
Abstract
Background:
Thyroid dysfunction is common in older adults and poses diagnostic and management challenges for clinicians. In this narrative review, we present published data focusing on special considerations in the diagnosis and management of hypothyroidism and hyperthyroidism in older adults.
Methods:
A comprehensive literature search of the PubMed and Ovid MEDLINE databases was conducted from January 2000 to December 2024 to identify pertinent articles in English for this narrative review.
Results:
Due to significant cardiovascular risk if untreated, both overt hypothyroidism and hyperthyroidism should be treated in older adults. Findings from observational studies do not support treating older adults with subclinical hypothyroidism with a thyrotropin (TSH) <7 mIU/L. However, observational data have demonstrated an increased risk of cardiovascular mortality and stroke in older adults with subclinical hypothyroidism with TSH 7.0–9.9 mIU/L and of coronary heart disease, cardiovascular mortality, and heart failure in those with TSH ≥10 mIU/L, suggesting levothyroxine treatment in these individuals should be considered. Data from clinical trials failed to show improvement with levothyroxine in hypothyroidism symptoms or fatigue in older adults with subclinical hypothyroidism compared with placebo. Over- and under-replacement with thyroid hormone is common and should be avoided, as population-based studies have shown associations with adverse cardiovascular and skeletal events. Subclinical hyperthyroidism with a TSH <0.1 mIU/L should be treated in older individuals as it has been associated with increased cardiovascular risk and bone density loss based on observational data. Randomized controlled trials have shown that long-term low-dose methimazole is a viable alternative to radioactive iodine in older adults with hyperthyroidism.
Conclusions:
A personalized approach should be undertaken in the diagnosis and management of thyroid dysfunction in older adults. Multiple factors should be considered, including physiological age-related changes in thyroid function, comorbidities, and polypharmacy. Care should be taken to maintain euthyroidism in order to avoid adverse events.
Introduction
Thyroid dysfunction, including hypothyroidism and hyperthyroidism, is common in older adults, and its incidence is increasing owing to the growth of the older adult population due to increasing life expectancy, 1,2 as well as due to overdiagnosis. 3 –8 Various physiological age-related changes in thyroid function are known to occur (Fig. 1). Several cross-sectional and longitudinal studies have demonstrated increased thyrotropin (TSH) concentrations with increasing age, independent of the presence of antibodies and without any changes in free thyroxine (fT4) concentrations, with higher TSH levels conferring a survival benefit and associated with longevity in older adults. 9 –12 Potential mechanisms for the association of a higher TSH level with longevity include a possible correlated lower bioactivity of thyroid hormone or decreased responsiveness of the thyroid gland to TSH, which may serve as an adaptive mechanism against catabolism by the lower basal metabolic rate in older adults. 13,14
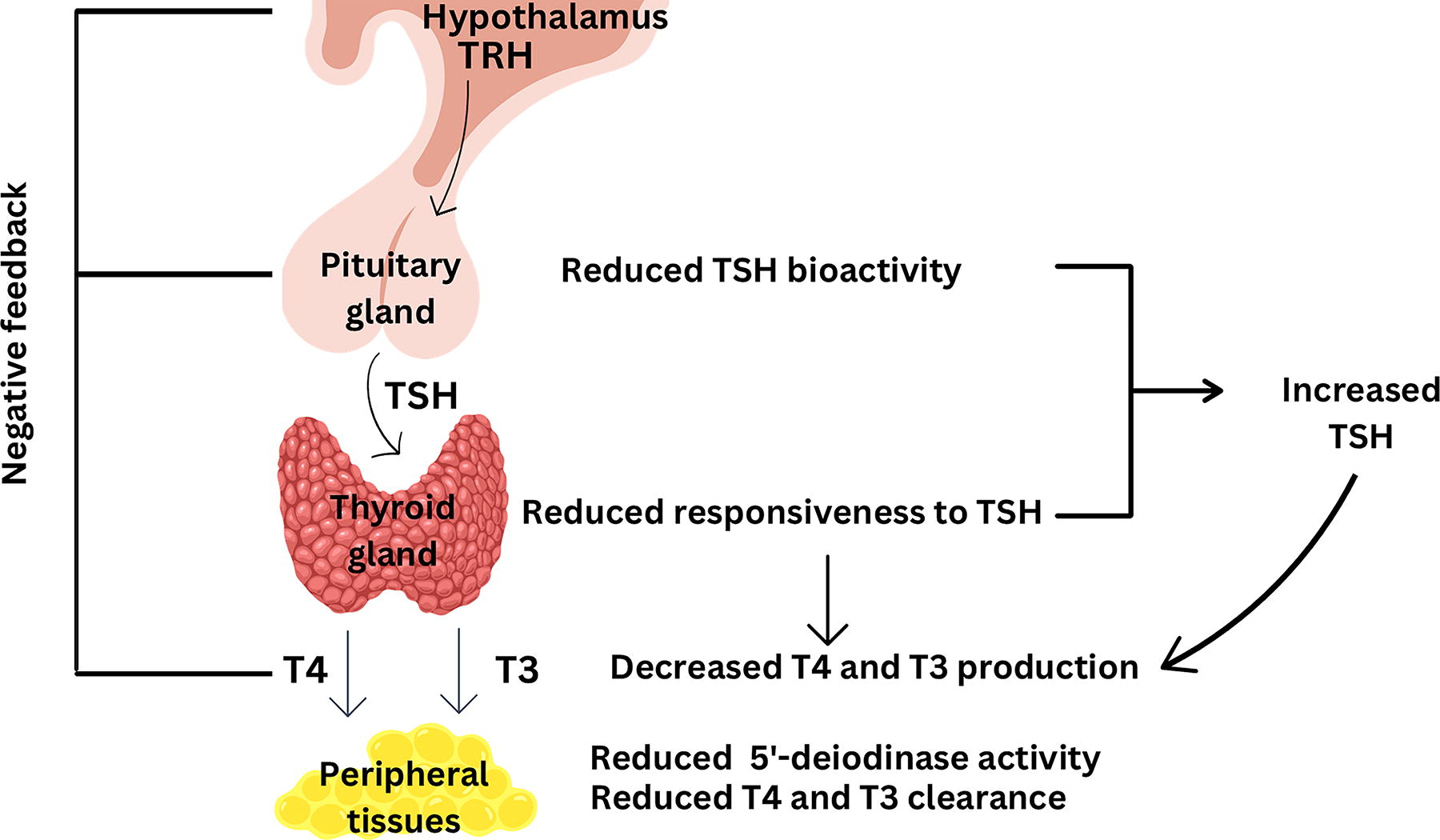
Physiological Age-Related Changes in Thyroid Function. This figure depicts physiological changes in thyroid function due to aging and potential mechanisms underlying these changes.
With advancing age, clearance of circulating thyroxine (T4) and triiodothyronine (T3) declines, resulting in longer half-life, from 7 days in younger individuals to 9 days in those aged 80 years and older. 15 In addition, there is a compensatory reduction in T4 and T3 production, with T3 levels being lower in older adults without acute illness compared with younger individuals, which may indicate an age-related decline in 5ʹ-deiodinase activity. The prevalence of antithyroid antibodies also increases with age, particularly in women, signaling an age-related rise in autoimmune thyroid disease. 9
Several factors complicating thyroid function test interpretation, including comorbid medical conditions, polypharmacy with medications that alter thyroid hormone absorption, metabolism or thyroid function tests, and age-dependent physiological changes in the hypothalamic–pituitary–thyroid axis, may delay diagnosis in the older adult population. 9,13,16 –19 It is also important to note that there are variations in TSH levels among healthy individuals and that TSH exhibits diurnal variation. Thyroid dysfunction in older patients also presents a diagnostic challenge as the classical symptoms of hypothyroidism and hyperthyroidism may be less frequently reported or absent in this population compared with their younger counterparts with the same degree of thyroid function abnormalities. 20 Symptoms such as fatigue, depression, cognitive decline, constipation, and falls, which are often attributed to advancing age, may hinder the diagnosis of thyroid dysfunction in older adults. 21 Moreover, special considerations should be undertaken to personalize the management of hypothyroidism and hyperthyroidism in older adults, taking into account symptomatology, weighing treatment benefits versus risks, and incorporating patient preferences and goals of care.
In this narrative review, we focus our discussion on the diagnosis and management aspects of thyroid dysfunction, including hypothyroidism and hyperthyroidism, in older adults in the outpatient setting. Key highlights are shown in Table 1. This review does not include nodular thyroid disease or thyroid cancer.
Key Highlights on the Clinical Aspects of Hypothyroidism and Hyperthyroidism in Older Adults
TSH, thyrotropin.
Methods
Pertinent articles published in English were identified for inclusion in this narrative review by searching the PubMed and Ovid MEDLINE databases from January 2000 to December 2024. Search terms used included “older adults,” “age,” “aging,” “thyroid dysfunction,” “hypothyroidism,” “hyperthyroidism,” “diagnosis,” “management,” “treatment.” We prioritized inclusion of randomized controlled trials, systematic reviews and meta-analyses, and observational studies. Additional studies were selected after review of the references of identified articles. For this narrative review, older adults were defined as 65 years and older.
Hypothyroidism
Diagnosis
Hypothyroidism may present with a broad spectrum of symptoms, with studies showing that older adults present with fewer signs and/or symptoms overall, as well as with diminished frequency of classical hypothyroid signs compared with younger patients. 22 In a prospective study comparing 24 symptoms and signs between older (age ≥70 years) and younger patients (age ≥55 years), the mean number of clinical signs in older adults was significantly lower than in younger patients (6.6 vs. 9.3; p < 0.01), with only fatigue and weakness being present in more than 50% of older adults with overt hypothyroidism. 22 Another population-based study compared the usefulness of a composite score of 13 hypothyroidism-associated symptoms in predicting overt hypothyroidism in different age groups (young: <50 years, middle age: 50–59 years, old: ≥60 years). 20 The authors found that the hypothyroidism symptom score was a good discriminating tool to identify hypothyroidism in young patients (area under the receiver operating characteristic curve = 0.91; [CI 0.82–0.998]) but failed to do so correctly in older adults (area under the receiver operating characteristic curve = 0.64; [CI 0.54–0.75]), suggesting the clinical presentation of hypothyroidism in this group is often subtle. 20 Therefore, a high index of suspicion is required for definitive diagnosis of hypothyroidism in older adults.
Clinically, hypothyroidism is a biochemical diagnosis with overt hypothyroidism defined by a serum TSH level above the upper limit of the reference range and serum fT4 level below the lower limit of the reference range, while subclinical hypothyroidism is characterized by a high TSH with a normal fT4 level. While the reference range for TSH depends on the laboratory assay used, it does not usually incorporate age-specific changes, where a reclassification from abnormal to normal thyroid function may occur due to older age. 23 Whether the use of age-specific TSH reference intervals improves the accuracy of hypothyroidism diagnosis in older adults and should be adapted in clinical practice remains controversial. 23 Of note, fT4 levels need to be interpreted in the absence of nonthyroidal illness or interfering medications.
Management
Thyroid hormone preparations
Levothyroxine, the most common synthetic thyroid hormone formulation, is widely prescribed to older adults, despite growing uncertainty over the appropriate interpretation of an isolated elevated TSH in this population. 24 Specifically, the proportion of adults who reported thyroid hormone use increased from 4.1% in 1997 to 8.0% in 2016, with most of the rise occurring among adults older than 65 years. 1 Increases in thyroid hormone use in this age group are thought to be predominantly from a rise in thyroid hormone initiation for the treatment of subclinical hypothyroidism, which is most frequently diagnosed in older adults and is sometimes but not always accompanied by hypothyroid symptoms. 3,4 In addition, once levothyroxine is initiated, it is continued lifelong in ∼90% of patients. 2
Levothyroxine monotherapy is currently considered the standard of care for all patients with hypothyroidism, including older adults. 25 The American Geriatrics Society Beers Criteria® lists desiccated thyroid extracts, which are derived from porcine or bovine thyroid glands and contain a supraphysiologic amount of T3, as potentially inappropriate medications to avoid in older adults, due to increased risk for cardiac adverse effects in adults aged 65 years and older. 26
Treatment initiation and dosing
Overt hypothyroidism should be treated with levothyroxine regardless of age. 25 Goals of treatment are to achieve biochemical euthyroidism, relieve patient symptoms, and avoid overtreatment. 25 Whether subclinical hypothyroidism should be treated and at what TSH thresholds should levothyroxine be initiated remains unclear. It is important to note that transient mild fluctuations in serum TSH may occur in older patients without thyroid disease and may subsequently normalize. Therefore, before considering initiation of levothyroxine therapy, thyroid function tests should always be repeated after initial testing to confirm persistent subclinical hypothyroidism, that is, mildly elevated TSH levels with normal fT4 for at least one month in patients who do not have abnormalities in the hypothalamic–pituitary–thyroid axis and without recent severe illness. 27
Observational studies showed no significantly increased incidence in cardiovascular, musculoskeletal, or neurocognitive adverse events or all-cause mortality in individuals with subclinical hypothyroidism aged 65 years and older when serum TSH concentration was above the upper limit of the reference range but lower than 7.0 mIU/L, compared with euthyroid adults. 15,28 –30 In a prospectively planned combined analysis of data from two randomized controlled clinical trials involving 251 adults aged 80 years and older with subclinical hypothyroidism, treatment with levothyroxine, compared with placebo, was not significantly associated with improvement in hypothyroid symptoms or fatigue (adjusted between-group difference = 1.3 [CI −2.7 to 5.2]; p = 0.53 and adjusted between-group difference = −0.1 [CI −4.5 to 4.3]; p = 0.96, respectively). 31 These findings suggest that routine use of levothyroxine for treatment of symptoms that may be attributed to subclinical hypothyroidism in adults aged 80 years and older may not be warranted. Furthermore, symptoms of hypothyroidism and cardiovascular parameters did not improve after levothyroxine treatment in older individuals with subclinical hypothyroidism. 32 –34 However, older adults with TSH levels ≥10 mIU/L and normal fT4 should be initiated on levothyroxine therapy due to the increased risk of progression to overt dysfunction and increased risk of coronary heart disease, cardiovascular mortality, and heart failure, 35,36 while consideration should be given to initiating treatment in those with a TSH 7–9.9 mIU/L in view of observational data showing increased risk of cardiovascular mortality and stroke in this subgroup of patients. 28 –30,36
In order to avoid overtreatment, it is important to note that older adults have lower thyroid hormone dose requirements compared with younger patients, which may be related to declining metabolic clearance, declining lean body mass, and interactions with medications prescribed for comorbid conditions. In general, older patients require 20–25% less per kilogram of body weight daily than younger patients due to the aforementioned reasons. 37,38 Treatment of hypothyroidism in older patients should also take into account the underlying health status of the patient, especially cardiovascular comorbidities, as well as goals of care.
Current guidelines on weight-based levothyroxine dose initiation and titration rely on estimates from younger populations. 25 Data from the Baltimore Longitudinal Study on Aging on 187 community-dwelling individuals aged 65 years and older demonstrated that the full replacement thyroid hormone dose per body weight estimates in older adults are one-third lower than current weight-based dose recommendations for younger populations (1.1 mcg/kg vs. 1.6 mcg/kg). 39 Specifically, 84% of euthyroid individuals in this study were on a thyroid hormone dose of less than the recommended full replacement dose used in younger patients, suggesting the need for increased clinician awareness when managing thyroid hormone replacement in older adults. 39
Overall, current clinical practice guidelines recommend a “start low and go slow” approach for patients aged 60 years and older (particularly due to the longer half-life of circulating thyroxine in older adults), with initiation of 50 mcg levothyroxine daily in patients with no known cardiac disease and 25 mcg daily for those with cardiac disease, followed by close biochemical monitoring and patient symptoms. 25
Ideal biochemical targets
Once thyroid hormone replacement is initiated, euthyroidism is determined by normalization of thyroid function tests, with TSH currently being considered the most sensitive test. However, the optimal TSH target for older adults is unclear. To assess whether a higher target TSH of 4.01–8.0 mIU/L is feasible and acceptable in patients aged 80 years and older who were on stable levothyroxine therapy with serum TSH levels within the standard reference range (0.4–4.0 mIU/L), Razvi et al. conducted a single-blind randomized controlled feasibility trial in 48 patients. Following 24 weeks, patients with a higher target serum TSH did not exhibit worsening patient-reported outcomes, including symptoms and quality of life, cardiovascular risk factors, or bone resorption markers. 40 The American Thyroid Association guidelines recommend that a TSH goal of 4–6 mIU/L is acceptable for patients who are 70 years and older. 25
In advancing our understanding of the impact of patient age in the management of hypothyroidism in real-world settings, a nationwide survey of primary care physicians and endocrinologists found that only 53% of physicians incorporated patient age in their decision making when managing hypothyroidism. 41 However, when presented with clinical scenarios differing in patient sex and age, 90% of respondents targeted a TSH >1.5 mIU/L in octogenarians, with TSH goal ranges increasing in a direct relationship to patient age. This may indicate clinicians’ attempts to avoid overtreatment in the oldest old. 41
Factors influencing treatment
Several factors can influence the management of hypothyroidism in older adults, including the presence of comorbid conditions and the concomitant use of multiple over-the-counter and prescription medications, which affect absorption, protein binding, or metabolism of levothyroxine. 42 –44 In a retrospective cohort study of 538,137 adults aged ≥65 years who were prescribed thyroid hormone replacement between 2004 and 2017 (median follow-up, 56 months), almost one-third of patients were on concomitant medications known to interfere with thyroid hormone metabolism. 45
Frailty status and cognitive function are also important considerations when treating older adults with hypothyroidism, as these patients are more vulnerable to adverse effects from overtreatment or nonadherence.
Thyroid hormone over- or under-replacement
Older adults represent a key population for careful thyroid function test monitoring while on therapy, as it has been previously shown that both thyroid hormone over- and under-replacement are fairly common in this population. 46,47 Data from 339 community-dwelling adults aged ≥65 years on thyroid hormone replacement therapy who are enrolled in the Cardiovascular Health Study showed that only 42.8% had a TSH in the euthyroid range, while 41% had a low TSH and 16.2% had a high TSH. 46 Thyroid hormone over-replacement leading to iatrogenic thyrotoxicosis was also prevalent in a cohort of older adults from the Baltimore Longitudinal Study on Aging, with 9.6% of participants having a low TSH, and the highest rates were observed among older women. 47 Similar findings were reported in other observational studies, including a staggering 48% of older adults taking thyroid hormone preparations who were enrolled in the Framingham Heart Study having a low TSH. 48,49
Thyroid hormone treatment intensity has more recently become a focus of investigation, particularly in trying to ascertain whether it is a modifiable risk factor for cardiovascular morbidity and mortality, especially in older adults. 50 –53 Flynn et al. studied a cohort of 17,684 patients (mean age = 61 years) and demonstrated increased risk of a composite outcome of cardiovascular admission or death with both suppressed or high TSH levels. 50 In another large study, Thayakaran et al. evaluated 162,369 patients with hypothyroidism, adjusting for levothyroxine treatment, and found that high TSH concentrations, suggesting under-replacement, were associated with increased risk of ischemic heart disease and heart failure compared with euthyroidism. 51 Using data from the Veterans Health Administration, two population-based studies showed increased risk of atrial fibrillation, stroke, and cardiovascular mortality in thyroid hormone users who were over- or under-replaced even when adjusting for relevant demographic and traditional cardiovascular risk factors, with risk being cumulative over time. 52 The risk of cardiovascular mortality was directly associated with the degree of thyrotropin abnormality outside the euthyroid range, with TSH concentrations lower than 0.1 mIU/L and higher than 20 mIU/L being associated with the highest risk. 52
There is also increasing awareness of the effect of thyroid hormone over-replacement on bone health, with current data supporting thyroid hormone excess being associated with increased bone loss and risk of fractures, particularly in postmenopausal women. An older meta-analysis of 41 controlled cross-sectional studies evaluating the impact of long-term levothyroxine therapy on bone mineral density (BMD) found that suppressive thyroid hormone therapy was associated with significant bone loss at the lumbar spine and hip in postmenopausal women, but not in premenopausal women. 54 A nested case–control study of 213,511 adults aged 70 years and older on levothyroxine showed that, after adjustment for several risk factors, current levothyroxine use was associated with a significantly higher risk of fracture compared with remote use (adjusted odds ratio = 1.88, [CI 1.71–2.05]) and exhibited a strong dose–response relationship. 55 Moreover, similar trends have been shown in several studies in patients undergoing long-term TSH suppression therapy due to differentiated thyroid cancer, with longer duration being more detrimental to bone density and strength in postmenopausal women. 56 –59
Whether thyroid hormone over- or under-replacement is associated with adverse cognitive outcomes in older adults remains unclear. 60 A meta-analysis of 11 studies with a total of 24,952 participants demonstrated an increased risk of dementia in individuals with TSH levels below the reference range or higher fT4 levels, when adjusting for thyroid medication use. 61 A cohort study that performed a longitudinal time-varying analysis of electronic health records of 65,931 patients aged 65 years and older at a single institution showed that a low TSH level including from iatrogenic thyroid hormone over-replacement was associated with higher risk of incident cognitive disorder, defined as mild cognitive impairment or any-cause dementia, with more severe iatrogenic hyperthyroidism having a stronger association. 62 Even though additional large, prospective cohort studies and randomized controlled trials are still needed to determine whether there is a causal relationship between thyroid hormone over- or under-replacement and dementia, clinicians considering thyroid hormone therapy in older adults should be cognizant to avoid inappropriate treatment.
These findings highlight the importance of maintaining euthyroidism in older patients receiving thyroid hormone therapy in order to reduce possible adverse effects on the cardiovascular, skeletal, and neurocognitive systems, as well as the risk of cardiovascular mortality.
Deprescribing
Even though thyroid hormone therapy is typically considered a lifelong therapy, it is appropriate to deprescribe in some settings, that is, lower the thyroid hormone dose when patients are overtreated or discontinue the medication when patients are on it without an appropriate indication. The most vulnerable are older adults. A systematic review and meta-analysis of 17 observational studies found that up to a third of patients remained euthyroid after thyroid hormone discontinuation, with a higher proportion of those remaining euthyroid having a diagnosis of subclinical hypothyroidism. 63 In a qualitative study of endocrinologists, geriatricians, and primary care physicians who prescribe thyroid hormone, barriers and facilitators to thyroid hormone deprescribing in older adults were reported at the patient, physician, and system levels. 64 The most prominent physician-reported facilitators to thyroid hormone deprescribing were effective physician-to-patient communication and positive physician–patient relationship, including patients’ trust in their treating physician, while barriers included lack of knowledge, physician inertia, and clinic visit time constraints. 64 At least two clinical trials are currently underway exploring the benefits and risks of deprescribing of levothyroxine treatment in older adults. 65,66
Hyperthyroidism
Diagnosis
Hyperthyroidism, defined as the overproduction of thyroid hormones by the thyroid gland, may be challenging to diagnose in older adults due to the confounding effects of concurrent chronic illnesses, medications, and/or the relative paucity of clinical symptoms and signs related to overstimulation of the sympathetic system. In fact, one-third of older adults present with atypical symptoms that have been termed apathetic hyperthyroidism. 13,21,67 –69 In a large cross-sectional study by Boelaert K et al. of 3049 consecutive patients with hyperthyroidism presenting to a single tertiary clinic, increasing age was associated with reduced adjusted odds ratio for the presence of classical symptoms (except weight loss and shortness of breath), independent of disease severity. 68 This study also showed that the majority of older adults reported only one or two symptoms, while younger patients reported five or more. 68 A smaller prospective cohort study comparing 19 classical signs of hyperthyroidism between older (age ≥70) and younger patients (age ≤50) found that only anorexia (32% vs. 4%) and atrial fibrillation (35% vs. 2%) were more frequently seen in older adults compared with their younger counterparts (p < 0.001). 21
Biochemically, subclinical hyperthyroidism, characterized by a low TSH and normal free thyroid hormones, is more common that overt hyperthyroidism in older adults, particularly in patients over the age of 70. 70,71 Left untreated, hyperthyroidism can lead to significant cardiovascular adverse effects, including cardiac arrhythmias and heart failure, which confer increased risk of mortality preferentially for older adults. 72 When the etiology of hyperthyroidism is not apparent based on clinical presentation and initial biochemical evaluation, diagnostic testing is indicated with a radioactive iodine uptake, including a scan if nodules are also present. When clinical suspicion is high, positive thyroid-stimulating immunoglobulin and/or thyroid-receptor antibodies can confirm the diagnosis of Graves’ disease. 73
Management
Rationale and candidates for treatment
Once a diagnosis of hyperthyroidism is confirmed, older adults with overt hyperthyroidism should always be considered for treatment due to well-known cardiovascular risks of persistent thyrotoxicosis, that is, the effects of excess thyroid hormone action in the body. 73
Current guidelines recommend that all individuals aged 65 years and older with subclinical hyperthyroidism and persistently suppressed TSH <0.1 mIU/L on repeated measurement over a 3- to 6-month period should be treated in view of epidemiological evidence showing increased rates of atrial fibrillation, mortality, and adverse skeletal events if left untreated. 35,73 –75 Sawin et al. initially reported a 2.8-fold increased risk of atrial fibrillation in patients over the age of 60 with subclinical hyperthyroidism, including when restricting to those not on thyroid hormone therapy. 48 Subsequently, individual participant data analyses from the Thyroid Studies Collaboration have provided significant evidence supporting this recommendation. In a study where individual data from 52,674 participants were pooled from 10 cohorts, age- and sex-adjusted analyses showed that subclinical hyperthyroidism was associated with increased total mortality (hazard ration [HR] = 1.24; [CI 1.06–1.46]), cardiovascular mortality (HR = 1.29; [CI 1.02–1.62]), coronary heart disease events (HR = 1.21; CI [0.99–1.46]), and atrial fibrillation (HR = 1.68; [CI 1.16–2.43]). 76 Risk of atrial fibrillation and cardiovascular mortality was highest when TSH was <0.1 mIU/L. Another meta-analysis of 17 cohort studies including older adults demonstrated increased relative risks (RRs) for cardiovascular disease (RR = 1.19, [CI 1.10–1.28]), cardiovascular mortality (RR = 1.52, [CI 1.08–2.13]), and all-cause mortality (RR = 1.25, [CI 1.00–1.55]) in individuals with subclinical hyperthyroidism compared with the reference group. 74 Additional data indicate that older adults with subclinical hyperthyroidism are also at a particular risk for the development of heart failure. 35,77
Majority of studies examining subclinical hyperthyroidism have shown reduced BMD in postmenopausal women. 78 Individual participant data analysis of 5458 adults with a median age 72 years from six prospective cohorts found that subclinical hyperthyroidism was associated with greater annual bone loss at the femoral neck compared with euthyroidism (%ΔBMD = −0.18 [CI −0.34, −0.02]; I 2 = 0.0%), which was more pronounced in patients with a TSH <0.1 mIU/L. 78 Contrary to these studies, others did not show any association between subclinical hyperthyroidism and osteoporosis or fractures. 79 –81 For example, data from the Cardiovascular Health Study of 4936 older adults aged ≥65 years found no association between subclinical hyperthyroidism and hip fracture risk or loss of BMD. 79
Studies to date have yielded conflicting results regarding possible correlations between hyperthyroidism and cognitive or physical functioning outcomes, 60,82,83 with some data supporting a possible association between subclinical hyperthyroidism with a TSH <0.01 mIU/L being associated with a higher risk of dementia and cognitive decline in older adults. 62,84
Overall, while long-term safety data on the use of low-dose methimazole and radioactive iodine (RAI) in older adults with subclinical hyperthyroidism are favorable, 85 shared decision making to consider risks versus benefits of treating versus not treating, life expectancy, and goals of care should be undertaken.
Treatment options
In addition to symptomatic treatment with beta-adrenergic blockade, treatment options for endogenous hyperthyroidism are the same as those used in younger patients and include antithyroid medications (methimazole is the preferred thionamide), RAI, and surgery. 73 Due to concerns for high relapse rates of hyperthyroidism in older adults upon discontinuation of antithyroid medications following 12–18 months of treatment, RAI has traditionally been preferred in this population. 73,86 However, treatment should be individualized based on underlying etiology, severity of hyperthyroidism, comorbidities, and risks and benefits of therapies. For example, long-term methimazole treatment may be preferred in select older adults if they have multiple comorbidities, are not good candidates to receive surgery or RAI, or have limited life expectancy. 73
A recent randomized controlled trial aimed to compare the effectiveness and safety of long-term methimazole use and RAI in the treatment of subclinical hyperthyroidism in older adults aged 65 years and older. 85 In this randomized parallel-group trial, 41 and 42 patients with a TSH <0.1 mIU/L were randomized to receive either 15 mCi RAI or long-term low-dose methimazole treatment (up to 10 mg daily for up to 5 years), respectively. All patients were euthyroid at the end of the study (with or without levothyroxine), and no adverse events were observed in either group. The authors concluded that both treatment modalities were effective and safe, with low-dose long-term methimazole being a reasonable alternative to RAI in older adults with subclinical hyperthyroidism. However, periodic clinical and biochemical evaluation of thyroid status should be undertaken in these patients to assess response and monitor for adverse effects. 73
Even though surgery for hyperthyroidism is not contraindicated in older adults, several studies have shown that this population is at higher risk of complications and morbidity, with frailty also being an independent predictor. 87 –90 A retrospective cohort study of 60,990 patients using the American College of Surgeons National Surgical Quality Improvement Program database from 2012 to 2015 found that patients aged ≥65 years were 1.4 times more likely to develop overall complications ([CI 1.19–1.63], p < 0.001), while patients aged ≥80 years were 2.67 times more likely to develop complications ([CI 2.02–3.53], p < 0.001) compared with patients aged 18–64 years. 87 In addition, patients aged ≥80 years had higher rates of thyroidectomy-related readmissions and extended length of hospital stay compared with younger adults (p < 0.05 and p < 0.001). In another study using data from the same database between 2016 and 2017 (N = 2189), authors used a five-factor modified frailty index in comparative analyses for patients who underwent thyroidectomy for multinodular goiter. 90 Compared with patients younger than 65 years, older adults (age ≥65 and <80) and the oldest old (age ≥80) had higher frailty index (14% vs. 22% vs. 31%, respectively, p < 0.001). Oldest old patients and those with a higher frailty index had higher rates of postoperative complications. Therefore, if surgery is pursued in older adults, for example, due to large goiters with obstructive symptoms or suspected or known malignancy, then it should be performed by experienced high-volume surgeons. 73
Summary and Conclusions
Thyroid dysfunction, particularly subclinical, is common in older adults and may be challenging to diagnose due to the concomitant chronic illnesses, interfering medications and paucity of clinical signs and symptoms. Several gaps in knowledge remain, and future research directions are outlined in Table 2. Management requires a personalized approach and should be individualized to take into consideration the risk–benefit ratio of treatments, presence of comorbidities, overall health status, frailty, and life expectancy.
Knowledge Gaps and Future Research
Footnotes
Acknowledgment
We would like to acknowledge Ms. Brittany Gay who assisted with article formatting and submission.
Authors’ Contributions
S.J.: Conceptualization, data curation, writing—original draft, and writing—review and editing. M.P.: Conceptualization, data curation, writing—review and editing, supervision, project administration, and funding acquisition.
Author Disclosure Statement
S.J. and M.P. have nothing to disclose.
Funding Information
M.P. is funded by R01 AG079833-01A1 from the National Institute on Aging of the National Institutes of Health.