
Abstract
Background:
Thyroid hormone exerts its function on virtually all tissues in the human body through binding to the thyroid hormone receptor (TR), making it an interesting vehicle for therapeutic intervention in nonthyroid conditions with metabolic consequences, as well as genetic thyroid hormone signaling disorders. Since the 1990s, several thyroid hormone analogs have been developed that have tissue specificity. Given the recent approval of two thyroid hormone analogs, the aim of this review is to give an update on developments in the field since 2020.
Summary:
Although initial therapeutic use of thyroid hormone analogs for nonthyroid conditions with metabolic consequences focused on cardiovascular disease and dyslipidemia, nowadays the primary focus is on the treatment of metabolic dysfunction-associated steatohepatitis (MASH). Clinical trials with MGL-3196 (resmetirom) showed significant improvement on hepatic steatosis, fibrosis, and lipids, which led to approval by the U.S. Food and Drug Administration in 2024 for the treatment of MASH. Results are currently awaited for prodrug VK2809, exerting organ specificity through prodrug conversion in the liver, ultimately targeting MASH. For the treatment of genetic thyroid hormone signaling disorders (resistance to thyroid hormone β [RTHβ] and monocarboxylate transporter 8 [MCT8] deficiency), different thyroid hormone analogs have been tested. 3,5,3ʹ-triiodothyroacetic acid (Triac), an endogenous thyroid hormone analog, has been prescribed on a compassionate use basis for RTHβ. In MCT8 deficiency, 3,5-diiodothyropropionic acid has been explored in patients, and Sob-AM2, a prodrug of which the active compound accumulates in the brain, has been investigated in preclinical studies. Recently, the European Medicines Agency has granted market authorization for Triac, being the first approved medicine for this rare disease.
Conclusions:
Ongoing strategies to enhance organ specificity of thyroid hormone analogs should include not only TR specificity but also other determinants of tissue selectivity, such as tissue-specific transporters or enzymes that activate the prodrug. This, together with the recent approval of two thyroid hormone analogs, may ensure a promising future for the development and application of thyroid hormone analogs.
Introduction
Thyroid hormones are important for the metabolism and development of virtually all tissues within the human body. 1,2 The thyroid gland is responsible for the production of thyroid hormones, producing predominantly the inactive precursor thyroxine (T4) and, to a lesser extent, the active hormone 3,3ʹ,5-triiodothyronine (T3). 2 Thyroid hormone production is stimulated by thyrotropin (TSH), secreted by the pituitary. In turn, TSH is regulated by thyrotropin-releasing hormone (TRH) from the hypothalamus. 3 Thyroid hormone homeostasis is achieved via a negative feedback loop, where TRH and TSH are inhibited by circulating T4 concentrations, which are locally converted to T3 at the hypothalamic and pituitary levels, respectively (Fig. 1A). 2,3
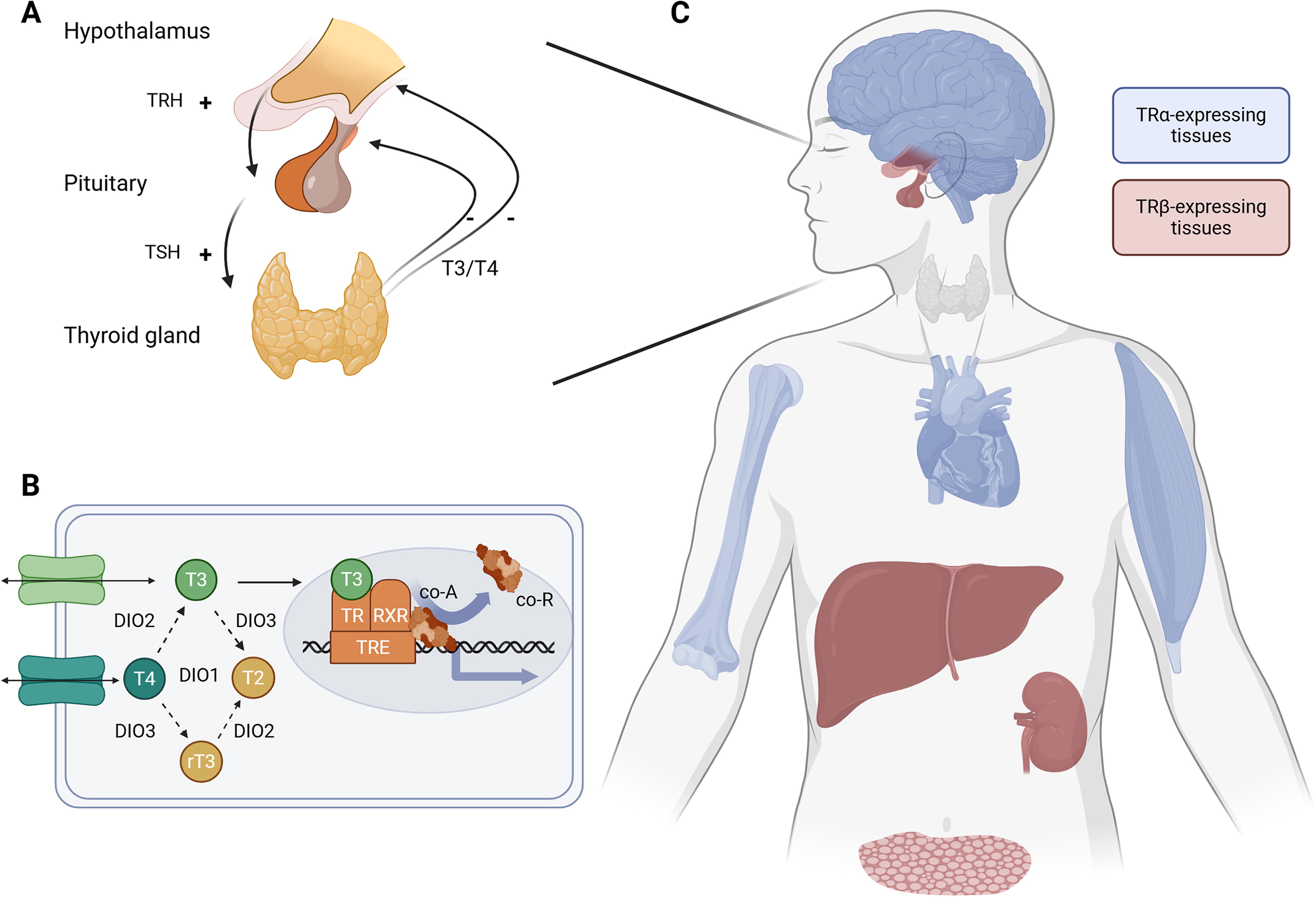
Thyroid hormone action within the human body.
The intracellular availability of thyroid hormones is regulated through different transmembrane transporter proteins and deiodinases, which activate or inactivate thyroid hormones (Fig. 1B). 1,2,4 –6 Intracellular bioactive T3 exerts its genomic actions through binding to nuclear thyroid hormone receptors (TRs) that regulate the transcription of T3-dependent target genes. 1,2 TRs bind to thyroid hormone response elements (TREs), located at the promotor region of T3-dependent target genes. Binding of T3 to the TR results in a dissociation of corepressors and recruitment of coactivators, enabling the transcription machinery to initiate transcription (Fig. 1B). 1 There are two TR types, TRα and TRβ, that differ in their tissue distribution. 1,7 TRα is predominantly expressed in brain, heart, skeletal muscle, and bone, while TRβ is mainly expressed in liver, kidney, and pituitary (Fig. 1C). An imbalance in circulating thyroid hormone concentrations affects all tissues. However, thyroid hormone analogs could potentially uncouple the beneficial and negative effects of thyroid hormones by targeting their thyromimetic activity to specific tissues.
In the past decades, there has been growing interest in developing thyroid hormone analogs for therapeutic application in various disorders (Fig. 2), ranging from nonthyroid conditions with metabolic consequences to genetic disorders in thyroid hormone signaling. Consequently, there have been multiple reviews highlighting several aspects in this field, including an elegant review on thyroid hormone analogs published in this journal in 2020. 8 –12 Therefore, this review will focus on the latest developments in the field from 2020 onward. We will discuss the pharmacological treatment for various nonthyroid conditions with metabolic consequences and for genetic disorders in thyroid hormone signaling. We will highlight two thyroid hormone analogs, MGL-3196 (resmetirom) and 3,5,3ʹ-triiodothyroacetic acid (Triac), that were recently approved by regulatory agencies. 13,14
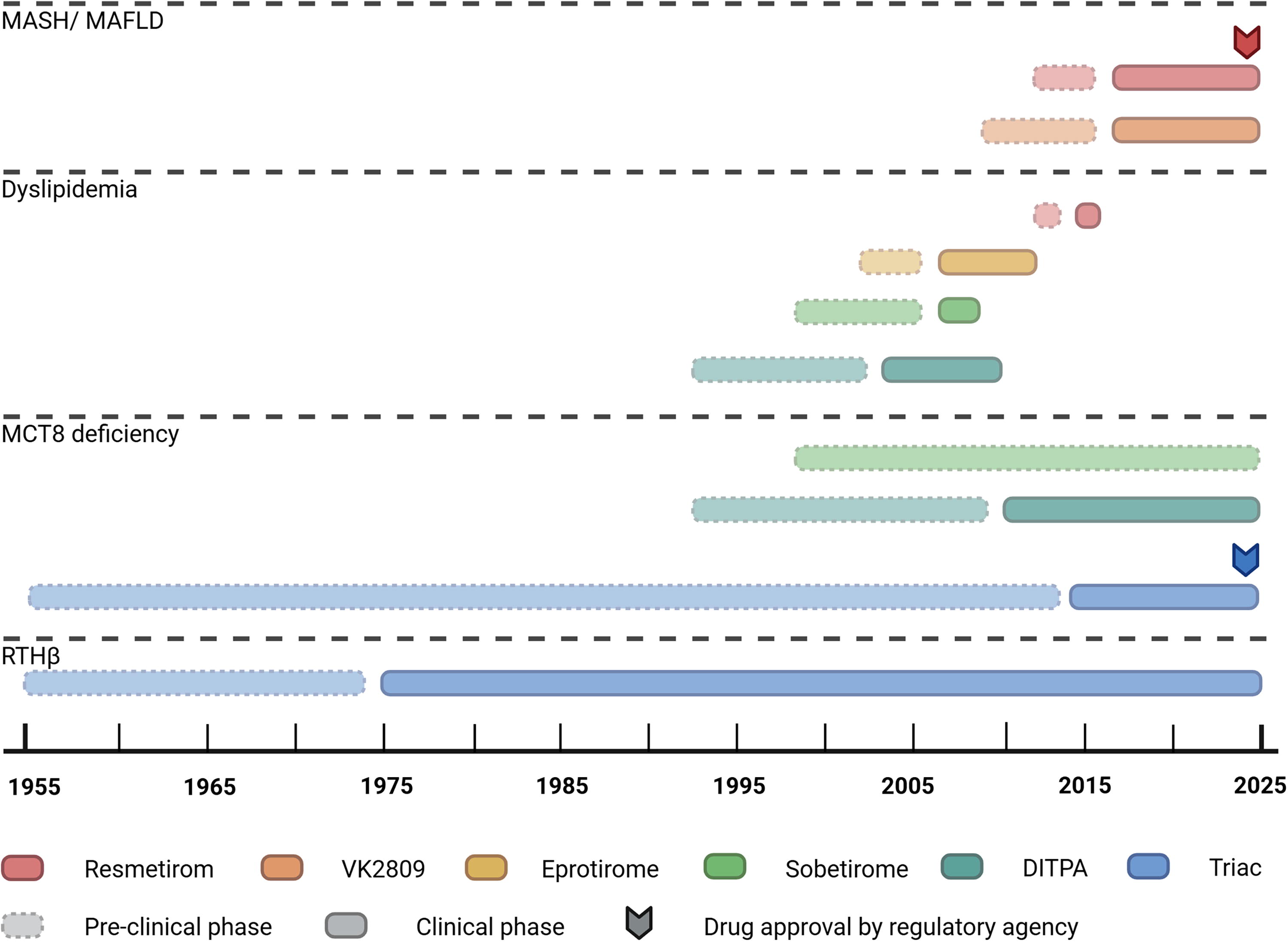
Developmental timeline of thyroid hormone analogs within different fields irrespective of application. The preclinical phase is defined as the period from the start of drug development to either the first administration in humans or the termination of preclinical studies. The clinical phase is defined as the interval between the first clinical administration in human subjects to the present date or termination of clinical studies. The drug approval by the regulatory agency coincides with the moment of the official press release issued by the respective authority. DITPA, 3,5-diiodothyropropionic acid; MAFLD, metabolic dysfunction-associated fatty liver disease; MASH, metabolic dysfunction-associated steatohepatitis; MCT8, monocarboxylate transporter 8; RTHβ, resistance to thyroid hormone β. Created in BioRender. Freund, M. (2025) https://BioRender.com/x08xfhg.
Brief Historical Overview
A shared underlying principle in the development of thyroid hormone analogs is the goal to achieve tissue-specific thyromimetic actions. 9 The clinical observation that thyrotoxicosis leads to an increased heart rate, weight loss, and lipid reduction triggered the exploration of thyroid hormone analogs as a treatment for cardiovascular disease and dyslipidemia. 9 However, treatment with dextrothyroxine, the synthetic mirror form of T4, in euthyroid patients with coronary artery disease proved to be counter effective, with a higher mortality, due to the TRα-mediated thyrotoxicosis. 15 This prompted the development of thyroid hormone analogs that mimic the beneficial thyromimetic effects, without inducing thyrotoxic side effects.
3,5-diiodothyropropionic acid
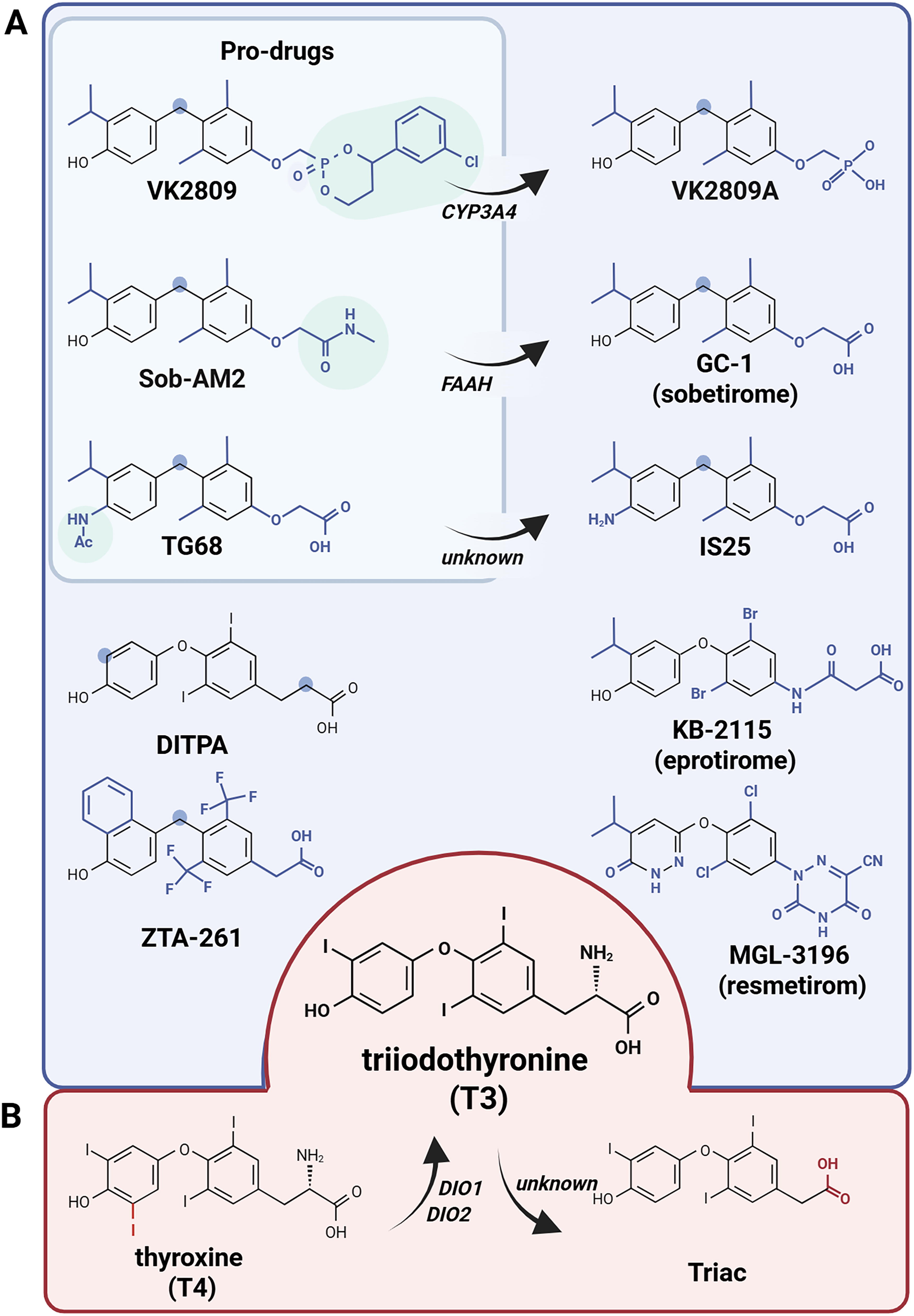
3,5-diiodothyropropionic acid (DITPA) was one of the first analogs that was designed and tested for cardiovascular disease and dyslipidemia. 16 DITPA is structurally different to T3 based on the absence of iodine at the outer ring and the amino group within the amino acid side chain (Fig. 3). It is a nonselective TR agonist with a TRβ binding affinity that is similar to TRα, albeit 350-fold smaller compared with T3. 17 Considering its inotropic effects with small effects on heart rate, it was selected as a candidate for therapeutic use for heart failure. 17 An initial pilot clinical trial showed positive effects on cardiac function as well as a reduction in serum cholesterol and triglycerides. 18 Although a randomized controlled phase II trial also showed positive hemodynamic and metabolic effects, including a reduction in body weight, DITPA was poorly tolerated without evidence for symptomatic benefit. 19,20
Chemical structure of synthetic
Another potential use of thyroid hormone analogs was for the treatment of dyslipidemia. In the liver, T3 stimulates the breakdown of triglyceride-containing lipid droplets via increased lipolysis and consecutive beta-oxidation in the mitochondria. 10 The favorable effects on cholesterol levels are exploited through decreased secretion, increased clearance, and conversion of cholesterol into bile acids. 21 Hence, several groups aimed to develop such molecules with liver-specific thyromimetic activity, thereby enabling favorable effects on lipids while avoiding thyromimetic effects in other tissues (e.g., the heart). To achieve this goal, they exploited the expression of TRβ in the liver to develop molecules with a preferential selectivity of TRβ over TRα. Although the ligand-binding domains (LBDs) are highly similar, there are some differences between the two receptor types. For example, TRα has a serine at position 277, whereas TRβ has an asparagine at the equivalent position. 22 Moreover, in TRβ helices, H3 and H11 seem to be more flexible, allowing larger molecules as ligands. 22,23 Such differences in the molecular structure of the TRs can be exploited to generate compounds with a higher affinity for TRβ. Two well-known examples are sobetirome and eprotirome, which were developed in the 1990s and 2000s, respectively. 9
Sobetirome
GC-1 [3,5-dimethyl-4-(4′-hydroxy-3′-isopropylbenzyl)-phenoxy acetic acid], or sobetirome, has enhanced TRβ specificity through different modifications, such as the amino acid side chain being replaced by an oxoacetic chain, enhancing the polar interaction with the arginine residues in the TRβ pocket (Fig. 3). 24 Furthermore, the iodine atoms, as well as the oxygen atom linking both aromatic rings of T3, are changed into alkyl groups, allowing sobetirome to form more stable interactions with TRβ. Sobetirome has a similar affinity for TRβ as T3, while the affinity for TRα is 10-fold lower, explaining the beneficial effects in the liver, while having limited effects on the heart in a clinical study (Table 1). 39,44,45
Overview of Thyroid Hormone Analogs Applied in Clinical Setting
Thyromimetic action is characterized by the selectivity of the compound to TRβ over TRα (TR selectivity) and its binding affinity to TR relative to T3 (TR potency). TR potency is classified as greater than T3 (<T3), lower than T3 (<T3), or equivalent to T3 (T3-like).
For clinical studies, if available, information is given on the number of patients included, age at baseline, treatment duration and treatment dose. All clinical trials are single-arm open-label studies, unless stated otherwise.
Changes in primary and secondary outcomes are presented as decreased (↓), increased (↑), or unchanged (∼). Relevant additional findings are reported in cursive, following an exclamation mark (!).
CK, creatine kinase; FAAH, fatty-acid-amide hydrolase; LDL, Low-density lipoprotein; MAFLD, Metabolic dysfunction-associated fatty liver disease; MASH, Metabolic dysfunction-associated steatohepatitis; MCT8, Monocarboxylate transporter 8; RTH, Resistance to thyroid hormone; SHBG, sex hormone-binding globulin; TFT, Thyroid function test; TR, Thyroid hormone receptor; TSH, thyroid stimulating hormone; (r)T3, (reverse) triiodothyronine; (f)T4, (free) thyroxine.
Eprotirome
In KB-2115 (3-[[3,5-dibromo-4-[4-hydroxy-3-(1-methylethyl)-phenoxy]-phenyl]-amino]-3-oxopropanoic acid), or eprotirome, the iodine atoms at the inner ring of T3 are replaced by bromine atoms, while the outer ring iodine is replaced by an isopropyl (Fig. 3). 29 The preferential actions of eprotirome on the liver are not only explained by its modest TRβ selectivity but likely also by its selective hepatic uptake through transporter solute carrier family 10A1 (SLC10A1), also known as Na+-taurocholate cotransporting polypeptide. 59 In double-blind randomized placebo-controlled trials (RCTs) in patients with statin-treated dyslipidemia and familial hypercholesterolemia, eprotirome showed substantial positive changes in total and low-density lipoprotein (LDL) cholesterol and triglycerides without effects on high-density lipoprotein (Table 1). 29,30,32 Similar results were obtained in an RCT with primary hypercholesterolemia, who were not on lipid-lowering therapy. 31 Long-term dosing of eprotirome in dogs showed adverse effects on cartilage, leading to the company’s decision to withdraw the drug from further development. 32
Thyroid Hormone Analogs as Pharmacological Treatment in Metabolic Dysfunction-Associated Steatotic Liver Disease
Metabolic dysfunction-associated steatotic liver disease (MASLD) and the more severe metabolic dysfunction-associated steatohepatitis (MASH) display a worrisome increase in prevalence across the world. 60 Fat accumulation in the liver (steatosis) due to metabolic abnormalities is a state called MASLD; once inflammation is present in MASLD, it is called MASH. If these conditions remain untreated, they may progress to cirrhosis, cancer, and liver failure. As such, there is a clinical need for treatment. Thyroid hormone exerts both metabolic effects in the liver (stimulation of lipolysis, beta-oxidation, and lipophagy) as well as anti-inflammatory and antifibrotic effects. 10 Therefore, these effects can be exploited by thyroid hormone analogs in the treatment of MASLD and MASH.
Resmetirom
To obtain MGL-3196 (2-[3,5-dichloro-4-(5-isopropyl-6-oxo-1,6-dihydropyridazin-3-yloxy)phenyl]-3,5-dioxo-2,3,4,5-tetrahydro[1,2,4]triazine-6-carbonitrile), also known as resmetirom, the phenolic outer ring of T3 is changed into a dihydropyridazinyloxy heterocycle, where a isopropyl replaces the iodine atom, while in the second ring two chlorine atoms replace iodine in T3, and the amino acid side chain is replaced by a triazine-carbonitrile heterocycle (Fig. 3). 33 Together, these changes attain a 30-fold selectivity for TRβ over TRα, although the affinity for TRβ is also reduced compared with T3 and other compounds such as sobetirome, explaining the need for higher doses. Further hepatic selectivity is conferred by liver uptake through the liver transporter solute carrier organic anion transporter family member 1B1 (OATP1B1). 61 Animal studies showed positive effects of resmetirom on total lipids and LDL cholesterol, and in a first-in-human study, these effects were also observed in healthy subjects (Table 1). 33,34
Several clinical trials have investigated the effects of resmetirom on different outcomes. In the placebo-controlled phase II MGL-3196-05 trial in 116 patients with MASH, resmetirom sustainably reduced hepatic fat, as assessed by magnetic resonance imaging (MRI) after 12 weeks of treatment. 35 Clinically relevant reduction of multiple atherogenic lipids, decreased liver enzymes, and inflammatory markers underscored these positive effects. Next, the placebo-controlled phase III (MAESTRO-NAFLD-1) trial in 972 patients with MASH showed that resmetirom was safe and well-tolerated with a treatment duration of 52 weeks. 36 Similar effects were observed in the reduction of hepatic fat, LDL, and triglycerides levels as in the earlier study, with a dose-dependent effect. Reported adverse events were diarrhea and nausea at the initiation of treatment. Only a minor reduction in free T4 concentration was observed, and no effects on TSH and free T3 concentrations were reported. Another phase III study, the MAESTRO-NASH trial in 966 patients with MASH showed a higher resolution of MASH after 52 weeks of treatment with resmetirom (and improvement in fibrosis). 37 These two phase III trials were pivotal for the approval of resmetirom for the treatment of MASH with moderate to advanced liver fibrosis by the Food and Drug Administration of the United States. 13 Currently, one additional study evaluates the effect of resmetirom in patients with well-compensated MASH cirrhosis (NCT05500222), of which the completion is expected in 2027.
VK2809
VK2809 (MB07811) (2R,4S)-4-(3-chlorophenyl)-2-[(3,5-dimethyl-4-(4′-hydroxy-3′-isopropylbenzyl)phenoxy)methyl]-2-oxido-[1–3]-dioxaphosphonane is a liver-specific prodrug (Fig. 3). 53 After first-pass hepatic extraction, this prodrug is converted into the active compound VK2809A (MB07344) (3,5-dimethyl-4-(4′-hydroxy-3′-isopropylbenzyl)phenoxy)methylphosphonic acid) through the oxidation of the benzylic methine proton by cytochrome P3A4 (CYP3A4). VK2809A is highly similar to sobetirome, albeit with a lower affinity for the TRs. Preliminary results of the phase IIa randomized, double-blind, placebo-controlled trial (NCT02927184) in 45 patients with MAFLD showed reduced hepatic fat as assessed by MRI after 12 weeks of treatment (Table 1). 57 Recently, the first results of the phase IIb VOYAGE trial (NCT04173065) with VK2809 were reported, in which 178 patients with MASH were treated for 12 months. 58 For all but the lowest dose, a significant reduction of steatosis after 3 months of treatment and improvement in liver fibrosis were observed after 52 weeks. No major safety issues were reported. Detailed results are awaited, as no follow-up studies have been announced.
Other analogs
Based on the success of resmetirom in the treatment of MASH, new analogs are still being developed. In 2020, compound IS25 (2-(4-(4-amino-3-isopropylbenzyl)-3,5-dimethylphenoxy)acetic acid) and its prodrug TG68 (2-(4-(4-acetamido-3-isopropylbenzyl)-3,5-dimethylphenoxy)acetic acid) were discovered (Fig. 3). 62,63 The structure of IS25 is highly similar to sobetirome, and with computational analysis, it was inferred that the specificity for TRβ was higher than for TRα. One of the newest thyroid hormone analogs is ZTA-261 (2-[4-[(4-hydroxynaphthalen-1-yl)methyl]-3,5-bis(trifluoromethyl)phenyl]acetic acid), a derivate of sobetirome, where the outer aromatic ring is changed into a naphthol to increase hydrophobic interaction with TR (Fig. 3). 64 The affinity for TRβ is similar to T3, but with a 100-fold lower affinity for TRα. Animal studies for these compounds showed significant reductions of serum and liver lipids, but clinical studies have not been planned. 64 –66
The anticipated added value of TRβ-specific analogs has ultimately led to the approval of resmetirom as the first treatment for MASH. Hence, both the European and American guidelines recommend treatment with resmetirom in adults with moderate to advanced liver fibrosis. 67,68 However, further clinical studies are needed to compare resmetirom to other therapies that have been shown to be effective. Although no head-to-head trials have been performed, other treatments such as vitamin E or glucagon-like-polypeptide-1 agonists seem equally or even more effective and are often available for lower costs. 69 –72
Still, with several clinical studies awaiting results and new compounds continuing to be developed, there is a promising future for even more advanced treatments for MASH via thyroid hormone analogs.
Thyroid Hormone Analogs in Resistance to Thyroid Hormone Beta
Resistance to thyroid hormone β (RTHβ) is typically caused by a heterozygous pathogenic variant in the LBD of TRβ (encoded by the THRB gene), with a prevalence of 1:19,000–40,000 individuals. 73,74 Mutant TRβ interferes with the normal function of wild-type TRβ, a phenomenon called dominant negative inhibition. 74 –76 TRβ-expressing tissues (e.g., pituitary, liver) are insensitive (resistant) to thyroid hormones, while TRα-expressing tissues (e.g., heart, bone) retain normal sensitivity. Due to reduced sensitivity of the hypothalamus–pituitary axis to thyroid hormones, patients with RTHβ demonstrate a distinctive biochemical profile, characterized by elevated (F)T4 and (F)T3 concentrations with nonsuppressed TSH concentrations.
Patients with RTHβ may exert clinical features of tissue-specific hypothyroidism (e.g., elevated cholesterol concentrations) and thyrotoxicity (e.g., anxiety and palpitations). 74,77 Recently, a 2–3 times elevated risk of mortality rate and ∼10-times risk of atrial fibrillation in untreated patients with RTHβ was reported. 78,79 Hence, there is a clear need for therapies that overcome the resistance in TRβ-expressing tissues while accomplishing a euthyroid state in TRα-expressing tissues. Ideally, a compound should have sufficient thyromimetic potency to overcome the reduced binding affinity of mutant TRβ, without further increasing thyromimetic action on TRα. 11,12
Triac
3,5,3ʹ-triiodothyroacetic acid, also called tiratricol or Triac, is an endogenous T3 metabolite found in human serum at concentrations ∼50-fold lower than T3 (Fig. 3). 80 In Triac, the amino acid side chain is replaced by an acetic acid, although the endogenous metabolism pathway has not been entirely elucidated. Compared with T3, Triac has a higher affinity for TRβ, which is also retained in a subset of TRβ mutants, while affinity of Triac for TRα is similar to T3. 81 –84 Therefore, Triac has been explored as potential treatment in patients with RTHβ, mostly reported as case reports or case series (Table 1). 11 Most patients favorably responded by a reduction in (F)T4 and TSH concentrations along with alleviation of thyrotoxic symptoms, such as goiter, tachycardia, and excessive perspiration. 11 Currently, the place of Triac in the treatment of RTHβ is not clear. 85 Clinical trials are necessary to investigate the effectiveness of Triac on different outcomes, including cardiovascular morbidity, in patients with RTHβ.
Thyroid Hormone Analogs in MCT8 Deficiency
Monocarboxylate transporter 8 (MCT 8) is a very specific thyroid hormone transporter, facilitating transport of T3 and T4. 4 Pathogenic variants within SLC16A2, the gene encoding MCT8, lead to MCT8 deficiency, estimated to occur in 1:70,000 male individuals. 86 –88 Patients with MCT8 deficiency exhibit a characteristic biochemical profile of elevated (F)T3, low-normal (F)T4, and a nonsuppressed TSH concentrations. 89 Due to the essential role of MCT8 in thyroid hormone transport across the blood–brain barrier, defective MCT8 results in cerebral hypothyroidism. 90 –92 Since thyroid hormones are crucial for brain development, 91 patients with MCT8 deficiency have severe intellectual and motor disabilities. 89,93 Simultaneously, tissues independent on MCT8 (i.e., liver, heart, muscle) are exposed to elevated T3 concentrations, leading to thyrotoxic symptoms such as tachycardia and elevated blood pressure and contributing to a low body weight. 89,93 Treatment of MCT8 deficiency should focus on increasing thyroid hormone availability in the brain while alleviating signs and symptoms of peripheral thyrotoxicosis. Thyroid hormone analogs that enter the cell independent of MCT8 may serve this therapeutic goal by alleviating the T3-mediated thyrotoxicosis through TSH suppression and by bypassing the defect at the blood–brain barrier.
DITPA
DITPA was first explored as a potential therapeutic compound in MCT8 deficiency when Di Cosmo et al. showed that in Mct8 KO mice, reflecting only the thyrotoxic phenotype of MCT8 deficiency, DITPA enters the cell independent of MCT8 (Table 1). 25 Subsequent research by Ferrara et al. showed a successful decrease in serum TSH and T3 concentrations in the same mouse model. 26 DITPA use in MCT8 deficiency has been reported in four patients between 8.5 and 25 months old who were treated for 26–40 months on a compassionate use basis. 28 All four patients showed a reduction in T3 upon DITPA initiation, although thyrotoxicity-related clinical effects varied, with some experiencing improvements in heart rate and body weight, while others showed no significant changes. 28 Potential rescue of the neurodevelopmental disorder in MCT8 deficiency is currently the topic of investigation during an ongoing trial (NCT04143295) that allows DITPA treatment to start prenatally.
Sob-AM2
2-[4-[[4-Hydroxy-3-(1-methylethyl)phenyl]methyl]-3,5-dimethylphenoxy]-N-methylacetamide, or Sob-AM2, is an amide prodrug of sobetirome where the negatively charged carboxylate group is replaced by an amide, thereby increasing the permeability of the blood–brain barrier (Fig. 3). 94,95 Sob-AM2 can be metabolized in the brain by fatty acid amide hydrolase and leads to a ∼20-fold increase in cerebral sobetirome concentrations while limiting circulating concentrations. 96 In 30-day old Mct8/Dio2 dKO mice, reflecting the thyrotoxic and neurological components of MCT8 deficiency, sobetirome and Sob-AM2 led to equivalent reductions in T4 and T3 concentrations and equal activation of cerebral T3-dependent target genes (Table 1). 38 The same murine model has been used to show that Sob-AM2 is able to cross the placenta and stimulate fetal cerebral T3-dependent target genes as well. 46 Although Sob-AM2 shows promising potential in targeting the neurological aspects of MCT8 deficiency, clinical experience is lacking, with no clinical trials planned in the near future.
Triac
Preclinical findings in cells and murine models demonstrated that Triac can enter cells independently of MCT8. 47 Several studies in Mct8/Oatp1c1 dKO, mimicking the thyrotoxic and neurological phenotype of MCT8 deficiency, demonstrated that Triac has the potential to fully rescue neurological impairment by restoring T3-dependent neural differentiation, white matter loss, myelination, and brain network dysfunction (Table 1). 47 –49 These effects were only observed when treatment was initiated before the third postnatal week in mice, indicating that (partial) rescue of the neurological phenotype might be possible in humans, given that treatment is initiated in early postnatal life. 49
In a single-arm phase II trial (Triac Trial I) in 46 pediatric and adult patients with MCT8 deficiency, Triac treatment for 12 months substantially reduced T3 concentrations. 51 Secondary outcomes on thyrotoxicity improved as well, including body weight, heart rate, premature atrial contractions, blood pressure, and tissue-specific biochemical markers. 51 These results were validated in a real-world retrospective cohort study of 67 patients with MCT8 deficiency, indicating that the amelioration of thyrotoxicosis in MCT8 deficiency is safe and sustainable. 50 The potential impact of Triac treatment on neurocognitive development in MCT8 deficiency is currently being investigated in a phase II clinical trial (NCT02396459), involving pediatric male patients under 30 months old, with results expected this year. In December 2024, the European Medicines Agency approved Triac as a drug for peripheral thyrotoxicosis treatment in MCT8 deficiency, being the first approved medicine for this rare disease. 14
Ongoing or Other Developments
New applications for thyroid hormone analogs are continuously being explored. This is exemplified in the work undertaken by Li et al. (2024), which proposes sobetirome as an anti-inflammatory strategy in acute lung injury and acute respiratory distress syndrome 97 building on a previous study by Yu et al. (2018), indicating that sobetirome significantly alleviates pulmonary fibrosis. 98 In glycogen storage disease type Ia, caused by deficient glucose-6-phosphatase, VK2809 has shown promising results in decreasing hepatic triglyceride levels, potentially mitigating the increased risks of hepatosteatosis present in this disease. 99 All abovementioned studies use murine models to reflect the respective disease entities, and developments have not yet progressed toward clinical applications. Nevertheless, these studies underscore the extensive reach of thyroid hormone signaling, highlighting the potential of thyroid hormone analogs for therapeutic application across a wide spectrum of diseases.
The beneficial effects of sobetirome and Sob-AM2 in several demyelinating murine models have opened the door for the potential use of thyroid hormone analogs as pro-remyelinating therapy targeting demyelinating diseases, such as multiple sclerosis, multiple system atrophy, and Pitt–Hopkins syndrome. 100 –103 Also for X-linked adrenoleukodystrophy, a genetic disorder with central nervous system demyelination and adrenal insufficiency, sobetirome has previously been shown to effectively lower very long-chain fatty acid accumulation in serum and tissues through upregulation of the ABCD2 gene in different murine models, addressing the presumed pathogenic mechanism behind the disease. 104,105 However, two previously planned clinical trials for X-linked adrenoleukodystrophy (NCT01787578, NCT03196765) were withdrawn, allegedly due to the need for revisions in the original protocol and lack of funding, respectively.
In the field of RTH syndromes, thyroid hormone analogs targeting specific mutants or corepressors have gained attention. One study developed a compound, called 16 g, that, apart from showing high TRβ selectivity, also shows efficient binding to one specific TRβ (H435R) mutant. 106 Another study by Romartinez-Alonso et al., focusing on resistance to thyroid hormone α, has identified ES08 as a compound to dissociate aberrant corepressor binding, which is a key mechanism underlying dominant negative inhibition in RTH. 107 Such studies highlight the potential to develop disease- and mutation-specific thyroid hormone analogs.
Future Perspectives
Since the discovery of sobetirome in the 90s as the first synthetic thyroid hormone analog specifically aimed at the TRβ isoform, the field of thyroid hormone analogs has expanded. Numerous thyroid hormone analogs have been developed with varying success rates. Although the original aim, namely a treatment for cardiovascular disease and dyslipidemia, is not prioritized anymore, the recent and first-ever approval of two thyroid hormone analogs shows the potential of this class of drugs.
Ongoing strategies to enhance organ specificity of thyroid hormone analogs should include not only TR specificity but also other determinants of tissue selectivity, such as tissue-specific transporters or enzymes that inactivate the drug or activate the prodrug. If the decades of experience in thyroid hormone analog development can be used in a fruitful way, we anticipate that the recent regulatory approvals of two thyroid hormone analogs are signposts to a promising future for this class of drugs.
Footnotes
Authors’ Contributions
M.F.T.F., F.v.d.M., and W.E.V.: Conceptualization (equal), investigation (equal), visualization (equal), writing—original draft (equal), and writing—review and editing (equal). S.G. and F.S.v.G.: Conceptualization (supporting) and writing—review and editing (equal).
Author Disclosure Statement
Erasmus Medical Center (Rotterdam, the Netherlands), which employs all authors, receives royalties from Egetis Therapeutics, the company manufacturing Triac. The authors do not benefit personally from these royalties. M.E.T.F., F.v.d.M., S.G., and W.E.V. have no conflicts of interest to disclose. F.S.v.G. is a paid consultant for Egetis Therapeutics and has no further conflicts of interest to disclose.
Funding Information
M.E.T.F., F.v.d.M., S.G., and F.S.v.G. have no funding information to declare. W.E.V. received funding from the Sherman Foundation.