
Abstract
Background:
Anaplastic thyroid cancer (ATC) is an aggressive cancer that leads to rapid death if left untreated. However, recent advances in ATC treatment have dramatically changed the prognosis in a select group of patients with BRAFV600E mutations. In these patients, BRAF/MEK inhibitors have been shown to dramatically and rapidly shrink tumors. Yet, these responses are short-lived unless additional treatment modalities are applied. In patients without a BRAFV600E mutation, the current available therapies are far less effective.
Summary:
In this article, we review the relevant literature and propose applying the “Total Therapy” approach used since the 1960s for another deadly but curable disease, acute lymphocytic leukemia, to ATC. We have adapted the concepts of Induction, Consolidation, and Maintenance, applying them to ATC. This regimen integrates the treatments we have found to be successful in ATC: combination systemic therapy using targeted therapy plus immunotherapy, surgery, radiation, and continuation of the systemic therapy for several years, thereby attempting to eradicate all residual ATC cells.
Conclusions:
There has been a renewed interest in understanding the genomics of ATC and treating these patients with urgency rather than just providing palliative care. This shift has led to significant improvements in the prognosis of ATC. With the right tools and a clear roadmap to guide us, we now aim to take on the challenge of curing these patients.
Introduction
Anaplastic thyroid cancer (ATC) is one of the most virulent cancers in humans with a historical survival measured in months, but it is a rare disease. Due to the rapid doubling time of the tumor cells (roughly 1–4 days), 1 the threat of airway compression resulting in asphyxiation, and resistance to cytotoxic chemotherapy, ATC has been extremely challenging to treat. In addition, at the time of diagnosis, most tumors are unresectable, half of the patients already have distant metastatic disease, and patients are usually older and have multiple comorbidities. 2 Patients without radiographically apparent metastatic disease at diagnosis often have micrometastatic disease, becoming apparent within the year. 3 Consequently, physicians historically shifted their efforts to palliative care, emphasizing symptom management and quality of life, rather than pursuing a cure. However, recent groundbreaking advances by multidisciplinary teams 4 at academic centers have yielded unprecedented overall survival rates, 5 transforming the once-unimaginable prospect of curing ATC into a tangible possibility.
In many ways, ATC is reminiscent of acute lymphocytic leukemia (ALL) before the late 1960s. In both cases, physicians have historically faced criticism for daring to attempt to cure such aggressive diseases. Similar to ALL, oncogenic drivers play a crucial role in managing ATC. In the case of ATC, BRAFV600E mutations (40%) and oncogenic fusions (∼6%) are targetable alterations. RAS mutations in ATC (25%) are not yet actionable but could be in the future. Like acute leukemias, ATCs demonstrate significant intratumoral heterogeneity, with multiple tumor subpopulations, fostering an environment conducive to the development of treatment resistance. 6 ATC cells can also evade immune surveillance. Consequently, a multi-step treatment approach involving various therapies is required to target the predominant cancer cells, resistant clones, and immune system clearance. It has become increasingly clear that no single treatment or modality will cure ATC, and that multi-step therapy with different modalities such as is used in ALL should be incorporated into the way forward. This type of approach is not typical for solid tumors, and may never be accepted by regulatory agencies, but could be integrated into treatment guidelines.
Early Discoveries in Cancer Therapeutics
The roadmap for a cure for ATC that is outlined in this article is not novel. It is based on the work of many pioneers of cancer therapeutics. Prior to the late 1940s, physicians were largely reluctant to treat patients with cancer, often permitting them to succumb to the disease without intervention. Those few who did administer therapies, such as nitrogen mustard, frequently observed that remissions were transient. In the late 1940s, Sydney Farber identified folate analogs and initiated treatment protocols for pediatric patients diagnosed with ALL, employing these agents in a sequential manner rather than in combination. In the 1960s, Frei and Freireich, at the National Cancer Institute, recognized that monotherapy and sequential chemotherapy regimens led to the rapid development of drug resistance. Consequently, they implemented combination chemotherapy strategies involving three to four agents for the treatment of childhood ALL. They repeated these chemotherapy cycles, which ultimately resulted in the successful cure of pediatric ALL cases. Freireich was undeterred by the fact that such intensive treatment protocols resulted in significant bone marrow suppression, leading to critically low levels of platelets, erythrocytes, and leukocytes. He innovatively developed methods for administering platelet transfusions and empirical antibiotic therapy to manage neutropenic fever, facilitating patient recovery and successful treatment outcomes. 7
Numerous researchers adopted the therapeutic framework established by Frei and Freireich, resulting in successful treatment outcomes for Hodgkin lymphoma, as evidenced by the work of Vincent DeVita, and testicular cancer, as demonstrated by Lawrence Einhorn. 7 Don Pinkel, at St. Jude Children’s Research Hospital, formulated a comprehensive treatment strategy for leukemia termed “Total Therapy,” which encompasses remission Induction, Consolidation, Continuation (currently referred to as “Maintenance”), and central nervous system prophylaxis. 8 Over five decades later, these foundational principles remain integral to the treatment of ALL.
Integrating Total Therapy for BRAF-Mutated ATC
BRAFV600E-mutated ATC serves as the foundational model upon which all other treatment strategies are based. The model is similar to the principles of management of acute leukemia: Induction, Consolidation, and Maintenance Therapy, modified for ATC and shown in Figure 1. This approach has been the standard of care at our institution 9 for patients with BRAFV600E-mutated ATC with locoregional disease (stage IVB) that is not meaningfully resectable and for patients with widely metastatic disease (stage IVC). A prospective clinical trial in which patients were treated accordingly was recently published. 10 Another clinical trial has now completed accrual and results will be published in the coming year (NCT04675710). 58 It should be noted that patients with localized disease that is meaningfully resectable, should undergo upfront surgical resection followed by chemoradiation per the American Thyroid Association (ATA) and National Comprehensive Cancer Network (NCCN) guidelines. 2,11
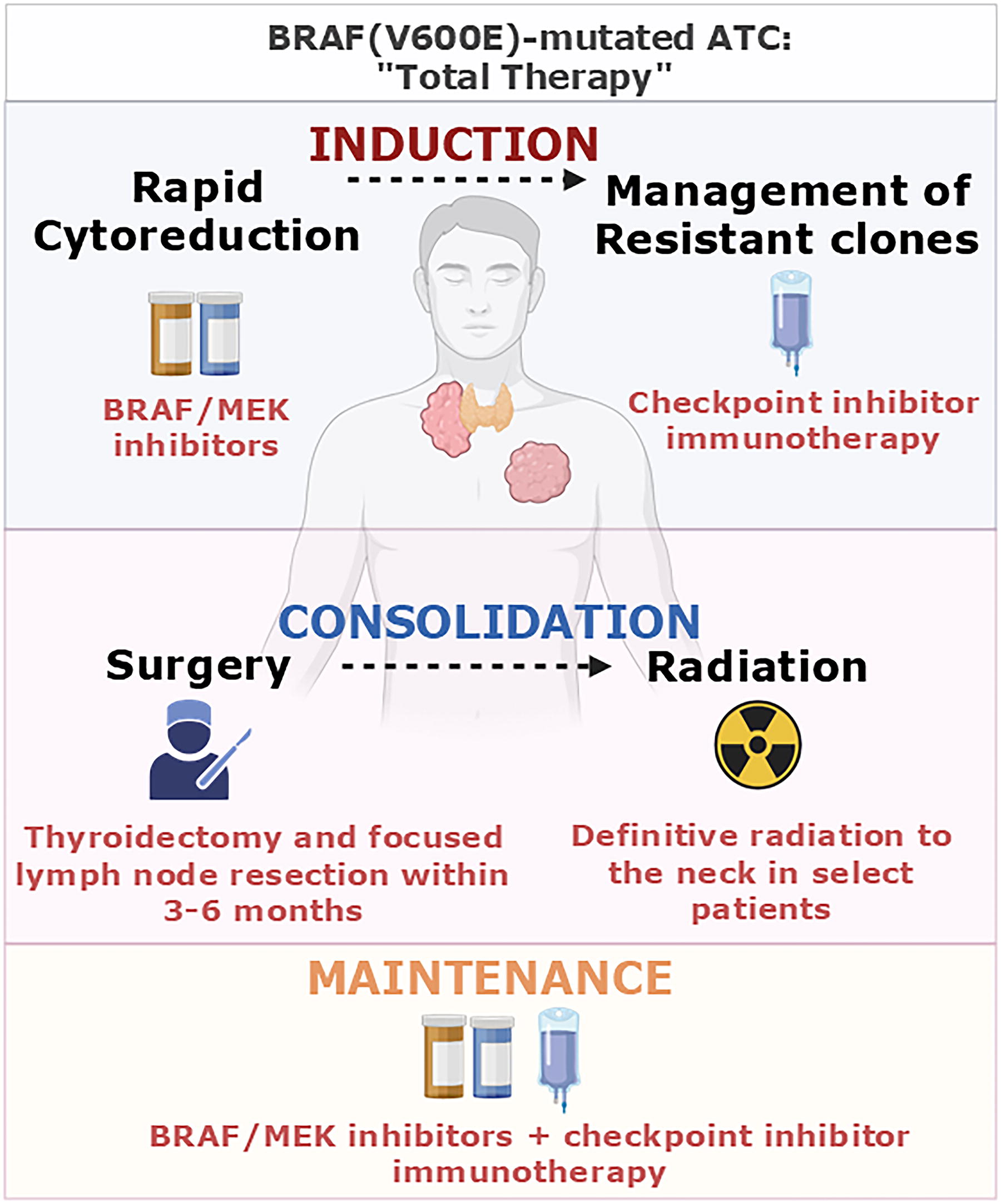
“Total Therapy,” as reimagined for anaplastic thyroid cancer (ATC), includes the same steps as those used in acute lymphocytic leukemia (ALL) but with different modalities. In BRAF-mutated ATC, this includes Induction Therapy with BRAF-directed therapy, followed by checkpoint inhibitors to deter the emergence of resistance. Consolidation is the next step once a response is achieved, which allows for the surgical removal of the primary tumor. This surgery is generally performed within 3–6 months of Induction Therapy. In select patients, those with localized disease (stage IVB) or low-volume distant metastatic disease (stage IVC), definitive radiation to the neck and high-risk distant sites is then considered. Maintenance Therapy soon follows with the resumption of BRAF-directed therapy plus checkpoint inhibitor. Created in BioRender. Cabanillas, M. (2025) https://BioRender.com/t78v677.
Induction therapy (“DTP”)
Rapid cytoreduction, particularly of the primary tumor, is necessary in patients with ATC, due to the threat of rapid compression of the airway. At the time of diagnosis, almost all patients are symptomatic, presenting with dyspnea, dysphagia, hoarseness, and/or neck pain that often radiates to the ear. In BRAF-mutated ATC, which comprises 40% of ATCs, 12,13 BRAF/MEK inhibitors result in rapid tumor shrinkage and subsequent relief of symptoms in the vast majority of these patients. Consequently, the BRAF status of the patient must be rapidly determined by immunohistochemistry, 14,15 single-gene PCR, or liquid biopsy 16,17 as soon as ATC is suspected. The BRAF/MEK inhibitor combination, dabrafenib/trametinib (DT), was FDA approved in 2018 in the United States, based on a phase 2 trial showing response rates of over 55% and a median overall survival (OS) of 14.5 months. 18,19 In this trial, 56% had a RECIST measurable response, 31% had stable disease (all with regression), and only 11% of the evaluable patients had progression as their best response. Thus, in patients with localized disease (M0) where an R0 surgery is unlikely, as well as patients with disseminated disease (M1), upfront DT should be initiated promptly. Unfortunately, while responses are impressive—almost miraculous—they are short-lived, with a median progression-free survival (PFS) of only 6 months. Analogous to most tumors, selective pressure on a single molecular pathway leads to the emergence of resistance in thyroid cancer with new mutations such as RAS and PIK3CA and the development of an immunosuppressive tumor microenvironment. This phenomenon requires proactive anticipation and strategic treatment planning. Thus, Induction Therapy is a two-step treatment that targets the subclones and resistant tumor cells. Once rapid cytoreduction has been achieved to alleviate existing or impending compressive symptoms, an immune checkpoint inhibitor targeting the PD-1/PD-L1 pathway should be started within 4 weeks to attempt to deter resistance. Both the ATC cells and the tumor immune microenvironment express PD-L1 in the majority of these tumors. Furthermore, single-agent anti-PD-1 checkpoint inhibition has shown some efficacy in ATC with an overall response rate of 19% and a median overall survival of 5.9 months. 20 Currently, the most studied combination is the addition of pembrolizumab to DT, a regimen coined “DTP”. 9,21,22 The DTP regimen significantly improved the median OS (17 months with DTP vs. 9 months with DT, p = 0.037) and median PFS (11 months with DTP vs. 4 months with DT, p = 0.049) compared with using dabrafenib and trametinib alone. 22 It should be noted that these patients were treated only with systemic therapy (“Induction Therapy”) without surgical consolidation, discussed below. We also emphasize that these data are retrospective, as prospective, randomized trials have not been realized at this time. While adding pembrolizumab at the time of progression has shown effectiveness, there is a concern that progression might be detected too late, potentially after symptom onset. Furthermore, not all patients exhibit a significant response to DT alone. 23 Consequently, our approach is to add immunotherapy within the first month of treatment, improving the probability of responding to the systemic therapies. 24
Consolidation therapy (surgery ± radiation)
Unlike in acute leukemia, Induction Therapy for BRAF-mutated ATC rarely achieves complete remission. Moreover, molecular characterization studies suggest that remaining thyroid tissues can harbor tumor cellular populations (i.e., papillary thyroid cancer) that can serve as a reservoir for additional ATC tumor populations to emerge. 6,25,26 Therefore, the next step in ATC management is to consolidate a good response with surgery and/or radiation therapy (RT). Our retrospective data shows that using neoadjuvant BRAF-directed therapy followed by surgical resection of the primary tumor has the best outcomes (median OS not reached, confidence interval [CI] 39.2–NA) compared with upfront surgery followed by BRAF-directed therapy (median OS 48.1 months, CI 7.1–NA) or only BRAF-directed therapy without surgery (median OS 11.4 months, CI, 6.7–17.6 months). 27 A subsequent study showed that patients treated with neoadjuvant DT (with or without pembrolizumab) had a median OS of 63 months (CI 15.5–110.5). 22
In our practice, restaging is performed at intervals not exceeding 3 months and surgical removal of the primary tumor is considered if the tumor is deemed resectable. 9 Ideally, surgery should occur following 3–6 months of Induction Therapy. Our observations support this as the optimal window in order to take advantage of cytoreduction while preventing progression, thereby returning to a state of unresectability. Trametinib, due to some anti-angiogenic activity, should be held 5 days prior to surgery. Dabrafenib does not require a drug hold prior to surgery. The drug hold for dabrafenib may begin the day of surgery. Dabrafenib may be resumed 1 day after surgery and trametinib may be resumed about 5–7 days after surgery if adequate healing has occurred. 9 Delays in resuming drug could lead to progressive disease. This neoadjuvant strategy using upfront DTP followed by surgery has been associated with the longest overall survival in BRAFV600E-mutated ATC. 27 Interestingly, the surgical pathology is predictive of outcomes, as those with a complete ATC pathological response have a significantly better OS than those who continue to have some ATC in the surgical specimen. 27 This may be due to the persistence of resistant clones and could help guide the intensity of aggressiveness of adjuvant therapy.
Patients presenting with only localized disease (M0) should then undergo postoperative RT to the neck with concurrent radiosensitizing chemotherapy, if the performance status of the patient permits. In patients with minimal distant metastatic disease, definitive-intent dose RT to the neck may be considered on a case-by-case basis, as well as stereotactic ablative RT (SBRT) to distant sites at risk of subsequent progression. This is due to the fact that DT is currently held during RT, placing the patient at risk of disease progression during the typical 6–7 week RT course. Studies are ongoing to determine the safety of concurrent DT with RT (NCT03975231 and NCT04675710). Should these trials demonstrate favorable safety profiles, patients with unresectable disease could be considered for combined DT and RT.
Maintenance therapy (“DTP”)
Following Consolidation Therapy, patients should undergo an extended period of Maintenance Therapy with DTP. In patients with metastatic disease or localized disease with persistent disease, DT should be continued indefinitely, while in patients without evidence of disease after Induction and Consolidation, the optimal duration of DT therapy is unknown. Although DT is currently continued indefinitely, discontinuation could be considered in the future in a selected group of patients with exceptional pathologic and clinical responses lasting at least 3–5 years. Currently, the recommendation is to administer pembrolizumab for a minimum of 1 year 9 and then discontinue after 2 years. This prolonged treatment strategy applies maximal pressure on the disease, targeting and eradicating potentially undetectable residual ATC cells. Maintenance Therapy helps eliminate these residual cells. The optimal duration of Maintenance Therapy remains unclear, as there is currently no validated biomarker of residual ATC. This knowledge gap underscores the importance of continued research to develop reliable markers of disease status.
The Current Strategy for Integrating Total Therapy for Non-BRAF-Mutated ATC
Unfortunately, only 40% of patients with ATC’s tumors harbor a BRAFV600E mutation. The only other oncogenes that are potentially targetable at this time are the rare gene fusions such as RET, NTRK, ALK, and BRAF fusions (collectively, ∼6%). 28 Compared with BRAF-mutated tumors treated with DT alone, non-BRAF-mutated tumors have even shorter duration of response to single-agent TKI. As with ALL, a more aggressive combinational approach is needed early on.
The major limitation of using the combination strategy of some of the drugs that target oncofusions in thyroid cancer with immunotherapy, is toxicity. 29,30 For example, larotrectinib, selpercatinib, and alectinib cause a high rate of hepatotoxicity as single agents, making it problematic to combine with immune checkpoint inhibitors in our experience. 28 A run-in period and using drugs with lower hepatotoxicity, such as the RET inhibitor, pralsetinib, could be considered as a candidate to combine with immunotherapy but have not been studied at this time.
Patients with non-BRAFV600E-mutated ATC and with localized disease (M0) should undergo surgery (if feasible) and/or external beam RT with radiosensitizing chemotherapy. 2,11 However, after surgery and chemoradiation, adjuvant pembrolizumab for 2 years is used at our institution. Contrary to the current guidelines that recommend follow-up without further treatment, 2,11 adjuvant pembrolizumab may offer a significant improvement in disease-free survival. 31 Updated data presented at the ATA 2024 comparing 16 patients treated with adjuvant pembrolizumab after upfront radiation (mostly with radiosensitizing chemotherapy) with a matched control arm of patients who were observed after upfront radiation, showed a significant difference in relapse rates (19% treatment arm, 82% control arm; p = <0.001), median PFS (not reached in treatment arm, 5.4 months in control arm; p = 0.002) and median OS (not reached in treatment arm, 31 months in control arm; p = 0.005) between the groups. However, we acknowledge the limitations of this study, which include the small numbers due to the rarity of patients presenting with localized disease, the retrospecive nature of the study, and differences in follow-up time in the treatment arm versus control group (23 months vs. 50 months, respectively).
Until we have better options for patients with metastatic (M1) ATC without a BRAF mutation, lenvatinib plus pembrolizumab is the current standard of care at our institution, and has been included in the 2024 NCCN guidelines. However, in our experience, responses are not as impressive as when compared with DTP. To date, only a small retrospective trial on six patients has been peer-reviewed and published. 32 Two clinical trials have completed enrollment, one in the United States and the other in Europe (NCT04171622, EudraCT 2017-004570-3). Only the European trial has been reported but it is in abstract form. Preliminary data show an overall response rate of 55% and a median OS of 11 months. 33 Another trial in Russia is accruing (NCT06374602). At our institution, when the primary tumor is not resectable or the patient has widely metastatic disease, we use palliative doses of external beam radiation to the primary tumor (and sometimes bulky or symptomatic metastases) during Induction Therapy, before starting lenvatinib/pembrolizumab. The radiation serves to quickly deliver effective control of the primary tumor, and may also prime the immune system to recognize tumor antigen 34,35 (Fig. 2). The efficacy of this treatment regimen is currently under investigation, but data should become available in the coming year. Similar to the strategy for BRAF-mutated ATC, Consolidation Therapy with surgery for resectable tumors has been incorporated into the regimen for these patients. This is followed by the resumption of lenvatinib plus pembrolizumab as Maintenance Therapy.
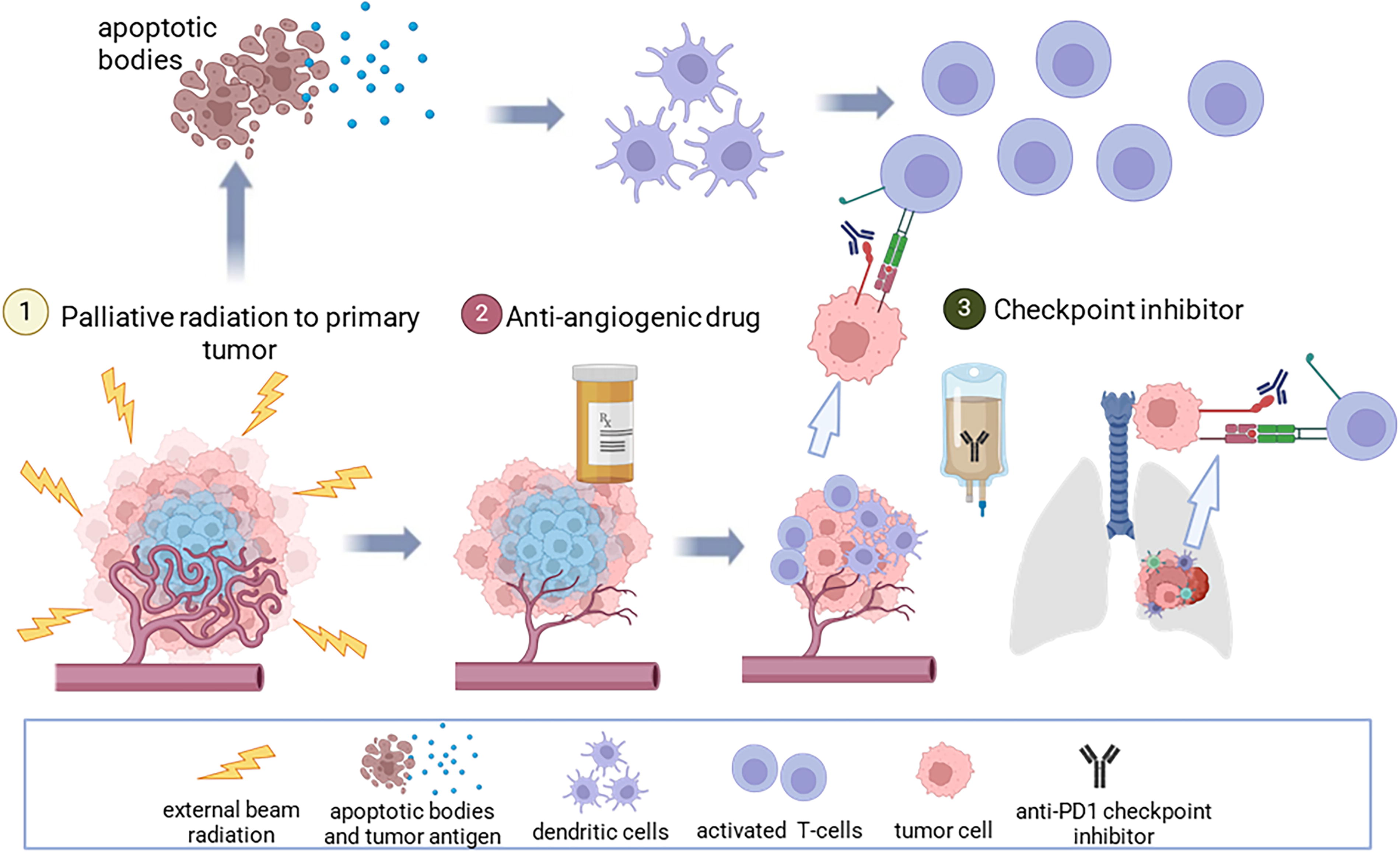
Proposed management of non-BRAF-mutated anaplastic thyroid cancer (ATC) with distant metastatic disease. Our current treatment strategy is extrapolated from the understanding of the tumor and immune responses from ATC and other tumor types and includes (1) low-dose radiation to the primary tumor, followed by (2) anti-angiogenic therapy and (3) checkpoint inhibitor therapy. Radiation helps control the primary tumor, leading to death of irradiated normoxic cells and tumor shrinkage. Radiation-induced apoptosis releases tumor antigens that may be recognized by the immune system, enhancing immune cell infiltration into the tumor. The anti-angiogenic drug works systemically on VEGF receptors in tumors, leading to pruning and organization of tumor vasculature, reducing tumor size, and allowing immune cell infiltration such as dendritic cells and cytotoxic T-cells. The checkpoint inhibitor blocks the interaction between PD-1 and PD-L1, resulting in an anti-tumor immune response in the primary tumor and metastatic disease. Created in BioRender. Cabanillas, M. (2025) https://BioRender.com/p25z347.
The major limitation of lenvatinib is that anti-angiogenic drugs are not recommended for patients who have had a myocardial infarction in the past 6 months, uncontrolled hypertension, or poor cardiac function. Patients with large, unhealed wounds, hemoptysis, colitis, diverticulitis, intestinal perforation, recent bowel surgery, and tumor invading the trachea or esophagus have a relative contraindication to lenvatinib. 36 In these patients, anti-angiogenics should be avoided if possible, or used at lower doses and with extreme caution, and patients should be advised of possible adverse effects that could be life-threatening. Lenvatinib also causes severe weight loss over time, which limits its use in some patients. It is important to have non-anti-angiogenic alternatives, as these drugs are not safe for all patients.
Two other non-anti-angiogenic combination therapies, both tested in a small cohort of patients with ATC are ipilimumab (anti-CTLA4) plus nivolumab (anti-PD1), 37 and cobimetinib (MEK inhibitor) plus atezolizumab (anti-PDL1). 10 In the latter study, 21 patients were treated with cobimetinib plus atezolizumab. The median OS was 8.74 months (CI, 5.13–36.96), median PFS 4.80 months (CI, 1.84–14.69). The study evaluating two checkpoint inhibitors, ipilimumab plus nivolumab, included only 10 patients with ATC. The combination showed promising results, with a 30% objective response rate. The advantage of this combination is that there appear to be some patients who are cured with the regimen, as evidenced by the flattening of the curve in this study. Ipilimumab, for a limited number of doses, plus nivolumab is a treatment that has been most effective in curing metastatic melanoma. 38 It may be an interesting strategy for Maintenance Therapy, particularly for patients who have residual ATC after neoadjuvant therapy followed by surgical resection, in order to address the resistant clones and create long-term “memory” 39 for the immune system.
Other Tools in the Toolbox
There are several other promising strategies for Induction and Maintenance Therapy. RAS mutations, particularly RASQ61x, may become targetable with pan-RAF or pan-RAS inhibitors in the future. Currently, studies are underway to determine if these are effective in thyroid cancer and other solid tumors (NCT05907304).
Antibody-drug conjugates are a newer class of targeted therapy being studied in oncology. The idea is to use a monoclonal antibody targeted toward an antigen that is expressed on ATC tumor cells (e.g., TROP-2, NECTIN-4, ICAM-1) and attach a cytotoxic drug that is internalized by the cell. The tumor would likely need to highly express the antigen for the drug to work in ATC, as these tumors are heterogeneous. Clinical trials are underway (NCT06311214 and NCT06235216), which could determine whether there is a response signal in ATC and could be applied during Induction and/or Maintenance Therapy.
Chimeric Antigen Receptor T-cells (CAR-Ts) and Chimeric Antigen Receptor NK-cells (CAR-NKs) are other strategies that could be employed in ATC. The former is already in clinical trials in ATC, having completed the dose-finding phase of the study 40 (NCT04420754). Like ALL 41 , CAR-T cells may be best utilized in patients with good performance status and low tumor volume. The disease must be well controlled since systemic therapy has to be discontinued in order to receive the CAR-T cells. Our vision is to employ engineered cytotoxic lymphocytes in patients who continue to have some disease that is not cleared during Consolidation Therapy, rather than in Induction when rapid control is needed.
Personalized mRNA vaccines that target specific tumor neoantigens are another promising form of treatment in oncology. 42,43 As with CARs, these are unlikely to be used for cytoreduction due to the length of time it would take to deliver a personalized vaccine to a patient. However, if initial clinical trials with vaccines appear promising in ATC, adding a checkpoint inhibitor to a personalized mRNA vaccine during Consolidation or Maintenance Therapy could be a favorable strategy to eliminate resistant clones. The limitation of a personalized vaccine is the need for tissue, which is sometimes not available. However, an “off-the-shelf” vaccine should also be studied.
Expansion of the Road Ahead
As with acute leukemias, minimal or molecular residual disease (MRD) measured in the patient’s serum is increasingly becoming a reality in solid tumors. 44,45 As we forge ahead in ATC, we are starting to incorporate serial cfDNA tests into clinical practice. 46 These tests are used as an adjunct biomarker to track responses and early relapses. As these tests become more sensitive, MRD could be utilized in the future to determine when Maintenance Therapy can be discontinued or when a patient needs a change in therapy due to early relapse.
Second-line therapy for relapsed ATC is a critical area that warrants further focus. These patients should undergo biopsies at the time of progression to gain insights into the tumor biology, which can inform treatment strategies. While there is no accepted second-line therapy, in general, with BRAFV600E-mutated patients, the BRAF inhibition should not be discontinued, as rapid progression ensues. 47,48 In a retrospective study in patients progressing on DT, adding pembrolizumab to DT at progression resulted in a median OS of 16 months vs. 3 months if DT was stopped or replaced by a different regimen. 48 At this time, each patient is treated in a personalized manner during relapse, based on the mutation profile of the refractory tumor. For example, patients with BRAF-mutated ATC who relapse on DTP and have an emergent RAS mutation are treated with DLP (dabrafenib, lenvatinib, pembrolizumab). Thus, continuing dabrafenib and replacing trametinib with another drug has been our strategy to address the emerging resistant clones while continuing the pressure on the BRAF-mutated population of ATC cells. A retrospective study has shown a median OS of 3 months with DLP, although the disease-control rate was 46%. 49 For patients with limited oligoprogression, metastasis-directed local therapy with RT may be considered to address resistant clones and facilitate the continuation of ongoing systemic regimens. 50 Pemetrexed plus carboplatin has shown promise in refractory thyroid cancer patients, including a patient with ATC who was successfully treated after third line therapy. 51 At this time, it is unclear how to treat patients who progress through first-line therapy, and the data to support any particular therapy are limited.
Better second-line therapies are needed for BRAF-mutated ATC without any identifiable resistant mutation. For example, TET2-mutant macrophages infiltrate ATC tumors and mediate resistance to BRAF/MEK inhibitors. 52 These macrophages overexpress TGF-β-family ligands, and inhibition of TGF-β signaling restores response to BRAF/MEK inhibitors in a mouse model. Thus, inhibition of TGF-β signaling in combination with BRAF/MEK inhibitors could be a valuable target in the future.
Working Through the Challenges
We acknowledge that there are many challenges to managing patients with ATC. First, not all patients want an aggressive treatment regimen that potentially could reduce their quality of life for various reasons. Our “Total Therapy” approach is meant for patients who are motivated with reasonable performance status. Therefore, the goals of care, potential benefits, risks, alternate therapeutic/palliative options, and quality of life implications of treatments are discussed with each patient with ATC before treatment begins. The prognosis for ATC, while it has improved greatly from a few months to ≥1 year, remains very serious, particularly for those without a BRAF mutation, and is shared with the patient.
Second, similar to acute leukemia, due to the aggressiveness of ATC, the treatment must be implemented swiftly. For example, at our institution, patients with ATC seeking an appointment are expedited and then evaluated within a week. Once they are evaluated, establishing the BRAF status is accomplished within days, and if mutated, DT is started within a week of the patients’ visit. We acknowledge that this could influence patient outcomes and that this may not be possible at all centers.
Third, many patients with ATC present with inability to swallow, or are intubated, making oral targeted therapy difficult to administer. Dabrafenib may be prescribed as a tablet for suspension, but this drug is usually not readily available in our pharmacy. While not recommended per the prescribing information, it is our practice to allow the patient (or inpatient pharmacy) to dissolve dabrafenib in water and crush trametinib, and this is also described in the literature. 53 The prescribing information for lenvatinib gives information on dissolving the drug in water. 54
Lastly, the United States is in a unique position compared with the rest of the world, because there are laws that allow for off-label use of cancer drugs under the Rockefeller-Levin Bill and the Right to Try Act. The former bill requires Medicare to cover off-label use of cancer drugs if they are included in compendia. This is why it is critical that guidelines, which are used by Medicare, stay updated and allow for reasonable data in rare cancers to be used in the guidelines. Clinicians and patients have the power to advocate for change, which will allow for coverage of off-label cancer drugs for ATC.
European, Latin American, Asian countries, and Canada 55 face greater challenges when it comes to off-label use of cancer drugs and, in some, molecular interrogation of tumors. The most feasible solution to this problem is clinical trials. Clinical trials for ATC in countries outside of the United States recruit faster due to the lack of accessibility to off-label drugs for cancer patients. Randomized-controlled trials may also be possible in these countries. However, the funding is the greatest challenge to opening these trials, which will require pharmaceutical companies and philanthropy to achieve these goals. Given the high cost of clinical trials and limited resources, there is a need to rethink how we conduct clinical trials in ATC. Another less costly approach is the Master Observational Trial, 56 which uses real-world prospective data to compare the efficacy of existing therapies in patients. At our institution, this type of trial, called “GRASSROOT”, has been initiated 46,57 and work is underway to open the clinical trial in Latin America, Canada, Europe, and Asia (NCT06507878).
Conclusions
In the past decade, there has been a resurgence of interest and concerted efforts in treating patients with ATC, rather than palliating them. This paradigm shift has led to success in opening and enrolling patients with ATC to clinical trials. Because of this, we now have an FDA-approved regimen for BRAF-mutated ATC and a regimen for non-BRAF-mutated ATC that is guideline recommended. While these treatments lead to responses initially, they fail to cure patients due to the emergence of resistant clones, as was first observed in the late 1960s with ALL. Multiple drug therapy and then the novel curative approach of “Total Therapy” are what led to success rates of nearly 90% in childhood ALL and cures of other tumors. We have reimagined this concept of “Total Therapy” for ATC, developing a comprehensive, multi-modal treatment strategy encompassing Induction, Consolidation, and Maintenance Therapy. Our approach builds upon the principles established by the pioneers of oncology, while leveraging cutting-edge therapeutic modalities such as targeted therapy and immunotherapy, and integrating surgery and RT, followed by prolonged suppressive therapy with targeted and immunotherapy to avoid resistance development. The tools to potentially cure ATC are at our fingertips, and the road ahead is no longer bleak. As eloquently articulated by Dr. Vincent DeVita, “at this date, we are not limited by the science; we are limited by our ability to make good use of the information and treatments we already have.” 7
Footnotes
Acknowledgments
The authors dedicate this article to Dr. Emil “Jay” Freireich whose genius lives on. The authors extend their heartfelt gratitude and appreciation to the many patients and their families who have entrusted them with their care and to the generous supporters and the donors to the multi-disciplinary ATC program at MD Anderson Cancer Center.* Finally, the authors express their appreciation to Dr. DeVita for inspiring us to challenge the status quo.
*The MD Anderson Cancer Center FAST Multidisciplinary Group (alphabetical order): Neal Akhave‡, Victoria Banuchi§, Naifa Busaidy†, Ramona Dadu†, Renata Ferrarotto‡, Gary B. Gunn‖, Sarah Hamidi†, Marie-Claude Hofmann†, S. Mohsen Hosseini#, Priyanka C. Iyer†, Stephen Y. Lai§, Anna Lee‖, Anastasios Maniakas§, Matthew S. Ning‡, Michael Spiotto‖, Jennifer R. Wang§, Michelle D. Williams#, Mark Zafereo§.
Authors’ Contributions
Conceptualization and drafting of the article: M.E.C. Critical review and editing of the article: N.A., V.B., N.B., R.D., R.F., G.B.G., S.H., M.-C.H., S.M.H., P.C.I., S.Y.L., A.L., A.M., M.S.N., M.S., J.R.W., M.D.W., and M.Z. All of the authors have reviewed the final version of the article and agree to be accountable for the content.
Author Disclosure Statement
M.E.C. has received consulting fees from Bayer, Exelixis, Lilly, Novartis and research funding from Merck, Genentech, Eisai, Exelixis. N.A. has sponsored research with Aveo Pharmaceuticals, Innocare Pharma, Bicara Therapeutics, and Pfizer/Genmab and has received consulting fees from Genmab/Pfizer. N.B. reports research funding from Eisai and personal consulting fees from Eisai and Eli Lilly. R.D. reports research funding from Eisai, Merck, Exelixis and AstraZeneca, and personal fees from Bayer and Exelixis. R.F. reports personal fees from Regeneron, Eisai Inc, Remix Therapeutics, Coherus BioSciences, Rgenta Therapeutics, BioAtla, Bicara Therapeutics, RAPT Therapeutics, and LEK consultant. She reports non-financial support (to institution) from ISA Therapeutics, Merck Serono, Viracta, Gilead, Remix Therapeutics, Rgenta Therapeutics, and Mersana Therapeutics outside the submitted work. A.M. reports research funding from JAZZ Pharmaceuticals and Thryv Therapeutics Inc. M.Z. has received research funding from Merck, Eli Lilly, and Exelixis. S.Y.L. is a medical affairs consultant for Cardinal Health. M.D.W. has research funding from Bayer. S.H., M.C.H., V.B., A.L., and M.S. have nothing to disclose.
Funding Information
No funding was received for this article.