk of 13–30% and 23–34%, respectively. 4 In this study, the postablation pathologically confirmed malignancy rate was 0.3%. Although this represents a significant reduction compared with the preablation risk, there remains a residual malignancy risk, which poses a concern. This is why current guidelines recommend surgery as the first-line treatment for ITNs (AACE/ACE/AME, ETA), with RFA not being recommended (ATA, KSThR). 24,25,66,67 Nevertheless, TA offers several advantages over surgery. First, the rate of malignancy after TA treatment of ITNs is low. However, given that most included studies, except for two, had relatively short follow-up periods (12–24 months), there remains a possibility of additional cases of regrowth, malignancy, and even distant metastasis over time. Although the malignancy risk can be reduced with complete ablation, the residual risk still necessitates careful follow-up, similar to the approach used for active surveillance or RFA of PTMC. 13,68,69 In this study, three cases confirmed as malignancy after surgery were associated with regrowth, indicating that regrowth during follow-up should raise suspicion for malignancy and warrants consideration of surgery. In addition, compared with surgery, TA has a lower complication rate, shorter procedure time, and lower invasiveness. 65,70 For patients who are poor surgical candidates, elderly, or who refuse surgery, TA offers a minimally invasive alternative.
TA is highly effective for reducing nodule volume, with the pooled VRR continuing to increase up to 48 months, before reaching a plateau. However, considering the malignancy risk associated with Bethesda III and IV nodules, the treatment goal should not be merely volume reduction, but complete ablation to eliminate the risk of malignancy. In this study, the group that underwent hydrodissection showed a significantly higher pooled VRR at 6 months than the group without hydrodissection, suggesting that hydrodissection may increase the likelihood of complete ablation. Moreover, to minimize marginal regrowth, the guidelines propose vascular ablation techniques. 71 –73 These techniques lead to more efficient and complete ablation. 72 In the subgroup analysis based on baseline nodule volume, setting higher thresholds for dividing the groups led to more significant differences in pooled VRR. Specifically, a statistically significant difference was observed at 12 and 24 months for nodules dichotomized with a 10 mL threshold, indicating that larger nodules have a higher likelihood of regrowth. Of the three cases confirmed as malignancy following surgery for regrowth after TA, two involved large nodules (>24 mL), while the remaining case did not report the nodule volume. A recent study by Ahn et al. found that large nodule size (≥3 cm) independently increased the malignancy risk in Bethesda Category III nodules categorized as low or intermediate suspicion on ultrasound. 74 In light of this, selecting only nodules of a manageable size for which complete ablation is achievable, and applying advanced techniques such as hydrodissection and vascular ablation, which are commonly used in RFA of benign thyroid nodules, could potentially improve treatment success rates for ITNs.
Although this study found no significant difference in pooled VRR between molecularly tested and untested groups, the high negative predictive value (>94%) of molecular tests suggests that genetic analysis may become a crucial step in deciding between TA and surgery for the treatment of ITNs, provided the cost is acceptable. 75 –77 In addition, a study focusing on ITNs with low SUV (SUV max <5) on PET/CT reported no malignancy among all the ablated nodules confirmed by biopsy. 59 In light of this, incorporating advanced diagnostic tools, such as molecular analysis and radioisotope imaging, into pretreatment evaluations could help identify nodules with a low likelihood of malignancy, thereby optimizing treatment decisions and improving patient outcomes. Ideally, ITNs with negative molecular profiles and low FDG uptake represent optimal candidates for TA.
The occurrence rate of major complications was low at 1.8%. All cases of transient vocal cord palsy fully recovered within 6 months without any specific treatment, and the one case of nodule rupture was resolved with oral medication. These findings confirm that TA is a safe method for treating ITNs.
This study has several limitations. First, 13 of the 15 studies had a short follow-up period of 12 to 24 months. This limited follow-up period may lead to underestimation, as malignancies that have not yet been detected could still emerge. To derive more definite conclusions about the safety and efficacy of TA, studies with long-term follow-up are crucial. Such studies could provide more reliable insights into delayed outcomes and better inform clinical decision-making. Second, post-TA biopsies were performed on only 3.0% of the nodules, and distant metastasis after TA was evaluated exclusively through US. This raises the possibility of undetected malignancies, potentially leading to an underestimation of the true malignancy rate. Third, since most of the included studies were retrospective, there is a risk of bias. Fourth, heterogeneity was present among the included studies. Fifth, in 10 of the 15 studies, the sample size was relatively small, with fewer than 50 patients. Last, our study lacks prior registration in a repository such as PROSPERO. Although a review of the PROSPERO database confirmed that no similar studies were registered at the time of our analysis, the absence of formal protocol registration limits the ability to fully ensure reproducibility and accountability.
In conclusion, TA may be considered a safe and effective treatment option for patients with ITNs who are not candidates for or decline surgery. However, caution is advised, and a thorough follow-up is essential due to the relatively short follow-up periods in most of the included studies. Larger nodules have a risk of incomplete ablation, and it is therefore important to selectively perform TA on nodules with a high likelihood of achieving complete ablation, using advanced techniques such as hydrodissection and vascular ablation, to ensure complete ablation. Limitations, including short follow-up periods, small study sizes, and study heterogeneity, emphasize the need for further research. Long-term prospective studies and randomized clinical trials are essential to better establish the reliability and clinical utility of TA.
Footnotes
Authors’ Contributions
H.L.: Conceptualization, formal analysis, investigation (lead), methodology, writing—original draft (lead), and writing—review and editing. S.J.C.: Conceptualization, formal analysis (lead), investigation, methodology (lead), supervision, and writing—review and editing (lead). Y.J.: Formal analysis, investigation, and methodology. S.Y.J.: Formal analysis, investigation, and methodology. J.H.B.: Conceptualization (lead), formal analysis, investigation, methodology, supervision (lead), and writing—review and editing.
Author Disclosure Statement
J.H.B. has been a consultant for two radiofrequency companies since 2017, STARmed and RF Medical.
Funding Information
This research received no external funding.
Supplementary Material
Supplementary Data
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.